
Abstract

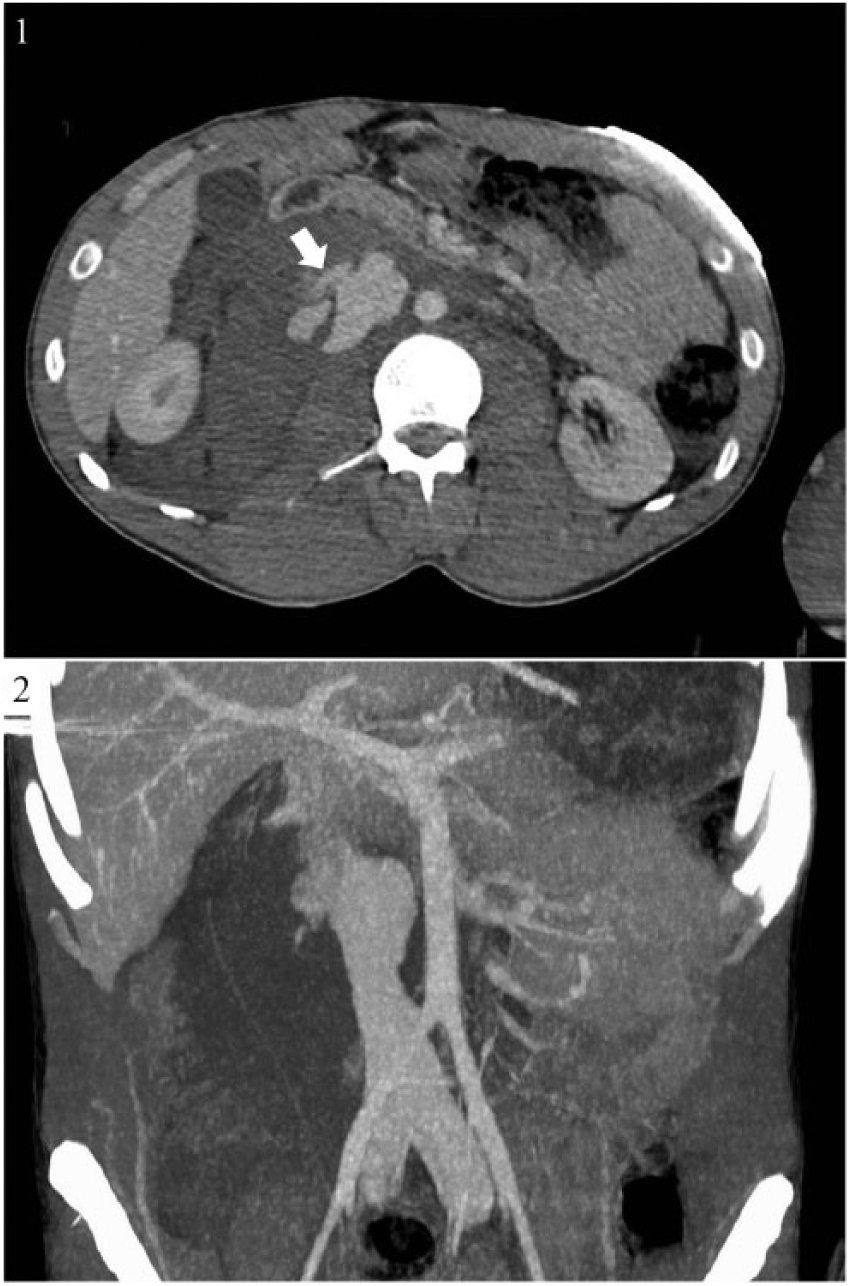
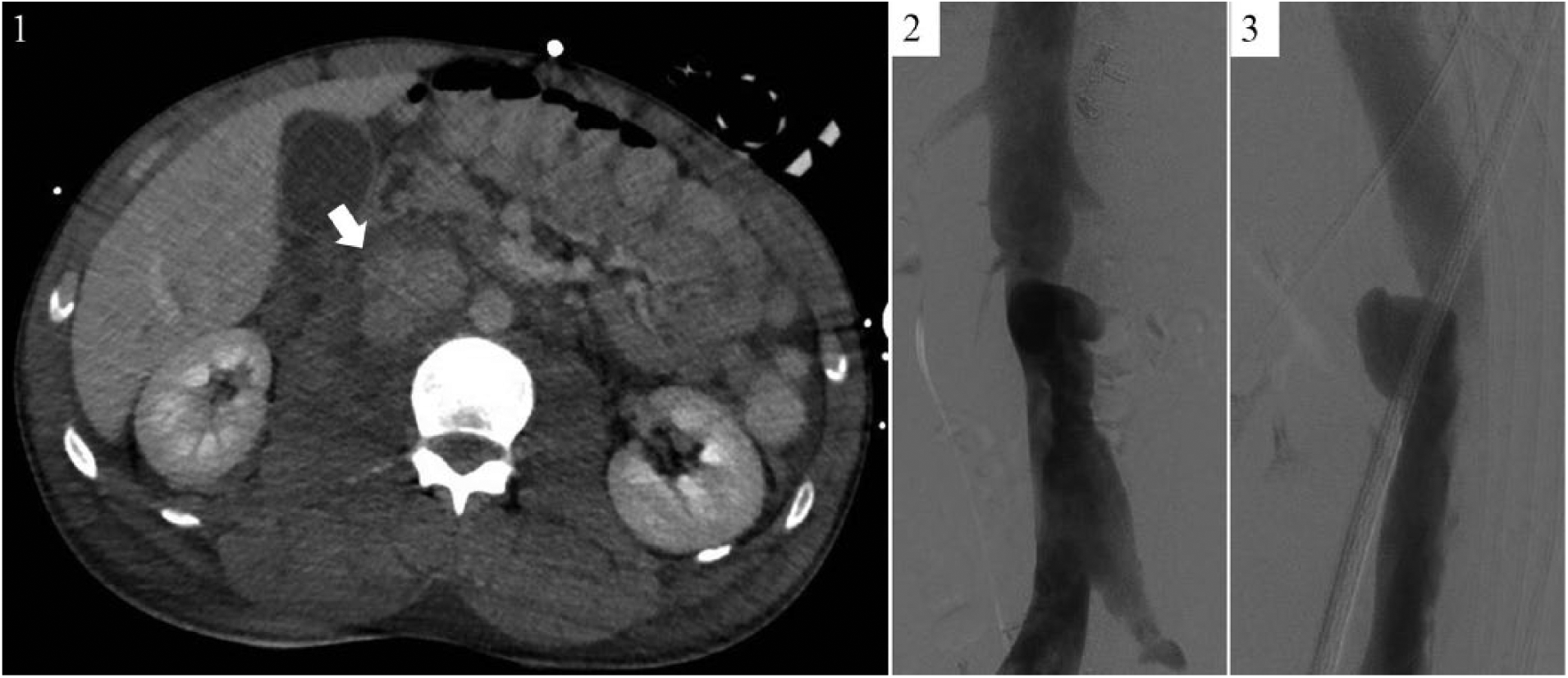
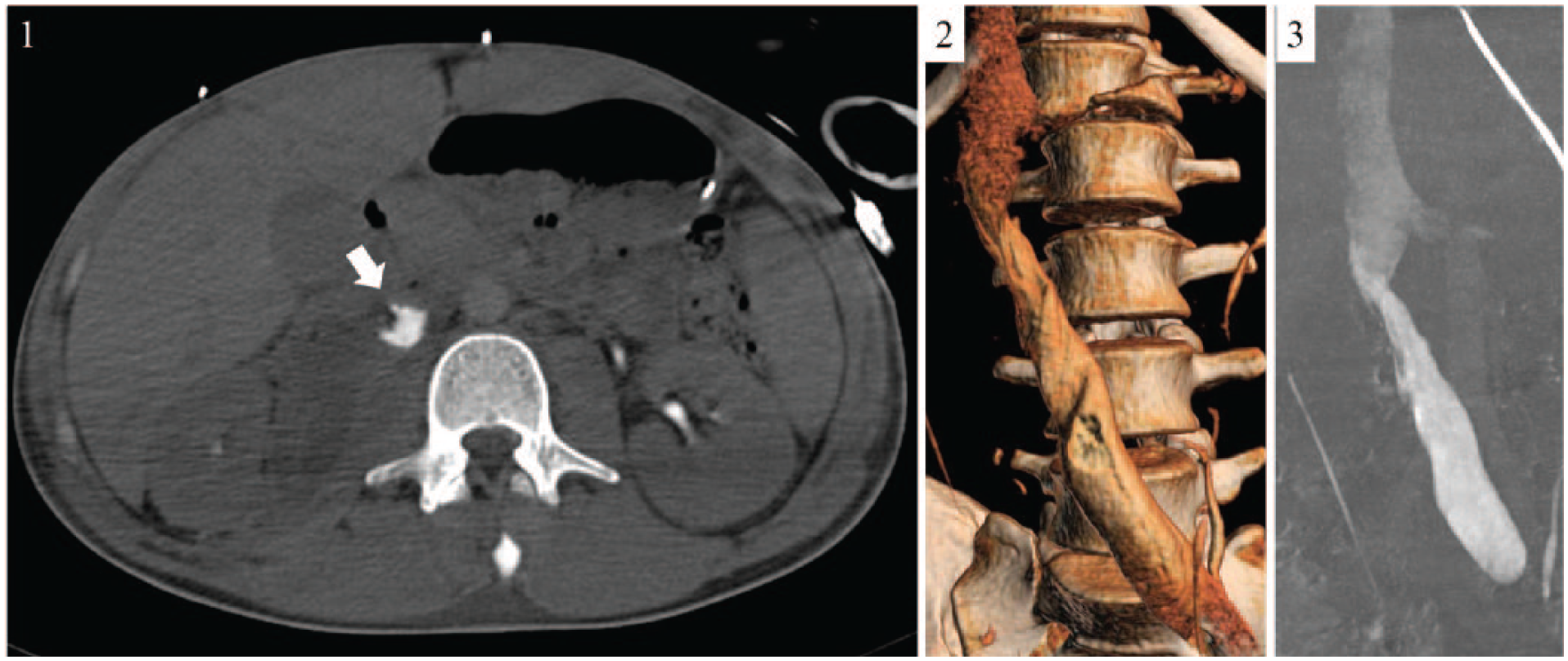
A 23-year-old male was struck by a truck whilst riding his bicycle. He was intubated at the scene, where his blood pressure was borderline stable (90/50 mmHg) and transiently responded to fluid resuscitation. A total body computed tomography angiogram (CTA) showed a small laceration (arrow) of the infra-renal inferior vena cava (IVC), with a large pericaval hematoma and compression of the lumen (Panel A1). Maximum intensity projection (MIP) displayed contrast outside the IVC with dilation of caudal venal districts and low enhancement of the cranial segment (Panel A2). Hemodynamics remained stable with massive transfusions after resuscitation; the patient was admitted into the intensive care unit. Three days later, CTA showed persistent but decreased contrast effusion (arrow) outside the cava (Panel B1) and cavography illustrated a pericaval pseudoaneurysm (Panel B2–3). Hemodynamic parameters remained sufficiently stable (95/60 mmHg). Two weeks after the injury, a new CTA scan documented the disappearance (arrow) of the pericaval pseudoaneurysm and reabsorption of the hematoma (Panel C1–3: axial slice, tridimensional reconstruction, maximum intensity projection, respectively) (See video for a timeline of the imaging follow-up and patient’s clinical evolution).
IVC injuries are a rare and potentially life-threatening event with a 50% mortality rate upon hospital arrival. 1 Blunt trauma is an infrequent cause of IVC lesions (0-16%) 2 with high in-hospital mortality (70%). 3 Peri/infra-renal segments are rarely involved. 3 Initial volume repletion and aggressive resuscitation are first-line treatment. In stable patients, CTA is the gold standard imaging modality to assess hematoma location and size as well as vena cava contour. 4 In cases of hemodynamic instability, open surgery is the treatment of choice, while endovascular treatment is reported to control venous bleeding from inaccessible segments (retrohepatic IVC). 5 Clinical observation and monitoring is a reasonable approach in patients who are hemodynamically stable. 6 Close follow-up with appropriate imaging is mandatory and multiple CTAs are usually performed. Spontaneous self-tamponade after IVC injury is reported in 50% 1 of the cases.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.