
Abstract
Postpartum reversible cerebral vasoconstriction syndrome (PPRCVS) is a rare but serious cause of headache that occurs in the early postpartum period. The rarity of this disorder has limited the current literature to single case reports and small, observational case series. The lack of familiarity with PPRCVS may contribute to mismanagement of these unique patients and lead to poor outcomes. To address current gaps in the understanding of PPRCVS, this review and data analysis characterizes the demographics, presentation, clinical course, management and prognosis of PPRCVS and provides a general review of the epidemiology, pathophysiology and diagnosis to assist clinicians who may care for patients with this rare disorder.
Introduction
Postpartum reversible cerebral vasoconstriction syndrome (PPRCVS), also known as postpartum cerebral angiopathy, is a rare but serious cause of headache, a common symptom during the puerperium in young, otherwise healthy women that is more often attributable to muscle tension or strain, dehydration, preeclampsia or sleep deprivation. 1 It is a recognized subset of reversible cerebral vasoconstriction syndrome (RCVS), a term that comprises of a group of vasculopathies which share similar clinical and angiographic features.2–6 RCVS is clinically characterized by the association of acute-onset, severe headaches, with or without additional neurologic signs and symptoms, and prolonged but reversible multifocal vasoconstriction of large and medium-sized cerebral arteries which spontaneously resolves within 3 months.2–5,7–10
A number of associated life-threatening emergencies, including intracranial hemorrhage (ICH), cerebral infarction and vasogenic brain edema, make PPRCVS clinically important. Owing to the seriousness of this disorder, it is essential for general practitioners and specialists in vascular and emergency medicine, obstetrics, neurology, neuroradiology and neurocritical care to be familiar with the clinical features, diagnosis and management of PPRCVS. The current understanding of PPRCVS is limited to single case reports and small, retrospective observational case series, and, to date, PPRCVS has been poorly characterized in the existing literature.11,12 To address current gaps in this knowledge and to assist clinicians in recognizing and managing this rare disorder, we used published PPRCVS literature to characterize PPRCVS. Since PPRCVS shares many similarities with RCVS, we also provide a general overview of RCVS.
Methods
We identified published PPRCVS literature using an electronic search strategy, supplementing this by scanning the references of retrieved articles. We searched MEDLINE, life science journals and online books using the search terms ‘reversible cerebral vasoconstriction syndrome’, ‘postpartum reversible cerebral vasoconstriction syndrome’ and ‘postpartum cerebral angiopathy’. Our search was limited to full-text articles available in English and was completed by 31 May 2014. Articles, case reports and case series of patients with proven or probable PPRCVS were eligible for inclusion. A total of 98 unique PPRCVS cases were identified.
Two reviewers independently extracted pre-specified data from all articles that fulfilled the eligibility criteria. Data extracted included patient age and symptoms at presentation, days from delivery to symptom onset, medication history, laboratory and imaging findings, management and outcomes. If pre-specified patient and clinical data were not reported in the original article, data points were recorded as ‘not reported’. If duplicate PPRCVS cases were identified across separate publications, data points were combined to ensure unique patients were only counted once. One patient was reported to have had a recurrent episode of PPRCVS, and for this occurrence the two episodes were counted as separate cases. Upon our review, we found a variety of ‘symptoms’ were reported across the different reports. Owing to the large variety of symptoms reported in these cases, we defined ‘symptom’ using a composite of headache, seizure, visual disturbance, hemiparesis, speech deficit, hemisensory deficit, hemiplegia, quadriplegia and coma.
Epidemiology
Although the exact incidence is unknown, RCVS is considered a rare clinical entity.2,5,8,10,11 During a 4-year period, Ducros and colleagues prospectively recruited a total of 89 patients with a diagnosis of RCVS and estimated that these 89 patients represented 0.26% of the overall patient population presenting to their institution’s stroke and emergency headache clinics (95% CI, 0.21% to 0.31%). 13 The prevalence of PPRCVS is even lower. Based on three large RCVS case series, only 7–9% of all RCVS cases occurred in the postpartum setting.4,13,14 RCVS is uncommon, and that fact that less than 10% of all RCVS cases occur during the postpartum period suggests that PPRCVS is an extremely rare disorder.
PPRCVS might be an under-recognized disorder because cerebral arterial imaging, an essential requirement for diagnosis, is not always performed in postpartum patients with headache or neurological symptoms.5,8,10,11 The increasing availability of newer, relatively non-invasive imaging techniques capable of assessing cerebral vasculature and blood flow, such as computed tomography angiography (CTA), magnetic resonance angiography (MRA) and transcranial Doppler ultrasonography, may lead to greater detection.2,3,15
Pathophysiology
The molecular pathophysiology of RCVS is not clearly understood at this time.3–5,8,14 Owing to the characteristic rapid clinical recovery and resolution of vasoconstriction often observed with RCVS, pathological evaluation has been limited. 16 The current hypothesis is that a transient disturbance of the regulation of cerebral vascular tone leads to segmental and multifocal arterial constriction and dilation.3–5,8–10,13 Alterations in cerebral vascular tone occur spontaneously or may be associated with exposure to vasoactive substances, including sympathomimetic and illicit drugs,3–5,8,9,13,14,17–20 selective serotonin-reuptake inhibitors (SSRIs),3–5,8,9,11,13,14,21–25 ergot alkaloid derivatives3–5,8,11,21,24,26–38 and catecholamine-secreting tumors.9,39,40 RCVS is also associated with exposure to immunosuppressants and blood products,4,9,41 uncontrolled hypertension, migraine, pregnancy and the puerperium,3–5,8,9 with the use of methenamine, 42 and following hysterectomy and bilateral salpingo-oophorectomy. 43 Since RCVS is comprised of a variety of syndromes sharing similar clinical and radiographic features, the underlying mechanisms may be multi-factorial. 10
Owing to the association of PPRCVS with pregnancy and the puerperium, it has been proposed that female reproductive hormones and pregnancy-related physiological changes may contribute to alterations in cerebral arterial tone.26,44 These physiological changes include a number of normal cardiovascular adaptations, such as increased blood volume and arterial stiffness, generalized vasodilation, impaired glucose tolerance, mild systemic inflammation, and decreased peripheral vascular resistance and blood pressure. 45 Akhter and colleagues assessed arterial wall health by comparing common carotid artery intima and media thickness, as well as intima-to-media ratios, throughout pregnancy versus 1 year post-delivery. Intima thickness and intima-to-media ratios 1 year after delivery were found to be decreased (improved) compared to measurements taken throughout pregnancy which remained fairly constant (p<0.001 for both). 45 These authors concluded that pregnancy-related vascular changes appeared to negatively impact arterial wall function and architecture. 45 Others have hypothesized that hormone factors causing acute elevations in blood pressure may contribute to alterations of the intima of cerebral vasculature.44,46 This theory has been supported by findings of intimal hyperplasia on autopsy of one patient with diagnosed PPRCVS. 44
Ergot alkaloid derivatives and SSRIs are commonly prescribed to reduce postpartum hemorrhage and suppress lactation. 5 We identified 98 unique PPRCVS patients in our literature review (Supplementary Table 1).2,6,11,12,16,19–22,24–38,44–84 Among those 98 patients, 32 patients were reported to have had recent exposure to at least one vasoactive substance.11,19–22,24–38,57,70 Among the 32 postpartum patients with vasoactive substance use reported, 23 had reported use of an ergot alkaloid derivative,11,21,24,26–38,57 eight had reported exposure to a SSRI,11,21,22,24,25,57 two had reported use of a sympathomimetic drug19,20 and one was reported to have taken dihydralazine. 32 Three patients were reported to have had exposure to both an ergot alkaloid derivative and a SSRI.11,21,24
Demographics
Overall, women appear to be more commonly affected by RCVS than men. In five case series, which included 16–139 patients with RCVS, female to male ratios ranged from 1.8:1 to 8.6:1.4,13,14,85,86 Onset of RCVS typically occurs during middle-age. In four of the largest RCVS case series that we know of to date, the mean age of RCVS onset ranged from 42 to 47.7 years.4,13,14,85 However, RCVS has been diagnosed in patients as young as 10 years 85 and as old as 70 years.4,13 Age of onset in women appears to occur later than in men. In a 2007 case series by Ducros and colleagues, the average age of RCVS onset in women was 46.9 years ± 11.5 years compared to 34.7 years ± 7.7 years in men (p<0.0001). 4 Similarly, Singhal et al. reported an average age of RCVS onset of 44.2 years ± 11 years in female patients versus 34.9 years ± 12 years in male patients (p<0.001). 14
Among PPRCVS patients identified in our literature search with age of PPRCVS onset reported, the age of onset ranged from 15 to 43 years, and the median age of onset was 32, with an interquartile range of [27, 36] years (Supplementary Table 1). This is younger than the mean age of onset reported in four large case series that included primarily non-postpartum RCVS patients.4,13,14,85 This observation is perhaps a reflection of the higher birth rates noted among women aged 20–34 years compared to those over 40 years of age. 87 This might also suggest that older women of childbearing age might be at an increased risk. Among PPRCVS patients with duration to symptom onset reported, the duration from delivery to symptom onset ranged from zero to 30 days, and the median duration to symptom onset was 5, with an interquartile range of [3, 8] days (Supplementary Table 1). Among patients with duration from delivery to PPRCVS onset reported, 71% had onset of symptoms occurring within 7 days of delivery, and only six patients had duration from delivery to symptom onset greater than 2 weeks (Supplementary Table 1).11,53,59,60,77,78
Most patients with PPRCVS have a history of uncomplicated pregnancy and normal labor and delivery.3,5,8,9 One literature review of 23 PPRCVS patients found that none had proteinuria. 31 However, this is in contrast to a retrospective review of 18 PPRCVS patients by Fugate et al. which found 47% of the pregnancies immediately prior to onset of PPRCVS were complicated by proteinuria and 11% were complicated by HELLP (hemolytic anemia, elevated liver enzyme, low platelet count) syndrome. 11 In this case series, preeclampsia or eclampsia was diagnosed in 39% of PPRCVS patients, and 28% of patients had preterm deliveries. 11 However, this was the only article we found in our literature search to report proteinuria in PPRCVS patients, and only two other publications reported eclampsia 57 or preeclampsia. 71 Among PPRCVS patients identified in our search, there were six patients that were reported to have proteinuria.11,57 Eclampsia and preeclampsia were each reported in one patient.57,71
Presentation
The clinical presentation of RCVS is predominantly marked by the acute onset of severe headache, often described as the thunderclap headache variety which peaks in intensity within 1 minute of onset.3–5,8,10 These headaches are commonly recurrent and associated with cerebral vasoconstriction. 3
Presentation with sudden onset of severe headache is characteristic of PPRCVS as well. In our literature review of PPRCVS patients, 95 patients had headache symptoms reported (Supplementary Table 1).
Headache due to RCVS can be associated with or without nausea, emesis, photosensitivity and focal neurological deficits, such as seizure, transient or permanent visual disturbances, speech defects, altered consciousness, hemiplegia, numbness and ataxia.2–5,11,13,14,86 In large case series, neurologic deficits have been observed in 24–43% and seizures in 3–17% of patients.4,13,14 Additionally, blood pressure elevations have been noted in one-third to 46% of RCVS patients during episodes of severe headache.4,13,85
In our literature review of PPRCVS patients, 75 had reported at least one focal deficit, which we defined as one or more of the following: seizure, visual disturbance, hemiparesis, speech deficit, hemisensory deficit, hemiplegia, quadriplegia and coma (Supplementary Table 1). Forty-three patients had one or more episodes of seizure reported, 33 had visual disturbances reported, 29 had hemiparesis reported and 13 had speech deficits reported. Three PPRCVS patients were reported to be quadriplegic upon presentation,29,71,79 and five were reported to be comatose.29,57,68,71,79 Elevated blood pressure was reported in 48 PPRCVS patients (Supplementary Table 1).
Physical examination and laboratory analyses
General physical examination is usually normal except when RCVS is associated with posterior reversible encephalopathy syndrome (PRES) in the setting of eclampsia, septic shock or other complex coexisting conditions.5,8,9 Laboratory analyses, including complete blood count, erythrocyte sedimentation rate (ESR), serum electrolytes, and renal and liver function tests are usually normal, and tests for rheumatoid factor, Lyme disease and antinuclear and antineutrophil cytoplasmic antibodies are generally negative.2,8,9 Cerebral spinal fluid testing may reveal slight abnormalities.4,9
Thirty-four PPRCVS patients identified in our literature review had abnormal laboratory findings reported (Supplementary Table 1). Notable findings reported in PPRCVS patients included mild elevations in C-reactive protein (CRP),25,57,65,73,79 mild non-specific cerebrospinal fluid (CSF) abnormalities,22,47,49,65,73 increased ESR,26,65,66,75,79 elevated urine protein,32,62,73 positive antinuclear antibodies62,65 and increased international normalized ratio. 57
Diagnostic criteria
Criteria for the diagnosis of RCVS have been adapted from the 2004 International Headache Society diagnosis criteria for ‘acute reversible cerebral angiopathy’ and from the criteria proposed in 2007 by Calabrese and colleagues.3,7,8 Although the diagnostic criteria have not been prospectively validated, experts have deemed the criteria to have considerable sensitivity and specificity in the appropriate clinical setting. 3 The proposed criteria are listed in Table 1. A definitive diagnosis can only be made after other causes of severe headache have been ruled out and serial angiography or transcranial Doppler ultrasonography demonstrate complete resolution or marked improvement of arterial vasoconstriction abnormalities.3,4,7–9 The proposed cutoff duration for which complete or at least substantial resolution of vasoconstriction should be demonstrated is 12 weeks. 9 Figure 1 demonstrates vasoconstriction and resolution of the middle cerebral arteries observed in a postpartum patient who presented to our institution.
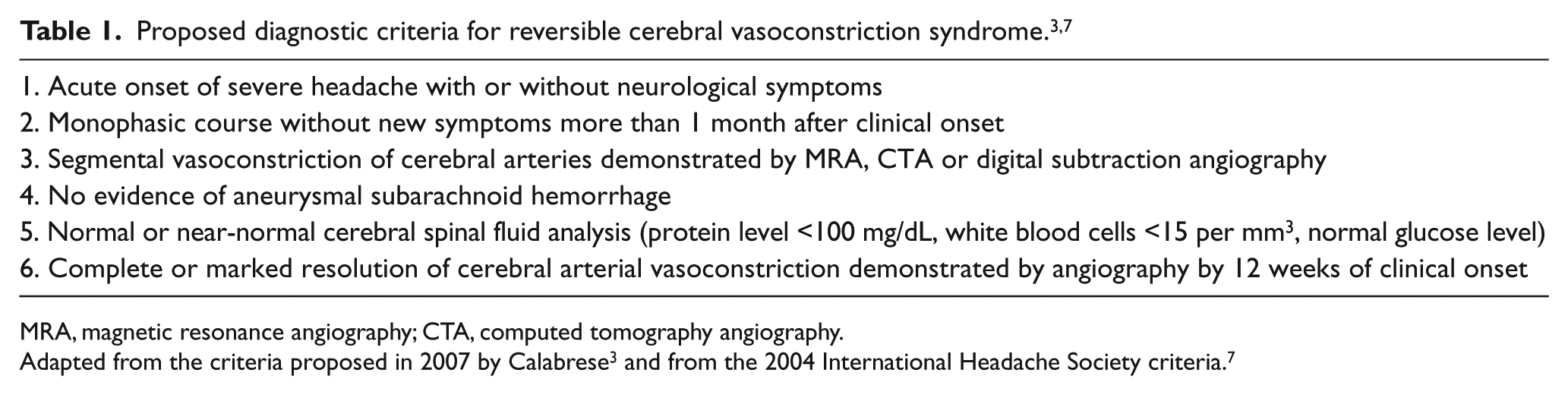
MRA, magnetic resonance angiography; CTA, computed tomography angiography.
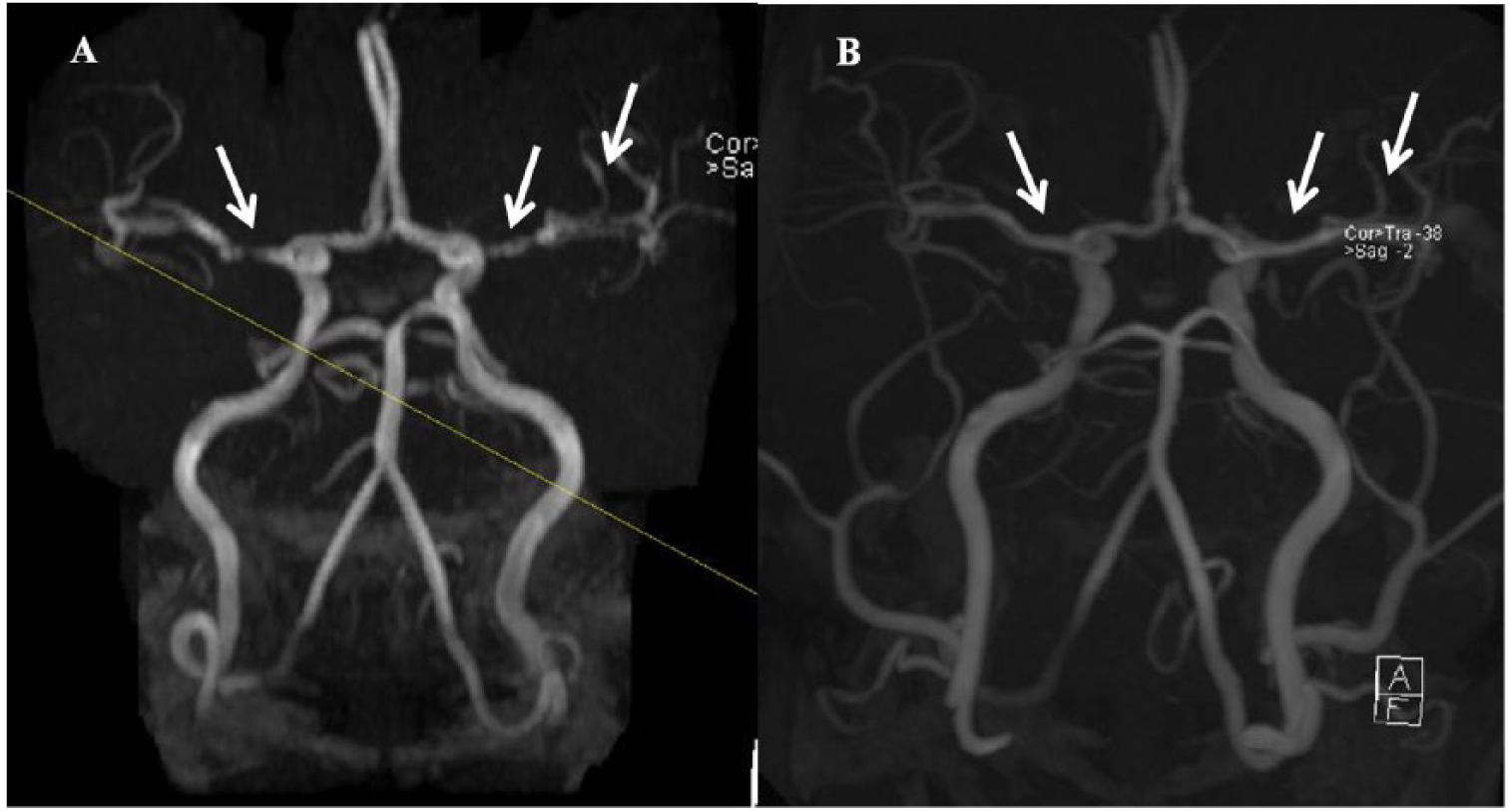
Vasoconstriction and resolution of the middle cerebral arteries on a head and neck MRA. (A) Angiographic images generated using the time-of-flight technique show segmental beading of the middle cerebral arteries bilaterally – left worse than right (white arrows). (B) A follow-up study 18 days later shows resolution of the findings.
Diagnosis
A thorough history, physical examination and, if indicated, appropriate cerebrovascular imaging studies are helpful to differentiate RCVS or PPRCVS from other possible cerebrovascular disorders that may have a similar presentation.3,10
While patients with mild postpartum headache can be managed conservatively without further testing, appropriate testing should only be ordered based on the suspicion of a specific disorder. The initial evaluation of patients presenting with severe intractable headache with alarming symptoms like neurological deficits should include an emergent, non-contrast brain CT to rule out subarachnoid hemorrhage (SAH), intraventricular and parenchymal brain hemorrhage, intracerebral and subdural hematoma, hydrocephalus and tumors.3,5,8,10 Negative CT scans should be followed by a lumbar puncture as CSF analysis may help rule out SAH and differentiate RCVS from central nervous system inflammatory conditions such as infection and cerebral vasculitis.3,10
In cases with severe, continuous and unexplained headache, normal CT scans and benign CSF exams should be followed by additional brain and neurovascular imaging with CTA, MRA or MR venography to assess other etiologies of severe headache.3,10
Brain MRI is frequently normal in patients with RCVS, but these imaging studies can reveal evidence of infarction, changes consistent with PRES, parenchymal brain hemorrhage and small, non-aneurysmal cortical SAH.3,22,88
Checking inflammatory markers and autoimmune serology, including rheumatoid factor, antinuclear and antineutrophil cytoplasmic antibody, should be considered if vasculitis is suspected.2,8,9 Normal ESR and CRP may help rule out giant cell arteritis, and a normal electrocardiogram study can rule out cardiac cephalagia due to myocardial ischemia, both of which are very rare causes of thunderclap headache. 8 If suspected, evaluation for potential vasoactive drug and medication use can be done with serum and urine toxicology screens, and urinary concentrations of vanillylmandelic acid and 5-hydroxyindoleacetic acid should be measured to rule out pheochromocytoma.2,8,9
Early angiographic studies of the brain and cerebral blood vessels may be normal in patients with RCVS, and vasoconstriction may only be observed on repeat testing.3,5,8,11 Among the 18 PPRCVS patients in the case series by Fugate and colleagues, seven (39%) had normal initial cerebral vessel imaging. 11 Of these 18 patients, 17 had non-invasive imaging and one had conventional digital subtraction imaging. 11 In addition, maximal mean flow velocities in the middle cerebral arteries on transcranial Doppler ultrasonography may be normal during the first few days and then begin to increase, reaching a peak up to 3 weeks after headache onset.4,8 Serial angiography with CTA, MRA or transcranial Doppler may be indicated in cases with recurrent alarming symptoms such as intractable headache and/or neurological deficit if initial angiography studies had been normal. However, to the best of our knowledge, there are no data to support repeat imaging studies over the long term as most of these cases have transient imaging abnormalities.
Vasoconstriction involving distal cerebral branches may not be adequately observed on CTA or MRA, and imaging with invasive catheter-based digital subtraction angiography may be necessary. Although invasive catheter-based digital subtraction angiography is considered the gold standard for the diagnosis of cerebrovascular disease and is indicated in patients who present with ICH, 15 this invasive approach is not feasible in patients requiring frequent follow ups and may expose patients to additional risks. 10 Figure 2 demonstrates middle cerebral artery vasoconstriction and dilation on catheter-based digital subtraction angiography.
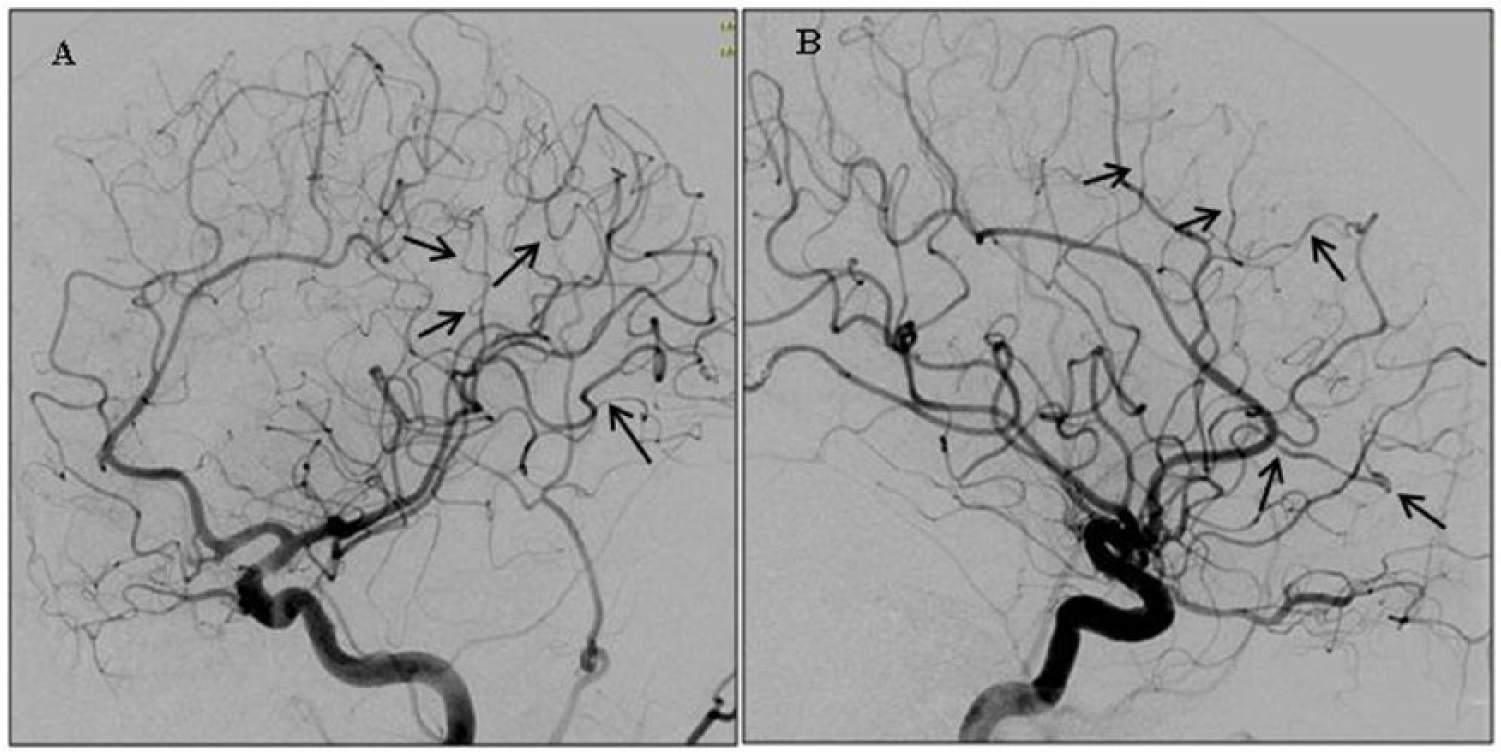
Cerebral vasoconstriction and dilation on a digital subtraction angiogram. (A) Left internal carotid artery injection showing segmental narrowing and dilatation of distal middle cerebral artery branches (beaded appearance delineated by the arrows); oblique view. (B) Lateral view of the same.
Differential diagnoses for postpartum headache
In the first week after delivery, nearly 40% of women experience postpartum headaches.75,89,90 More than three-fourths of postpartum headaches are primary headache disorders of the migraine or tension-type variety. 75 We recommend avoiding unnecessary workup in the absence of alarming symptoms like neurological deficit. However, postpartum headaches can be secondary to numerous other etiologies that share similar clinical and imaging features with RCVS. Differential diagnoses include postdural puncture headache, ischemic or hemorrhagic stroke, carotid or vertebral artery dissection, aneurysmal SAH, parenchymal brain hemorrhage, unruptured saccular aneurysm, cerebral venous sinus thrombosis, meningitis, encephalitis, pituitary apoplexy, tumor (third ventricle colloid cyst), preeclampsia or eclampsia, PRES, spontaneous intracranial hypotension and cerebral vasculitis, especially the variant primary angiitis of the central nervous system (PACNS).3,5,8,9,75
The workup process for postpartum headache can be very challenging as many of these patients have benign conditions including migraine, hormonal imbalance, and epidural anesthesia-related headaches that do not require further workup. We recommend thorough medical history to cover symptom details, medications and procedures like epidural anesthesia, along with a full physical exam to help make a decision on the appropriate next management step that might involve any of the diagnosis modalities described earlier. Thunderclap headache might indicate PPRCVS, postural headache in the sitting up position might indicate an epidural anesthe-siainduced CSF leak, and severe constant headache might indicate cerebral sinus vein thrombosis.
Differential diagnoses for postpartum vascular stenosis
The finding of multiple segmental narrowing of the cerebral arteries with cerebral angiography is often non-specific. Possible etiologies include RCVS, intracranial atherosclerotic disease, cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) and cerebral vasculitis. 91 In one retrospective study of patients undergoing cerebral angiography followed by cortical and leptomeningeal biopsy for possible PACNS, Kadkhodayan and colleagues found none of the 14 patients with typical angiographic findings of cerebral vasculitis had PACNS at brain biopsy. 91 Differentiating RCVS from PACNS is clinically important in order to avoid the risks of intense, prolonged immunosuppressive therapy and brain biopsy.3,5,8,14 Patients with RCVS generally have: (1) acute onset of severe, recurrent headache followed by a monophasic course without any new complications after 4 weeks; (2) a recent history of childbirth or exposure to vasoactive substances; (3) normal or near-normal CSF unless there is an associated non-aneurysmal SAH; (4) normal brain parenchyma on CT or MRI, although some patients show symmetric arterial infarction, parenchymal brain hemorrhage, small cortical SAH or reversible brain edema; and (5) prompt reversibility of vasoconstriction.3–5
With PACNS, there is typically a chronic or more gradual onset of dull headache. Additionally, CSF abnormalities are present in 95% of patients and intracranial blood vessel abnormalities are frequently irreversible.3,5 Additionally, catheter-based digital subtraction angiography is frequently normal with PACNS, while it is by definition always abnormal with RCVS.5,8 Conversely, MR imaging is often normal in RCVS (up to 70% of cases) but is abnormal in most cases of PACNS (up to 90% of cases).3,5,8,92 In patients with persisting diagnostic uncertainty or severe clinical deterioration, a brain-leptomeningeal biopsy may be an acceptable approach to rule out cerebral vasculitis. 93
Complications
Early complications associated with RCVS are listed in Table 2. Earlier RCVS case series have reported brain infarcts in 3–39%,4,11,13,14 brain edema in 35–38%,11,14 ICH in 34–39%,11,13 SAH in 22–34%4,13,14 and PRES in 7–17% of patients.4,13,11 Cervicocephalic artery dissection has rarely been described in patients with RCVS.4,24 In rare cases, death has also been reported.11,44,57,75,81,94
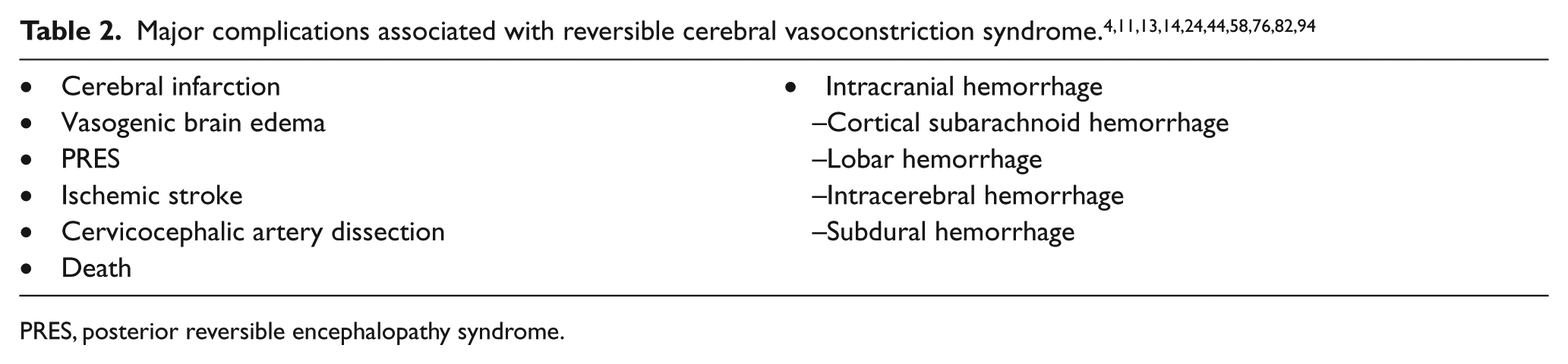
PRES, posterior reversible encephalopathy syndrome.
Among the PPRCVS patients identified in our literature review (Supplementary Table 1), 38 patients had an ICH reported, of which 23 had a SAH reported. There were 32 PPRCVS patients with brain ischemia or infarction reported, 19 with PRES reported, and 22 with brain edema reported. Cervicocephalic artery dissection coexisting with PPRCVS was reported in 11 patients in our literature review. Although RCVS and PPRCVS are extremely rare etiologies for cervicocephalic dissection, they should be considered as possible differential diagnoses, especially in patients with a suggestive history and clinical presentation.
Management
To the best of our knowledge, no clinical trials of any treatment for RCVS have been conducted, and thus, management is guided by observational data and expert opinion.3,8,9 All patients should be advised to rest and to avoid possible triggers of severe headache.5,8,9 Owing to the self-limiting nature of RCVS, simple observation alone is reasonable in patients who show no signs of clinical progression.2,23,86 However, patients should be monitored closely as it is not uncommon for symptoms to clear but then return days later and culminate in a stroke.3,86,95,96 Patients with visible vasoconstriction, and patients who have consistent clinical and brain imaging features, no evidence for another cause of symptoms and normal initial cerebral angiograms, should receive symptomatic treatment. 9 Symptomatic treatment should include the avoidance of vasoconstrictive substances, headache relief, blood pressure control and treatment of associated conditions, including stroke, seizure and cerebral edema.8,93
Calcium-channel blockers and magnesium sulfate have been reported to alleviate vascular abnormalities.3,8,22,86,88,95 Treatment with analgesics, antiepileptic drugs for seizures, close blood pressure monitoring and intensive care unit admission in severe cases are recommended. 9 Immunosuppression agents such as steroids should only be administered in patients with brain-leptomeningeal vasculitis confirmed on brain biopsy or given while awaiting brain biopsy results.5,93 Long-term treatment should include secondary stroke prevention and the treatment of any complications. 93
In our review of the literature, antihypertensive therapy with calcium-channel blockers, corticosteroids and magnesium sulfate were commonly reported (Supplementary Table 1). Balloon-angioplasty was reported in five severe cases; however, four of these patients died.11,57,76 There is no evidence to support the use of antiplatelet agents for uncomplicated cases of RCVS or PPRCVS. Owing to the risk of bleeding in these patients, we recommend considering antiplatelet agents only in concurrent dissection and/or thromboembolic stroke.
Prognosis
Typically, RCVS has a self-limiting course with no new onset after 1 month, and many patients diagnosed with RCVS demonstrate full recovery with few if any sequelae.3,4,14 Patients with a stroke or ICH appear more likely to experience residual deficits than those who do not.4,13 In an earlier case series of 67 RCVS patients, each of the four patients with persistent neurological deficits at first follow-up visit had suffered a stroke during hospital admission. 4 When this group was expanded to 89 patients, the 30 RCVS patients with coexisting ICH were noted to have a greater risk of persistent focal deficits (30% vs 2%; p=0.0002), cerebral infarction (13% vs 2%; p=0.039), and PRES (17% vs 3%; p=0.041), and were more likely to have the inability to resume normal activities at 6 months (27% vs 0%; p<0.0001) compared to the 59 RCVS patients without an ICH. 13 Disease recurrence has also been observed, 80 but with a paucity of long-term follow-up studies the rate is unknown. 8
In our literature review of PPRCVS cases (Supplementary Table 1), 65 patients were reported to have improved with resolution of symptoms, and two patients were reported to have been readmitted but later improved.19,47 There were five PPRCVS patients reported to have hemiparesis,11,32,69,79 four reported to have visual deficits,11,69,71 two reported to have hyperreflexia,59,69 one reported to have mild speech deficits, 26 and one reported to be in a rehabilitation facility with significant memory difficulties. 71 There were seven deaths reported in our review of the literature.11,44,57,75,81 To the best of our knowledge, there is no evidence to discourage repeat pregnancy for PPRCVS survivors. Given the rarity of PPRCVS and low likelihood of recurrence, we do not feel there is sufficient evidence to discourage PPRCVS survivors from future pregnancy.
Limitations
Our literature search was limited to ‘reversible cerebral vasoconstriction syndrome’, ‘postpartum reversible cerebral vasoconstriction syndrome’ and ‘postpartum cerebral angiopathy’, and only included full-text articles available in English and was completed by 31 May 2014. The search did not include eclampsia cases with cerebrovascular vasospasm.
Conclusion
PPRCVS is a rare vascular pathology that affects women during the early postpartum period. The majority of women with PPRCVS present with severe headache, with onset typically within 1 week of delivery. Focal deficits, including seizure, visual disturbances and hemiparesis are common. Making this diagnosis and choosing the appropriate workup can be very challenging since there are many benign and serious conditions that can mimic PPRCVS. Management of PPRCVS is based on symptom severity and possible concurrent complications. Although prognosis is generally favorable with few sequelae, PPRCVS has been reported with ICH, stroke, and, in rare cases, death. We recommend that postpartum women presenting with the sudden onset of severe headache receive evaluation for PPRCVS.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.