
Abstract

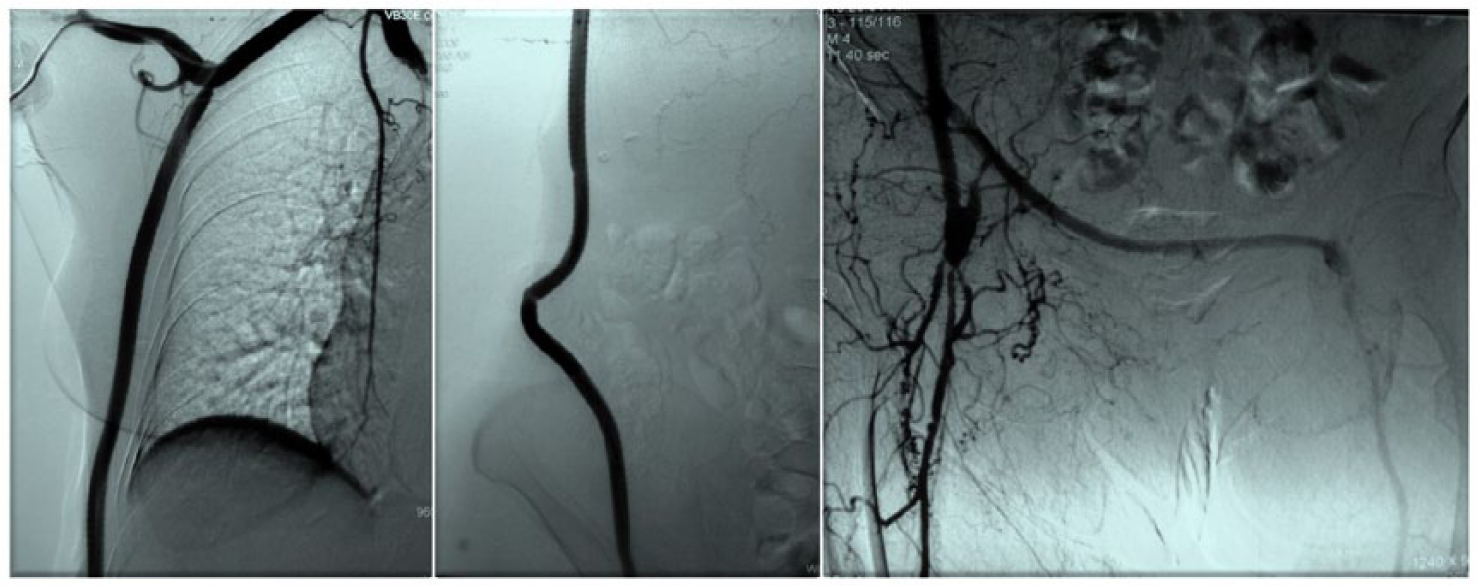
A 79-year-old female patient with chronic obstructive pulmonary disease and ischemic cardiomyopathy was admitted for critical limb ischemia secondary to diffuse aortoiliac occlusive disease (AIOD). Consequently a right axillary–biprofunda bypass using an externally supported polyester prosthesis was successfully performed. Twelve months later, after suffering multiple compression fractures of osteoporotic lumbar vertebrae, with clinically noticeable loss of stature, the patient developed tender skin discoloration over the axillofemoral graft limb (Panel A: contour of tortuous subcutaneous prosthesis, with an area of devitalized skin corresponding to the apex of the kinked distal portion). Transaxillary angiography revealed a patent but acutely angulated graft (Panel B, middle) . Under local anesthesia, the redundant prosthetic segment was resected, accompanied by the excision of the compromised skin and primary suture.

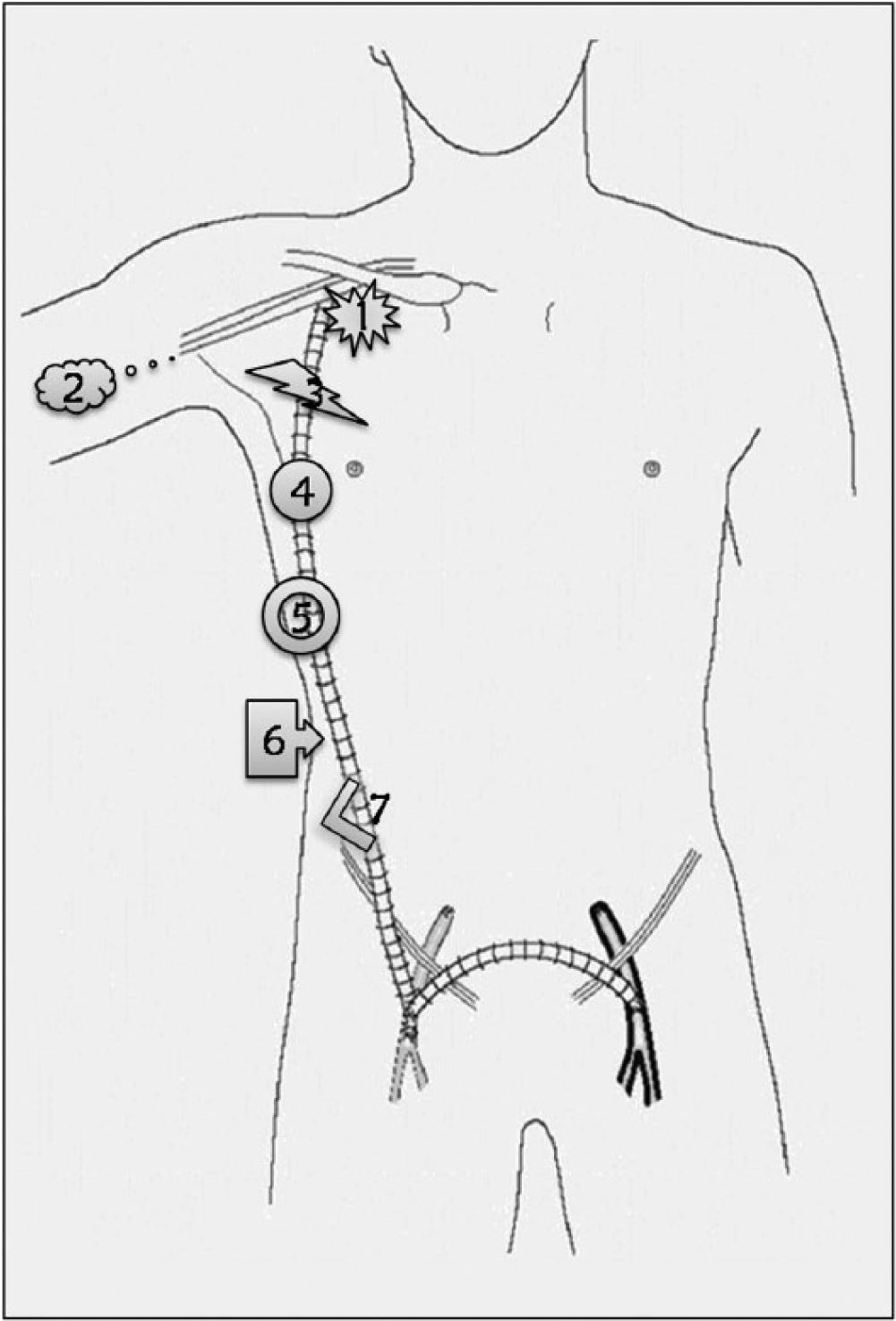
Although performed infrequently, axillobifemoral bypass (AxBFB) is a well-established and valuable reconstructive procedure, used mostly for (1) indirect open repair of AIOD in patients with local or systemic contraindications for laparotomy, and (2) ex situ treatment of an infected infrarenal aortic graft or stent-graft.1,2 Since its introduction 50 years ago, 3 a number of studies and case reports describing problems unique to or more common with this type of extra-anatomic bypass have been published. 1 These include graft tunnel hematoma, heightened susceptibility to graft thrombosis and infection, and other complications (Panel C): (1) proximal anastomotic pseudoaneurysm (‘axillary pullout syndrome’), (2) upper extremity distal thromboembolism, (3) graft fracture, (4) non-anastomotic graft (pseudo)aneurysm, (5) perigraft seroma, (6) external graft compression, and (7) graft elongation and angulation with possible skin erosion and prosthetic material contamination.
As with any type of vascular reconstruction, prerequisites for a successful and durable outcome of AxBFB are appropriate patient selection and operative technique. However, patient-related factors leading to late postoperative complications are not always predictable and preventable.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather L Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.