
Abstract
Peripheral arterial stiffness and endothelial function, which are independent predictors of cardiac events, are abnormal in firefighters. We examined the effects of aspirin on peripheral arterial stiffness and endothelial function in firefighters. Fifty-two firefighters were randomized to receive daily 81 mg aspirin or placebo for 14 days before treadmill exercise in thermal protection clothing, and a single dose of 325 mg aspirin or placebo immediately following exertion. Peripheral arterial augmentation index adjusted for a heart rate of 75 (AI75) and reactive hyperemia index (RHI) were determined immediately before, and 30, 60, and 90 minutes after exertion. Low-dose aspirin was associated with lower AI75 (–15.25±9.25 vs −8.08±10.70, p=0.014) but not RHI. On repeated measures analysis, treatment with low-dose aspirin before, but not single-dose aspirin after exertion, was associated with lower AI75 following exertional heat stress (p=0.018). Low-dose aspirin improved peripheral arterial stiffness and wave reflection but not endothelial function in firefighters.
Introduction
Sudden cardiac events are the leading cause of mortality in firefighters, accounting for approximately half of line-of-duty fatalities. 1 This line-of-duty death rate outnumbers that for any other occupation in the United States. 1 It is thought that the combination of high levels of heat stress and physical exertion lead to sudden cardiac events in susceptible firefighters2,3 through hyperthermia, dehydration, inflammation and considerable cardiovascular strain.4,5 Research also indicates that prolonged periods of firefighting have an unfavorable impact on vascular function, including increased arterial stiffness and wave reflection, 6 both of which predict all-cause and cardiovascular mortality in the general population.7,8 Subclinical vascular dysfunction may mediate the link between firefighting activities and sudden cardiovascular events. Therefore, a preventative strategy to reduce cardiovascular death in firefighters may include therapeutics targeting subclinical vascular dysfunction.
Aspirin, which has both anti-inflammatory and anti-thrombotic properties, is beneficial for primary and secondary prevention of vascular disease.9–11 Previous studies indicate that aspirin mitigates endothelial dysfunction 12 that is associated with acute systemic inflammation in humans. 13 However, the effects of aspirin on exertional heat stress, which is known to be associated with systemic inflammation, 14 has not been established. Whether aspirin alters peripheral arterial stiffness, wave reflection and endothelial function after exertional heat stress, in firefighters, is presently unknown. Therefore, we investigated the acute and chronic effects of aspirin on peripheral arterial stiffness, wave reflection and endothelial function in a double-blinded, factorial randomized controlled study of firefighters subjected to exertional heat stress.
Methods
Study population
Subjects were a subgroup from a larger study examining the effect of aspirin and active cooling on platelet function in firefighters. 15 In that study, active cooling was delivered after exertion by 20 minutes of hand and forearm immersion into cold-water immersion. Only subjects randomized to receive passive cooling are included in this analysis. Subjects were volunteer and career firefighters recruited from fire departments and emergency services agencies from Western Pennsylvania via direct mailings to firehouses, electronic mail announcements from the County and State Fire Academies, and by presentations made at training classes and union meetings. Subjects with a history of cardiovascular disease, smoking, use of medications expected to blunt the physiologic response to a treadmill exercise, prescription medications with known side effects of impaired thermoregulation, and use of medications and supplements known to alter vascular function (e.g. arginine, omega-3 fatty acids, NSAIDS, tobacco products), known history of platelet dysfunction, or aspirin allergy/intolerance were excluded. Female subjects were screened for pregnancy prior to the screening and protocol visits. Those with a positive pregnancy test were excluded. The University of Pittsburgh Institutional Review Board approved the Enhanced Firefighter Rehab Trial (clinicaltrials.gov NCT01066923) and all subjects provided written informed consent prior to participation.
Screening
Subjects received a physical examination from a study physician including a 12-lead electrocardiogram (ECG) and maximal exercise ECG stress test. Height was determined with a stadiometer and mass using a digital scale accurate to 0.5 g (Kern & Sohn GmBH, Germany). Body fat was determined by three skinfold measurements. Exclusion criteria included hypertension during screening and a resting or exercise ECG suggesting the presence or history of coronary heart disease.
Protocol
Subjects were randomly assigned to receive aspirin (81 mg) or placebo taken daily for 14 days prior to the protocol visit and a single dose of chewable aspirin (325 mg) or placebo administered immediately after exercise. Based on this factorial randomization before and after exertional heat stress, subjects were categorized into four groups: aspirin before and aspirin after (AA); aspirin before and placebo after (AP); placebo before and aspirin after (PA); and placebo before and placebo after (PP) exertional heat stress. The 81 mg low dose before exertional heat stress was chosen because it is the common dose used in primary and secondary prevention of adverse cardiovascular events. A single 325 mg dose immediately after exertional heat stress was chosen because it is the recommended dose given immediately after acute cardiovascular events including acute coronary syndromes and stroke.
To ensure equivalent pre-exertional heat stress nutrition, subjects received a standardized meal consisting of meal replacement bars (PowerBar; Glendale, CA, USA, and Clif Bar; Berkeley, CA, USA) and 400–600 mL of water 1 hour before testing. Subjects were fitted with a heart rate monitor and skin temperature probes. Following instrumentation, subjects were dressed in a standard uniform of long pants and a short-sleeve cotton t-shirt and donned thermal protective clothing consisting of turnout pants and coat (Body-Guard; Lion Apparel, Dayton, OH, USA), Nomex hood (Majestic Fire Apparel, Inc., Lehighton, PA, USA), steel-toed rubber boots (Servus Products, Rock Island, IL, USA), polycarbonate helmet (Paul Conway, Dayton, OH, USA), and leather gloves. Subjects wore a self-contained breathing apparatus (SCBA) (Firehawk; MSA, Pittsburgh, PA, USA). The SCBA mask was worn during the protocol but left open to room air. Depending on the subject’s size, thermal protective clothing and SCBA mass varied slightly by around 20 kg.
Subjects walked on the treadmill in a room heated to 38.9±1.1°C and 19.8±3.8% relative humidity (RH). They performed a treadmill exercise protocol designed to simulate the timing of interior fire suppression. 4 Subjects initially walked at 4.5 km/h on a 2.5% incline. After 20 minutes, the treadmill was lowered to a level position and the speed was decreased to 2.5 km/h for 3 minutes to mimic exiting the fire structure followed by a 4-minute standing period to simulate having their SCBA cylinder changed. Following the standing period, subjects again walked at 2.5 km/h on a 0% incline for 3 minutes, followed by a 20-minute bout of walking at 4.5 km/h on a 2.5% incline to simulate returning to the fire structure for a second period of fire suppression. Total protocol duration length was 50 minutes. Subjects ended exercise when they completed the 50-minute protocol or when one of the following termination criteria was achieved: (1) subject request; (2) heart rate exceeding 220 – age + 10 bpm; (3) body core temperature exceeding 39.5°C; and (4) unsteady gait while walking on the treadmill.
Following exercise, subjects exited the hot room and removed the protective clothing. The recovery period began 10–15 minutes after the end of exercise. During recovery, subjects sat in a folding chair and consumed 325 mg of chewable aspirin or chewable placebo pills at time zero of recovery.
Digital pulse amplitude tonometry
Peripheral arterial wave reflection and endothelial function were assessed immediately before (baseline) and then at 30, 60, and 90 minutes following exertional heat stress using non-invasive digital pulse amplitude tonometry (PAT).
Endothelial function assessment
Baseline pulse amplitude was measured in a fingertip from each hand for 5 minutes. 16 Arterial blood flow was interrupted in one arm for 5 minutes by a blood pressure cuff placed on a proximal forearm at whichever occlusion pressure was higher: 200 mmHg or 60 mmHg above systolic blood pressure. The cuff was abruptly deflated after 5 minutes of arterial occlusion, and the PAT signals from both hands were recorded for an additional period of 5 minutes (post-deflation). The contralateral finger was used as a control for measuring non-endothelial-dependent systemic changes. Pulse amplitude was analyzed by a computerized, automated algorithm (EndoPAT; Itamar Medical, Israel) that provides the average pulse amplitude for each 30-second interval after forearm cuff deflation up to 5 minutes. The contralateral finger was utilized as a control for measuring non-endothelial-dependent systemic changes. PAT reactive hyperemia index (RHI), a measure of endothelial dysfunction, was defined as the natural logarithm of the ratio of post-deflation to baseline averaged PAT signal amplitudes in the hyperemic finger divided by the same ratio in the contralateral finger that served as control. 17
Peripheral arterial stiffness and wave reflection
PAT augmentation index (AI), a measure of peripheral arterial stiffness and wave reflection, was determined by a computerized algorithm generated to automatically identify pulse wave peak pressures and inflection point. AI was derived by EndoPAT by averaging multiple pulses and was calculated by the following formula: AI = (P2 − P1) ×100 / P1 (%), where P1 = systolic peak pressure and P2 = pressure corresponding to the inflection point. Since AI varies with heart rate, AI was normalized to a standard heart rate of 75 beats/minute (AI75). 18
Statistical analysis
Continuous and categorical variables were expressed as means ± standard deviations and frequencies with proportions, respectively. Demographic (gender, age) and morphometric (height, mass, and body fat) data were compared across the groups to assess the balance in baseline characteristics. Continuous variables were compared by t-test or one-way analysis of variance (ANOVA) as appropriate; the chi-squared test was applied for categorical variables.
Two-way repeated-measures ANOVA was used to examine the effects of exertional heat stress on outcomes (peripheral arterial stiffness and endothelial function) based on the main effect of time, the main effect of treatment group, and the interaction between those two effects as follows: all randomization arms (aspirin–aspirin versus aspirin–placebo versus placebo–aspirin versus placebo–placebo); first randomization arms (aspirin–aspirin plus aspirin–placebo versus placebo–aspirin plus placebo–placebo); and second randomization arms (aspirin–aspirin plus placebo–aspirin versus placebo–placebo plus aspirin–placebo) at four time points (baseline, 30, 60, and 90 minutes). To complement these analyses, subgroup analyses were performed with two-way repeated measures ANOVA comparing outcomes in placebo only (PP) to: (1) low-dose aspirin only (AP) and (2) single high-dose aspirin only (PA) groups. Statistical significance was set at p < 0.05. SPSS 21 (IBM Corp., Armonk, NY, USA) was used for all analyses.
Results
Baseline characteristics
Overall, 52 career and volunteer firefighters (100% white, mean age 31.8±8.6 years, 92.3% male) were randomly assigned to aspirin before and after exercise (AA, n=13), placebo before and after exercise (PP, n=13), aspirin before and placebo following exercise (AP, n=14), and placebo before and aspirin following exercise (PA, n=12) groups. For the entire sample, the mean body mass index was 27.7 kg/m2. The mean AI75 and RHI were −11.8 and 1.9, respectively. The baseline demographic and clinical characteristics were similar among the groups as detailed in Table 1. Physiologic responses to exertional heat stress have been reported in the main trial. 15 Of note, physiologic responses to exertional heat stress were not significantly different among AA, PP, AP and PA groups. 15
Baseline characteristics of study participants by treatment groups.
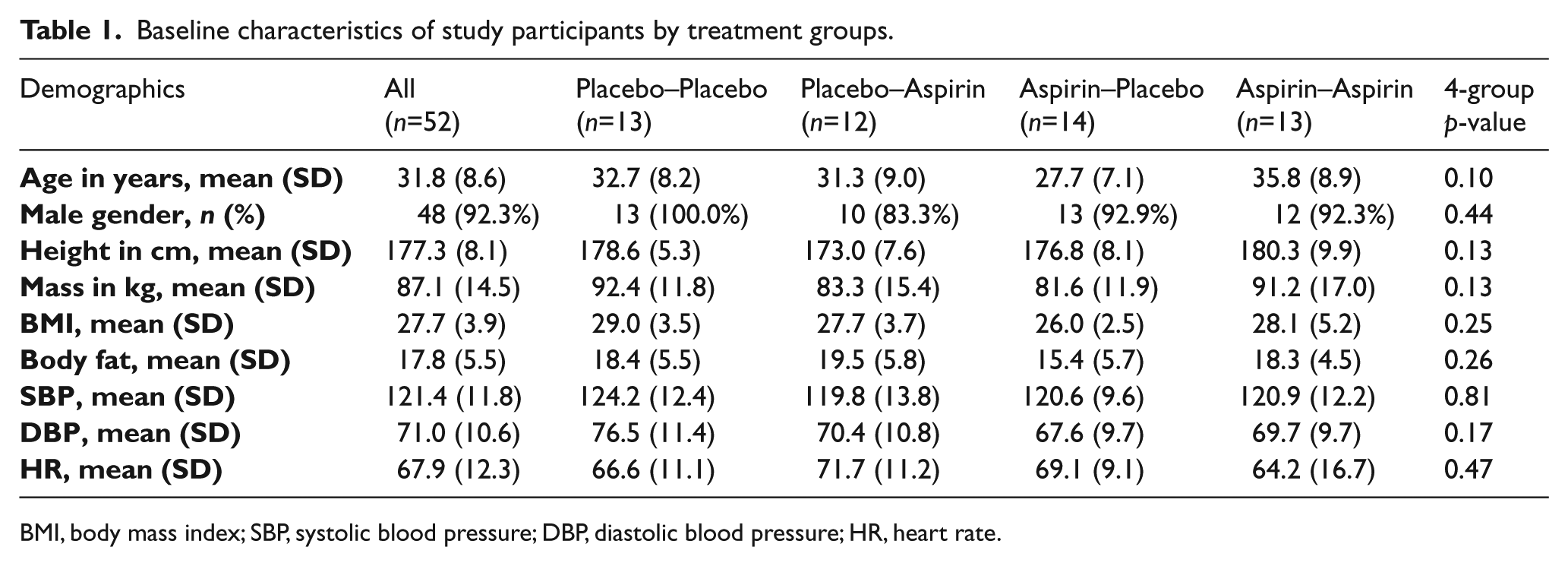
BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate.
Vascular response to exertional heat stress
Lower AI75 and higher RHI indicate healthier blood vessels. Analysis based on all the randomization arms are presented in Figure 1 and Table 2. There was an initial nominal, non-significant rise in AI75 at 30 minutes after exertional heat stress (p=0.185). AI75 decreased significantly to lower values as time progressed from 30 minutes up to 90 minutes in all four groups (p<0.001), denoting decreasing peripheral arterial stiffness (Figure 1A). Similarly, there was a nominal, non-significant decrease in endothelial function determined by RHI at 30 minutes (p=0.333) in the overall study population, followed by a significant increase (i.e. improvement) in RHI as time progressed to 90 minutes after exertional heat stress (p=0.03) (Figure 1B). Overall, the aspirin treatment group was significantly associated with AI75 (p=0.03). The treatment group was not significantly associated with RHI (p=0.84). There was no interaction effect between time and aspirin treatment allocations on AI75 (p=0.44) and RHI (p=0.18).
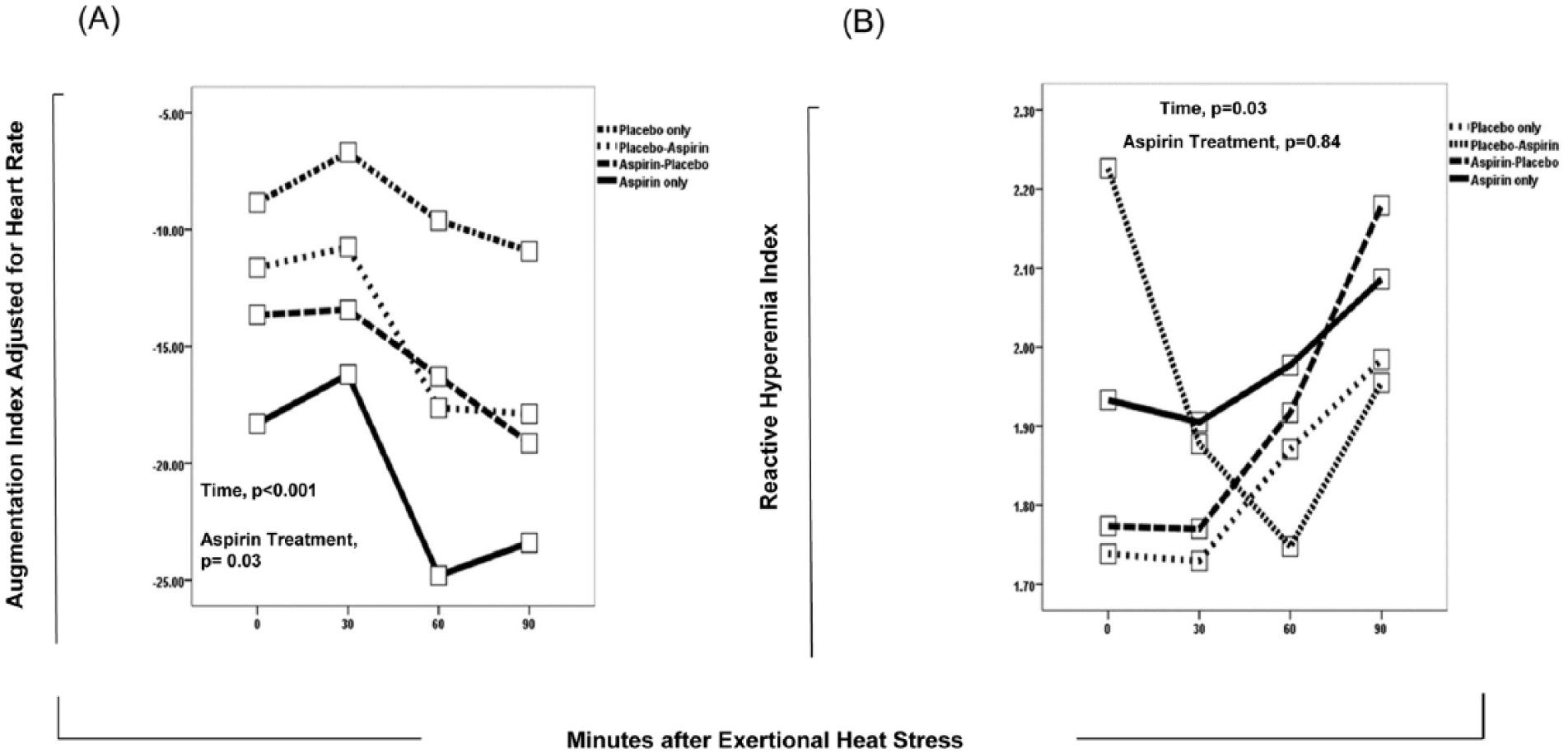
Changes in augmentation index adjusted for heart rate (A) and reactive hyperemia index (B) by time and aspirin treatment assignment.
Adjusted augmentation index (AI) and reactive hyperemia index (RHI) by groups and time.
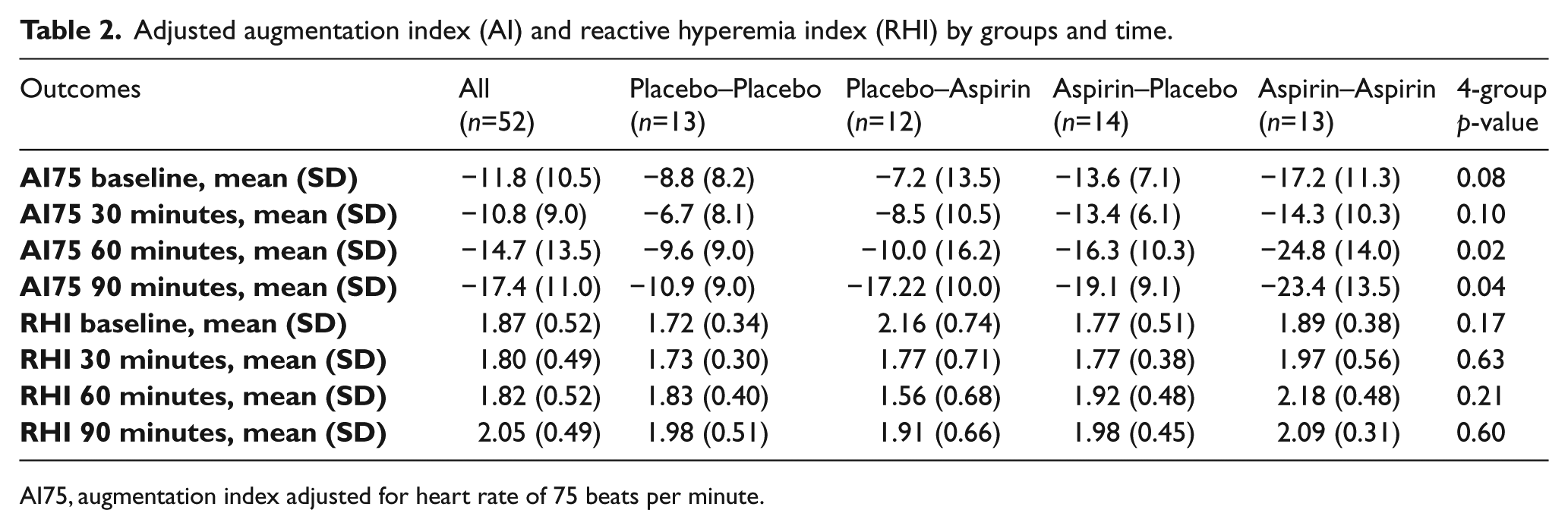
AI75, augmentation index adjusted for heart rate of 75 beats per minute.
Effect of daily low-dose aspirin pre-treatment on primary outcomes
For the analysis based on first randomization by low-dose aspirin pre-treatment, the group that received daily low-dose (81 mg) aspirin for 2 weeks had lower AI75 compared to placebo (–15.25±9.25 vs −8.08±10.70, p=0.014) prior to exertional heat stress. On repeated measures analysis, AI75 remained significantly lower (p=0.018) in the low-dose aspirin group after exertional heat stress compared to placebo, indicating that the 2-week pre-treatment with aspirin had a beneficial effect on peripheral arterial stiffness both before and after exertional heat stress (Figure 2A). Subgroup analysis showed that the low-dose aspirin pre-treatment only (AP) group had a significantly lower AI75 (p=0.029) compared to the placebo only (PP) group.
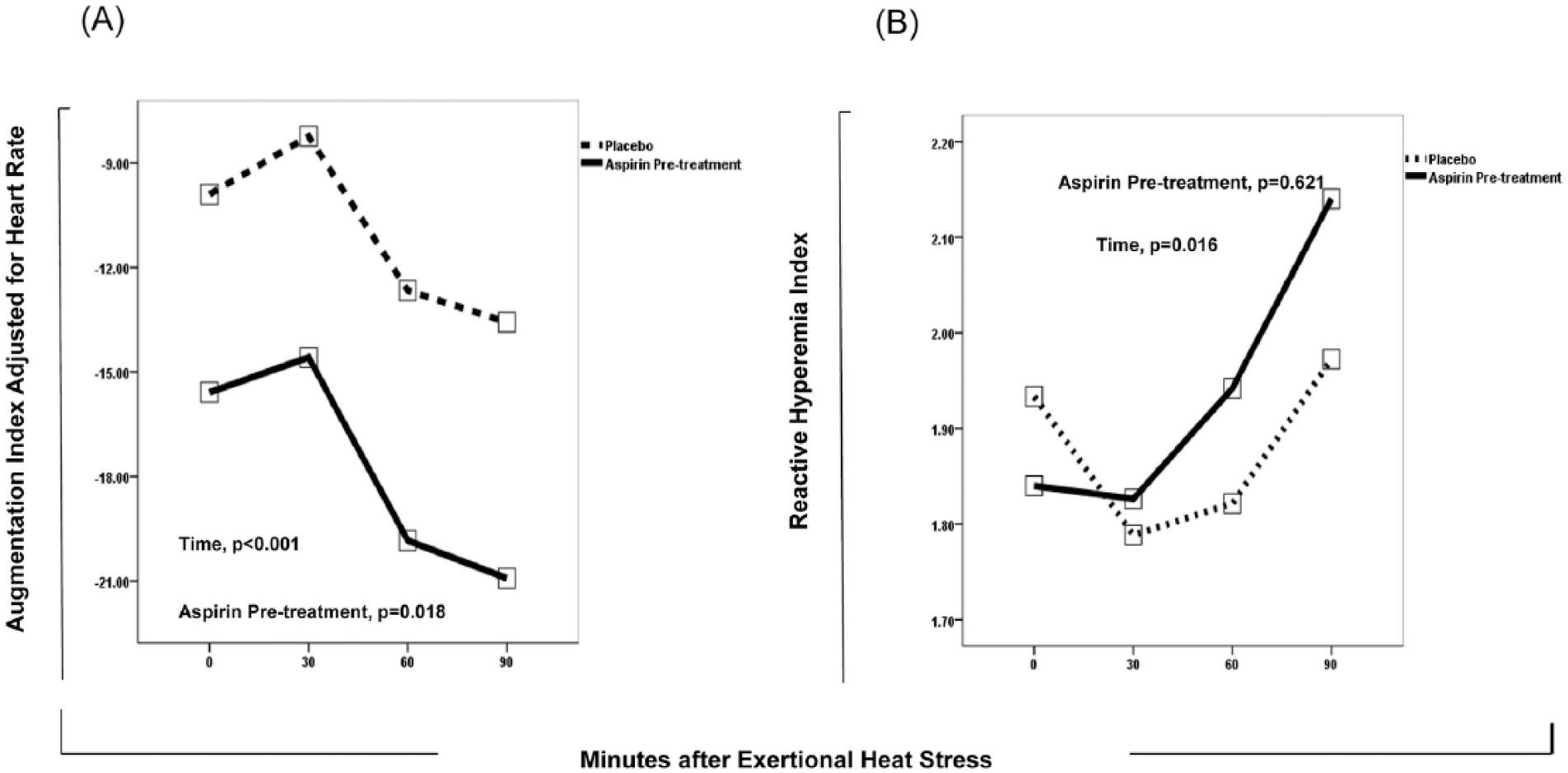
Changes in augmentation index adjusted for heart rate (A) and reactive hyperemia index (B) by time and low-dose aspirin pre-treatment assignment.
In contrast, pre-treatment with low-dose aspirin (81 mg) had no effect on RHI before (1.83±0.45 vs 1.92±0.59, p=0.521) or after exertional heat stress (p=0.84) (Figure 2B).
Effect of single-dose (325 mg) aspirin chewed after exertional heat stress on primary outcomes
For the analysis based on second randomization by a single dose (325 mg) of aspirin chewed immediately after exertional heat stress, the group that received single-dose aspirin showed a trend towards being associated with a lower AI75 (p=0.058) (Figure 3A). However, adjusted analysis controlling for baseline differences in AI75 showed that single-dose aspirin was not independently associated with a lower AI75 in the 90 minutes following exertional heat stress (p=0.152), suggesting that 2 weeks of daily low-dose aspirin is responsible for observed differences between the groups. Further subgroup analysis comparing the group that had single-dose aspirin only (PA) to the placebo only (PP) group did not show any significant association of single-dose aspirin with AI75 (p=0.167). Similarly, single-dose aspirin had no significant effect on RHI (p=0.443) based on second randomization by single-dose (325 mg) aspirin (Figure 3B), and in subgroup analysis comparing the group that received aspirin post-treatment alone to the placebo group (p=0.576).
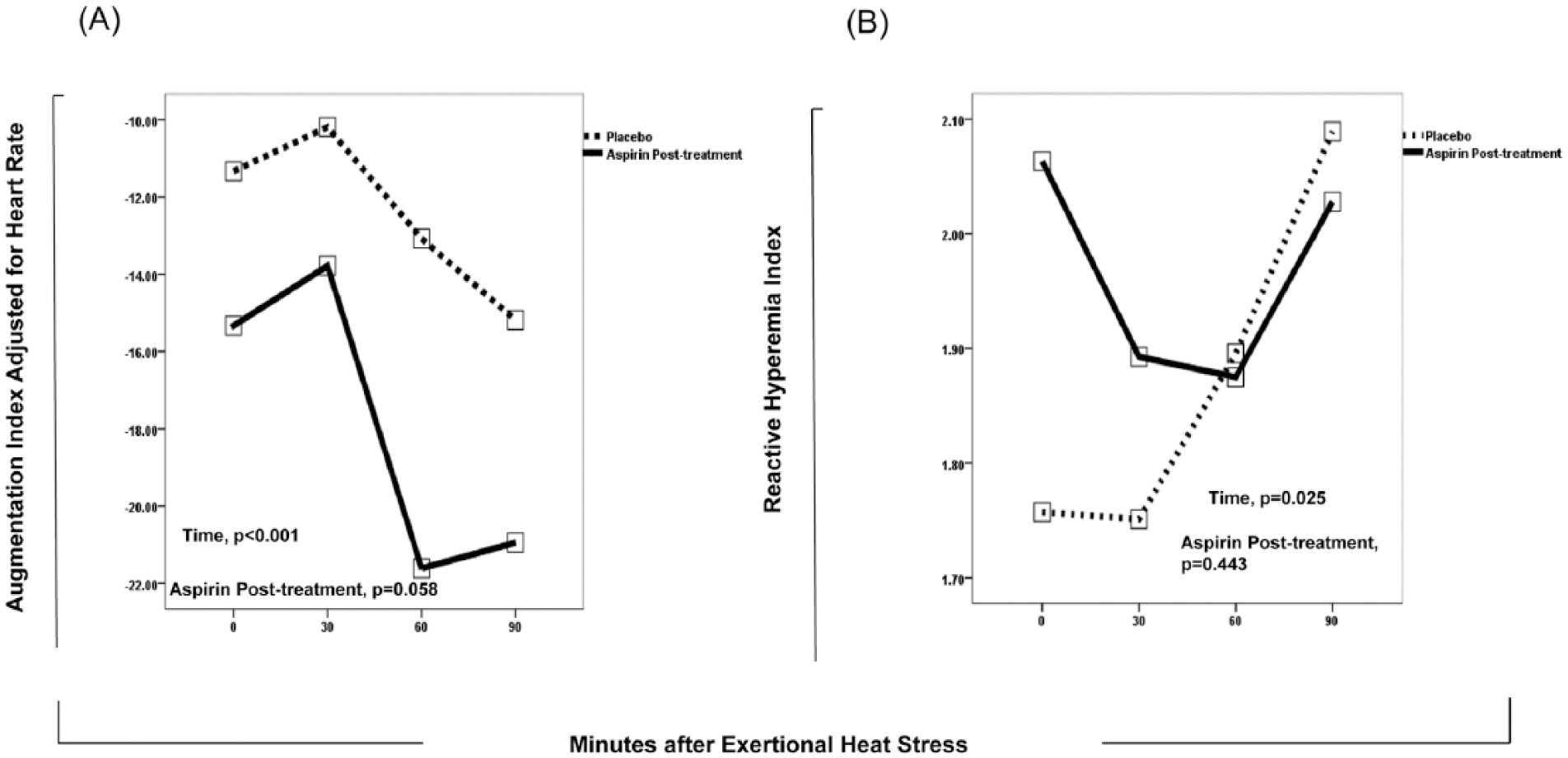
Changes in augmentation index adjusted for heart rate (A) and reactive hyperemia index (B) by time and single-dose 325 mg aspirin treatment assignment.
Discussion
To our knowledge, this is the first study to show that daily low-dose (81 mg) aspirin for 2 weeks is associated with lower peripheral arterial stiffness and wave reflection before and after exertional heat stress in firefighters. In contrast, a single high dose (325 mg) of aspirin chewed immediately after exertional heat stress had no significant effect on peripheral arterial stiffness. However, low-dose and single high-dose aspirin were not associated with significant effects on endothelial function.
There are multiple pathophysiological processes associated with exertional heat stress and firefighting that may be expected to exert vascular effects.4,5,15 Platelet activation, a rapid rise in core body temperature (approximately 1.0–1.5°C in 20 minutes), hypohydration, and maximal exertion are known to affect the cardiovascular system during fire suppression.4,5,15 Furthermore, AI and pulse wave velocity have been observed to increase with firefighting activities. 6 Increased AI, indicating enhanced arterial wave reflections and peripheral arterial stiffness, leads to increased left ventricular (LV) afterload and mechanical strain of the LV, 19 and is an early manifestation of vascular disease. 20 In a recent study, increased AI was also found to be predictive of future cardiovascular events and all-cause mortality in the general population. 8 In another study involving patients with grade I hypertension, a 2-week course of aspirin (162 mg) administration had a favorable effect on aortic stiffness and, to a lesser degree, on AI. 21 Given these observations, it stands to reason that strategies designed to improve arterial stiffness and wave reflection may be of clinical importance to firefighters. In that regard, our findings have important implications by showing that low-dose aspirin, which has generally been used to prevent the occurrence of cardiovascular events, 11 may favorably alter peripheral arterial stiffness and wave reflections in firefighters.
Although the use of digital pulse and applanation tonometry to measure arterial stiffness, wave reflection and endothelial function has grown in recent years, we are aware of only one prior study using this technique to assess the effect of firefighting on vascular function. 6 Among 69 volunteer and career firefighters, Fahs and colleagues observed increases in aortic diastolic blood pressure, heart rate, AI, pulse wave velocity and RHI, and significant decreases in brachial and aortic pulse pressure following firefighting activities. They also reported that treatment with vitamin C had no effect on these hemodynamic and vascular parameters when compared to a placebo. 6 In our study, we found that exercise in thermal protective clothing resulted in a transient non-significant increase in AI followed by a significant drop in AI at 90 minutes after exertional heat stress. Additionally, we observed a beneficial effect of daily low-dose aspirin on peripheral arterial stiffness, but not on endothelial function, before and after exertional heat stress. Differences between our results and findings from Fahs et al. 6 may be related to differences in firefighting activity protocol and timing of arterial stiffness assessment rather than the technique itself. While arterial stiffness indices were determined by Fahs et al. using a SphygmoCor device within 30 minutes of firefighting activity, we performed serial arterial stiffness measurements up to 90 minutes after exertional heat stress using the EndoPAT device. Although a prior study has shown a strong correlation between SphygmoCor- and EndoPAT-derived arterial stiffness indices, 22 differences in the duration of study protocol and timing of arterial stiffness assessment after firefighting activity and exertional heat stress may provide an explanation for differences in the results of these two studies. Specifically, our study protocol was longer than that of Fahs et al. 6
Although the mechanism of arterial stiffness improvement with daily low-dose aspirin is not completely understood, it is possible that aspirin exerts an effect on arterial stiffness via its anti-platelet and anti-inflammatory action which decreases arterial tone.23,24 It has been suggested that low-dose aspirin preferentially inhibits biosynthesis of potent vasoconstrictors, thromboxane A2. 23 This observation may partly explain the beneficial effect of 2 weeks of low-dose aspirin over a single high-dose of aspirin on peripheral arterial stiffness in the present study. However, lack of improvement in endothelial function by low-dose aspirin remains unclear. This may suggest that peripheral arterial stiffness and endothelial dysfunction represent different aspects of vascular disease.
Our study has some limitations. Although our subjects performed exercise in thermal-protected clothing to mimic firefighting drills, this is not completely the same with firefighting activities, and most importantly lacks the mental stress and exposure to smoke and toxicants involved with firefighting. Additionally, subjects in this study were well hydrated prior to exertion which may not typically be the case for most firefighters reporting for duty. 25 It is unclear how the interaction between mental stress, inhalation of toxicants, heat stress, exertion, and hypohydration might affect our findings. Furthermore, our study was designed to assess vascular function during a single bout of exertional heat stress and the immediate recovery period (up to 90 minutes). Other situations, such as multiple bouts of heat stress, were not studied. Although we did not directly evaluate endothelial function by measuring responses to an infusion of an endothelium-independent vasodilator in the forearm, prior studies have validated the EndoPAT-derived RHI as a measure of peripheral and coronary endothelial dysfunction.16,17 Finally, the minimum dose of aspirin required before and/or after exertional heat stress to lower peripheral arterial stiffness, wave reflection and improve endothelial function was not studied. These questions may warrant further investigations.
In conclusion, our study shows that pre-treatment with daily low-dose aspirin for 14 days has a beneficial effect on peripheral arterial stiffness and wave reflection but not on endothelial function before and 90 minutes after exertional heat stress in healthy firefighters. Additional clinical studies are required to determine the dose and timing of aspirin to optimize the risk to benefit ratio among firefighters. Large-scale clinical trials are needed to determine whether chronic aspirin may reduce long-term cardiovascular risk in firefighters.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
Funding for this study was provided by the Federal Emergency Management Agency, Assistance to Firefighters Grants Program, Fire Prevention & Safety (EMW-2008-FP-01638) and the National Institutes of Health (Grant Number UL1-TR-000005 and 5K12HL109068-04).