
Abstract

Authors will present posters based on the following abstracts at the 2014 SVM 25th Anniversary and Scientific Sessions. The poster session will be at 3:15 p.m., Thursday, June 12, 2014.
In honor of Jay D. Coffman (1928–2006), distinguished internist and researcher of vascular medicine and clinical cardiology, SVM sponsors an annual award in vascular medicine and biology research. The top finalists will make oral presentations at the meeting during Session 5: Jay D. Coffman Young Investigator Award Presentations Luncheon, 11:30 a.m., Thursday, June 12, 2014.
The winners of the Jay D. Coffman Young Investigator Award (YIA) will be announced during the Award Presentations, 9:15 a.m., Friday, June 13, 2014.
All events will take place at the Hilton La Jolla Torrey Pines, La Jolla, California, USA.
For more information about the meeting, see the SVM website: www.vascularmed.org/am25
Poster abstracts are organized by category.
Basic science – Vascular medicine YIA 1
Proton pump inhibitors inhibit the cardiovascular enzyme DDAH and regulate processes underlying idiopathic pulmonary fibrosis
Yohannes T Ghebremariam1, Qingtao Zhou2, Joao de Andrade3, Lawrence Ho4, Glenn D Rosen4, John P Cooke1
1Houston Methodist Research Institute, Houston, TX, USA; 2Peking University Third Hospital, Beijing, China; 3University of Alabama at Birmingham, Birmingham, AL, USA; 4Stanford University, Stanford, CA, USA
Rationale: The cardiovascular enzyme dimethylarginine dimethylaminohydrolase (DDAH) has recently been implicated in the progression of idiopathic pulmonary fibrosis (IPF). By degrading asymmetric dimethylarginine (ADMA), an endogenous inhibitor of inducible nitric oxide (NO) synthase (iNOS), DDAH releases the brake on a pathway implicated in lung injury and fibrosis.
Objectives: To discover DDAH inhibitors, and to assess the effect of such inhibitors on processes underlying IPF.
Methods: We performed high throughput screening (HTS) of over 130,000 small molecules and discovered that the proton pump inhibitors (PPIs) directly inhibit DDAH. In addition, we assessed the effect of PPIs on collagen synthesis by IPF lung fibroblasts. Finally, retrospective analysis of interstitial lung disease (ILD) database was performed to assess the effect of PPIs on transplant-free survival of IPF patients.
Results: We found that the PPIs inhibit DDAH activity in biochemical assays, cell culture and in vivo. In addition, the PPIs reduced the production of soluble collagen by primary IPF lung fibroblasts in response to the pro-fibrotic cytokine TGFβ and regulated both proliferation and survival of lung alveolar epithelial cells. Retrospective review of the ILD database of 215 IPF patients (of who 130 were on PPIs for >1 year) revealed a survival advantage (i.e. time to transplant or death when calculated from the time of diagnosis) of the patients on PPIs compared to controls.
Conclusions: Our data reveal a plausible biological explanation for the clinical benefit of the PPIs in IPF. The reported reduction in radiologic fibrosis score and survival advantage of IPF patients on PPIs may be due to modulation of the DDAH/NOS pathway.
Clinical science/epidemiology – Arterial and aortic disease YIA 2
Association between angiotensin converting enzyme inhibitor use and major adverse cardiovascular events among patients with critical limb ischemia
Ehrin J Armstrong1, Debbie C Chen2, Gagan D Singh2, Ezra A Amsterdam2, John R Laird2
1University of Colorado, Denver, CO, USA; 2University of California, Davis, Sacramento, CA, USA
Background: Angiotensin converting enzyme inhibitors (ACEI) are recommended for secondary prevention in peripheral arterial disease, but their effectiveness in patients with critical limb ischemia (CLI) is uncertain.
Methods: Four hundred and fourteen patients (177 women, 237 men) with CLI underwent diagnostic angiography or therapeutic endovascular intervention from 2006 to 2012 at a multidisciplinary vascular center. ACEI or angiotensin receptor blocker use was assessed at the time of angiography and confirmed during the follow-up period. Major adverse cardiovascular events (MACE), mortality, and major adverse limb events (MALE) were assessed during a 3-year follow-up. Propensity matching was used to adjust for baseline differences between patients taking and not taking ACEI.
Results: 234 (57%) patients were prescribed ACEI. Patients prescribed ACEI had more baseline comorbidities including diabetes (70% vs 53%, p=0.001) and hypertension (94% vs 72%, p=0.001). Patients prescribed ACEI had lower 3-year unadjusted rates of MACE (40% vs 46%), mortality (34% vs 42%), and major amputation (18% vs 23%). After propensity matching, ACEI use was associated with significantly lower rates of MACE (HR 0.76, 95% CI 0.58–0.99) and overall mortality (HR 0.71, 95% CI 0.53–0.95). There was no significant association between ACEI use and MALE (HR 0.77, 95% CI 0.58–1.03) or major amputation.
Conclusions: ACEI use is associated with lower MACE and mortality in patients with CLI, but no effect on limb-related outcomes.

YIA 3
Fibromuscular dysplasia is a morbid disease with low associated mortality: A report of the United States Registry for Fibromuscular Dysplasia
Sarah O’Connor1, Jeffrey W Olin2, Xiaokui Gu3, J Michael Bacharach4, Yung-Wei Chi5, James Froehlich3, Bruce Gray6, Esther SH Kim7, Eva Kline-Rogers3, Pamela Mace8, Robert McBane9, Aditya Sharma10, Heather Gornik7
1Cleveland Clinic Lerner College of Medicine, Cleveland, OH, USA; 2Mount Sinai School of Medicine, New York, NY, USA; 3University of Michigan, Ann Arbor, MI, USA; 4North Central Heart, Sioux Falls, SD, USA; 5University of California, Davis, Sacramento, CA, USA; 6Vascular Health Alliance, Greenville, SC, USA; 7Cleveland Clinic Foundation, Cleveland, OH, USA; 8Fibromuscular Dysplasia Society of America, Rocky River, OH, USA; 9Mayo Clinic, Rochester, MN, USA; 10University of Virginia Health System, Charlottesville, VA, USA
Background: Fibromuscular dysplasia (FMD) is an uncommon non-atherosclerotic disease of medium sized arteries. The natural history of this disease remains unknown.
Methods: Prevalence of major vascular events at the time of enrollment and during initial Registry follow-up are reported. Major vascular event was defined as: death, dissection, MI, coronary revascularization, TIA, stroke, SAH, mesenteric ischemia, or renal infarction.
Results: Among 913 patients, mean age at enrollment was 55.9±12.8 years (range 18–90), and 91.9% were female. 38.1% of patients had at least one major vascular event at the time of enrollment (Table). 23.7% (207/873) of patients had ≥1 arterial dissection and 23.1% (201/871) had ≥1 aneurysm. Median follow-up for 488 patients who were enrolled ≥1 year and with ≥1 follow-up visit was 23.9 months (IQR 12.4–36.3). During follow-up, 29 major vascular events occurred in 22 patients at a rate of 2.9 events per 100 patient-years (Table). There was no significant difference in the risk of subsequent major vascular event between groups with and without prior vascular events, HR=1.2 (95% CI 0.5–3.2; p=0.71). There were 4 deaths (0.8%), 3 of which were due to malignancy and 1 of unknown cause.
Conclusions: FMD is a morbid vascular disease associated with a high rate of major vascular events but low mortality (Table). While many FMD patients present with dissection, stroke, or infarction, few proceed to have further vascular complications during surveillance. There is no evidence that history of a major vascular event was associated with increased risk of subsequent events during the first 2 years of follow-up.
Distribution of vascular events at baseline and follow-up.

Clinical science/epidemiology – Other YIA 4
Registry findings of fibromuscular dysplasia of the mesenteric arteries
Erin K Moore1, Xiaokui Gu2, Jeffrey W Olin3, James B Froehlich2, J Michael Bacharach4, Michael R Jaff5, Barry T Katzen6, Eva Kline-Rogers2, Pamela D Mace7, Alan H Matsumoto8, Robert D McBane9, Christopher J White10, Esther SH Kim11, Heather L Gornik11, Bruce H Gray1
1Greenville Health System, Greenville, SC, USA; 2University of Michigan, Ann Arbor, MI, USA; 3Mount Sinai Medical Center, New York, NY, USA; 4North Central Heart, Sioux Falls, SD, USA; 5Massachusetts General Hospital, Boston, MA, USA; 6Miami Baptist Cardiac/Vascular Institute, Miami, FL, USA; 7Fibromuscular Dysplasia Society of America, Rocky River, OH, USA; 8University of Virginia Health System, Charlottesville, VA, USA; 9Mayo Clinic, Rochester, MN, USA; 10Ochsner Clinic, New Orleans, LA, USA; 11Cleveland Clinic Foundation, Cleveland, OH, USA
Introduction: Fibromuscular dysplasia (FMD) most commonly affects the renal, carotid and vertebral arteries. The prevalence and natural history of mesenteric arterial FMD (mFMD) is unknown.
Methods: Data from the United States Registry for Fibromuscular Dysplasia was collected from the registry for patients who had assessment of their mesenteric arteries and compared to those with renal, carotid and/or vertebral artery FMD. Prevalence, demographics (including history and physical examination), other vascular beds involved, and interventions performed were compared with patients who had no mesenteric involvement.
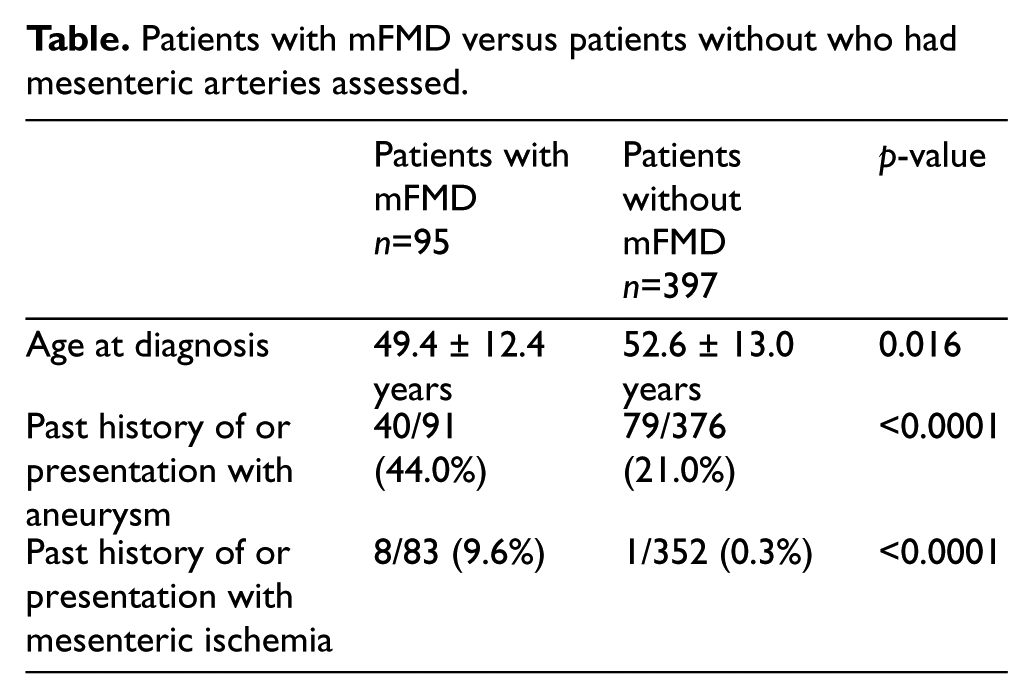
Results: Of 873 patients in the registry, 492 (56.4%) patients had their mesenteric vessels imaged. 95 (19.3%) had involvement of their mesenteric arteries (mFMD). Of the 95 mFMD patients, 15 (15.8%) were male. Compared to the patients without mFMD, they were younger (49.4±12.4 vs 52.6±13.0, p=0.016) and often present with abdominal complaints, like post prandial abdominal pain (18.8% vs 6.5%, p=0.001), flank or abdominal pain (34.9% vs 17.7%), abdominal bruit (30.5% vs 7.8%, p<0.0001), aneurysm (44.0% vs 21.0%, p<0.0001) and mesenteric ischemia (9.6% vs 0.3%, p<0.0001). Of the mFMD patients who had other vascular beds imaged, 79/92 (85.9%) had renal involvement, 55/80 (68.8%) had carotid FMD, and 45/79 (57%) had both. Aneurysm (41.2%) or dissection (35.6%) were common in those with mFMD, compared to 19.7% and 20.6% of those without (p<0.0001/p=0.0046). These mFMD patients required intervention (18.6%) less frequently than those with renal FMD (90.3%) and those with carotid FMD (26.5%).
Conclusions: Involvement of the mesenteric arteries in FMD is much more common than previously thought. Patients with involvement of their mesenteric vessels often have another vascular bed affected as well. Aneurysms and dissection are quite common in these patients. They present most commonly with abdominal complaints and many go on to require intervention for their mesenteric disease.
Patients with mFMD versus patients without who had mesenteric arteries assessed.
Clinical science/epidemiology – Vascular medicine YIA 5
The clinical utility of a simple question quantifying physical activity sufficiently intense to induce diaphoresis in the prediction of future risk for PAD and all-cause mortality
Peter Chang
National University Hospital Singapore, Singapore, Singapore
Background: Physical activity and exercise capacity are correlated with outcomes in PAD patients. Formal stress testing is expensive and time consuming. The role of simple correlates of exercise intensity in the prediction of outcomes for PAD is unclear.
Methods: Binary response to participation in regular activity intense enough to work up a sweat, at least once a week, was assessed in individuals undergoing non-emergent coronary angiography. Clinical demographics and questionnaires including WIQ were collected. Subjects were followed prospectively for mortality over a mean period of 5.0 years.
Results: Participation in regular intense activity is inversely associated with PAD (odds ratio [OR] 0.58) and associated with higher ABI measurements (coefficient 0.045). Regular intense activity also correlated with higher WIQ scores. Adjusting for cardiovascular risk factors, CAD and other confounders, participants of regular intense activity experienced significantly lower total mortality rates (hazard ratio [HR] 0.48) compared with those who did not. The addition of this simple question to the Framingham Risk Score (FRS) significantly improved the net reclassification index (NRI) for predicting all-cause and cardiovascular mortality (NRI of 33.5% and 31.9%, respectively).
Conclusions: Patients with PAD who engage in regular activity intense enough to work up a sweat have a lower mortality rate even after adjusting for other co-morbidities. Such activity correlates with a higher ABI and greater WIQ scores and adds prognostic value to the FRS. This simple and inexpensive question can predict objective measures of functional performance and disease outcome, suggesting relevance as a prognostic tool.

Adjusted for age, gender, race, systolic blood pressure, medications, BMI, smoking, diabetes, cholesterol levels, coronary artery disease, and creatinine * Adjusted with addition of peripheral arterial disease
Basic science – Angiogenesis/vasculogenesis Poster 1
ERK1/2 mediates lipopolysaccharide-upregulated FGF-2, UPA, MMP-2, MMP-9, and cellular migration in primary cardiac fibroblasts
Wei Syun Hu
Shuang Ho Hospital, Taipei, Taiwan
Upregulation of fibroblast growth factor (FGF), urokinase plasminogen activator (uPA), tissue plasminogen activator (tPA) and matrix metallopeptidases (MMPs) is associated with the development of myocardial infarction (MI), dilated cardiomyopathy, cardiac fibrosis and heart failure (HF). Evidences suggest that lipopolysaccharide (LPS) participates in the inflammatory response in the cardiovascular system; however, it is unknown if LPS is sufficient to upregulate expressions and/or activity of FGF-2, uPA, tPA, MMP-2 and MMP-9 in cardiac fibroblasts. In the present study, we treated primary cardiac fibroblasts with LPS to explore whether LPS upregulates FGF-2, uPA, tPA, MMP-2, MMP-9 and cellular migration, and further to identify the precise molecular and cellular mechanisms behind these upregulatory responses. Here we show that LPS challenge increased the protein levels of FGF-2, uPA, MMP-2 and MMP-9, and induced the activity of MMP-2 and MMP-9 in cardiac fibroblasts. After administration of inhibitors including U0126 (ERK1/2 inhibitor), SB203580 (p38 MAPK inhibitor), SP600125 (JNK1/2 inhibitor), CsA (calcineurin inhibitor) and QNZ (NFkB inhibitor), the LPS-upregulated expression and/or activity of FGF-2, uPA, MMP-2 and MMP-9 in cardiac fibroblasts is markedly inhibited only by ERK1/2 inhibitors, U0126. Collectively, these results suggest that LPS upregulates the expression and/or activity of FGF-2, uPA, MMP-2 and MMP-9, and the subsequent cell migration through the ERK1/2 signaling pathway in primary cardiac fibroblasts. Our findings further provide a link between the LPS-induced cardiac dysfunction and the ERK1/2 signaling pathway that mediates the upregulation of FGF-2, uPA, MMP-2, MMP-9 and cellular migration in primary cardiac fibroblasts.
Basic science – Arterial and aortic disease Poster 2
In vivo study of multilayer flow modulator stents and their delivery system in porcine aneurysm models
Edel P Kavanagh, Niamh Hynes, Sherif Sultan
Western Vascular Institute, Galway, Ireland
Objective: The aim was to examine a new concept in vascular endoprosthesis, the Cardiatis (Isnes, Brussels) multilayer flow modulator (MFM) stent. This study tested the hypothesis that the MFM stent could treat aortic aneurysms through intra-arterial hemodynamic modulation, without substantial parent or small branch artery compromise.
Methods: An experimental aneurysm was implemented in eight porcine test animals using external jugular vein which was grafted onto the abdominal aorta. Performance in the repair of the aneurysm was assessed, as well as demonstration of the absence of short and medium-term undesired effects. After the implantation periods were complete, all animals were then euthanized, devices withdrawn and explants examined. Assessment of the expected technical performance of the delivery system was also conducted on a separate porcine test animal that did not have an induced aneurysm. The facility, safety, reliance of navigability, and release of the stent without complication was evaluated. Placement, deployment and ease of withdrawal of the delivery system was satisfactory and without complication.
Results: A follow-up of the induced aneurysm models at 8 days with angiography showed three aneurysms were reduced in size and one was totally excluded. After 1 month, the devices and vessels were explanted and examined in detail. The opening of the aneurysm was nearly occluded with thrombus in two of the explants. The wall of the venous graft had also thickened significantly, suggesting an evolution into an arterial type vessel wall. Total absence of intimal hyperplasia was observed in all explants. The visceral arteries covered by the stent remained patent, and the stent adhered to the arterial wall with endothelization clearly visible. The stent was placed without intra-arterial compromise, and the aneurysms were stabilized while adequate blood flow to the collateral arteries was preserved.
Conclusion: Further studies to assess its long-term safety and effectiveness are needed, including in vitro studies and clinical trials.
Poster 3
Study of endothelialisation kinetics of single versus multilayer arterial stents
Edel Kavanagh, Niamh Hynes, Sherif Sultan
Western Vascular Institute, Galway, Ireland
In order to understand in more detail the integration phenomenon of this 3-dimension Cardiatis multilayer flow modulator (MFM) stent into the arterial wall, a comparative study on the endothelialisation processes and kinetics of a number of commercially available stents was conducted. The endothelialisation kinetics were evaluated by histology, immunohistochemistry and ultrastructural analysis in five porcine models. Nineteen arteries consisting of the left and right iliac and carotid arteries were implanted with the MFM stent (n = 10), and two control stents: the EucaPWS (Eucatech AG, Rheinfelden, Germany) (n = 4) and SMART (Cordis Corporation, Bridgewater, NJ, USA) stents (n = 5). The devices and arteries were explanted at 1, 2, 3, 4 and 5 weeks of implantation. To identify the endothelial cells at the surface of the neoformed tissue, an RNA study by quantitative PCR, and labelling with the anti-Von Willebrand factor antibody were carried out. Scanning electronic microscopy (SEM) analysis of the lumen of the vessels, and histological sections were also conducted. Results demonstrated the MFM showed faster signs of integration and thinner neointimal coverage as compared to each of the controls. The EucaPWS stent group overall showed delayed signs of healing, while the SMART and MFM behaved quite similarly. SEM and immunohistochemistry confirmed the presence of early endothelial cells overlaying the three stents. No significant signs of local intolerance were observed with the stents. This study highlighted that the endothelialisation process of the MFM stent differed from that of the single layer stents. The MFM stents showed signs of faster integration and thinner neointimal development and coverage compared to the control single layer stents. This resulted from the beneficial impact of the 3-dimension structure of the MFM stent on intra-arterial blood flow. Further studies to assess the MFM stents’ long-term safety and effectiveness are needed, including in vitro studies and long-term clinical trials.
Poster 4
Assessment of carotid artery intima-media thickness and aortic pulse wave velocity in diffuse coronary artery ectasia
Emre Yalcinkay1, Cem Barcin2
1Aksaz Military Hospital, Mugla, Turkey; 2Gulhane Military Medical Faculty, Ankara, Turkey
Objectives: It has been shown that carotid intima-media thickness (CIMT) and aortic pulse wave velocity (PWV) constitute important independent risk factors for cardiovascular disease. We hypothesized that CIMT and aortic PWV are increased in patients with diffuse coronary artery ectasia.
Study design: Diffuse coronary artery ectasia (CAE) has been defined as a diffuse dilatation in at least one coronary artery and localized or diffuse disease in the other coronary artery. The study group consisted of 54 consecutive patients with diffuse CAE; 58 patients without CAE comprised the control group. CIMT and aortic PWV were measured in two groups of patients who underwent coronary angiography.
Results: Study and control groups were similar in terms of age, sex, body mass index, and the frequencies of hypertension, hyperlipidemia, diabetes mellitus, and smoking (p>0.05). The mean CIMK and aortic PWV were significantly higher in the study group compared to the control group (0.81±0.16 mm and 0.74±0.13 mm, p=0.021; and 11±2.4 m/sec and 9±2.7 m/sec, p<0.001, respectively). A significant but a weak relationship was found between CIMK and the presence of diffuse CAE (r=0.219; p=0.021). Compared to CIMT, a more powerful positive correlation was found between aortic PWV and the presence of diffuse CAE (r=0.370; p<0.001). Logistic regression analysis showed that the relationship between diffuse CAE and aortic PWV (OR 1.339; 95% CI 1.135–1.579; p=0.001) was independent of other factors. An aortic PWV ≥9.3 m/sec measured on admission had a 78% sensitivity and 62% specificity in predicting diffuse CAE at ROC curve analysis.
Conclusion: According to the results of the present study, both CIMT and PWV were increased in patients with diffuse CAE. Of note, only the PWV was found to have an independent relationship with the presence of CAE. It may be speculated that the involvement of media compared to intima is more likely in patients with CAE. This pathophysiology may explain why PWV, compared to CIMT, has a more powerful relationship with CAE.
Basic science – Endothelial function and surrogate markers Poster 5
Preserved endothelium-dependent dilation is not associated with lower endothelin activity in women with atherosclerotic risk factors
Vijaywant Brar1, Carmine Cardillo2, Manfredi Tesauro3, Julio A Panza4, Umberto Campia5
1MedStar Washington Hospital Center, Washington, DC, USA; 2Catholic University, Rome, Italy; 3Tor Vergata University, Rome, Italy; 4Westchester Medical Center, Valhalla, NY, USA; 5MedStar Heart Institute, Washington, DC, USA
Background: Compared with age-matched men, middle-aged women have higher endothelium-dependent dilation (EDD) and lower vascular activity of the vasoconstrictor and proatherosclerotic peptide endothelin-1 (ET-1). Whether the presence of atherosclerotic risk factors (ARFs) abrogates gender differences in EDD and ET-1 activity has not been investigated. This study tested the hypothesis that ARFs blunts gender differences in EDD and ET-1 activity between middle-aged men and women.
Methods: Forearm blood flow (FBF) responses were measured by strain-gauge plethysmography during the intra-arterial infusion of the endothelium-dependent vasodilator acetylcholine (ACh), the endothelium-independent vasodilator sodium nitroprusside (SNP), and the selective ETA receptor blocker BQ-123 in 50 women and 64 men with atherosclerotic risk factors.
Results: Baseline characteristics of study participants are reported in the Table. EDD to ACh was significantly higher in women compared with men (p<0.05). In contrast, responses to SNP were similar between women and men (p=NS). BQ-123 administration resulted in a significant progressive vasodilator response in both the female and male group (p<0.001 for both). When these responses were compared between the two gender groups, no significant differences were observed (p=NS).
Conclusions: Women with ARFs have preserved EDD compared with men. However, their vascular ET-1 activity appears to be similar to men. The lack of difference in ET-1 activity between women and men suggests that, despite a preserved EDD, the presence of ARFs is associated with endothelial dysfunction, which may promote the development of atherosclerosis, thereby increasing the cardiovascular risk of women.
Baseline characteristics of study participants.

Values are reported as mean ± SD
Poster 6
Poster 7
Impaired vascular endothelial growth factor A and inflammation in patients with peripheral artery disease
Omar L Esponda1, Donald E Parker2, Polly S Montgomery3, Danuta Sosnowska3, Ana I Casanegra1, Zoltán Ungvári3, Anna Csiszár3, William E Sonntag3, Andrew W Gardner3
1OUHSC, Department of Medicine, Cardiovascular Section, Oklahoma City, OK, USA; 2OUHSC, Department of Biostatistics and Epidemiology, Oklahoma City, OK, USA; 3OUHSC, Reynolds Oklahoma Center on Aging, Oklahoma City, OK, USA
Background: The greater comorbid burden in patients with PAD contributes to higher levels of inflammation and oxidative stress, but it is not clear whether these comorbid conditions exert additional influence on inflammatory and vascular biomarkers beyond that seen from the atherosclerotic burden of PAD.
Methods: We compared apoptosis, cellular oxidative stress, and inflammation of cultured endothelial cells treated with sera from 130 patients with peripheral artery disease (PAD) and a control group of 36 patients with high burden of comorbid conditions and cardiovascular risk factors. Second, we compared circulating inflammatory, antioxidant capacity, and vascular biomarkers between the groups.
Results: The groups were not significantly different (p>0.05) on apoptosis, hydrogen peroxide, hydroxyl radical antioxidant capacity, and nuclear factor kappa-light-chain enhancer of activated B cells. Circulating tumor necrosis factor alpha (TNFα; p=0.016) and interleukin 8 (IL-8; p=0.006) were higher in the PAD group, whereas vascular endothelial growth factor A (VEGF-A; p=0.023) was lower.
Conclusion: The PAD does not impair the endothelium beyond that which already occurs from comorbid conditions and cardiovascular risk factors in patients with claudication. However, patients with PAD have lower circulating VEGF-A than the control group and higher circulating inflammatory parameters of TNFα and IL-8.
Basic science – Vascular medicine Poster 8
Transflammation: Its role in direct conversion of fibroblasts into endothelial cells
Shu Meng, Nazish Sayed, Wing Tak Wong, John P Cooke
Houston Methodist Research Institute, Houston, TX, USA
Background: Our research mission is directed towards endothelial regeneration for the treatment of vascular diseases. My hypothesis is derived from the radical concept that somatic cell phenotype is fluid when epigenetic plasticity is increased by optimal activation of innate immunity. We have discovered that efficient nuclear reprogramming of human fibroblasts to pluripotency required activation of the TLR3 pathway (Lee et al., Cell, 2012). Optimal activation of innate immunity leads to increased epigenetic plasticity and fluidity of cell phenotype.
Hypothesis: With the recognition of the role of innate immunity in nuclear reprogramming, we hypothesized that activation of TLR3, together with activators of key pathways involved in EC development (VEGF, BMP4) that drive endothelial cell (EC) specification, may induce the transdifferentiation of fibroblasts into ECs (‘iECs’).
Results: Importantly, we have found that PolyI:C, the TLR3 agonist, when combined with exogenous endothelial growth factors, are effective to transdifferentiate human fibroblasts into iECs (with a high yield of more than 10% CD31+ iECs) in the absence of viral vectors or exogenous transcription factors. These iECs show typical EC phenotype similar to human microvascular ECs in terms of tube formation, acetylated-LDL uptake, and angiogenic cytokine secretion under hypoxia. Interestingly, the NF-κB inhibitors block the transdifferentiation process. In vivo study demonstrated that iECs significantly improved hindlimb blood perfusion and neovascularization in the mouse hindlimb ischemia model.
Conclusion: By increasing epigenetic plasticity, and by providing the correct environmental cues, it appears that we can attain effective transdifferentiation. Thus, we have generated a small molecule based strategy to transdifferentiate fibroblasts to iECs. This study allows us to gain insights into mechanisms of direct reprogramming and to generate a small molecule approach for therapeutic transdifferentiation.
Basic science – Vascular surgery Poster 9
In vivo assessment of the biocompatibility and thread number of multilayer stents
Edel Kavanagh, Niamh Hynes, Sherif Sultan
Western Vascular Institute, Galway, Ireland
The aim was to examine in vivo, the biocompatibility of the Cardiatis (Isnes, Brussels) multilayer flow modulator (MFM) stent. Three time periods were taken into account: 1, 3 and 6 months. A porcine model was used to assess the presence or absence of complication, confirmation or not of biocompatibility of the stent and appropriate fitting of the devices to the vessels. Twelve implanted stents had a 56-thread design while 14 implanted stents had a denser mesh of 80–96 threads. Two, three or four stents were implanted in each animal, in the iliac and carotid arteries. One animal received a stent in a renal artery. Upon sacrifice of the animals, the stents and sections of the artery in which they were placed were explanted and prepared for gross examination, histological examination and scanning electron microscopy (SEM). A total of 26 stents were deployed in eight pigs. Percentage stenosis was calculated upon explantation. For the 3-month interval, the mean percentage stenosis for the 56-thread stents was roughly half (16.9 ± 5.1%) of the mean percentage stenosis recorded in the 80–96 thread stents (33.4 ± 10.2%). For the 6-month interval, the mean percentage stenosis was 21.7 ± 9.9% and 33.6 ± 12.4%, for 56-thread and 80–96-thread, respectively. SEM showed that the stents selected for SEM analysis were well deployed, integrated into the vessel wall and endothelialized. Overall, the stent group with 56 threads (3 and 6 months) were well-tolerated locally and yielded fewer signs of inflammation and neointimal hyperplasia. The stenosis percentages evaluated in the two groups were considered within the normal range for stented carotid, iliac or renal arteries. This study concluded that no significant stenosis formation or inflammatory response was recorded across the implanted arteries, with the 56-thread stents yielding less response. The MFM stent therefore offers a biocompatibly viable intra-arterial stent alternative. Further studies to assess its long-term safety and effectiveness are needed, including in vitro studies and long-term clinical trials.
Poster 10
Ultrasound guided percutaneous external ligation of trauma-induced pseudoaneurym of the scalp artery: A case report
Erwin Jannino O Ybanez, Roselyn E Sialongo, Homobono B Calleja, Fatima R Collado, Florimond Garcia
St Luke’s Medical Center, Quezon City, Philippines
This is a case of an 83-year-old male, diabetic and post CABG (2006), who came in owing to a fall, sustaining soft tissue contusion of the right parietal area. A cranial CT scan showed no evidence of acute territorial infarct, intracranial hemorrhage and minimal soft tissue swelling in the right parietal region. Seven months after, the patient had loss of consciousness and a cranial CT scan and MRI showed interval progression of scalp swelling and hematoma of the right parietal region. A carotid duplex showed significant stenosis of the left distal common carotid artery to proximal internal carotid artery. Carotid stenting was done. However, after 3 weeks he had recurrence of loss of consciousness; a repeat cranial CT scan showed insignificant findings. Hyponatremia was noted and considered as a possible cause of dizziness. Due to progression of right scalp hematoma, he was referred to surgery for possible evacuation. The vascular service evaluated the pulsatile scalp mass and a duplex scan showed a vascular mass consistent with pseudoaneurysm with high flow velocity of the feeding artery. Ultrasound compression for 1 hour and 43 minutes of the feeding artery was attempted and showed absent color flow and Doppler signal within the vascular mass. Compression dressing was maintained for 3 days but it showed recurrence of pseudoaneurysm. Ultrasound-guided compression was again attempted for 1 hour and 30 minutes but it did not stop the feeding artery. Since the patient has been taking dual anti-platelet due to recent carotid stenting, ultrasound-guided percutaneous external ligation of scalp artery was successfully done. On follow-up after 4 weeks, it showed no recurrence of pseudoaneurysm.
Basic science – Venous disease Poster 42
Early look at the genetic underpinnings of varicose vein disease
Eri Fukaya1, Yiran Guo1, Hakon Hakonarson1, Rebecca Jonas1, Syed A Hussain2, Deeba Faruq1, Emile R Mohler1
1University of Pennsylvania, Philadelphia, PA, USA; 2Sinai Grace Hospital, Detroit, MI, USA
Background: Varicose vein formation involves complex interplay between genetic makeup and predisposing risk factors. Increased hydrostatic pressure and wall tension causes matrix metalloproteinase (MMP) activation and endothelial cell injury. This triggers extracellular matrix degeneration, which leads to venous wall weakening, dilation and valvular insufficiency. This study aims to identify genetic variations associated with varicose veins by analyzing multicase families.
Methods: Peripheral blood, 14 samples from four families with clustering of varicose veins, was obtained for DNA analysis. Following whole genome genotyping using the 610Q SNP chip from Illumina, genetic linkage analysis using a web-based software Superlink Online SNP was performed to determine chromosomal regions for varicose vein susceptibility. Regions of high LOD score (10-based logarithm of odds) were identified and submitted for sequencing.
Results: Suggestive linkage with LOD >1.5 were detected on chromosomes 11 and 19 indicating possible genetic sharing within these region of interest. Among the genes are MMPs 1, 3, 8, 10, 12, 13, 20, 27 on chromosome 11 and zinc finger proteins on chromosome 19 that present as interesting biological candidates. Given the number of genes at these loci we elected to submit the DNA for whole exome sequencing with focus on primary analysis in these LOD score regions.
Conclusion: Regions in chromosome 11 and 19 demonstrated enriched sharing in patients with familial varicose veins. Both harbor interesting biological candidates and an in-depth search for varicose vein susceptible variants and genes is underway using next generation sequencing technology.
Clinical science/epidemiology – Arterial and aortic disease Poster 11
A case report of diffuse large B-cell lymphoma involving the abdominal aorta
Mahyar Khaleghi, Raymond C Shields, Manju Kalra
Mayo Clinic, Rochester, MN, USA
Background: Inflammatory abdominal aortic aneurysms are rare and often present with significant symptoms. We present a case report of a symptomatic inflammatory aneurysm associated with B-cell lymphoma.
Methods: This is a case report of a 74-year-old male who presented with back pain, 40 lb of weight loss over 6 months, and rapidly expanding abdominal aortic aneurysm. Abdominal CTA showed significant mural thrombus in the aneurysm at 4.8 cm compared to 2.8 cm in 2 months. NMPET/CT showed hypermetabolism in abdominal aortic aneurysm plus the mesenteric and renal arteries. Due to worsening pain and rapid enlargement of the saccular aneurysm, concerning for mycotic aneurysm, he underwent an open juxtarenal aortic aneurysm repair with debranching to celiac artery, superior mesenteric artery, and renal arteries, and replacement with a 16-mm tube graft.
Results: The procedure was successful without any major complications. Pathologic examination revealed a diffuse large B-cell lymphoma in the setting of Epstein-Barr virus positivity within the thrombus in the aortic aneurysm as well as part of the aortic wall. The lesion appeared to have been completely excised at surgery. Further workup, including a bone marrow biopsy, was negative. The patient was started on chemotherapy with R-CHOP regimen for stage IAE large B-cell lymphoma affecting abdominal aorta. The patient has been doing well after six cycles of chemotherapy.

Conclusion: To our knowledge, this is the first reported case of a large B-cell lymphoma affecting the abdominal aorta and highlights the importance of close monitoring and a broader differential of a symptomatic rapidly expanding aneurysm.
Poster 12
Poster 13
Brachial artery fibromuscular dysplasia: A case series
Jonathan West, Nicholas Hendricks, Alan Matsumoto, Aditya M Sharma
University of Virginia, Charlottesville, VA, USA
Background: Fibromuscular dysplasia (FMD) is a noninflammatory arteriopathy that has multiple different angiographic appearances. FMD can involve multiple vascular beds and typically involves renal arteries and cerebrovascular arteries. FMD of the brachial artery is a rare entity with only a handful of case reports in the literature. We present a case series of patients with brachial FMD.
Methods: We queried our database at University of Virginia from March 2008 to December 2013 to identify patients with brachial FMD and a retrospective chart review was performed.
Results: Of the 225 patients, 7 patients had brachial FMD: 6/7 were women. Brachial FMD was diagnosed with CT or invasive angiogram in six patients and one was diagnosed with duplex ultrasonography. Four were symptomatic: 3 presenting with embolic event and 1 with claudication. All symptomatic patients underwent angioplasty with some or complete relief of symptoms. Identification of 2/3 asymptomatic patients was by brachial bruit confirmed with imaging and 1 was incidentally diagnosed on imaging. Age ranged from 29 to 68 years, with delays between initial FMD diagnosis in other vessels and diagnosis of brachial FMD from 0 days to 9 years. Four of 7 patients had FMD in multiple arterial beds ranging from 2 to 6 different beds and all were multifocal in appearance. All of them had hypertension with 4 diagnosed with renal FMD. One patient had a cervical dissection and 1 had a radial pseudoaneurysm.
Conclusion: Brachial FMD is a rare, easily overlooked finding, but can be clinically important. A thorough examination including assessing for brachial bruits and obtaining blood pressure in both arms is extremely vital in this group of patients.

Poster 14
Predictors of clinical outcome among patients with Marfan syndrome undergoing aortic aneurysm repair at the Philippine Heart Center
Gertie May B Plameras, Rosella Arellano
Philippine Heart Center, Quezon City, Philippines
Marfan syndrome (MFS) is an autosomal dominant connective tissue disorder having multisystem involvement, particularly the cardiovascular, ocular and skeletal systems. Thoracic aortic aneurysm with Stanford A dissection is one of the most common presentations and the primary cause of mortality among these patients. The objective of this study is to determine the predictors of in-hospital mortality and morbidity among MFS patients who underwent aneurysm repair at the Philippine Heart Center (PHC). This is a retrospective cohort study which reviewed the records of MFS patients seen at the PHC from 2000 to 2010. A total of 33 charts were retrieved for analysis. Among the clinical characteristics, age (p=0.044) and length of hospital stay (p=0.026) significantly predict clinical outcome. In-hospital mortality rate was 9% (3/33). In-hospital complications occurred in 63.63% (21/33) of patients. These include pulmonary complication, particularly pneumonia (52.4%), arrhythmia (23.8%), stroke (14.3%), renal failure (14.3%), wound infection (14.3%), bleeding (9.5%), pericardial effusion (9.5%) and psychosis (9.5%). Age and length of hospital stay are predictive of in-hospital morbidity and mortality among MFS patients who underwent aortic repair at the PHC.
Clinical science/epidemiology – Clinical trials Poster 43
Live video diet and exercise intervention in overweight adolescents and vascular health
Susan Nourse1, Inger Olson1, Rita A Popat1, Katie J Stauffer1, Chau Vu1, Samuel Berry1, Jeffrey Kazmucha1, Olga Ogareva1, Sarah C Couch2, Elaine M Urbina2, Elif Seda Selamet Tierney1
1Stanford University, Palo Alto, CA, USA; 2University of Cincinnati, Cincinnati, OH, USA
Background: Atherosclerosis begins in childhood and is accelerated by obesity, altered lipid profile and sedentary lifestyle. Success of pediatric diet and exercise intervention is hindered by low adherence rates. Advances in live video technology allow supervised programs to extend into households. This study evaluated feasibility and impact of a live video diet and exercise intervention on vascular and functional health in overweight adolescents.
Methods: Adolescents with BMI >85%ile were included. The 12-week intervention included one-on-one videoconference sessions with a trainer (3× week) and weekly diet consultations. Vascular and functional health indices including pulse wave velocity (PWV), augmentation index, reactive hyperemia index (RHI), carotid artery stiffness, cardiopulmonary exercise testing, functional movement screening (FMS) and fasting lipid levels were measured at baseline and study end.
Results: 16 adolescents were enrolled (14.7±2.1 years, BMI 96.2±4.8%ile). 14 participants completed the program (88%), attending 95±6% of sessions. Significant changes were observed in total and low-density cholesterol (160±29 vs 147±26 mg/dL, p=0.005 and 90±21 vs 79±18 mg/dL, p=0.005, respectively), maximum heart rate (193±18 vs 185±19 bpm, p=0.005), and FMS score (13±2 vs 17±1, p<0.001). Participants with abnormal baseline RHI or PWV (RHI<1.9; PWV>4.6 m/s) showed significant improvement (1.5±0.2 vs 2.1±0.8, p=0.03 and 5.8±1.0 vs 4.7±0.9 m/s, p=0.04, respectively).

Conclusion: A 12-week live video diet and exercise intervention is feasible with excellent compliance and improves vascular and functional health of overweight adolescents. Telehealth could herald a new era of effective preventive care in this population.
Clinical science/epidemiology – Endovascular therapies Poster 16
Assessment of procedural stroke etiology in carotid artery stenting
Andrew Higgins1, Adam Castano1, James Wilentz2, William Gray1, Ali Aboufares1
1Columbia University Medical Center, New York, NY, USA; 2Weill Cornell Medical Center, New York, NY, USA
Background: Carotid angioplasty and stenting (CAS) has emerged as a viable alternative to carotid endarterectomy (CEA) for stroke prevention in patients with carotid stenosis. Although the mechanisms of procedural stroke in CAS remain poorly understood, preliminary analysis suggests they are attributable to operator error or high-risk patient / lesion selection; however, the relative frequency of different errors has yet to be established.
Methods: Core-lab procedural angiograms from the EMPiRE, ARMOUR, EMBOLDEN, and PROTECT trials were obtained for every patient with a study-adjudicated CVA (n=29) along with a similar number of non-stroke controls (n=34). Three blinded interventionalists individually reviewed each angiogram for quality of angiography, lesion characteristics, and potential operator error (inadequate flow cessation/reversal, problematic balloon sizing or filter deployment) and mechanism of stroke.
Results: Preliminary analysis demonstrates an identifiable potential error in 33% of cases: 57% of those had a CVA. The most commonly identified error among all cases was wire / stent manipulation (23% of errors); one such case is shown in the Figure below. In proximal protection cases, insufficient ECA occlusion was observed in 44% of identified errors, while inadequate flow cessation / reversal was observed in 32%. In distal protection cases, filter non-deployment or deployment on angulation / bend was observed in 30%.
Conclusion: Although operator error had been suggested as a major risk factor for CVA in CAS, the findings here illustrate that this mechanism is dominant, suggesting that the safety profile of CAS could potentially be further improved with operator training. Device failure was not significantly implicated as an etiology of CVA in our analysis.
Poster 17
Assessing the rate of inferior vena cava filter use and retrieval
Olusegun Osinbowale1, Syed Ahsan2
1Ochsner Clinic, New Orleans, LA, USA; 2Henry Ford Health System, Detroit, MI, USA
The American College of Chest Physicians recommends treatment with anticoagulation for all cases of acute deep vein thrombosis (DVT) and pulmonary embolism (PE). The introduction of inferior vena cava filters (IVCFs) and the ease of insertion have spurred their use without strong evidence or follow-up to assess either efficacy or longer-term clinical outcomes. Despite decreased PE incidence, increased rates of proximal DVT and lack of overall mortality benefit after IVCF placement, have called attention to device utilization and outcomes. The present abstract reports findings from a chart review of subjects who received an IVCF within the Ochsner Health System in New Orleans, LA from December 2008 through December 2011. During this interval, 443 IVCFs were successfully deployed. The most common associated diagnoses were acute lower extremity DVT (24.2%) and pulmonary embolism/infarct (18.7%). History of venous thrombosis/embolism, prophylaxis for treatment measure and prophylactic measure NEC (not elsewhere classified) accounted for 8.8%, 8.8% and 5.9% of cases, respectively. 10% of IVCFs were successfully retrieved, with a failure rate of 1.8% due to thrombus in filter or technical considerations. Retrieved filters were in place for a mean duration of 110 days. Documentation to leave the filter in place was present in 5.6% of cases. Notably, 20.5% of subjects carried a diagnosis of active malignancy. Contraindication to anticoagulation or abnormal coagulation profile was rarely coded as primary or secondary indications for filter placement. The current findings suggest that IVCF retrieval and surveillance remain inadequately performed or documented despite routine device use. Notwithstanding the limited generalizability of this single-center retrospective chart review, further longitudinal research into clinical outcomes including rates of recurrent venous thromboembolism (VTE) and VTE-related anticoagulation may beneficially impact patient care.
Poster 18
Outpatient ultrasound-guided thrombin injection of post-catheterization pseudoaneurysm is safe and effective
David L Ain1, Phillip A Erwin2, Susan Gustavson1, Qi Zheng3, Victoria Teodorescu1, Jeffrey W Olin1
1Icahn School of Medicine at Mount Sinai, New York, NY, USA; 2Cleveland Clinic, Cleveland, OH, USA; 3Albert Einstein College of Medicine at Montefiore Hospital, New York, NY, USA
Background: Femoral artery pseudoaneurysm (PSA) is a known complication of cardiac catheterization. Ultrasound-guided thrombin injection (UGTI) for treatment of post-procedure PSA has been shown to be safe and effective, but its use in the outpatient setting has not been evaluated.
Methods: A retrospective analysis from the vascular laboratory database was performed in patients who had undergone UGTI for treatment of post-catheterization PSA from 2003 to 2012 to determine if PSA can be safely treated by UGTI in the outpatient setting.
Results: UGTI was performed in 360 patients: at the time of the first UGTI, 259 were inpatients and 101 were outpatients. The patients successfully treated as an outpatient were allowed to leave the vascular laboratory as soon as the procedure was completed. On average, 0.6 cc of thrombin was injected. Immediate post-procedure success, defined as complete PSA thrombosis by ultrasound, was >99% for both groups (Table). There was no difference in procedural success or complications between patients treated as inpatients or outpatients.

Conclusions: Post-catheterization PSA can be safely and effectively treated with UGTI in the outpatient setting. These results have important implications for containment of hospital patient length of stay and associated costs.
Poster 19
Venous balloon modulation of autonomic function, initial assessment and safety
Michael Arata
Synergy Health Concepts, Newport Beach, CA, USA
Background: Patients undergoing central venous angioplasty (CVA) have demonstrated improvement in autonomic parameters, perhaps a result of low pressure baroreceptor stimulation during balloon inflation. This report describes the autonomic effect of CVA and safety of this approach.
Methods: 131 patients exhibiting symptoms of ANS dysfunction were treated and assessed by HRV analysis. Dilation of each central vein (internal jugular, azygos and renal veins) occurred regardless of the presence of vascular abnormalities. The effect upon ANS function was indicated by HRV parameters as the outcomes of interest. Data are presented as mean±SD. The distribution of each parameter was checked for normality. The before and after measurements of each parameter were compared using paired t-test for normal distribution and Wilcoxon signed rank test for skewed distribution. All statistical testing was performed at a two-sided 5% level of significance and used Statistical Analysis System version 9.3 software (SAS Institute, Cary, NC).
Results: The TVAM procedure was successfully completed in all cases (technical success 100%). Post-treatment HRV analysis demonstrated an objective response by increases in MCR, E/I and postural components, MCR reaching statistical significance of 0.75±2.1, p<0.01. Acute adverse events did not occur during any of the procedures.
Conclusion: The ANS effect of CVA was demonstrated by HRV analysis, and the procedure appears safe. Validation and elucidation of this effect is warranted in light of the lack of definitive treatment options for autonomic dysfunction patients.
Poster 20
Case report: Successful endovascular repair of a spontaneous superficial femoral artery dissection
Victoria Fasick, Vasu Sunkara, Para Yoges-Waran, Nishant Koradia, Matthew Becker
St Vincent Medical Center, Erie, PA, USA
Spontaneous dissection of the superficial femoral artery (SFA) is rare. We present a case with a novel treatment option. A 59-year-old male with a history of HTN, smoking, DM and a chronic non-healing ulcer of the L calf was referred for angiography. Standard PA aortography and L lower extremity arteriography were performed via access through the R common femoral artery (CFA). We discovered a spontaneous ‘double barrel’ dissection originating at an atheromatous plaque in the proximal SFA and extending beyond the popliteal artery into the anterior tibialis (AT) artery. Notably, the tibioperoneal (TP) trunk and posterior tibialis arteries (PTA) were supplied entirely by the false lumen. Technical challenges to percutaneous revascularization in this case included performing angioplasty and stenting the true lumen without closing the false lumen and compromising flow to the TP trunk and PTA. To achieve this, we passed a 0.014” Command ES 3 wire through the SFA lesion into the AT true lumen and dilated with an Ultraverse 4 mm balloon. Although significant improvement was gained, flow persisted in both lumens. Fenestration of the dissection flap and entry into the TP trunk was achieved with an Outback re-entry catheter. Dilation of the fenestration with a 5×2 cm Rival balloon resulted in antegrade flow into the TP trunk through the true lumen. Two SUPERA stents were placed from the distal popliteal to SFA, covering the proximal atheromatous lesion. Final angiography and IVUS revealed excellent stent apposition and flow into both AT and TP. The patient was given antiplatelet therapy and discharged home. At the 2-month follow-up, there was complete resolution of the wound.

Pre- and post-procedure comparison of HRV parameters.

Paired t-test.
Wilcoxon signed rank test.
Clinical science/epidemiology – Exercise physiology Poster 21
Exercise training significantly reduces TNF
α
in patients with diabetic kidney disease
Ulf G Bronas, Dereck Salisbury, Daniel Duprez, Diane Treat-Jacobson, Mark Rosenberg
University of Minnesota, Minneapolis, MN, USA
Background: We have previously reported that exercise training significantly improves vascular function in patients with stage 2–4 diabetic CKD (DKD). TNFα appears to mediate signaling processes that initiate vascular inflammation, induce oxidative stress and reduce nitric oxide bioavailability. This study tested the hypothesis that exercise training would reduce plasma levels of TNFα in patients with stage 2–4 DKD. We further postulated that the change in TNFα would be associated with changes in markers of oxidative stress (F2-isoprostane), and the eNOS inhibitor ADMA.
Method: Secondary analysis of a randomized controlled trial involving 91 participants (62 male, age 64.1±9.2 yrs) with stage 2–4 DKD completing either 12 weeks of moderate-intensity walking exercise training, 4×/wk for 45 minutes (n=46) or a usual medical care control group (n=45).
Results: At 12-week follow-up, group comparisons were analyzed by ANCOVA using baseline, age, and weight change as covariates. TNFα was significantly reduced by −0.09 pg/mL (95% CI −0.20 to 0.03) in the exercise-intervention group vs an increase of 0.12 pg/mL (95% CI 0.02 to 0.23) in the control group. Mean difference between groups was 0.21 (±0.08) pg/mL (p=<0.012, 95% CI −0.37 to −0.05). Levels of TNFα were strongly correlated with ADMA (r=0.57, p=<0.001) and oxidative stress (r=0.42, p=<0.001) at 12 weeks. Change in TNFα was moderately correlated with change in oxidative stress (r=0.32, p=0.05) in the exercise group only.
Conclusion: This study demonstrates for the first time that walking exercise training reduces TNFα in patients with DKD. The reduction of TNFα was associated with reduced levels of oxidative stress, providing insight into one of the mediating links of the apparent vascular benefits of exercise in this population.
Poster 22
Exercise training reduces interleukin-8 in patients with diabetic kidney disease
Ulf G Bronas, Dereck Salisbury, Daniel Duprez, Diane Treat-Jacobson, Mark Rosenberg
University of Minnesota, Minneapolis, MN, USA
Background: Systemic inflammation is known to cause metabolic, biochemical, and hemodynamic derangements that contribute to the etiology and progression of diabetic kidney disease (DKD). Interleukin-8 (IL-8) has emerged as important inflammatory mediator in the pathogenesis and exacerbation of DKD, contributing to the development of glomerulosclerosis. The purpose of this study was to test the hypothesis that IL-8 is a potential mediator in the apparent anti-inflammatory effect of exercise.
Method: In an exploratory analysis, plasma levels of IL-8 were obtained in a subsample (n=39, 26 males, age 64.5±8.8 yrs) of participants enrolled in a randomized, controlled trial investigating the effect of walking exercise training, 4×/wk for 45 minutes, on vascular function in participants with stage 2–4 DKD.
Results: There were no differences between groups in baseline demographic, medical, or pharmacological variables. At 12-week follow-up, group comparisons were analyzed by ANCOVA using baseline as a covariate. IL-8 was significantly reduced from 7.65 (±8.6) pg/mL to 5.32 (±4.0) pg/ml in the intervention group (n=21), with a mean difference in IL-8 of 4.25 pg/mL between groups (p=0.044, 95% CI −8.38 to −0.12). IL-8 was strongly correlated with TNFα (r=0.51, p.001), IL-6 (r=0.60, p=<0.001), and moderately correlated with hs-CRP (r=0.33, p<0.044) at 12-week follow-up.
Conclusion: This study demonstrates for the first time that walking exercise training reduces IL-8 in patients with DKD, supporting an apparent exercise-induced reduction in systemic inflammation. The strong association between IL-8 and markers of inflammation suggests that IL-8 is an important mediator in the apparent anti-inflammatory effect of exercise in this population.
Clinical science/epidemiology – Imaging Poster 23
Feed-forward active contour analysis for improved brachial artery reactivity testing
Daniel N Pugliese, Chandra Sehgal, Courtney Reamer, Laith R Sultan, Emile R Mohler
University of Pennsylvania, Philadelphia, PA, USA
Background: Flow-mediated dilation (FMD) is an important marker of vascular endothelial function, but it has not been adopted for more widespread clinical use due to technical limitations, including inter-observer variability and differences in technique across clinical sites. We developed a novel feed-forward active contour (FFAC) algorithm with the goal of validating a more reliable standard.
Methods: 46 healthy volunteers underwent brachial artery reactivity testing according to standard technique. Video clips of ultrasound images lasting 5 seconds each were obtained pre-cuff inflation and at minutes 1 through 5 after cuff deflation in both sagittal and transverse views. Automated segmentation using the FFAC algorithm with initial boundary definition from three different observers was used to segment the image sequences to measure artery diameter or cross-sectional area profile over the cardiac cycle. Flow-mediated dilation percentage (FMD) was calculated for average diameters and areas, as well as for minimum and maximum values.
Results: The application of FFAC to calculate FMD using transverse views at end-diastole yielded an average coefficient of variation (CV) of 24.1% compared to 65.1% (p=1.58E-06) using sagittal views. Transverse FFAC also yielded decreased variability in FMD analysis with average and maximum measurements over the cardiac cycle (p=2.76E-06 and 5.03E-06).
Conclusions: Transverse views using the novel FFAC method provide less inter-observer variability than traditional sagittal views when assessing FMD. Improved reproducibility may allow adoption of brachial artery reactivity testing in a clinical setting.
Results: summary.

Poster 25
Comparison of angiographic features of superficial femoral artery disease in diabetics and non-diabetic patients
Atif Mohammad1, Avantika Banerjee2, Karan Sarode1, Gene Pershwitz2, Subhash Banerjee1
1UT Southwestern Medical Center, Dallas, TX, USA; 2VA North Texas Health Care System, Dallas, TX, USA
Background: There are limited data regarding distribution and severity of atherosclerotic peripheral arterial disease in diabetics (DM) and non-diabetics (non-DM) despite differences in outcomes following superficial femoral artery (SFA) revascularization.
Methods: We conducted a blinded analysis of peripheral angiograms of 489 patients (282 DM and 207 non-DM) enrolled in the XLPAD registry between July 2005 and October 2013 with Rutherford category ≥3 symptoms.
Results: Mean age was 63.8 years. DM had greater distal SFA involvement than non-DM (48% vs 19%; p<0.001) and multi-level SFA disease (59% vs 38%; p=0.01). DM had more severe (grade 3) calcification (81% vs 65%, p=0.03), and similar frequency of total occlusions (67% vs 65%, p=0.70) and lesion lengths (129±76 mm vs 123±67.7 mm, p=0.35). SFA lesion severity by Bollinger score in DM vs non-DM was 14.0±2.1 and 12±4.7, p<0.001. Number of run-off vessels with ≥50% stenosis was 2.3 for non-DM vs 2.0 for DM (p=0.01). Stent implant rate (DM=74% vs non-DM=71%; p=0.58) and lengths (115.0±47.8 mm vs 107.0±43.4 mm; p=0.09) were similar in both groups. Clinical outcomes at median follow-up of 240 days are shown in the Figure. There was a strong trend towards higher amputations in DM.
Conclusions: SFA disease in DM is more distal, with greater severity of calcification and is more likely to have multi-level involvement, contiguous with below the knee vessels compared to non-DM.

Poster 26
Carotid duplex ultrasound is the highest yield diagnostic test for the detection of subclinical atherosclerosis in a screening population
Esther SH Kim1, Raul Seballos2, Richard Lang2, Roxanne Sukol2, Steven Feinleib2, Alice Chen2, Kristen Bede2, Ruchi Sanghani2, Neil Poria2, Heather L Gornik2
1Cleveland Clinic, Avon, OH, USA; 2Cleveland Clinic, Cleveland, OH, USA
Introduction: Non-invasive screening programs for the presence of atherosclerotic vascular disease typically include a carotid duplex ultrasound (CDU), abdominal aortic ultrasound for detection of aneurysm (AAA), and the ankle–brachial index (ABI). We sought to investigate the relative yield of these tests for detecting subclinical atherosclerosis.
Methods: The Executive Health Program at the Cleveland Clinic offers comprehensive physical examination and diagnostic testing to assess overall wellness. Vascular screening in the form of a limited CDU to assess for carotid plaque, duplex ultrasound to assess for AAA and aortic plaque, and an ABI is performed as a part of this program. We queried the Non-Invasive Vascular Laboratory database for all patients who underwent vascular screening from 2/18/2011 to 5/23/2013. Carotid plaque was defined as arterial wall thickening ≥50% greater than the adjacent segment or measuring >1.5 mm, significant carotid stenosis was defined as peak systolic velocity >150 cm/sec, AAA was defined as an aortic diameter ≥3 cm or doubling of diameter in adjacent segments, and an abnormal ABI was defined as ABI ≤0.90 or ≥1.40. Patients with known atherosclerotic disease were excluded from analysis.
Results: 1232 patients underwent vascular screening over a 27-month period (Table). 135 patients were excluded due to known atherosclerotic disease. 78.1% were male, mean age 57.6 (±7.5) years, mean BMI 28.6 (±5.5), mean waist circumference 96.1 (±14.6) cm. 50.1% (546/1091) of patients had carotid plaque on either side with or without carotid stenosis. 0.83% (9/1090) had hemodynamically significant carotid stenosis. 22.4% (237/1057) of patients had aortic plaque, 1.52% (16/1054) had aortic aneurysm, and 0.37% (4/1084) had an abnormal ABI.
Conclusions: In a population of healthy middle-aged patients without known cardiovascular disease, half have carotid plaque detected on screening CDU. In a screening program including CDU, AAA screen, and ABI, CDU for presence of plaque is of highest yield.
Demographic and clinical characteristics.

Clinical science/epidemiology – Thrombosis and hemostasis Poster 27
Outcomes of platelet transfusion in patients with heparin induced thrombocytopenia: A case series
Chompunut Asava Aree, Lee Joseph, John R Bartholomew
Section of Vascular Medicine, Department of Cardiovascular Medicine, Cleveland Clinic, Cleveland, OH, USA
Introduction: There is limited and often conflicting evidence regarding the safety of platelet transfusion in patients with heparin induced thrombocytopenia (HIT) and it is often considered contraindicated for concerns that it may precipitate thrombosis. We present, to our knowledge, the largest series of patients with serologically proven HIT who received platelet transfusions during their acute illness, and their outcomes.
Methods: We retrospectively reviewed medical records from our registry of 56 patients with confirmed HIT, who received platelet transfusion within 30 days after their diagnosis.
Results: Sixteen of 56 patients with confirmed HIT received platelet transfusion within 30 days after diagnosis. The mean age was 66.6±15.3 years. Fifteen patients (93.8%) were critically ill. Platelets were transfused within an average of 2.5±6.1 days of diagnosis, and 13 patients (81.25%) received platelet transfusion within 48 hours. Indications for platelet transfusion included: bleeding control (9 patients, 56.3%), pre-procedural prophylaxis (6 patients, 37.5%) and postoperative prophylaxis (1 patient, 6.3%). The mean pre-transfusion platelet count was 41.5±28.0 K/ul and mean post-transfusion platelet count was 54.1±31.3 K/ul. Nine patients (56.3%) developed a total of 12 post-transfusion thrombosis (mean 6.1 days after platelet transfusion), which included: 6 DVTs; 1 superficial venous thrombosis; 1 pulmonary embolism; 1 arterial thrombosis requiring below knee amputation; 1 left ventricular thrombus; 1 splenic infarction; and 1 stroke. The 30-day all-cause mortality rate was 37.5% (6 patients); however, none were related to platelet transfusion.
Conclusion: Our series demonstrates that platelet transfusion is associated with a high risk for thrombotic complications in patients with acute HIT, particularly within the initial 2 days of diagnosis. It should be administered in such patients with caution and only after thorough consideration of the risks and benefits.
Poster 28
The incidence of peripherally inserted central catheter pulmonary embolism after line removal: A retrospective review
Omar L Esponda1, Julia L Reffert2, Matthew L Bird2, Winter J Smith2, Donald L Harrison2, Suman Rathbun1
1OUHSC, Department of Medicine, Cardiovascular Section, Oklahoma City, OK, USA; 2OUHSC, University of Oklahoma College of Pharmacy, Oklahoma City, OK, USA
Background: PICC (peripherally inserted central catheter) associated deep vein thrombosis (DVT) accounts for up to 35% of all diagnosed upper extremity DVT (UEDVT) with 2–36% developing pulmonary embolism (PE); however, to date, there are no recommendations regarding the timing of removal of PICC lines in the presence of confirmed UEDVT. We aim to determine the incidence of PE in patients with PICC-associated UEDVT according to treatment strategy.
Methods: We conducted a retrospective cohort study at our 400-bed academic hospital. Adult patients who received a PICC in 2011 with documented UEDVT or superficial thrombosis (UESVT) by vascular ultrasound were included. Patients’ demographic characteristics, co-morbid disease states, medications, ultrasound findings, treatment strategy for UEDVT/SVT and occurrence of symptomatic PE after line removal was recorded.
Results: 124 patients had PICC-associated UEDVT or UESVT; 60 males and 64 females with mean age 52.2 years, 71 patients with UEDVT and 34 patients with UESVT. Of these, 59 patients had not received pharmacologic prophylaxis. Of 105 patients with follow-up information available, there were no episodes of symptomatic PE documented after PICC line removal. Regarding timing of removal, 30 patients had their PICC line removed within 24 hrs after UEDVT diagnosis (0 of 30, 95% CI 0.00–0.115), 28 patients within 1 week (0 of 28, 95% CI 0.00–0.123), 15 patients within 2 weeks (0 of 15, 95% CI 0.00–0.218), 21 patients within 1 month (0 of 21, 95% CI 0.00–0.161) and 10 patients at more than a month (0 of 10, 95% CI 0.00–0.308) after diagnosis of UEDVT. One patient had PE the day after diagnosis of PICC-associated UEDVT while the PICC was still in place.
Conclusion: This retrospective analysis reveals a low rate of PE with removal of PICC in the presence of UEDVT or UESVT if performed within 24 hrs, and an overall low rate of PE events regardless of treatment strategy and duration of PICC insertion. These findings are hypothesis generating and should be confirmed in a prospective trial.
Clinical science/epidemiology – Vascular medicine Poster 29
Family history as a risk factor for carotid artery stenosis
Mahyar Khaleghi, Iyad Isseh, Hayan Jouni, Kent R Bailey, Iftikhar J Kullo
Mayo Clinic, Rochester, MN, USA
Background: Identifying patients who benefit from screening for carotid artery stenosis (CAS) is an important strategy for prevention of ischemic stroke. We investigated whether family history of stroke or coronary heart disease (CHD) is associated with presence of CAS, independent of conventional risk factors.
Methods: The study cohort included 864 patients (72±8 y, 68% men) with severe CAS and 1698 controls (61±11 y, 55% men) referred for non-invasive vascular evaluation. Severe CAS was defined as having ≥70% stenosis in the internal carotid artery ultrasound or history of carotid artery revascularization. Controls were patients without severe CAS or history of cerebrovascular disease or CHD. Family history of stroke and CHD was obtained using a detailed questionnaire and defined as having at least one first-degree relative who had stroke or CHD before age 65. Logistic regression analyses were used to evaluate whether family history of stroke or CHD were associated with presence of CAS, independent of conventional risk factors.
Results: Family history of stroke and CHD was present more often in severe CAS patients than in controls (19.8% and 50.6% vs 10.9% and 33.7%, respectively) with a resulting odds ratio (OR) (95% confidence interval) of 2.02 (1.61–2.53) and 2.01 (1.70–2.37), respectively. The associations were weakened but remained significant after adjustment for age, sex, body mass index, smoking, diabetes, hypertension and dyslipidemia; ORs: 1.41 (1.06–1.90) and 1.69 (1.35–2.10), respectively. A greater number of affected relatives with stroke or CHD was associated with higher odds of CAS; adjusted ORs: 1.25 (0.91–1.72) and 1.46 (1.14–1.89) vs 2.65 (1.35–5.40) and 2.13 (1.57–2.90) for patients with 1 and ≥2 affected relatives with stroke and CHD, respectively.
Conclusion: Family history of stroke or CHD is associated with presence of severe CAS independent of conventional risk factors. Further work is needed to assess the utility of screening with carotid ultrasound for patients with positive family history.
Poster 30
Optimal medical therapy in patients with atherosclerotic peripheral vascular disease
Aditya M Sharma, Karnika Ayinapudi, Divya Srinivasan, Brian Annex, Gilbert Upchurch
University of Virginia, Charlottesville, VA, USA
Introduction: Peripheral vascular disease (PVD) is a polyvascular disease with a 5-year mortality of >15%. Appropriate medical therapy can significantly improve their cardiovascular (CV) outcomes. We aim to obtain compliance with optimal medical therapy in patients (PTS) with atherosclerotic PVD admitted to the vascular service at University of Virginia.
Methods: Retrospective chart review of PTS admitted to vascular service was performed.
Results: Between August 1st 2012 to June 30th 2013, 583 unique PTS were admitted to the vascular service. 61% were male and 76% were ≤75 years of age. 62% had lower extremity peripheral arterial disease (LEPAD), 28% had extracranial carotid artery disease (ECAS) and 48% had coronary artery disease (CAD). 48% of PTS with LEPAD had CAD and 66% of PTS with ECAS had CAD. 35% smoked and 39% had diabetes. 21% of diabetics had sub-optimal control of diabetes. Only 22% had LDL >70 mg/dl. Among PTS ≤75 years, only 23% were on high-intensity statins and among PTS >75 years, only 54% were on either high/moderate-intensity statins. PTS were more likely to be on a high-intensity statin especially if they had CAD compared to those without known CAD (30% vs 14%, p-value <0.0001). 86% of PTS were on antiplatelets. Only 54.7% of PTS were on ACEI/ARB within 6 months of date of admission. However, use of ACEI/ARB was higher when PTS had known concomitant CAD (63% vs 48%, p-value = 0.0064).
Conclusion: Although PTS with PVD are high risk for CV morbidity and mortality, compliance with appropriate medication is suboptimal. Multidisciplinary care including preventive vascular medicine specialist are necessary to provide optimal care.
Statin use in patients with atherosclerotic peripheral vascular disease.

Poster 31
Adherence to guideline-recommended therapies among patients with diverse manifestations of vascular disease
Debbie C Chen1, Ehrin J Armstrong2, Gagan D Singh1, Ezra A Amsterdam1, John R Laird1
1University of California, Davis, Sacramento, CA, USA; 2University of Colorado, Denver, CO, USA
Background: Current treatment guidelines recommend aspirin, statins, angiotensin-converting enzyme inhibitors (ACEI), and smoking abstinence for all patients with vascular disease. There is little data on the variation in adherence to guideline-recommended therapies among patients with different clinical manifestations of vascular disease.
Methods: We analyzed a comprehensive database of all patients with critical limb ischemia, claudication, acute limb ischemia (ALI), carotid artery stenosis, subclavian stenosis, renal artery stenosis, and mesenteric ischemia who underwent angiography between 2006 and 2013 at a vascular center.
Results: Among 1114 patients with vascular disease, adherence to guideline-recommended therapy at time of angiography included use of aspirin in 936 (84%), statins in 753 (68%), ACEIs in 673 (60%), and smoking abstinence in 788 (71%). A total of 335 (30%) patients met all four guideline-recommended therapies. Adherence to four guideline-recommended therapies was lowest among patients with ALI (14%) and highest among patients with renal artery stenosis (37%). Among patients with diverse manifestations of vascular disease, the range of adherence to individual guideline-recommended therapies was 64–91% for aspirin, 43–83% for statins (Figure), 49–66% for ACEIs, and 47–78% for smoking abstention.
Conclusions: The majority of patients with diverse manifestations of vascular disease take aspirin and abstain from smoking, while fewer patients are prescribed ACEIs and statins. While statin prescription is on average 66%, there is greatest variation in statin use. Less than 50% of patients with diverse manifestations of vascular disease are prescribed all four guideline-recommended therapies. Further study of the impact of adherence to guideline-recommended therapies in this patient population is required.

Poster 33
Major tissue loss in critical limb ischemia is associated with left ventricular systolic dysfunction and left atrial enlargement
Sarah Elsayed, Nicole Basler, Christos Theophanous, Parveen Garg, David Shavelle, Leonardo Clavijo
University of Southern California, Los Angeles, CA, USA
Background: Critical limb ischemia (CLI) is associated with high cardiovascular morbidity and mortality. However, a detailed evaluation of left ventricular (LV) function has not been previously described. A better understanding of LV function in CLI patients undergoing vascular surgery may help to improve perioperative care. The aim of this study was to determine the prevalence of systolic and diastolic dysfunction in CLI patients.
Methods: We performed a retrospective study of 116 patients with CLI admitted to a single academic center who all underwent 2D and M-mode transthoracic echocardiography. Demographic and clinical variables were collected including Rutherford class and cardiac risk factors. Among the relevant echocardiography data to determine LV ejection fraction (EF) and diastolic dysfunction (DD) grade, were Simpson’s modified biplane apical 4 chamber and 2 chamber, left ventricular end diastolic and systolic volumes, left atrial size, and mitral valve inflow E/A ratio.
Results: Of these 116 CLI patients, 78 were Rutherford class 4/5 and 38 were class 6 (Table). 27 (23%) were found to have systolic dysfunction. 12 (10.3%) had EF 41–50% (mild), 9 (7.7%) with EF 30–40% (moderate), and 6 (5%) with EF less than 30% (severe). Rutherford class 4/5 patients had more normal systolic function: 66 (84%) compared with 23 (60.5%) class 6 patients (p=0.004). In regards to diastolic dysfunction, 71 (61%) had grade I–II (mild), 13 (11%) had grade II–III (moderate), and 14 (12%) had grade III–IV (severe). Mean left atrial volume index was 28.6±9.3 ml/m2 in the Rutherford 4/5 group and 34.4±11.7 ml/m2 in the Rutherford 6 group (p=0.007).
Conclusion: LV systolic and diastolic dysfunction are prevalent in patients with CLI. Major tissue loss (Rutherford class 6) is associated with worse LV systolic function and larger left atrial size compared to minor tissue loss and rest pain. This can have a direct impact on the operative risk in these patients. Prospective studies are necessary to confirm these findings and assess clinical impact.

Poster 34
International training workshop on ‘Fundamentals in Clinical Vascular Medicine’ for physicians in Hiche, Haiti
Jessica Mintz1, Jennifer Furin2, Sandra Yesenko1, Heather Gornik1, Bruce Mintz3
1Cleveland Clinic, Cleveland, OH, USA; 2Case Western Reserve University, Cleveland, OH, USA; 3St Clare’s Riverside Medical Center, Denville, NJ, USA
Background: Non-communicable diseases are on the rise in resource poor settings throughout the world. These include the cardiovascular risk factors of HTN, hyperlipidemia and diabetes. With the mounting prevalence of these risk factors, peripheral vascular disease (PVD) has become a clinical problem. The aim of the project is to determine if a short educational course on the fundamentals of vascular medicine given in the central plateau of Haiti can enhance diagnosis and treatment of PVD and its risk factors.
Methods: This 5-day program in clinical vascular medicine will include comprehensive lectures, hands-on sessions for the vascular physical exam, use of hand-held Doppler, ABI and an ultrasonographic approach to vascular anatomy. Program objectives are as follows:
To train physicians in the central plateau of Haiti fundamentals in the diagnosis of PVD.
To teach physicians how to perform and interpret the ABI.
To provide locally relevant training in treatment of cardiovascular risk factors, PAD, VTE and wound care. A pre and post-test assessment will be given to all participants. After the course, participants will be asked to document all cases related to PVD in the following 6 months in an attempt to further understand PVD in the central plateau of Haiti.
Results: There has been limited training in vascular medicine and PVD in Haitian medical schools and needs assessment of providers in the central plateau indicates that further education would be helpful for their clinical practice. The program will be taught in Haiti from March 17 to March 21 2014 and findings of the pretest and post-test assessment will be presented.
Poster 35
Clinical presentation of patients at the diagnosis of premature peripheral artery disease (PAD)
Pavel J Levy, Jeanette Stafford, Matthew S Edwards
Wake Forest School of Medicine, Winston-Salem, NC, USA
Background: Severe PAD in younger adults has been diagnosed with increasing frequency. Symptoms of PAD are under-reported, often related to other more common conditions resulting in a delayed PAD diagnosis. Previous studies provided limited information on clinical manifestations of early PAD.
Methods: A prospective database of consecutive 565 patients (pts) <55 years of age at PAD diagnosis who were treated at our vascular center between 1998 and 2010 was utilized. Of these, 547 (96.8%) pts who had symptomatic PAD at diagnosis were studied. All analyzed data were available at PAD diagnosis. Simple and multivariable logistic regression models were used to evaluate associations between patient characteristics and selected PAD manifestations.

AID, aorto-iliac disease.
Results: Mean age at diagnosis was 46.6±6.9 years; 308 (56.3%) were diagnosed in our center. A total of 408 (75.8%) pts had no other cardiovascular disease preceding diagnosis of PAD (‘PAD first’); 39 (7.1%; 11.2% of females vs 3.7% of males; p<0.05) had cancer at the time of PAD diagnosis; and 60 (11.1%; 17.6% of black pts vs 9.5% of white pts; p<0.05) had systemic disease. 149 (27.2%) pts had acute leg ischemia [45 (30.2%) without prior intermittent claudication (IC)], of whom 86 (58.9%) had ‘blue toe syndrome’; and 398 (72.8%) presented with chronic symptoms of IC. 213 (39.2%) complained of chronic lower back pain (LBP) [median (IQR) 36 (24–72) months’ duration], 38.3% had depression, and 104 (21.7%) were disabled before PAD diagnosis. Multivariable regression analysis identified the following associations with various PAD manifestations (Table).
Conclusions: The vast majority of patients were symptomatic at diagnosis of early PAD, and more than ¼ presented with limb-threatening ischemia. Chronic lower back pain was common and was associated with severe AID.
Poster 36
What happens in vagus: A case of post-prandial syncope
Natalie M Ertz, Samuel Money, Joseph Hoxworth, Juliana Kling, Fadi Shamoun
Mayo Clinic, Scottsdale, AZ, USA
Introduction: Paragangliomas (PGL) are extremely rare, extra adrenal tumors originating from neuroectoderm and occur anywhere from the skull base to the pelvic floor. We report a case of an extensive, unresectable paraganglioma with a hereditary component.
Case: A 59-year-old, previously healthy woman presented with 2 weeks of post-prandial syncope, labile blood pressure, diagnosed with vasovagal bradycardia at an outside facility. She had endured a 4-month history of light-headedness and intermittent neck pain prior to her first syncopal episode. Physical exam demonstrated bilateral palpable masses under the angle of the mandible. She endorsed having this neck mass for a number of years. She also reported having a paternal family history of benign, asymptomatic, neck masses in three generations. Therefore, the mass was initially attributed to an incidental congenital anomaly not related to the syncopal episodes.
Magnetic resonance imaging revealed multiple bilateral paragangliomas extending from the carotid bifurcations to the base of the skull. The tumors engulfed the vagus nerve deeming them in-operable. The tumors were non-functional by laboratory assessment of metanephrines and catecholamines. Genetic analysis revealed a succinate dehydrogenase mutation, an autosomal dominant mutation resulting in risk of paraganglioma tumors.
Radiation therapy was selected as the best option available giving the local extension of the tumors. The patient underwent stereotactic radiation treatment of 30 Gy over 5 days with a positive response on imaging and reduced frequency of syncopal events overall.
Discussion: PGLs occurring in the head and neck are tumors of the parasympathetic division of the autonomic nervous system. PGL tumors are usually benign in nature and are cured surgically if anatomic location is permitting of intervention. More recent literature suggests stereotactic radiation therapy should be first-line therapy. Given the scarcity of cases it is likely best to consider each case on an individualized basis.
Clinical science/epidemiology – Venous disease Poster 37
Chronic venous outflow obstruction – Anatomical findings and clinical presentations
Hyoungtae E Kwon, Windsor Ting, Angeliki G Vouyouka, Michael L Marin, Peter L Faries
Icahn School of Medicine at Mount Sinai, New York, NY, USA
Chronic venous outflow obstruction in the pelvis is increasingly recognized as a contributing etiology of venous disease in the lower extremities. Better characterization of the anatomical findings among these patients and their clinical presentations may improve the diagnosis of this condition.
Methods: A retrospective single-institution review of patients with chronic ilio-femoral venous occlusive disease treated with stents from December 2012 to January 2014 was conducted.
Results: Fifty-one consecutive patients had a total of 85 stents placed for chronic ilio-femoral venous occlusive disease. Sixty-three percent of patients were male and mean age was 61 years (range 31–90). Clinical presentations included: varicose veins (with/without ulcer) 34 patients (66%), post-thrombotic syndrome (with or without ulcer) 16 patients (31%), and isolated lower extremity edema 14 patients (27%). Venogram and intravascular ultrasound showed classic May–Thurner (extra-luminal compression of the proximal left common iliac vein) 13 patients (25%), May–Thurner variant (extra-luminal compression at other locations) 8 patients (16%), both classic May–Thurner and May–Thurner variant 14 patients (27%), findings of a remote DVT (intraluminal stenosis) 16 patients (31%), both extra-luminal compression and intraluminal stenosis 13 patients (25%), intraluminal stenosis without obvious compression 3 patients (6%). Among clinical presentations, ulcer was seen in May–Thurner variants (62.5%) in a significantly higher proportion than classic May–Thurner patients (15.4%) (p=0.03).
Conclusions: In this population treated for chronic venous outflow obstruction, May–Thurner syndrome and variants of May–Thurner were the most common anatomic findings in chronic venous outflow obstruction. These patients presented with varicose veins, DVT and post-thrombotic syndrome, and isolated edema.
Poster 38
Role of new oral anticoagulants in the treatment of superficial venous thrombosis of the lower extremities
Mohsen Sharifi1, Joshua Ostrue2, Wilbur Freeman2, Erin Carey2, Mirali Sharifi3
1Arizona Cardiovascular Consultants & Vein Clinic; AT Still University, Mesa, AZ, USA; 2AT Still University, Mesa, AZ, USA; 3Arizona Cardiovascular Consultants & Vein Clinic, Mesa, AZ, USA
Background: The optimal approach to the treatment of lower extremity (LE) symptomatic superficial venous thrombosis (SVT) remains controversial. Treatment strategies have consisted of expectant observation, non-pharmacologic approaches (limb elevation and application of ice), topical or oral non-steroidal anti-inflammatory agents or anticoagulation. Anticoagulation has been recommended for LE SVT of ≥5 cm involvement. There is a paucity of data on the role of new anticoagulants (NOAC) in this setting.
Methods: We treated 23 patients with LE SVT with NOAC. Rivaroxaban at 20 mg daily was given to 16 patients and apixaban at 5 mg orally twice daily to 7 patients. The mean duration of anticoagulation with NOAC was 4±0.5 weeks and the mean follow up was 16±2 months. Presence of thrombophilic state was investigated in 19 patients.
Results: Spontaneous SVT was found in 14 patients. SVT was bilateral in 9 of 23 patients. Some form of thrombophilia was found in 7 patients (30%). Alcohol dependence or an episode of binge drinking within 3 days preceding SVT was identified in 5 patients (22%). A reduced ejection fraction (EF) of <40% was found in 4 of 16 patients who had an echocardiogram in the preceding 6 months or subsequent 2 months. Patients’ symptoms substantially improved or resolved within the first 24 hours of treatment. Despite early symptomatic improvement all affected superficial veins remained occluded at 16 months. There were no venous thromboembolic events or bleeding in any patient.
Conclusion: The results demonstrate that a 4-week course of anticoagulation with NOAC is safe and effective in the treatment of LE SVT leading to substantial improvement in symptoms early in the course of therapy. Further evaluation is required to investigate the association of SVT with reduced EF, alcohol intake and thrombophilic states.
Poster 39
Cardiac tamponade: A complication of inferior vena cava filter retrieval
Jackson J Liang, Sunil V Mankad, C Michael Johnson, Leslie T Cooper
Mayo Clinic, Rochester, MN, USA
Case: A 75-year-old woman who was admitted for hemorrhagic stroke was found to have an acute left femoral vein DVT on hospital day 13. Since anticoagulation was contraindicated, a temporary IVC filter was placed. Upon resolution of the intracerebral hemorrhage, warfarin was commenced on day 24.
On day 37, she underwent IVC filter removal. Cavogram demonstrated that the filter tip was in an abnormal location, either in the right renal vein or tightly against the right lateral IVC wall (Figure 1A). There was some difficulty grasping the IVC filter hook with the snare due to its angulation. Eventually, the filter was grasped using alligator forceps for retrieval. As the filter was pulled through the heart, the struts were visualized to be deformed from the efforts to grasp the filter (Figure 1B).
Following the filter retrieval, she developed hypotension and tachycardia. Emergent echocardiogram demonstrated a large circumferential pericardial effusion with evidence of early diastolic right ventricular collapse, consistent with cardiac tamponade. She underwent emergent pericardiocentesis with drainage of 325 cc blood and a pigtail catheter was left in place for continued drainage. Her condition stabilized and the catheter was removed after 2 days.
Discussion: IVC filters are recommended in some patients to protect against pulmonary embolism, particularly in those with acute lower extremity DVT and contraindications to anticoagulation. The long-term complications of IVC filters have been increasingly recognized, and include thromboembolic events, vessel wall penetration, filter migration, and filter fracture and embolization. Filter retrieval, while usually straightforward, may be complicated in some cases due to filter tip tilt and excessive endothelial growth embedding the hook. We report a rare case of IVC filter retrieval resulting in cardiac perforation and cardiac tamponade. This case should alert clinicians to consider cardiac tamponade to be a possible serious complication of IVC filter retrieval.

Poster 40
Reversal of lower extremity venous reflux post stenting in May–Thurner syndrome
Brian Fowler, Jeannette Clayton, Raghu Kolluri, Mitchell Silver
Ohio Health Heart and Vascular Physicians, Columbus, OH, USA
Case: A 32 y/o female presented in clinic with complaints of left lower extremity (LE) pain, heaviness and swelling and a complex history of left LE DVT, superficial thrombophlebitis, ulcerations and venous insufficiency. Pertinent physical findings included advanced lipodermatosclerosis of the left LE; presence of a healed ulceration with atrophy blanche in the medial gator area of the ankle; reticular veins and 1+ pitting edema of the foot.
The patient underwent venous insufficiency (VI) testing, CTV and subsequent venogram. The VI study revealed chronic DVT in the common femoral vein and extensive deep venous reflux from the proximal femoral vein (Figure 1A) through the popliteal vein. The venogram demonstrated an 80% stenosis of the common iliac vein which was stented. A follow-up venous duplex revealed a decrease in vein diameter and a remarkable reduction in deep venous reflux (Figure 1B). The patient reported near complete resolution of symptoms.
Discussion: May–Thurner syndrome (MTS) is present in 2–5% of patients undergoing VI examination. The proximal restriction of MTS results in stagnation of venous flow which can lead to thrombosis, dilation of the veins and reflux. Endovascular revascularization of this condition has become an accepted method for MTS management. We report the utility of ultrasound in the management and diagnosis of MTS and also demonstrate its usefulness in follow up of these patients post intervention.

Left proximal femoral vein pre-stenting: 3 seconds of reflux noted.

Left proximal femoral vein post-stenting: no reflux noted.
Poster 41
Portal vein aneurysm: Misdiagnosed as cancer
Rohan Mankikar, Balsam Elhammali
Morehouse School of Medicine, Atlanta, GA, USA
Portal vein aneurysm is a rare diagnosis and represents 3% of portal venous aneurysms. It is often misdiagnosed and treatment has been very controversial.
We present a 48-year-old male with a history of chronic pancreatitis due to alcohol abuse that presented with persistent mid epigastric pain for 6 months. It was associated with involuntary weight loss of 40 lb and night sweats. The patient’s BP was 144/90, HR 68, SaO2 100%, temp 99.3, pain 6/10. In the ED, a CT abdomen was performed which showed a large pancreatic head mass that was also concerning for a portal vein thrombosis. Subsequently, an abdominal US was also performed to evaluate for chronicity of the portal vein thrombosis because this would help with portal pressures and would dictate whether he would need to be started on a heparin drip. The portal vein thrombosis was deemed to be chronic due to evidence of esophageal and gastric varices so he was not started on heparin. Subsequently, GI was consulted and they were concerned about a possible malignancy and recommended an MRCP. This further characterized the mass to be a large portal vein aneurysm containing a bland thrombus. His SMV and splenic vein showed partial thrombosis as well. Furthermore, Vascular Surgery was consulted and they were not comfortable in performing surgery; the films were evaluated by IR who did not feel that surgery was appropriate either (they suggested that thrombosis of the SMV and splenic vein would be a contraindication to TIPS procedure). The patient was offered symptomatic therapy with pain medications, and to reduce portal pressures he was started on nadolol 40 mg with a goal HR of 55–65.


The presenter will discuss the key elements of pathophysiology, presentation and unique treatment in this case.