
Abstract
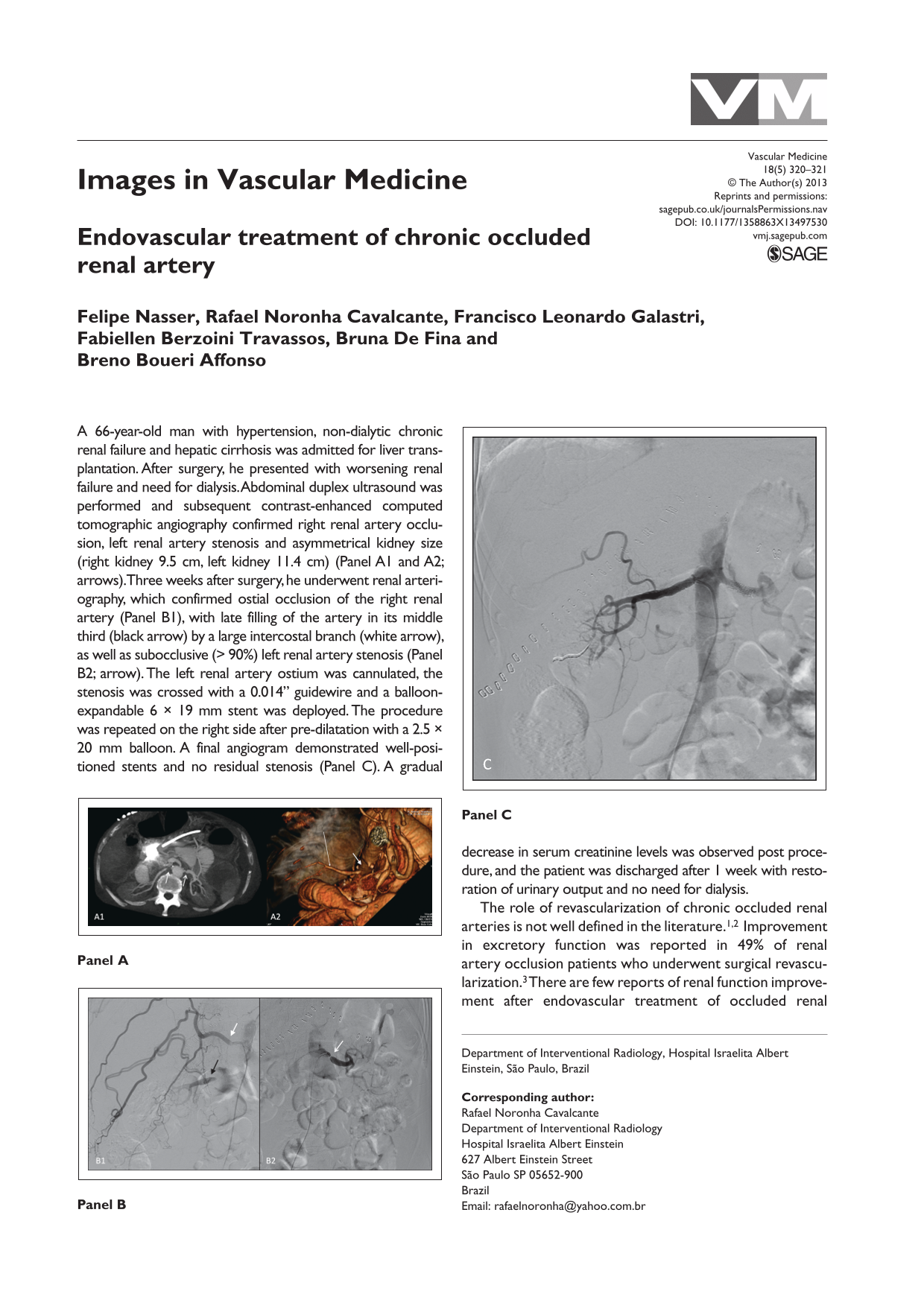
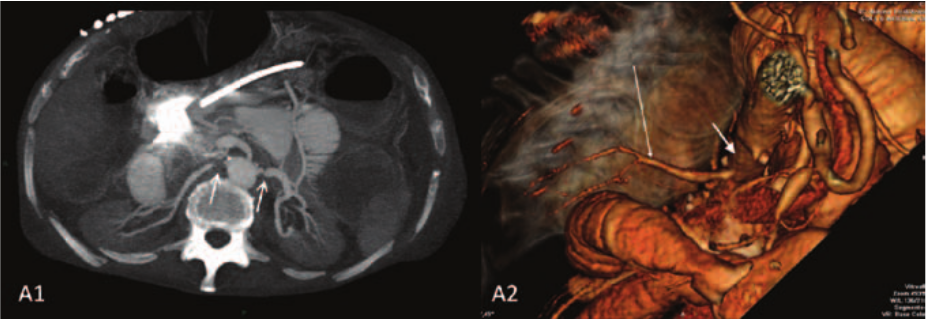
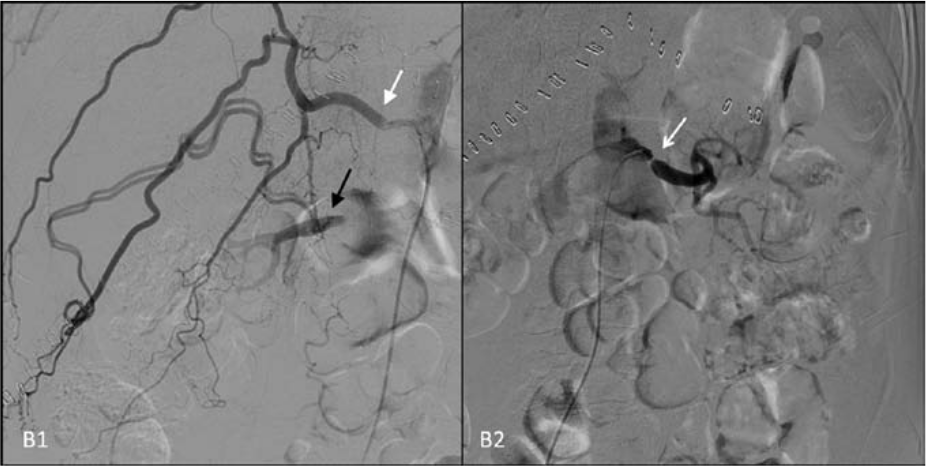
A 66-year-old man with hypertension, non-dialytic chronic renal failure and hepatic cirrhosis was admitted for liver transplantation. After surgery, he presented with worsening renal failure and need for dialysis. Abdominal duplex ultrasound was performed and subsequent contrast-enhanced computed tomographic angiography confirmed right renal artery occlusion, left renal artery stenosis and asymmetrical kidney size (right kidney 9.5 cm, left kidney 11.4 cm) (Panel A1 and A2; arrows). Three weeks after surgery, he underwent renal arteriography, which confirmed ostial occlusion of the right renal artery (Panel B1), with late filling of the artery in its middle third (black arrow) by a large intercostal branch (white arrow), as well as subocclusive (> 90%) left renal artery stenosis (Panel B2; arrow). The left renal artery ostium was cannulated, the stenosis was crossed with a 0.014” guidewire and a balloon-expandable 6 × 19 mm stent was deployed. The procedure was repeated on the right side after pre-dilatation with a 2.5 × 20 mm balloon. A final angiogram demonstrated well-positioned stents and no residual stenosis (Panel C). A gradual decrease in serum creatinine levels was observed post procedure, and the patient was discharged after 1 week with restoration of urinary output and no need for dialysis.

The role of revascularization of chronic occluded renal arteries is not well defined in the literature.1,2 Improvement in excretory function was reported in 49% of renal artery occlusion patients who underwent surgical revascularization. 3 There are few reports of renal function improvement after endovascular treatment of occluded renal arteries.1,2,4,5 Dwyer et al. reported improvement in five cases of acute renal failure that underwent successful endovascular treatment. 5 In this case, the revascularization of the occluded renal artery was adequate because the kidney was still viable; however, treatment of the contralateral subocclusive stenosis also played a major role in the renal function improvement observed during follow-up.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Mark A Creager, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.