
Abstract
To analyze the necessity of venous thromboembolism (VTE) prophylaxis for patients undergoing high ligation and stripping of the great saphenous vein (GSV) and to estimate the efficacy and safety of different anticoagulant protocols in a single-center randomized controlled trial with large sample size. A total of 2196 patients undergoing high ligation and stripping of the GSV were randomized to one of the following postoperative VTE prophylaxis protocols: group A, no VTE prophylaxis (n=542); group B, subcutaneous low-dose unfractionated heparin (LDUH) hypodermic injection, 125 U/kg per day in three divided doses (n=531); group C, low-molecular-weight heparin (LMWH) 6000 IU once a day (n=573); and group D, LMWH 4000 IU twice daily (n=550). Groups were compared for the incidence of VTE and major hemorrhage within 1 month following surgery. Varicose vein severity was classified by CEAP (Clinical, Etiologic, Anatomic, Pathophysiologic elements) score. The clinical characteristics of the patients were equally matched between groups. Postoperative deep vein thrombosis (DVT) and pulmonary embolism (PE) were significantly higher in group A (DVT 5.17%, PE 1.48%) compared to groups B (0.56%, 0%), C (0.35%, 0%) and D (0.36%, 0%) (p<0.01). The incidence of VTE did not differ between the three active chemoprophylaxis arms. Hemorrhagic complications were low for each group but higher in group B (0.75%) compared to the other groups (group A 0.18%; group C 0.17%; group D 0.18%, p<0.01). Hemorrhagic complications did not differ amongst groups A, C and D. In conclusion, postoperative VTE chemoprophylaxis following high ligation and GSV stripping effectively reduces the venous thrombosis complications of this procedure. Of the three active strategies tested, no difference in efficacy was noted; however, thrice daily LDUH did increase bleeding complications.
Introduction
Varicose veins are a common cause of lower extremity pain and swelling with a negative impact on the cosmetic appearance of legs. 1 Progressive varicose veins may lead to pruritis, dander, increasing pigmentation, dermal thickening and ultimately venous ulceration. 2 Although mild varicose veins can be controlled with compression stockings or sclerotherapy, severe varicose veins may require surgical stripping. 3
Traditional varicose vein interventions used worldwide include surgical high ligation and great saphenous vein (GSV) stripping, combined with stab avulsion of related varicosities. More recently, endovenous laser ablation (EVLA), transilluminated powered phlebectomy (TIPP), and subfascial endoscopic perforator vein surgery (SEPS) are commonly pursued. 4 Although these new technologies are increasingly used, venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), remain a serious and potentially life-threatening complication.5,6 Although many surgeons provide VTE prophylaxis for patients undergoing surgery, the need for postoperative VTE prophylaxis is neither widely endorsed nor adopted. The reasons for this omission are manyfold and include perceived low incidence of thrombotic complications and concerns for major bleeding. Arguments for anticoagulation are focused on the aspects of necessity, safety, therapeutic regimen and dosage. 6
In keeping with Virchow’s theory (venous stasis, hypercoagulability, and venous intimal lesions), one might anticipate that varicose vein-related procedures may carry an increased thrombotic risk. Indeed, current guidelines recommend risk stratification with appropriate delivery of VTE prophylaxis in high-risk patients.7,8 Neither the incidence of postoperative VTE following varicose vein surgery nor the appropriate chemoprophylaxis strategy have been adequately established in large patient population studies. To address these limitations, patients referred for varicose vein surgery were randomized to receive one of four VTE prophylaxis strategies. The incidence of VTE in patients with and without chemoprophylaxis was defined. The efficacy and safety of three active chemoprophylactic strategies were compared. To our knowledge, few studies have adequately assessed these strategies in a large sample of patients undergoing high ligation and GSV stripping. 6
Methods
Patients
Patients with varicose veins referred to the Vascular Surgery Department of The 2nd Affiliated Hospital of Harbin Medical University of China for high ligation and GSV stripping (between 1 November 2002 and 31 October 2012) were approached for study participation. Patients were eligible for enrollment if they had isolated varicose veins of the lower extremity requiring conventional surgery (high ligation and stripping of the GSV, and removal of superficial varicosities).
Patients were excluded from participation if any of the following criteria were met: prior varicose vein procedure (i.e. surgical stripping, endovenous ablation, sclerotherapy); prior VTE; leg trauma within 2 years; congenital venous malformations (i.e. Klippel–Trenaunay syndrome); autoimmune diseases (i.e. systemic lupus erythematosus, rheumatoid arthritis, antiphospholipid syndrome); stenosis or occlusion of the inferior vena cava; anticoagulant, antiplatelet, or hormonal therapy; cancers; or nephrotic syndrome.
The study protocol firmly conformed to the guidelines of the Declaration of Helsinki and the Ethics Board of Harbin Medical University, Heilongjiang, China. Written informed consents were obtained from each patient prior to random assignment.
Preoperative examination
A complete lower extremity duplex ultrasound of both superficial and deep veins was performed on all patients prior to surgery. The inferior vena cava and iliac veins were formally imaged as part of this evaluation. Abnormal reflux was also evaluated by ultrasound in both supine and standing positions. The degree of deep veins reflux was measured using the Kistner classification. 9 CEAP classification (Clinical, Etiologic, Anatomic, Pathophysiologic elements) was used to evaluate the extent of varicose veins. 10
Hemostatic screening assays including prothrombin time (PT), activated partial thromboplastin time (APTT), thrombin time (TT), fibrinogen (Fbg) and D-dimer, and chemistry group were obtained on all patients prior to surgery.
Surgery for varicose veins
Under general or epidural anesthesia, conventional surgery involved high ligation, and stripping of the GSV from the ankle to a level of 0.5 cm distal to the saphenofemoral junction (SFJ). Stab avulsion of associated superficial varicosities was also performed, limiting the number of incisions where possible. Hemostasis was carefully addressed while minimizing undue stretch injury of the SFJ. After surgery, compression bandaging was placed from foot to groin. After 2 days, this was replaced by compression stockings. All patients were encouraged to ambulate as soon as possible postoperatively. Ambulation for a minimum of 4 hours per day was encouraged post hospital dismissal.
VTE prophylaxis and grouping
Patients were randomly assigned to one of four groups for venous prophylaxis. These groups included: no VTE prophylaxis (group A, n=542); low-dose unfractionated heparin (LDUH), 125 U/kg per day divided into thrice daily subcutaneous injections (group B, n=531); enoxaparin sodium (Sanofi-Aventis, USA) 6000 IU once daily (group C, n=573); and enoxaparin 4000 IU twice a day (group D, n=550). For those patients allocated active chemoprophylaxis, treatment was delivered for 3 days postoperatively. For patients receiving neuraxial anesthesia, the first injection was given over 6 hours after surgery.
VTE identification and treatment
The primary efficacy outcome was prevention of VTE (DVT and PE) occurring within the first 30 days postoperatively. Ultrasound DVT screening was performed for all the patients at weeks 1, 2, and 4 after surgery. Patients with DVT or/and PE received 3–6 months of anticoagulant therapy, including LMWH 100 IU/kg twice per day for 14 days, followed by vitamin K antagonist (VKA) with a target of international normalized ratio (INR) range 2.0~3.0, without inferior vena cava filter. Patients found to have a DVT also underwent a computed tomography pulmonary angiography (CTPA) scan for PE detection.
The primary safety outcome was postoperative bleeding occurring within the first month postoperatively. With any evidence of hemorrhage, anticoagulation therapy was discontinued. This included any evidence of continuous incision bleeding, extensive ecchymosis (over half of the whole leg), or spinal hematoma.
All events were adjudicated by a central committee consisting of all departmental personnel.
Statistical analysis
Analysis of variance (ANOVA) and least significant difference (LSD) tests, and chi-squared tests were appropriately used to compare the differences between the groups. The analysis was conducted with SPSS 18.0 software (SPSS Inc., Chicago, IL, USA). Two-tailed p<0.05 were considered significant.
Results
In total, 3182 varicose veins (VV) patients were evaluated for study participation. Of these, 730 patients were excluded according to the exclusion criteria. Eventually 2196 VV patients (mean age, 47.62±10.37 (mean±SD) years; range, 23–68 years) were assigned to one of four VTE prophylaxis strategies. Groups were equally matched for age, sex, limb involvement, CEAP scores, and Kistner classification (Table 1). According to CEAP classification, C3 and C4 were the most common in each group. According to Kistner classification, grade I and grade II were more frequent in each group.
Clinical characteristics of the participants.
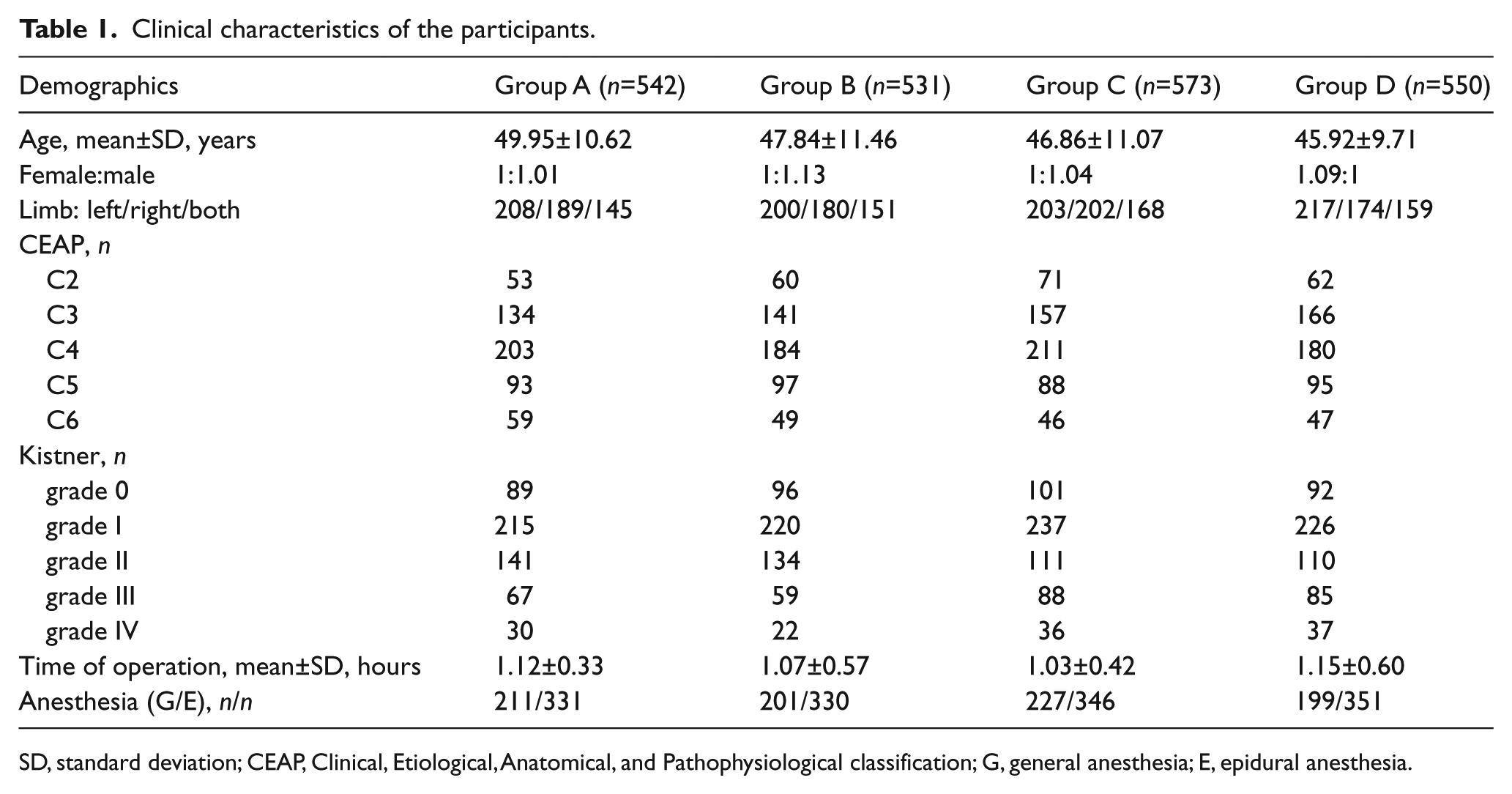
SD, standard deviation; CEAP, Clinical, Etiological, Anatomical, and Pathophysiological classification; G, general anesthesia; E, epidural anesthesia.
The mean operating time (p=0.282) and type of anesthesia (p=0.192) were similar across groups. Biochemical data including hemostatic testing were similar between groups (Table 2).
Results of laboratory biochemical investigations.
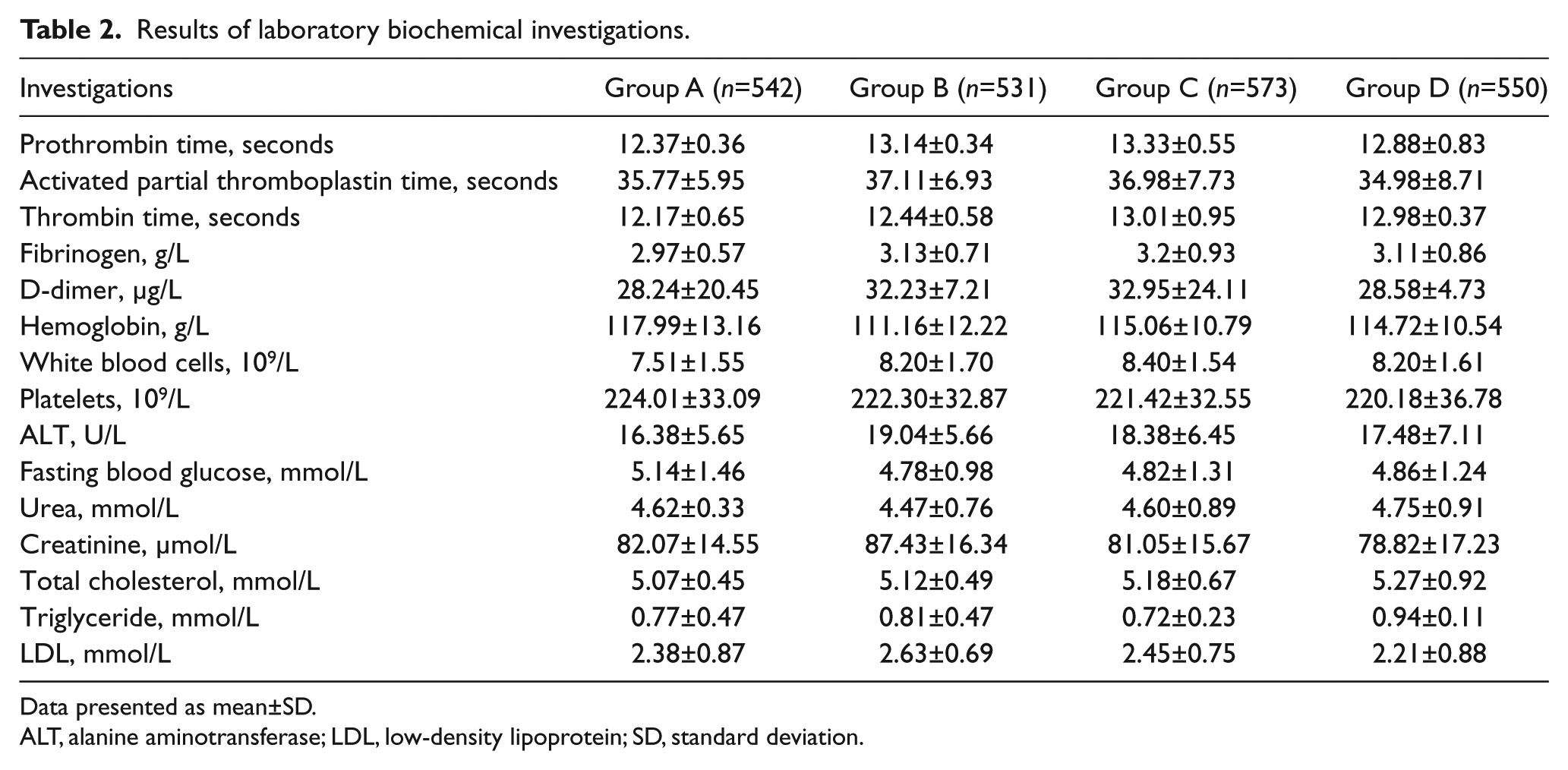
Data presented as mean±SD.
ALT, alanine aminotransferase; LDL, low-density lipoprotein; SD, standard deviation.
In group A, DVT occurred in 28 patients (5.17%) and PE occurred in eight patients (1.48%) (Table 3), which was higher than in other groups (p<0.01). The majority of these events (67.86% (19/28) in group A) occurred within 2 weeks after surgery. The incidence of DVT was similar amongst groups B, C, and D. There were no documented PE in any of the active chemoprophylaxis groups. There were no differences for incidence of DVT and PE between groups B, C and D (p=0.88). In these groups, all DVTs occurred after 2 weeks.
Incidence of DVT, PE and hemorrhage.
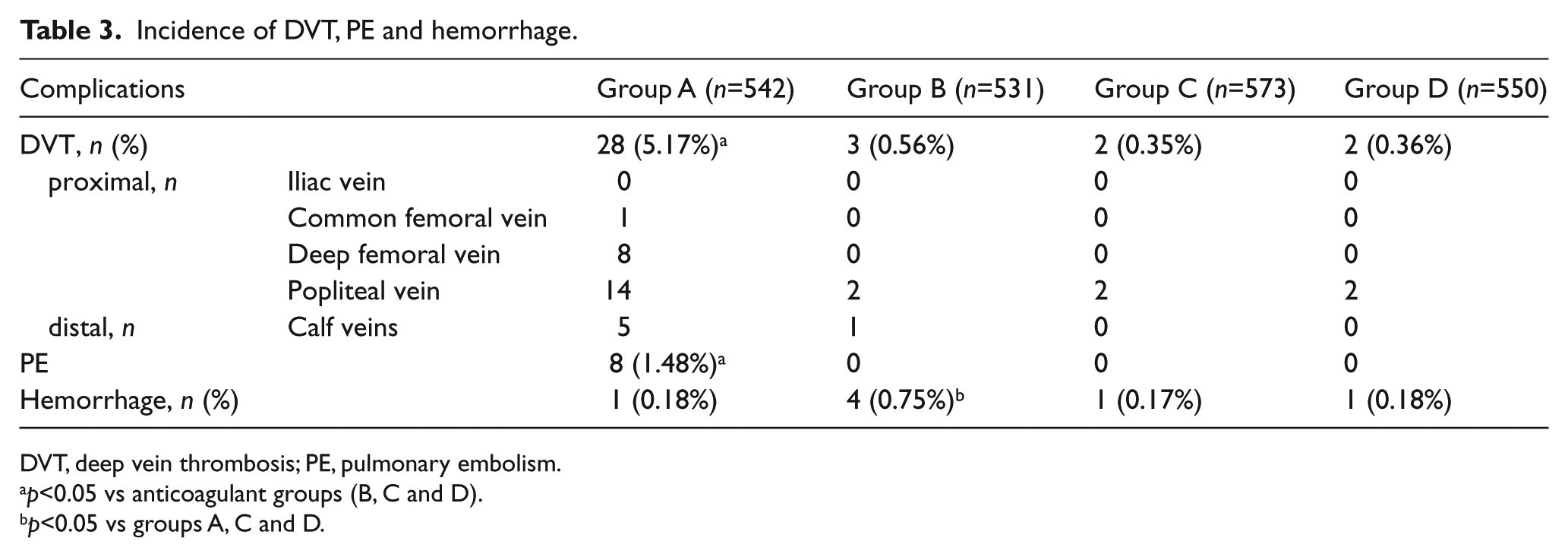
DVT, deep vein thrombosis; PE, pulmonary embolism.
p<0.05 vs anticoagulant groups (B, C and D).
p<0.05 vs groups A, C and D.
There were four (0.75%) patients with a hemorrhage complication in group B, including two with extensive ecchymosis, one with a moderate incisional bleeding and one with a slight spinal epidural hematoma. The incidence of hemorrhage complication in group B was higher than in the other groups (p<0.01). Within this group, all hemorrhagic events occurred within the first week after surgery. There was one case of extensive ecchymosis in group C and group D, respectively. Anticoagulant therapy was stopped in each of these patients immediately. There was no fatal bleeding. There was no significant difference of bleeding risk between groups A, C and D (p=0.53) (Figure 1).
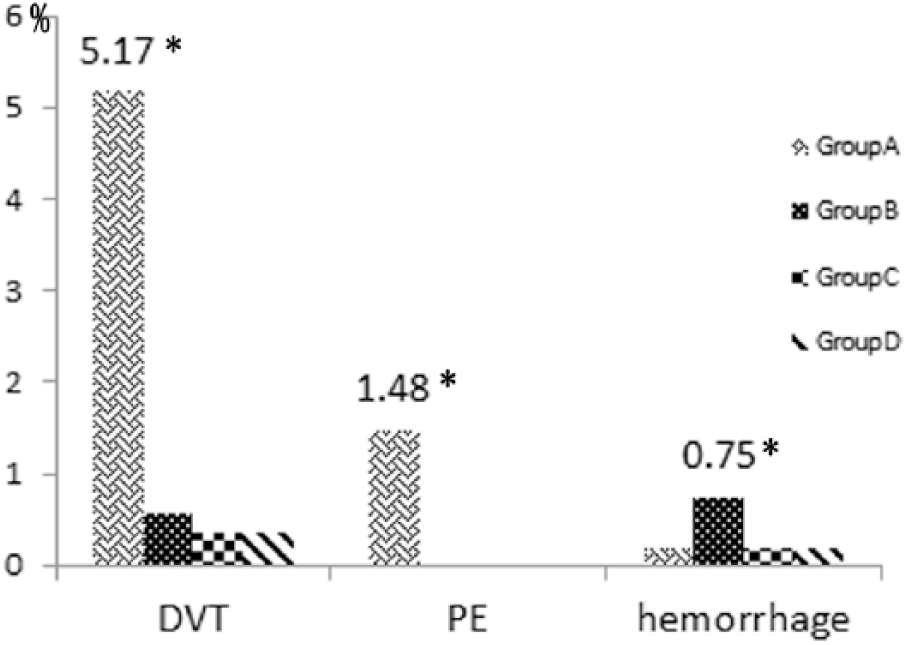
The incidence of deep vein thrombosis (DVT), pulmonary embolism (PE) and hemorrhage in the total 2196 varicose veins patients, including 542 patients without venous thromboembolism (VTE) prophylaxis in group A, 531 patients with low-dose unfractionated heparin (LDUH) in group B, 573 patients with low-molecular-weight heparin (LMWH)-once in group C, and 550 patients with LMWH-twice in group D. The incidence of DVT and PE in group A was significantly higher than other groups (5.17% vs 0.56, 0.35, 0.36; p<0.01) and (1.48% vs 0; p<0.01). There was no distinction for incidence of DVT and PE between groups B, C and D (p=0.88). The incidence of hemorrhage in group B was significantly higher than groups A, C and D (0.75% vs 0.18%, 0.17%, 0.18%; p<0.01). There was no significant difference of bleeding risk between groups A, C and D (p=0.53).
Discussion
High ligation with GSV stripping is a common surgical procedure for patients with symptomatic varicose veins. 11 Although various new techniques have been developed in recent years, conventional surgery is still the most widely used in China and Third World countries today.12,13 This procedure, however, may be complicated by DVT or PE as a morbid and possible mortal complication of this procedure. 5 Neither the incidence of postoperative VTE following varicose vein surgery nor the appropriate chemoprophylaxis strategy have been adequately established in large patient population studies. 6 The principal finding of this study is an estimate of DVT/PE following high ligation and GSV surgical stripping in patients who are given no chemoprophylaxis postoperatively. We now show in a large study population that the risk for such an intervention is low but not negligible with a rate of DVT of just over 5% and PE of approximately 1.5%. These percentages are in keeping with data found in other studies. In a series of studies, the incidence of symptomatic DVT after VV surgery was 0.15–5.3%.6,14 The mechanism for postoperative VTE in such patients fits neatly with Virchow’s theory, including stretching of the SFJ with associated venous endothelial injury, activation of the coagulation cascade, and venous stasis associated with the procedure. Although early ambulation alone is widely accepted, this does not appear to be adequate to prevent thrombotic outcomes in such patients. Intermittent pneumatic compression (IPC) may be useful; however, many of these procedures are done as an outpatient protocol, thus limiting the application of this form of prophylaxis.
The second important finding of this study is the efficacy of three different chemoprophylaxis regimens including thrice daily LDUH, enoxaparin 6000 IU once daily and enoxaparin 4000 IU twice daily. These three regimens reduced the incidence of DVT by 90% and eliminated the occurrence of PE. Each regimen included a minimum of injections, which were limited to 3 days postoperatively. These brief regimens are therefore both feasible and economical for widespread implementation.
The third important finding of this study is an estimate of major bleeding if one of these regimens is adopted. The risk of bleeding was greatest for those patients randomized to receive thrice daily LDUH (group B). For the other two active chemoprophylaxis regimens, bleeding complications were infrequent and largely limited to ecchymosis. The safety of these strategies would therefore argue for their implementation for such procedures. LMWH appears to be safe and has played an important anticoagulant role since its implementation in China in 1989. 15
In summary, postoperative VTE chemoprophylaxis following high ligation and GSV stripping effectively reduces the venous thrombosis complications of this procedure. Of the three active strategies tested, no difference in efficacy was noted; however, thrice daily LDUH did increase bleeding complications.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.