
Abstract
Patients with abdominal aortic aneurysm (AAA) are prone to vascular infection with chronic Q-fever. There is a rising incidence of up to 8% of chronic Q-fever in The Netherlands. Increased vascular aortic aneurysm infection with chronic Q-fever is reported. This report shows two rare cases of primary aortoduodenal fistulae in patients with chronic Q-fever and an AAA. We describe the clinical symptoms, diagnostic tools for detection of Coxiella burnetii infection and treatment.
Introduction
Recent reports show an increasing incidence of abdominal aortic aneurysm (AAA) infected with chronic Q-fever.1–5 Owing to a rising incidence of chronic Q-fever, caused by a large outbreak in 2007 in The Netherlands, growing numbers of aortic aneurysms infected with chronic Q-fever have been reported. We describe two cases of primary aortoduodenal fistula (PADF) in combination with chronic Q-fever.
Case report 1
A 66-year-old male was admitted to our clinic with abdominal pain. A computerised tomography (CT) scan showed an infrarenal AAA measuring 5.4 cm and a 3.6 cm aneurysm of the left common iliac artery (CIA). Prior medical history included myocardial infarction and diabetes mellitus type II. Open repair with an aorto bi-iliacal prosthesis was performed. During the operation we found a contained rupture of the left iliac artery and, furthermore, the duodenum was stuck on the aorta. After close inspection and manipulation, an aortoduodenal fistula (ADF) was revealed. Replacement was performed with a rifampin-soaked, silver-coated Dacron graft. An omentum pedicle was wrapped around the abdominal graft. The duodenum was stapled transversely and sutured with a 3/0 Monocryl. Serology and three specimens (aorta and CIA) were all polymerase chain reaction (PCR) positive for Coxiella burnetii. Doxycycline was commenced at 100 mg 2dd1 and hydroxychloroquine at 200 mg 3dd1. Forty-one days after surgery the patient died of respiratory insufficiency.
Case report 2
A 67-year-old female presented to our emergency room with symptoms of haematemesis and melaena. Physical examination showed tachycardia (100 beats per minute (BPM)) and systolic blood pressure (BP) 100/50. Gastroscopy raised the suspicion of an ADF (Figure 1). A CT scan showed a 4.8 cm AAA, occlusion of the left CIA and an ADF. Images showed an ulcer in the aorta and induration was seen around the aorta (Figure 2). A median laparotomy was performed showing a fistula between the aorta and the duodenum. A rifampin-soaked prosthesis was sited and the fistula opening was removed and sutured. It was necessary to resect 30 cm of the jejunum as a result of a serosal injury. One day after surgery the patient developed a myocardial infarction and despite cardiopulmonary resuscitation the patient died. Serology and aorta wall and clot PCR were both positive for C. burnetii.
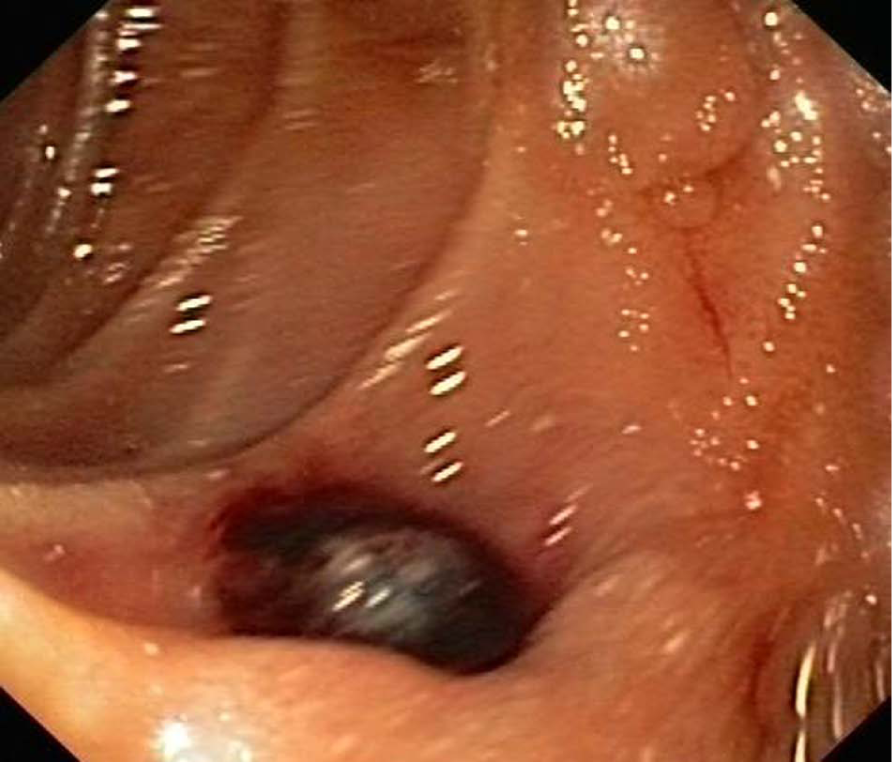
Gastroscopy in the second part of the duodenum, showing a blood clot with some oozing – a suspected Aortoduodenal fistula.
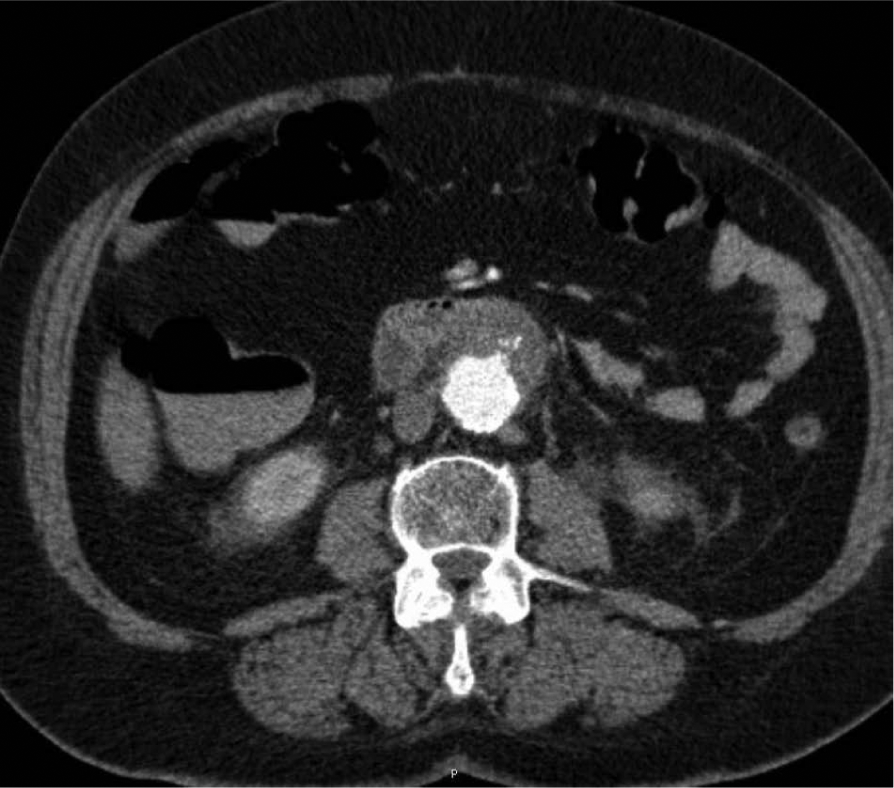
An abdominal aortic aneurysm of 4.8 cm with induration around the aorta and contrast leakage towards the duodenum.
Discussion
The combination of chronic Q-fever with PADF is very rare, described in only two earlier reports.3,4 PADF is a communication between the lumen of the aorta and duodenum. 6 A primary fistula occurs in native aorta without prior vascular intervention, with the incidence ranging from 0.04% to 0.07%. 6 Secondary ADFs occur due to mechanical erosion of a prosthetic graft through the bowel following vascular surgery and have a higher incidence (0.5–2.3%). 6 A predominance for the duodenum is explained by anatomical aspects. 6
Infection of an aortic aneurysm is a rarity, with an incidence of approximately 1%, most commonly caused by Staphylococcus and Salmonella. The incidence of AAAs infected with C. burnetii is seen increasingly. Animal reservoirs of most importance are goats, sheep and cattle. C. burnetii is spread in urine, faeces, milk and, especially, birth products. Chronic Q-fever will develop in 1–11% of the population that suffers from acute Q-fever. Symptoms of the acute form are usually flu-like. Chronic Q-fever will manifest as endocarditis or vascular infection (9%).4,5 Acute infection results in antibodies to phase II antigens, followed by phase I antibodies. Persisting high levels of antibodies to phase I and phase II antigens are considered indicative for chronic Q-fever. 5 The international cut-off point for chronic Q-fever infection is for phase I IgG > 1:800. 7 Patients at risk for chronic Q-fever are those with prior cardiac valve defects, aneurysms or vascular grafts, pregnant women and immunocompromised patients. 7
A recent review identified 58 cases of vascular infections with chronic Q-fever. 8 Recently, some other case reports have described chronic Q-fever-infected aortic aneurysms or prosthetic grafts.1,3,8 The vascular complications described in patients with chronic Q-fever show endocarditis to be the most common, followed by aortic aneurysm or aortic graft infection. Other complications are ADF, rupture of the aneurysm, infectious spondylitis and embolisation of the distal limbs.3,8
As our hospital is located in a hotspot, in our clinic we currently screen all patients with a known AAA for chronic Q-fever vascular infections. Patients who test positive are treated with antibiotics and then seen every month for serology and a 3-monthly ultrasound examination.
It has been hypothesised that quick growth of the aneurysm in a short time might be due to all kinds of aetiologies. However, in an endemic area of chronic Q-fever, this aetiology should be considered in case of rapid expansion.
The preoperative diagnosis of chronic Q-fever is difficult. International cut-off point for phase I IgG is >1:800. C. burnetii culture sensitivity is only 40% and 52.9% in blood specimens. 7 PCR shows a low sensitivity of 22.9% in blood specimens. In cardiac valves, however, the sensitivity is 100%. 7 Gastroscopy has a low sensitivity (30%) for diagnosing ADF. 9 Therefore, a CT scan is the diagnostic tool of choice. Ectopic gas within or adjacent to the aortic lumen is the most important finding in Aortoduodenal fistulas.
During aortic repair, biopsies of the potentially infected aorta should be made and sent for PCR testing. Following surgical repair, treatment should exist of at least doxycycline in combination with hydroxychloroquine for at least 1.5 years. 7 Follow-up after surgery should consist of 3-monthly clinical and microbiological check-ups. 7
Conclusion
Chronic Q-fever leading to vascular infections is increasing, and mortality and complication rates are high. The diagnosis is difficult to make but screening in endemic areas is justifiable. Although primary ADF is an uncommon complication, clinicians should be suspicious when treating patients with a prior history of AAA in Q-fever endemic areas.
Footnotes
Declaration of conflicting interest
The authors declare no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.