
Abstract

A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force
Abstract
The American College of Cardiology Foundation (ACCF), in partnership with key specialty and subspecialty societies, conducted a review of common clinical scenarios where noninvasive vascular testing (venous ultrasound and physiological testing) is frequently considered. The indications (clinical scenarios) were derived from common applications or anticipated uses, as well as from current clinical practice guidelines and results of studies examining the implementation of the original appropriate use criteria (AUC). The 116 indications in this document were developed by a diverse writing group and scored by a separate independent technical panel on a scale of 1 to 9, to designate appropriate use (A) (median 7 to 9), maybe appropriate use (M) (median 4 to 6), and rarely appropriate use (R) (median 1 to 3).
Keywords
ACCF Appropriate Use Criteria; imaging; peripheral vascular disease; ultrasound
Preface
In an effort to respond to the need for the rational use of imaging services in the delivery of high-quality care, the American College of Cardiology Foundation (ACCF) has undertaken a process to determine the appropriate use of cardiovascular imaging for selected patient indications. Appropriate use criteria (AUC) publications reflect an ongoing effort by the ACCF to critically and systematically create, review, and categorize clinical situations where diagnostic tests and procedures are utilized by physicians caring for patients with cardiovascular diseases. The process is based on current understanding of the technical capabilities of the imaging modalities examined. Although impossible to be entirely comprehensive given the wide diversity of clinical disease, the indications are meant to identify common scenarios encompassing the majority of situations encountered in contemporary practice. Given the breadth of information they convey, the indications do not directly correspond to the Ninth Revision of the International Classification of Diseases (ICD-9) system, as these codes do not include clinical information, such as symptom status.
The ACCF believes that careful blending of a broad range of clinical experiences and available evidence-based information will help guide a more efficient and equitable allocation of healthcare resources in cardiovascular imaging. The ultimate objective of AUC is to improve patient care and health outcomes in a cost-effective manner, but it is not intended to ignore ambiguity and nuance intrinsic to clinical decision making. AUC thus should not be considered substitutes for sound clinical judgment and practice experience.
We are grateful to the technical panel, a professional group with a wide range of skills and insights, for their thoughtful and thorough deliberation of the merits of peripheral vascular ultrasound for various indications. We would also like to thank the individuals who provided a careful review of the draft of indications, the parent AUC Task Force, and the ACC staff, Z. Jenissa Haidari and Joseph Allen, for their exceptionally skilled support in the generation of this document.
Heather L. Gornik, MD, FACC, FAHA
Chair, Testing for Venous Disease and Evaluation of Hemodialysis Access
Michael J. Wolk, MD, MACC
Chair, Appropriate Use Criteria Task Force
1. Introduction
Improvements in cardiovascular imaging technology and their application, coupled with increasing therapeutic options for cardiovascular disease, have led to an increase in cardiovascular imaging. Diagnostic imaging services reimbursed under Medicare’s physician fee schedule grew more rapidly than any other type of physician service from 1999 to 2003, although more recently, the rate of imaging volume growth in Medicare has been slowing. Still, the armamentarium of noninvasive diagnostic tools has expanded greatly, offering a variety of new and more sophisticated imaging techniques. As imaging technology and clinical applications continue to advance, the healthcare community needs to understand how to best incorporate these technologies into daily clinical care and how to choose between new and long-standing established imaging technologies. In an effort to respond to this need and to ensure the effective use of advanced diagnostic imaging tools, the Appropriate Use Criteria (AUC) project was initiated. This document serves as the second in a 2-part series evaluating noninvasive testing for peripheral vascular disorders with ultrasound and physiological testing. The focus of this document is clinical indications associated with evaluation of the venous system as well as preparation for and evaluation of dialysis access (e.g., arteriovenous fistulas). Appropriate use criteria for evaluation of peripheral arterial disorders (carotid, lower and upper extremities, abdominal aorta, visceral artery) have been previously published (1). The indications and findings from this AUC process are meant to help inform and ensure the highest quality and most efficient use of vascular laboratory testing (vascular ultrasound and physiological testing) in the evaluation of the venous system.
2. Methods
The indications included in this publication cover a wide array of cardiovascular signs and symptoms as well as clinical judgments as to the likelihood of cardiovascular findings. Within each main disease category, a standardized approach was used to capture the majority of clinical scenarios without making the list of indications excessive. During the development of this document, the AUC Task Force revised the terminology and definitions to better clarify the appropriateness categories to avoid misinterpretation and misuse of appropriate use criteria documents (2).
The indications were constructed by experts in peripheral vascular disease and in other fields and were modified on the basis of discussions among the task force and feedback from independent reviewers and the technical panel. Wherever possible, indications were mapped to relevant clinical guidelines and key publications/references where available in the medical literature (Online Appendix).
Indication Development
The indications were constructed by a writing group with expertise in both the science and clinical practice of vascular ultrasound and physiological testing, vascular medicine and vascular surgery, and vascular imaging and intervention. The writing group was tasked with developing a list of clinical scenarios covering the majority of patients that clinicians might consider referring for noninvasive ultrasound and physiological testing. The term “indication” is used interchangeably with “clinical scenario” in the document for brevity and does not imply that a procedure should necessarily be performed. Indication modifications were made through discussions with the American College of Cardiology Foundation (ACCF) AUC Task Force and feedback from reviewers that include additional experts in the areas noted in the previous text. The current document includes indications related to noninvasive vascular testing for venous disease and for hemodialysis access. Appropriate use criteria for the evaluation of arterial disorders have been previously published (1).
Rating Process and Scoring
The technical panel first rated the indications independently. The technical panel then convened for a face-to-face meeting to discuss each indication. At this meeting, panelists were provided with their scores and a blinded summary of their peers’ scores. After the meeting, panelists once again independently rated each indication according to the originally published classification terms to indicate their final scores. The technical panel then completed an additional third rating process to address a few areas that required further clarification and to incorporate the revised indication classification terminology (2). During this final rating, the technical panel was asked to reexamine the indications using the new terms and expanded definitions, realizing that the use of new terms could result in some reclassification of the clinical scenarios.
When rating each clinical scenario, the technical panel was asked to assess whether ultrasound and/or physiological testing was appropriate, maybe appropriate, or rarely appropriate, according to the following definition of appropriate use:
The technical panel scored each indication as follows:
Median Score 7 to 9: Appropriate Care
Median Score 4 to 6: Maybe Appropriate Care
Median Score 1 to 3: Rarely Appropriate Care
The division of these scores into 3 levels of appropriateness is somewhat arbitrary, and the numeric designations should be viewed as a continuum. Further, there is diversity in clinical opinion for particular clinical scenarios, such that scores in the intermediate level of appropriate use should be labeled “maybe appropriate,” because critical patient or research data may be lacking or discordant. This designation should be a prompt to the field to carry out definitive research investigations whenever possible. It is anticipated that the AUC reports will continue to be revised as further data are generated and information from the implementation of the criteria is accumulated.
To prevent bias in the scoring process, the technical panel was deliberately composed of a minority of specialists in vascular noninvasive testing. In addition, care was taken in providing objective, nonbiased information, including guidelines and key references, to the technical panel.
The level of agreement among panelists as defined by RAND (3) was analyzed based on the BIOMED rule for a panel of 14 to 16 members. As such, agreement was defined as an indication where 4 or fewer panelists’ ratings fell outside the 3-point region containing the median score.
Disagreement was defined as where at least 5 panelists’ ratings fell in both the appropriate and the rare appropriate categories. Any indication having disagreement was categorized as maybe appropriate regardless of the final median score. Indications that met neither definition for agreement or disagreement are in a third, unlabeled category.
3. Assumptions
To prevent any inconsistencies in interpretation, specific assumptions are provided that were considered by the technical panel in rating the relevant clinical indications for the appropriate use of peripheral vascular ultrasound and physiological testing:
Clinical indications assume that a history and physical examination has been performed by a qualified healthcare provider before performance of the vascular ultrasound or physiological testing examination.
A peripheral vascular ultrasound and physiological testing examination and report will include performance of the vascular ultrasound or physiological testing examination using a standardized
Interpretation of the vascular ultrasound or physiological testing examination by a physician interpreter using
Appropriate equipment is used for each specific type of testing, including appropriate frequency ultrasound transducers and properly sized cuffs and others sensors for physiological testing.
Documentation that the vascular sonographer used optimal angle correction techniques to ensure accurate angle of insonation for reporting of Doppler velocity measurements. In general, an angle of insonation of 60° or less is used with appropriate sample volume placement.
All standard vascular ultrasound and physiological testing techniques have a sensitivity and specificity similar to those found in the published literature for the specific examination type.
Testing should be performed by a credentialed technologist (registered vascular technologist [RVT] or registered vascular sonographer [RVS]) and interpreted by a credentialed physician (registered physician in vascular interpretation [RPVI]). Finally, the testing should be done in a facility accredited in vascular testing (e.g., IAC–Vascular Testing or ACR).
If prior testing is of poor technical quality, repeat imaging may sometimes be appropriate in a different facility or after the conditions that restricted the prior testing are no longer present (e.g., bowel gas, open wounds) prior to the specified timeframes.
The appropriate use of testing is assumed to have the potential to impact clinical decision making and to direct therapeutic interventions.
The range of potential indications for vascular ultrasound and physiological testing is quite large, particularly in comparison with other cardiovascular imaging tests. Thus, the indications are, at times, purposefully broad to cover an array of vascular signs and symptoms as well as the ordering physician’s best judgment as to the presence of vascular abnormalities. Additionally, there are likely clinical scenarios that are not covered by the current indications in this document.
Venous duplex examinations that are performed to assess for suspected venous thrombosis in the limbs require performance of gray scale (B-mode) compression maneuvers in addition to color flow and spectral Doppler examination.
Complete vascular examinations (ultrasound and physiological testing) require bilateral studies in the majority of clinical cases, though specific clinical indications may warrant a unilateral or limited study, (e.g., unilateral leg pain and swelling and suspected lower extremity deep vein thrombosis). The decision to perform a complete bilateral or unilateral examination should be determined by the study indications and the standardized laboratory scanning protocol.
When a unilateral venous examination is performed, a spectral Doppler waveform from a contralateral proximal deep vein (e.g., subclavian or internal jugular vein for the upper extremities or common femoral vein for the lower extremities) should be recorded to allow for comparative assessment of flow patterns in the limbs.
For the clinical scenarios presented in the section on Hemodialysis Vascular Access Duplex Ultrasound (Table 8) it is acknowledged that the appropriate vascular laboratory assessment might include more than duplex ultrasound of the extremity veins. Depending on the scenario, additional testing could include arterial duplex scanning and physiological tests such as segmental limb pressures and digit pressure measurements.
To optimize patient care and minimize need for unnecessary repeat studies, it is generally recommended that repeat or serial scans (e.g., for surveillance of calf vein thrombosis with contraindication to anticoagulation) be performed in the same facility.
Raters were instructed to consider cost implicitly when making the appropriate use determination.
Raters were instructed to consider patient safety implicitly in the appropriate use determination.
If the reason for a test can be assigned to more than 1 clinical indication, it should be matched to the indication with the highest appropriate use score.
For each indication, the rating should reflect whether the test is reasonable for the patient according to the appropriate use definition, not whether the test is better or worse than another modality.
The category of “maybe appropriate” should be used when insufficient clinical data are available for a definitive categorization or there is disagreement as defined in the methods. The designation of “maybe appropriate” is assumed to not provide grounds for denial of reimbursement.
Unless explicitly stated, the indications in this document indicate only whether vascular ultrasound or physiological testing by itself is reasonable. The indications do not address whether it is reasonable to perform vascular ultrasound or physiological testing instead of or in conjunction with another test, either before or after the test.
4. Definitions
Physiological testing:
Evaluation of the peripheral venous circulation based on measurement of limb blood flow using plethysmographic sensors (e.g., air, strain gauge, or photoplethysmography) with physiological maneuvers (e.g., limb positioning, limb exercise, tourniquet application), or other parameters, without utilizing data from direct imaging of the blood vessels.
Screening examination:
Testing conducted to determine the presence or absence of disease in an asymptomatic patient.
Surveillance examination:
Testing conducted to monitor disease progression based solely on the passage of time since initial diagnosis or revascularization (e.g., calf vein thrombosis with contraindication to anticoagulation). It is assumed that baseline testing has already been conducted.
5. Abbreviations
ACR = American College of Radiology
AVF = autogenous arteriovenous fistula (including venous transpositions)
AVG = prosthetic arteriovenous graft
CHF = congestive heart failure
DVT = deep vein thrombosis
IAC = Intersocietal Accreditation Commission
ICU = intensive care unit
IVC = inferior vena cava
RPVI = registered physician in vascular interpretation
RVT
RVS
TIPS = transjugular intrahepatic portosystemic shunt
6. Peripheral Vascular Ultrasound and Physiological Testing Part II: Testing for Venous Disease and Evaluation of Hemodialysis Access Appropriate Use Criteria (by Indication)
Section 1: Upper Extremity Venous Duplex Ultrasound
Venous Duplex of the Upper Extremities for Patency and Thrombosis.
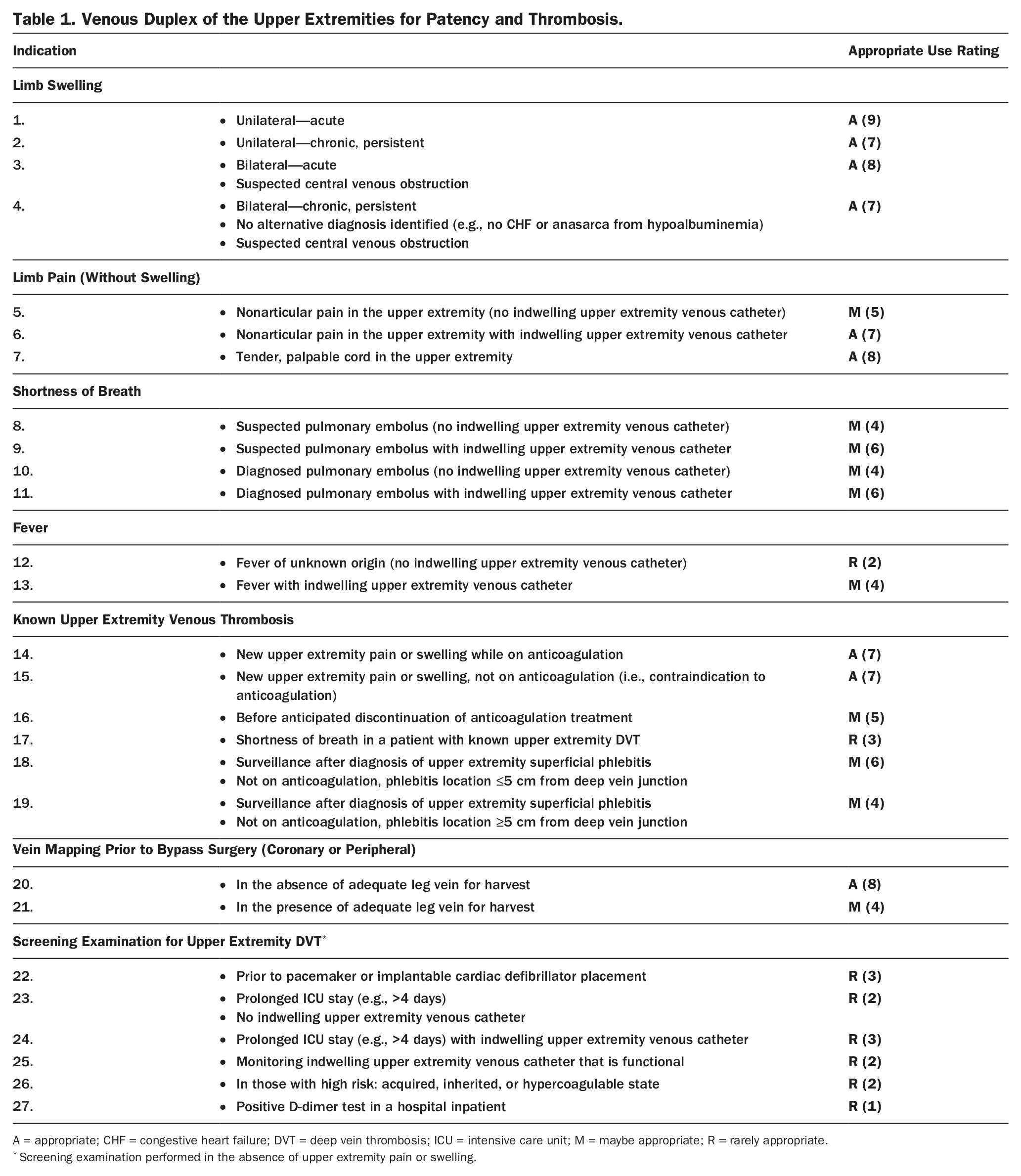
A = appropriate; CHF = congestive heart failure; DVT = deep vein thrombosis; ICU = intensive care unit; M = maybe appropriate; R = rarely appropriate.
Screening examination performed in the absence of upper extremity pain or swelling.
Summary: Upper Extremity Venous Duplex Ultrasound
Upper extremity venous duplex ultrasound was rated as an appropriate test in the setting of limb swelling, non-articular upper extremity pain or palpable cord, and when new pain or swelling is noted in the presence of known upper extremity deep vein thrombosis (DVT). It was deemed rarely appropriate to perform an upper extremity venous ultrasound for evaluation of fever of unknown origin in the absence of an indwelling upper extremity venous catheter or for evaluation of shortness of breath in a patient with known upper extremity DVT.
Screening for upper extremity DVT in an asymptomatic patient was rated as rarely appropriate across 6 of 6 clinical scenarios, including the patient with prolonged intensive care unit (ICU) stay (with or without an upper extremity venous catheter), prior to pacemaker or defibrillator placement, for monitoring of a functional upper extremity venous catheter, or for upper extremity DVT screening in those with hypercoagulable state or with positive D-dimer test.
Upper extremity vein mapping (e.g., of cephalic and basic veins) prior to coronary or peripheral bypass surgery was rated as an appropriate test in the absence of adequate leg vein for harvest and as maybe appropriate in certain settings when adequate leg vein conduit is present.
Section 2: Lower Extremity Venous Duplex Ultrasound
Summary: Lower Extremity Venous Duplex Ultrasound
Lower extremity venous duplex ultrasound (Table 2) was rated an appropriate test in the setting of limb swelling, nonarticular lower extremity pain or palpable cord, pulmonary embolism, and when new pain or swelling is noted in the presence of known lower extremity DVT. Testing was also rated as appropriate for certain surveillance indications, namely surveillance of calf vein thrombosis for proximal extension of DVT when anticoagulation is contraindicated and for superficial thrombophlebitis of the legs (i.e., great or small saphenous vein) located near a deep vein junction. Venous ultrasound was rated as appropriate for early procedural follow-up after endovenous saphenous ablation procedures (in the patient with or without symptoms). Lower extremity venous duplex ultrasound was rated as appropriate for further evaluation of the patient with patent foramen ovale with suspected paradoxical embolism and for the patient with evidence of lower extremity venous obstruction on venous physiological testing (plethysmography) that suggests the possibility of DVT.
Venous Duplex of the Lower Extremities for Patency and Thrombosis.
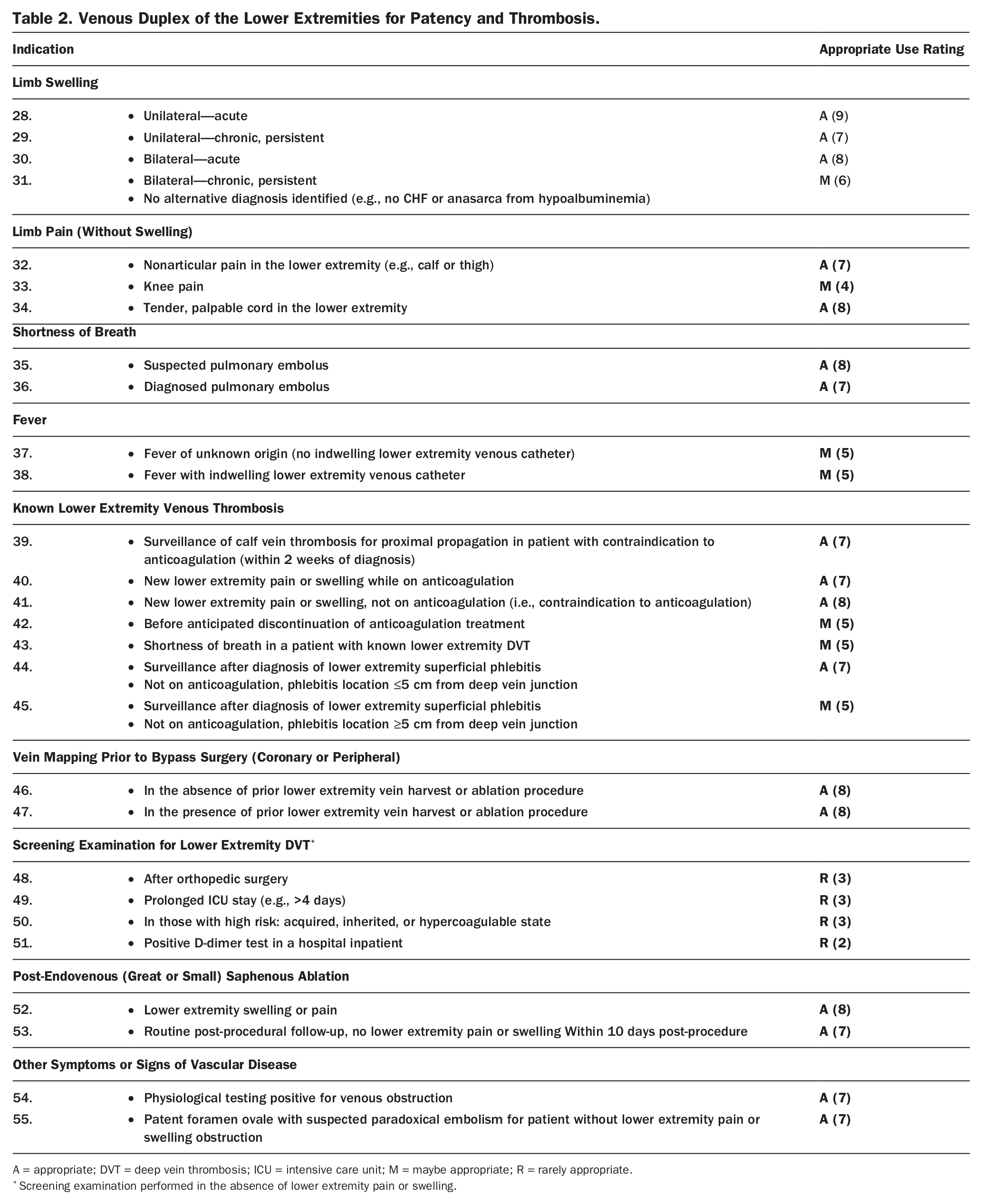
A = appropriate; DVT = deep vein thrombosis; ICU = intensive care unit; M = maybe appropriate; R = rarely appropriate.
Screening examination performed in the absence of lower extremity pain or swelling.
Screening for lower extremity DVT with duplex ultrasound in an asymptomatic patient was rated as rarely appropriate across multiple clinical scenarios, including the patient with a prolonged ICU stay, following orthopedic surgery, for those with hypercoagulable state, or with a positive D-dimer test. This was consistent with the rarely appropriate ratings for upper extremity venous duplex ultrasound discussed in the preceding text.
Lower extremity vein mapping (of the saphenous veins) prior to coronary or peripheral bypass surgery was rated as an appropriate test regardless of whether or not the patient has previously undergone lower extremity vein harvest or ablation procedure.
Similar to the upper extremities, lower extremity venous duplex ultrasound for evaluation of fever of unknown etiology was rated as maybe appropriate in certain clinical scenarios, though the evidence to support this practice is limited (5–7).
Duplex ultrasound evaluation for venous incompetency, with provocative physiological maneuvers such as distal limb augmentation and/or Valsalva, was rated as appropriate in the setting of significant clinical symptoms and signs of venous disease, including: active or healed venous ulcer, varicosities with lower extremity discomfort, swelling, or chronic skin changes (Table 3). Duplex ultrasound for venous incompetency was rated as maybe appropriate for evaluation of the patient with significant, though asymptomatic, varicose veins (e.g., large, disfiguring varicose veins) or for the patient with lower extremity pain or heaviness without signs of venous disease.
Duplex Evaluation for Venous Incompetency.
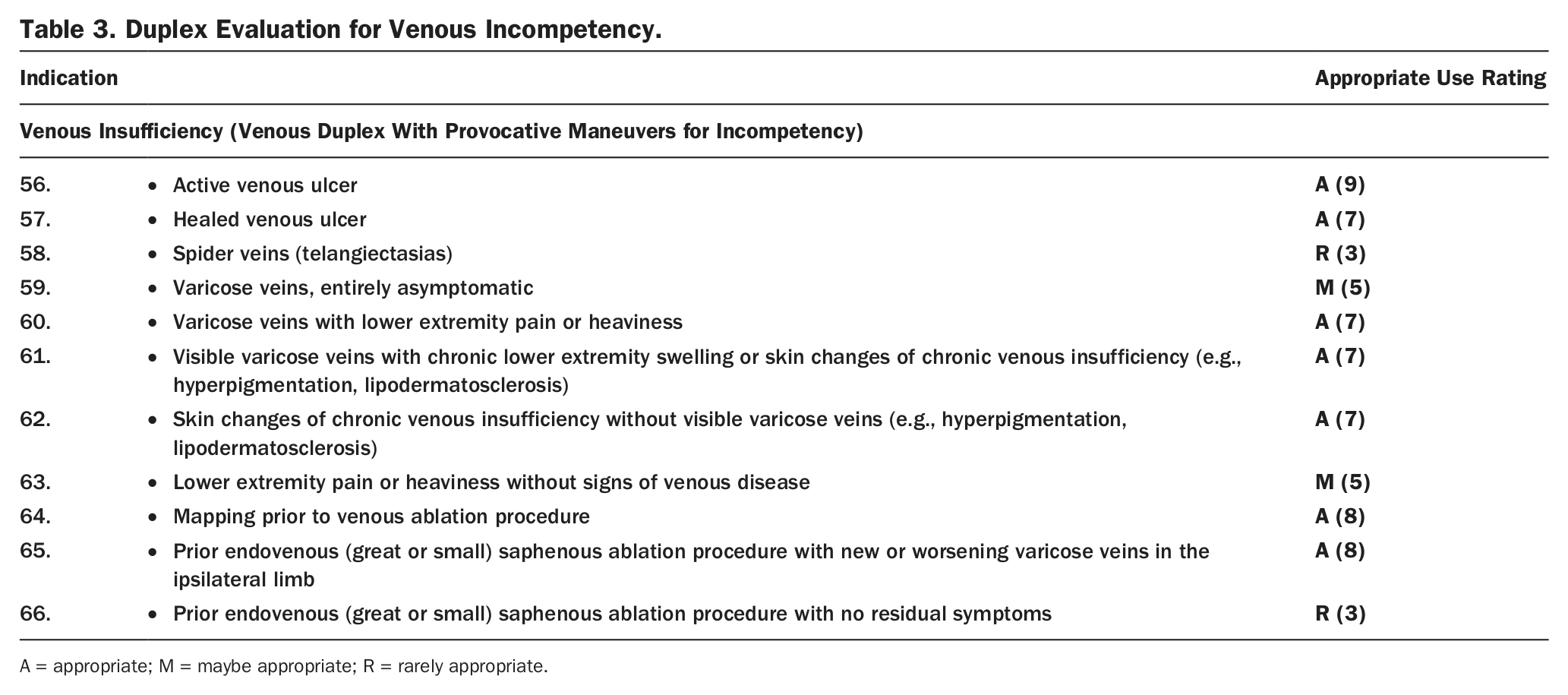
A = appropriate; M = maybe appropriate; R = rarely appropriate.
Venous Physiological Testing (Plethysmography) With Provocative Maneuvers to Assess for Patency and/or Incompetency.
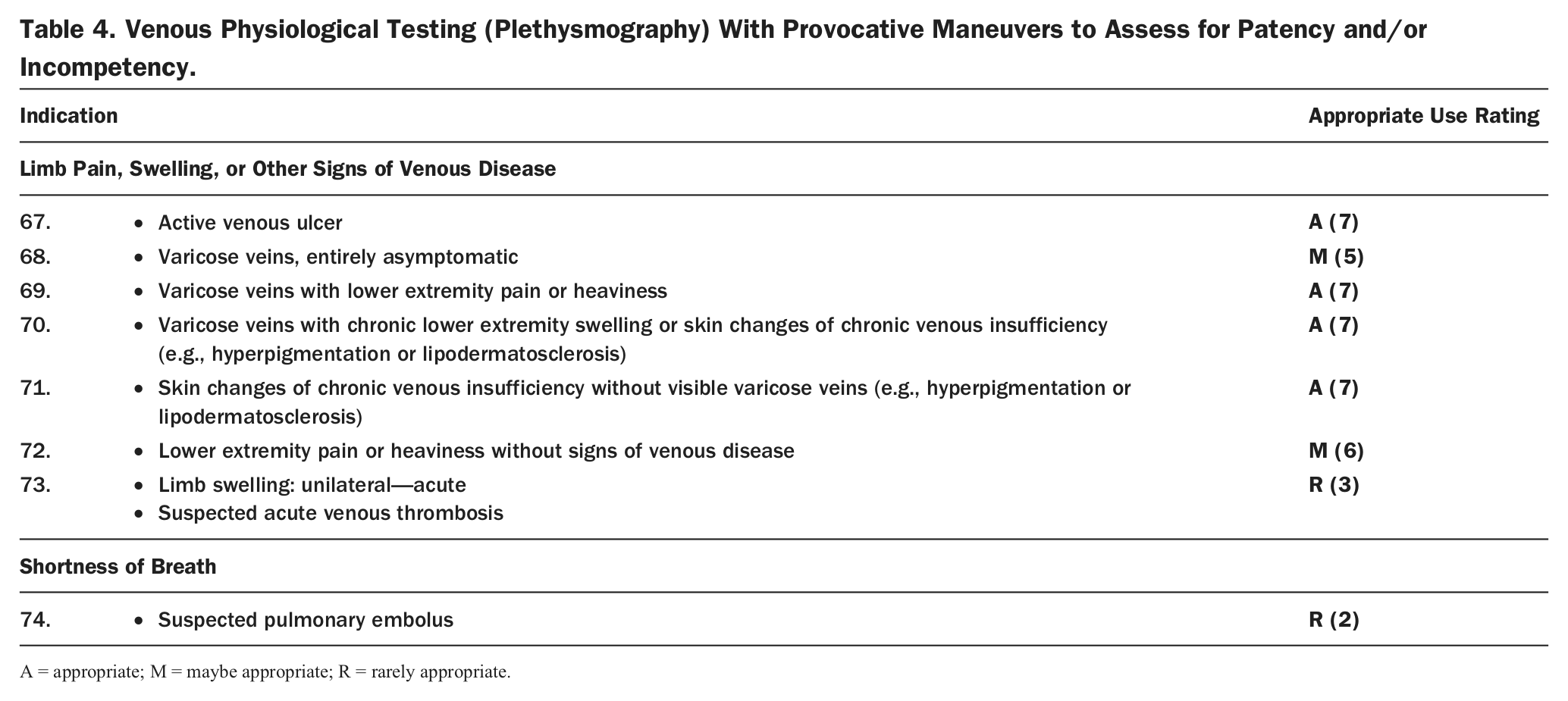
A = appropriate; M = maybe appropriate; R = rarely appropriate.
Duplex ultrasound was rated as rarely appropriate for evaluation of isolated spider veins (telangiectasias) without other stigmata of venous disease or for the patient with prior saphenous vein ablation with no residual symptoms (although initial follow-up duplex for within the initial 10 days after the procedure was rated as appropriate, see the preceding text).
Summary: Venous Physiological Testing
Selected clinical indications for venous physiological testing (plethysmography) with provocative maneuvers were evaluated. Venous physiological testing was rated as appropriate in the setting of significant clinical symptoms and signs of chronic venous insufficiency, including: active venous ulcer, symptomatic varicose veins, and chronic skin changes such as lipodermatosclerosis or hyperpigmentation. Similar to the indications for venous duplex ultrasound for venous incompetency, venous physiological testing was rated as maybe appropriate for evaluation of the patient with asymptomatic varicose veins or for the patient with lower extremity pain or heaviness without signs of venous disease.
Importantly, venous physiological testing was rated as rarely appropriate for evaluation of the patient with suspected acute lower extremity DVT or pulmonary embolism. In the case of suspected acute lower extremity DVT, duplex ultrasound would be the best initial test.
Section 3: Duplex Evaluation of the Inferior Vena Cava and Iliac Veins
Summary: Duplex Evaluation of the Inferior Vena Cava and Iliac Veins
In the setting of evaluation for suspected DVT, iliocaval duplex was rarely appropriate as a “stand-alone test,” but was rated as appropriate or maybe appropriate for use either routinely or selectively in conjunction with lower extremity venous duplex scanning (Table 5). Scanning of the inferior vena cava (IVC) and iliac veins was rated as appropriate when performed selectively with a positive lower extremity venous duplex demonstrating proximal DVT or when an abnormal flow pattern was found in 1 or both common femoral veins. Similarly, in the setting of suspected pulmonary embolism, iliocaval duplex was rated as rarely appropriate as a “stand-alone test” but as maybe appropriate when combined routinely with a lower extremity venous duplex examination in this setting. The indications of abdominal pain, abdominal bruit, and fever of unknown origin were all rated as rarely appropriate for IVC and iliac vein duplex. Duplex ultrasound of the IVC and iliac veins was rated as maybe appropriate for procedural planning prior to IVC filter placement.
Duplex of the IVC and Iliac Veins for Patency and Thrombosis.
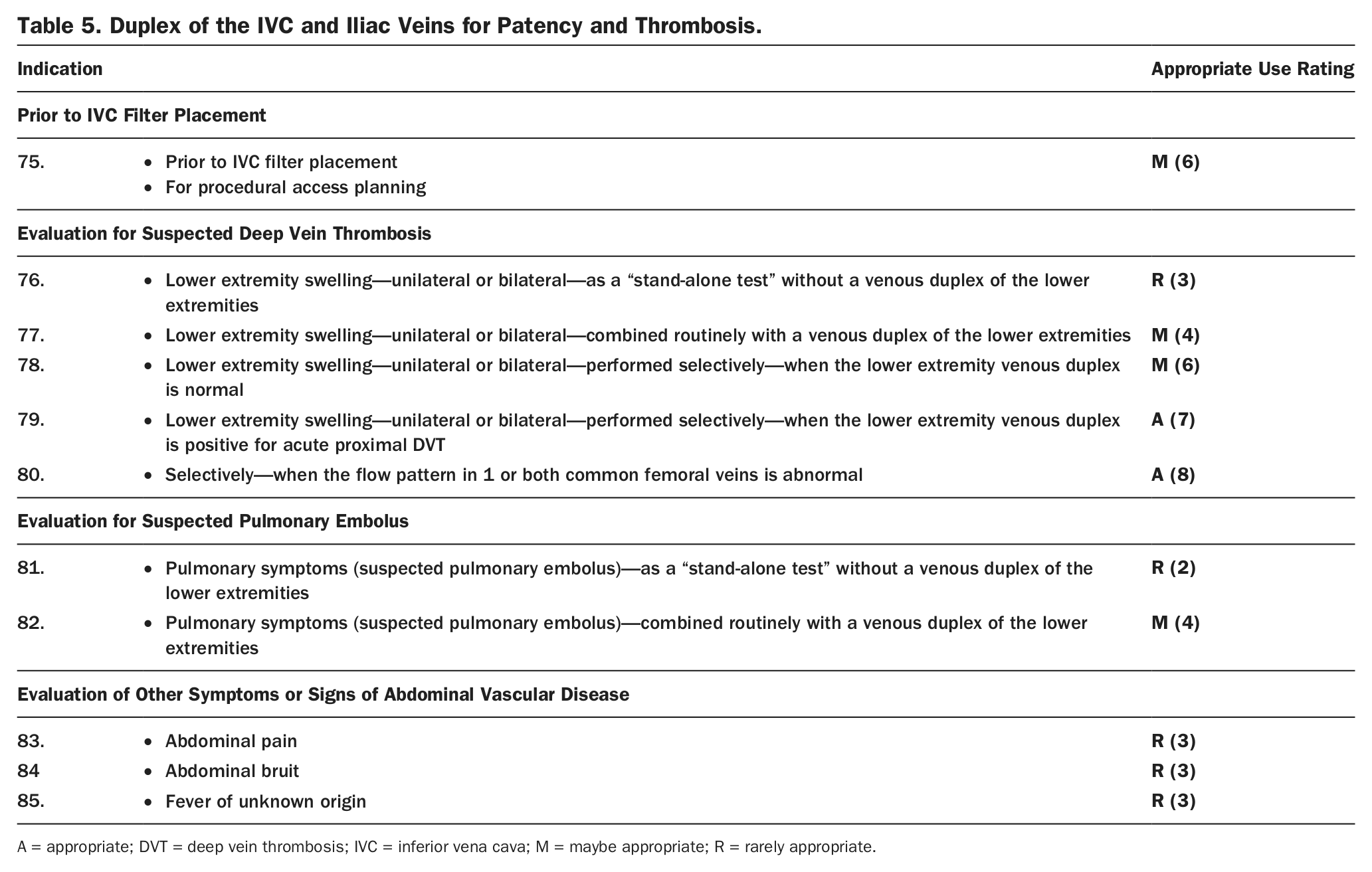
A = appropriate; DVT = deep vein thrombosis; IVC = inferior vena cava; M = maybe appropriate; R = rarely appropriate.
Section 4: Hepatoportal and Renal Venous Evaluation
Summary: Hepatoportal and Renal Venous Duplex Ultrasound
Duplex scanning of the hepatoportal system (Table 6) was rated as appropriate for the evaluation of cirrhosis without ascites, hepatomegaly and/or splenomegaly, and portal hypertension. Duplex scanning was rated as rarely appropriate as an initial diagnostic test in patients with jaundice but maybe appropriate for evaluation of patients with abnormal liver function tests and jaundice with no alternative diagnosis identified after an initial workup. Follow-up after a transjugular intrahepatic portosystemic shunt (TIPS) procedure was rated as appropriate for duplex scanning. Hepatoportal scanning was rated as maybe appropriate for abdominal pain and rarely appropriate for fever of unknown origin and cor pulmonale or pulmonary symptoms.
Duplex of the Hepatoportal System (Portal Vein, Hepatic Veins, Splenic Vein, Superior Mesenteric Vein, Inferior Vena Cava) for Patency, Thrombosis, and Flow Direction.*
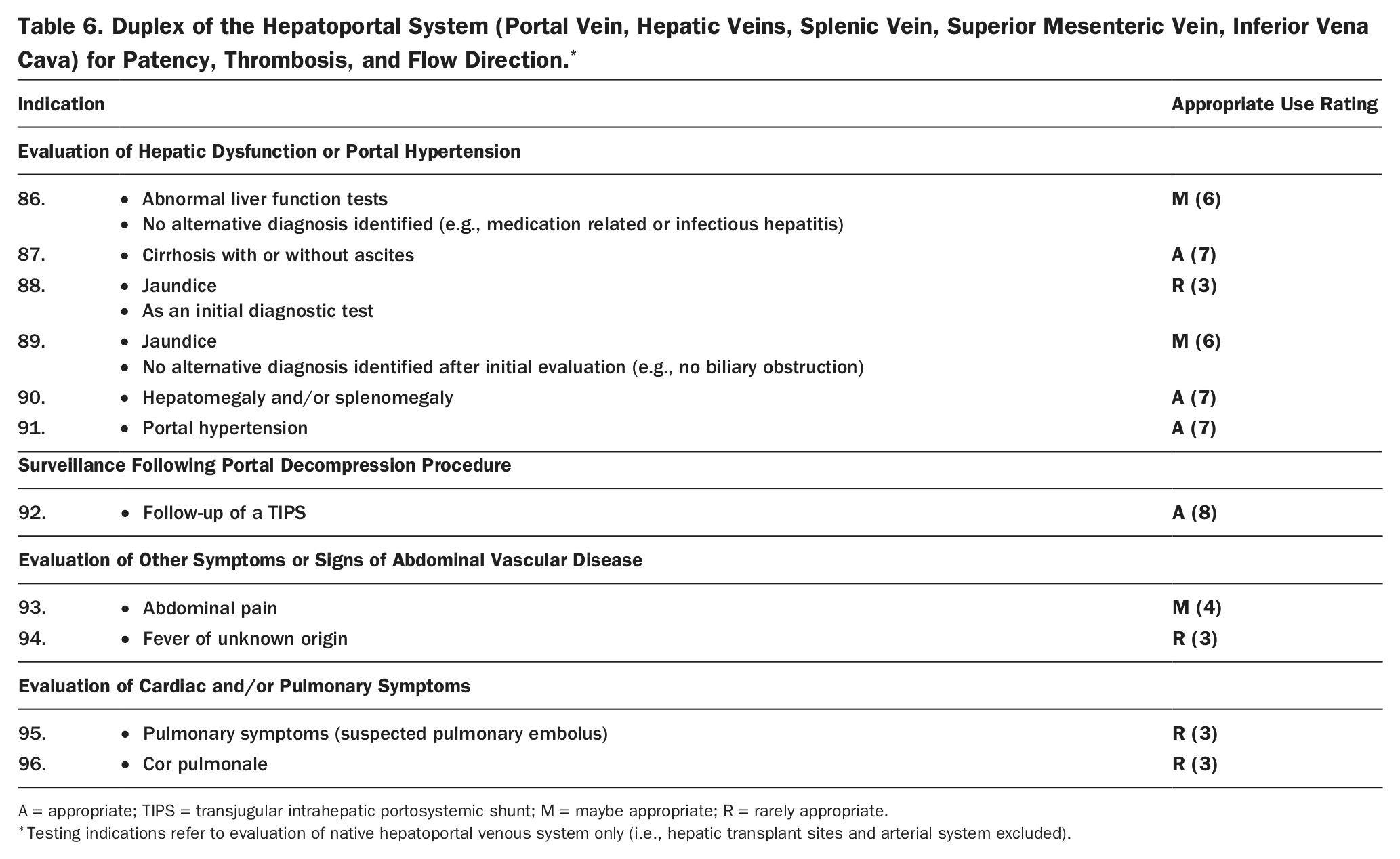
A = appropriate; TIPS = transjugular intrahepatic portosystemic shunt; M = maybe appropriate; R = rarely appropriate.
Testing indications refer to evaluation of native hepatoportal venous system only (i.e., hepatic transplant sites and arterial system excluded).
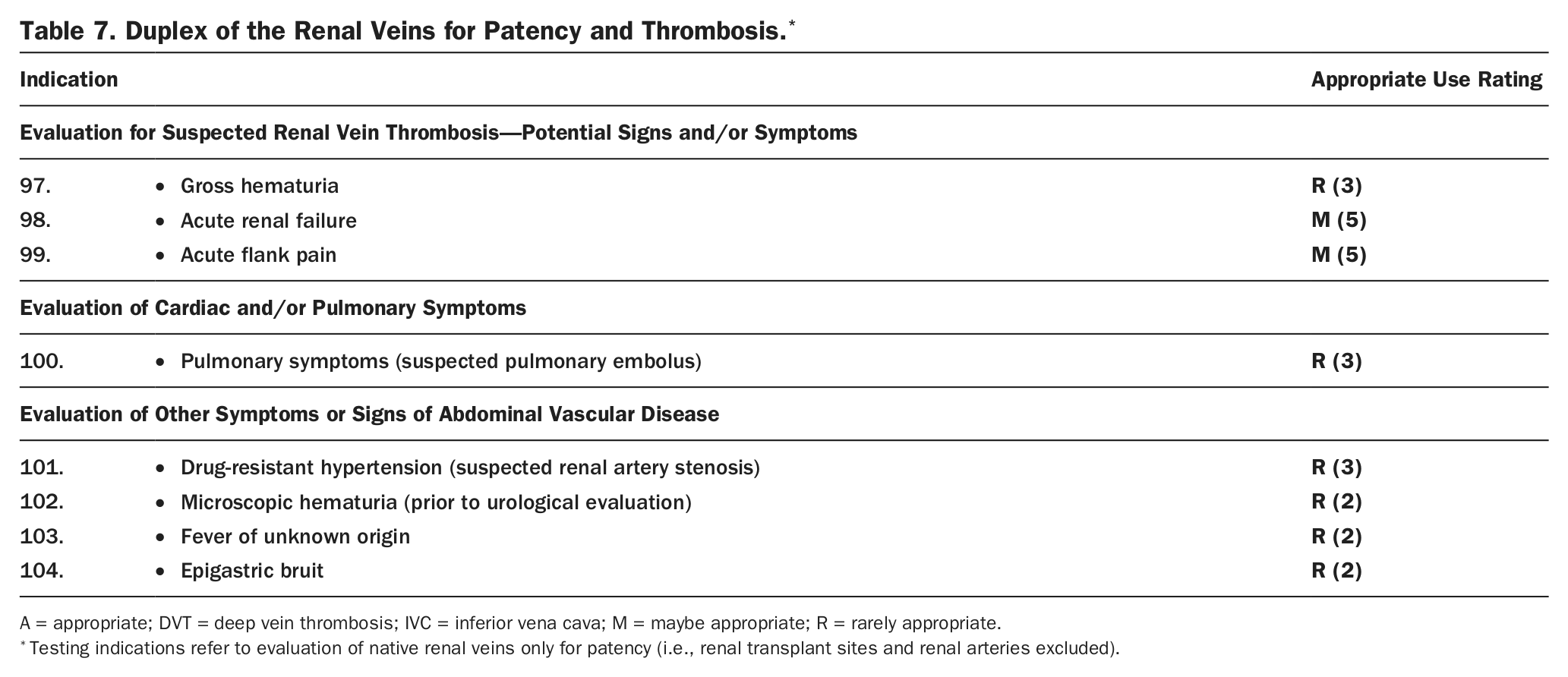
Likely reflecting the uncommon nature of isolated renal vein pathology as a cause of genitourinary symptoms or signs, there were no clinical indications rated as appropriate for assessment of the native renal veins with duplex ultrasound (Table 7) in this document. For the indications of acute renal failure and acute flank pain, symptoms of renal vein thrombosis, renal vein duplex ultrasound was rated as maybe appropriate. Renal venous duplex was rated as rarely appropriate for evaluation of gross or microscopic hematuria, pulmonary symptoms, or fever of unknown origin. Renal venous duplex was rated as rarely appropriate for evaluation of epigastric bruit or drug-resistant hypertension, scenarios for which arterial duplex testing would be a more appropriate test (1).
Duplex of the Renal Veins for Patency and Thrombosis.*
A = appropriate; DVT = deep vein thrombosis; IVC = inferior vena cava; M = maybe appropriate; R = rarely appropriate.
Testing indications refer to evaluation of native renal veins only for patency (i.e., renal transplant sites and renal arteries excluded).
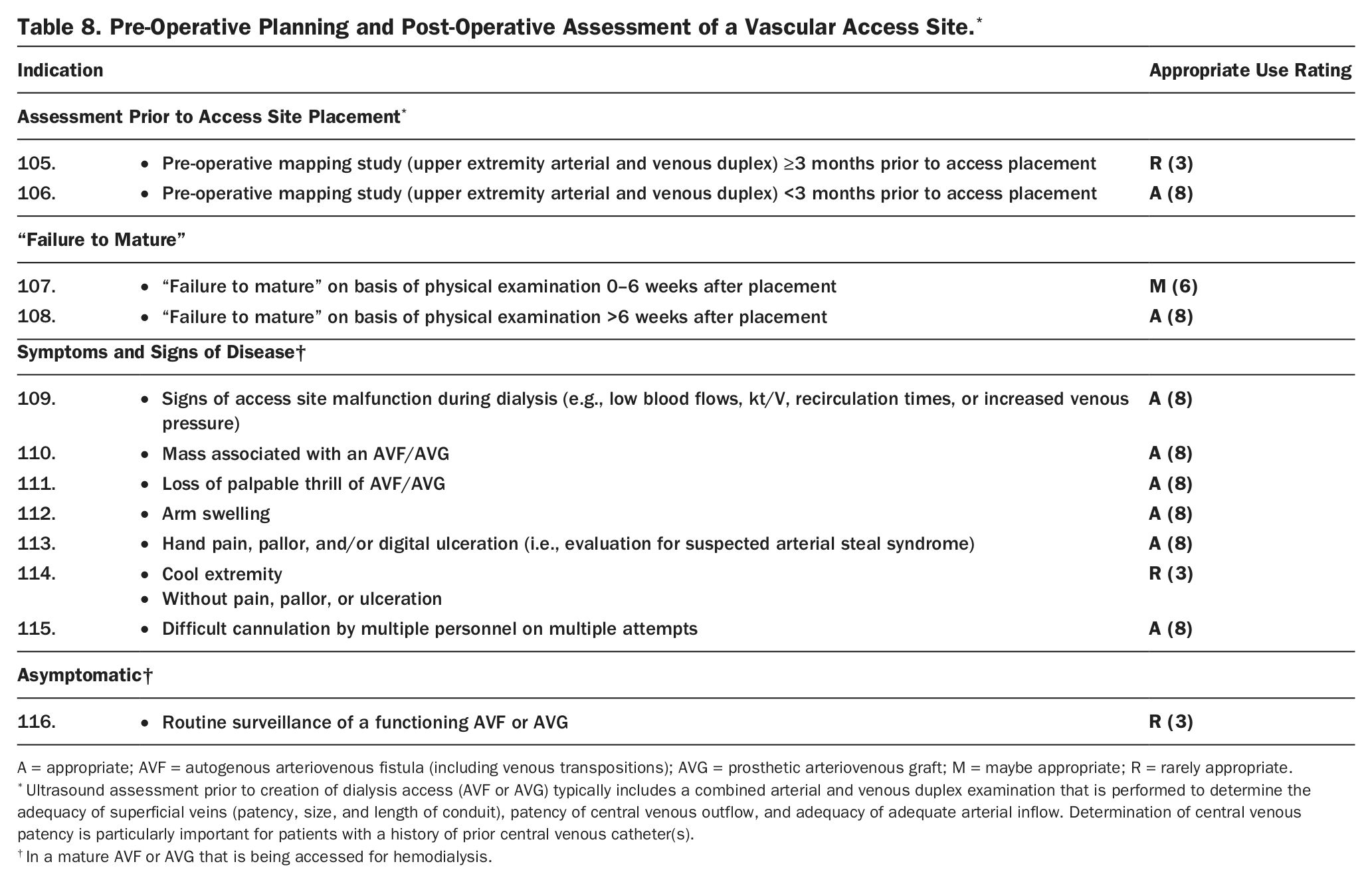
Pre-Operative Planning and Post-Operative Assessment of a Vascular Access Site.*
A = appropriate; AVF = autogenous arteriovenous fistula (including venous transpositions); AVG = prosthetic arteriovenous graft; M = maybe appropriate; R = rarely appropriate.
Ultrasound assessment prior to creation of dialysis access (AVF or AVG) typically includes a combined arterial and venous duplex examination that is performed to determine the adequacy of superficial veins (patency, size, and length of conduit), patency of central venous outflow, and adequacy of adequate arterial inflow. Determination of central venous patency is particularly important for patients with a history of prior central venous catheter(s).
In a mature AVF or AVG that is being accessed for hemodialysis.
Section 5: Hemodialysis Vascular Access Duplex Ultrasound
Summary: Hemodialysis Vascular Access Duplex Ultrasound
For vascular assessment (or mapping) prior to the placement of hemodialysis access, duplex ultrasound was rated as appropriate when performed less than 3 months prior to the procedure. Vascular assessment prior to access placement was rated as rarely appropriate when performed earlier than this time, reflecting the potential for interval development of vascular lesions in the hemodialysis patient (e.g., superficial or deep vein thromboses). Following dialysis access placement, indications were rated according to presence and nature of symptoms and time interval following access placement. For the assessment of access that has failed to mature on the basis of physical examination findings, duplex ultrasound was rated as an appropriate test beyond 6 weeks after access placement and maybe appropriate within 0 to 6 weeks of placement. Duplex ultrasound was rated as an appropriate test for most clinical scenarios related to upper extremity symptoms in the patient with mature dialysis access, including mass associated with an autogenous arteriovenous fistula (AVF)/prosthetic arteriovenous graft (AVG), arm swelling, or signs of digital ischemia due to steal phenomenon (hand pallor, pain, or ulceration). Similarly, duplex ultrasound was rated as an appropriate test for signs of malfunction and/or occlusion in a mature and previously functional AVF/AVG, including repeated difficulties with access cannulation, low flow or other signs of malfunction during dialysis sessions, and loss of palpable thrill over the access. Evaluation of a cool, but otherwise entirely asymptomatic, upper extremity with duplex ultrasound was rated as rarely appropriate. The technical panel rated routine duplex surveillance of a functional AVF/AVG in an asymptomatic patient with no signs of access malfunction as rarely appropriate.
7. Discussion
The noninvasive vascular laboratory plays a central role in the evaluation and surveillance of peripheral vascular disorders. The scope of this document includes common and less common clinical indications encountered among patients with suspected or known venous disease, the most common of which being venous thromboembolism (e.g., DVT, pulmonary embolism, and superficial thrombophlebitis) and chronic venous insufficiency, either due to primary varicose veins or secondary to prior DVT (post-thrombotic syndrome) or other nonthrombotic venous pathology (e.g., congenital venous anomaly). Indications for vascular testing prior to or after placement of hemodialysis access are included in this document, as evaluation of the superficial, deep, and central veins of the upper extremity constitutes a large component of these examinations. It is assumed that protocols for assessment prior to and following hemodialysis access will also include imaging of the arterial system, as determined by the clinical indication and type of dialysis access.
Due to the diversity of peripheral vascular disorders, it is likely that many potential clinical indications are not included in this document. Rather than an exhaustive compendium of clinical indications, it is intended that this document address the most common and important clinical scenarios encountered in the patient with manifestations of peripheral vascular disease. Although this document largely focuses on ratings for duplex ultrasound, some common clinical indications for venous physiological testing were included, recognizing that physiological testing is used in some clinical centers as a tool for evaluation of the patient with lower extremity symptoms suspicious for venous disease. Importantly, venous physiological testing was rated as rarely appropriate for evaluation of the patient with acute lower extremity swelling and suspected DVT, for whom venous duplex ultrasound was rated an appropriate test.
It is intended that this document, along with appropriate use criteria for arterial testing published in 2012 (1), will provide guidance for clinicians in maximizing the appropriate use of the noninvasive vascular laboratory for the care of patients with suspected or known peripheral vascular disorders. In addition, it is intended that this document identify critical evidence gaps in the field and serve as a reference for policy makers with regard to noninvasive vascular testing. Although the Part I and Part II Peripheral Vascular Ultrasound AUC documents share a common intent, methodology, and structure, there are important differences to note. In the Part I document, 159 clinical indications related to arterial testing were rated, including numerous indications which rated timing of surveillance studies either prior to (e.g., asymptomatic carotid artery stenosis) or following revascularization (e.g., testing for patency and restenosis of lower extremity bypass grafts and stents). Reflecting the more focused spectrum of pathology in the venous system, as well as fewer distinct vascular beds to image, this venous testing document presents ratings for 116 clinical indications. In the venous document, there are fewer indications related to repeated testing or surveillance of known disease. Although vascular testing is commonly repeated for surveillance of arterial atherosclerotic disease or aneurysms to determine the need for revascularization or repair (e.g., severe internal carotid artery stenosis or large abdominal aortic aneurysm), there are far fewer clinical scenarios in which surveillance testing for venous disease is performed (e.g., for surveillance of known calf DVT with contraindication to anticoagulation). Similarly, unlike the arterial document in which multiple clinical indications for testing following surgical or endovascular treatment were rated, the role of duplex ultrasound for follow-up after venous procedures (e.g., pharmacomechanical thrombolysis or venous stenting for DVT) is not as well established. Finally, it is important to note that the Part II venous testing document incorporates clinical indication classification terminology that has been revised since publication of the arterial document (appropriate care, maybe appropriate care, rarely appropriate care).
Summary of Evidence and Call for Additional Research
The current evidence base and clinical practice guidelines were used to develop and rate the clinical indications whenever available, although for a large number of clinical indications, the available scientific literature was limited and clinical consensus or expert opinion played a larger role. Clinical practice guidelines and additional literature reviewed are presented in the Online Appendix. Specifically, with regard to diagnosis of DVT, the writing committee reviewed recently published guidelines from the American College of Chest Physicians (ACCP) (8) and recognized that the ACCP document serves to provide global diagnostic algorithms for venous thromboembolism that incorporate pre-test probability assessment, D-dimer testing, and alternative imaging modalities, the scope of which is beyond that of this appropriate use document that focused on venous duplex ultrasound and physiological testing. In addition, the consensus of the writing committee, in contrast with that of the ACCP guidelines, is that the entire lower extremity (whole-leg ultrasound including the calf veins) should be evaluated in cases of suspected lower extremity DVT when technically possible.
As was the case for arterial testing, the writing committee recognizes a need for clinical and cost-effectiveness studies focused specifically on noninvasive testing for venous disease. The writing committee identifies the following areas as among those in greatest need of focused research:
Comparative clinical and cost effectiveness of various algorithms for diagnosis of DVT, including pre-test probability assessment tools (e.g., Wells score), D-dimer, and venous duplex ultrasound.
Comparative clinical and cost effectiveness of clinical algorithms incorporating venous duplex testing for the diagnosis of pulmonary embolism.
Role of venous duplex ultrasound in clinical algorithms to determine duration of anticoagulation therapy among patients with unprovoked DVT.
Comparison of anticoagulation therapy versus duplex ultrasound surveillance among patients with isolated calf DVT.
Accuracy and clinical benefit of venous duplex ultrasound following venous intervention (e.g., pharmacomechanical thrombolysis, angioplasty, stenting).
Optimal timing and utilization of duplex ultrasound in clinical practice for assessment of dialysis access maturity.
Footnotes
Appendix A: Additional Methods
See the Methods section of the report for a description of panel selection, indication development, scope of indications, and rating process.