
Abstract
Pseudoaneurysm of an extra-cranial carotid artery is a rare occurrence. 1 Penetrating or blunt injury of the neck is one of the reasons for carotid artery pseudoaneurysm. 2 Endovascular stenting is an alternative to conventional surgical repair in such cases. 2 We hereby report a case of post-traumatic right common carotid artery (CCA) pseudoaneurysm, which was successfully managed with an endovascular stent graft.
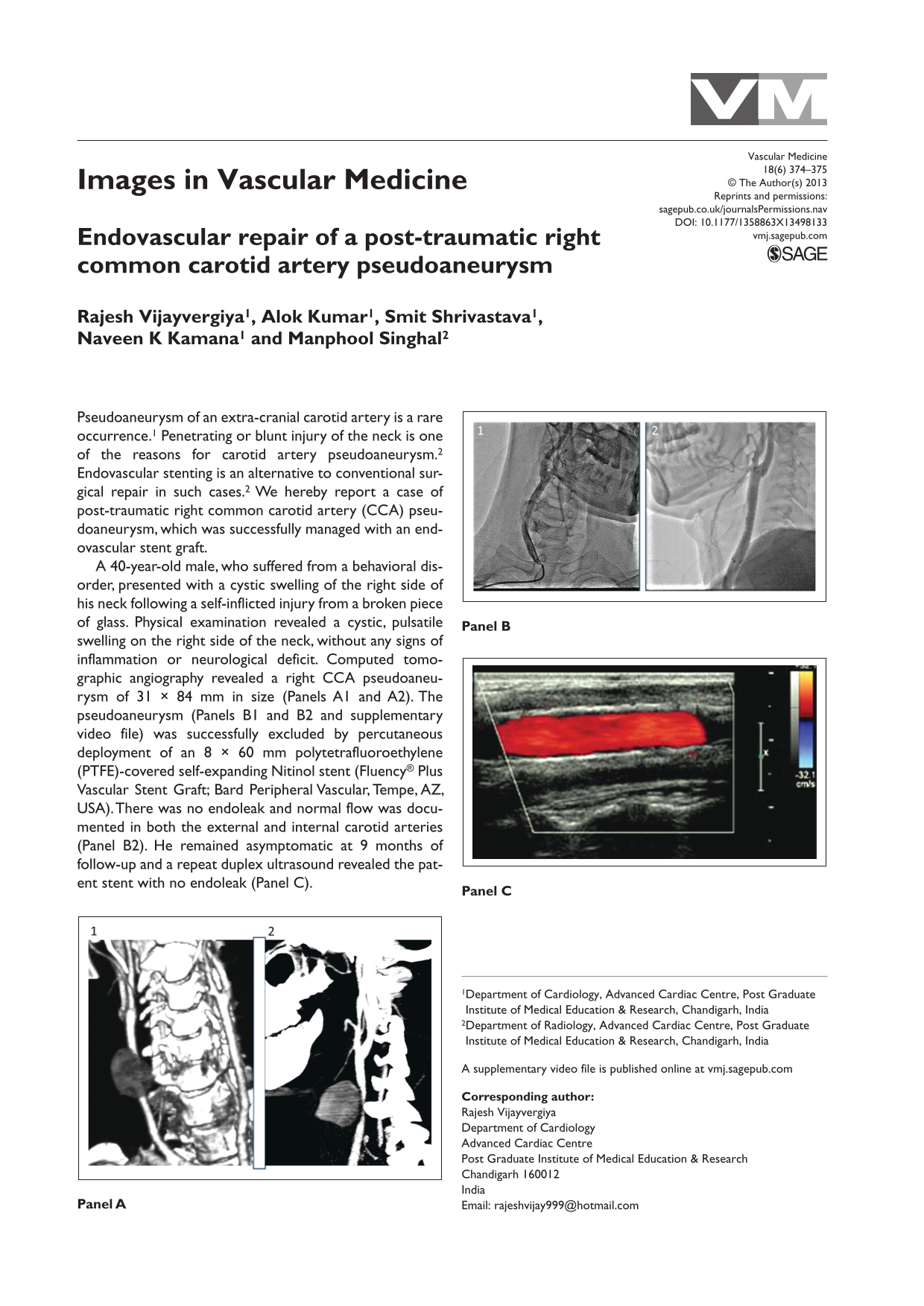
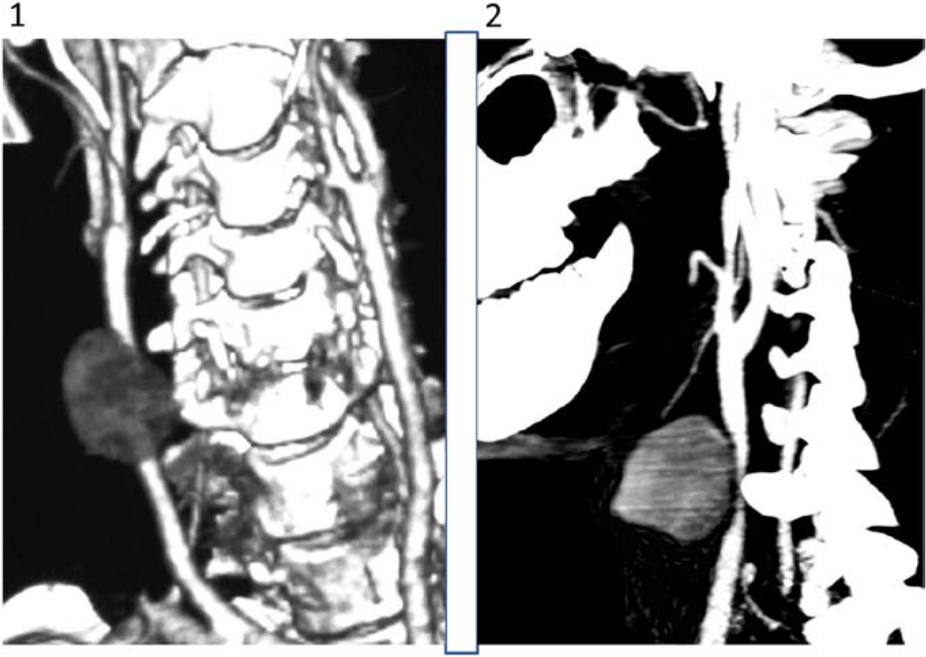
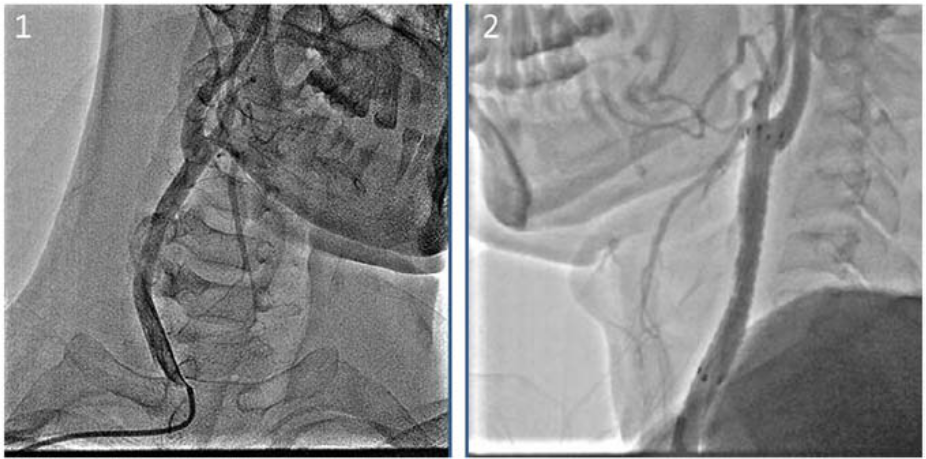
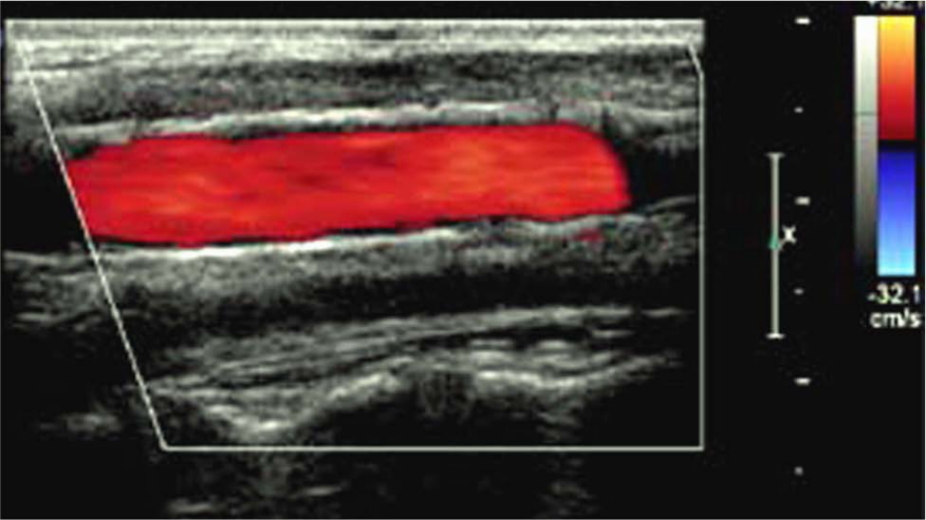
A 40-year-old male, who suffered from a behavioral disorder, presented with a cystic swelling of the right side of his neck following a self-inflicted injury from a broken piece of glass. Physical examination revealed a cystic, pulsatile swelling on the right side of the neck, without any signs of inflammation or neurological deficit. Computed tomographic angiography revealed a right CCA pseudoaneurysm of 31 × 84 mm in size (Panels A1 and A2). The pseudoaneurysm (Panels B1 and B2 and supplementary video file) was successfully excluded by percutaneous deployment of an 8 × 60 mm polytetrafluoroethylene (PTFE)-covered self-expanding Nitinol stent (Fluency® Plus Vascular Stent Graft; Bard Peripheral Vascular, Tempe, AZ, USA). There was no endoleak and normal flow was documented in both the external and internal carotid arteries (Panel B2). He remained asymptomatic at 9 months of follow-up and a repeat duplex ultrasound revealed the patent stent with no endoleak (Panel C).
A large CCA pseudoaneurysm, as in this case, warrants an intervention to prevent local vascular complications and distal thrombo-embolic events.1–3 While surgical repair is considered the gold standard, it carries a significant morbidity and mortality. 1 Surgical repair is technically challenging in patients with hostile neck (e.g. post-irradiation or prior neck surgery), in those with a large aneurysm adherent to adjacent structures, and those with an aneurysm localized distally beneath the skull.1,4 In contrast, endovascular repair is a minimally invasive, safe, and effective alternative to surgical repair.2,3 Endovascular repair can be performed by a PTFE-covered self-expanding stent-graft deployment,1–3,5 as done in this case. There is a risk of stent thrombosis and restenosis with stent-graft placement;2,3,5 however, thus far, our patient has had a favorable clinical outcome and continues to be followed.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Mark A Creager, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.