
Abstract
A 75-year-old man presented to his general practitioner for evaluation of vague abdominal pain. His medical history was significant for hypertension and an episode of left eye retinal vein occlusion that occurred 15 years before and completely recovered with medical treatment. Clinical examination revealed a large, non-tender, pulsatile mass in the epigastric region.
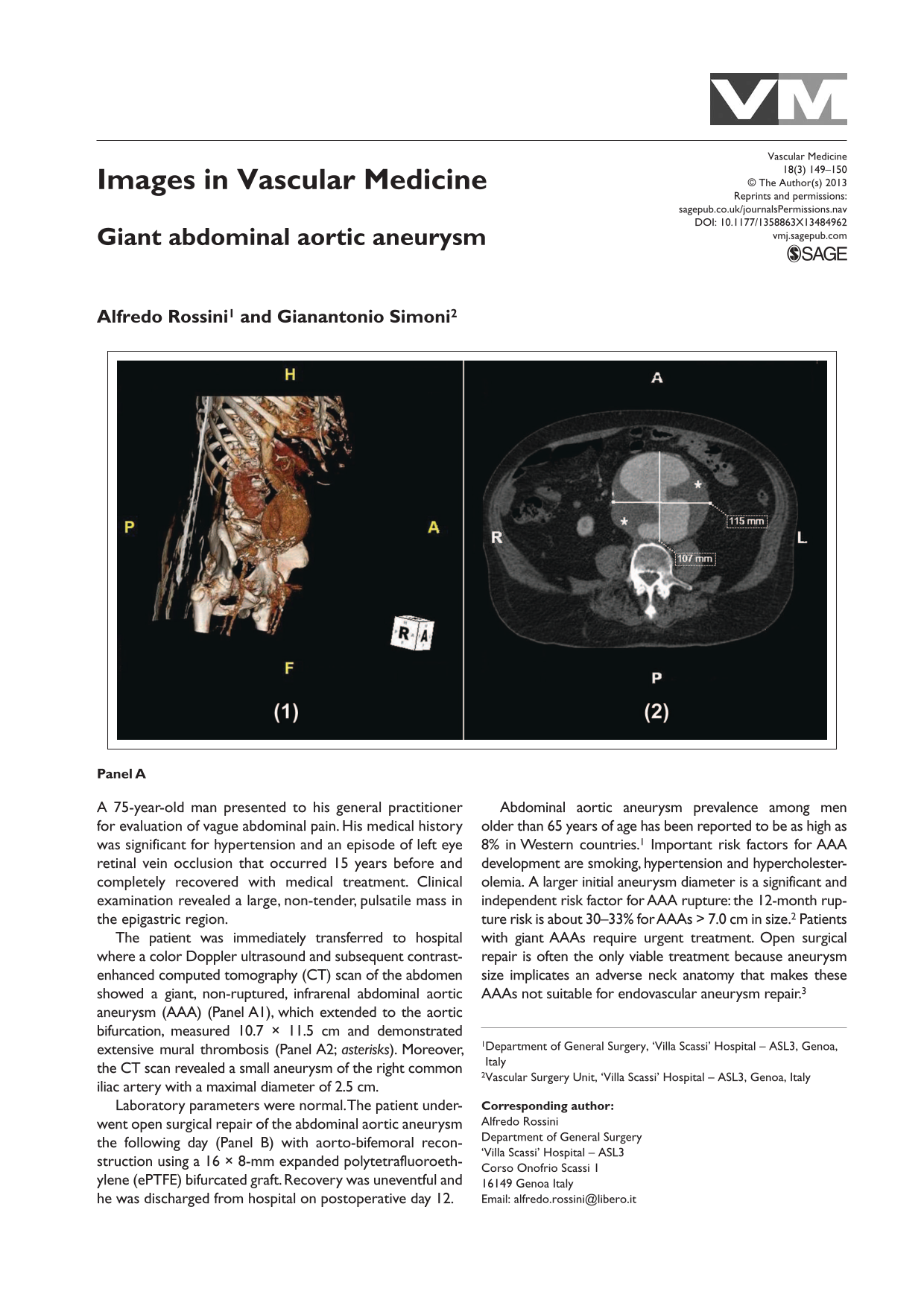
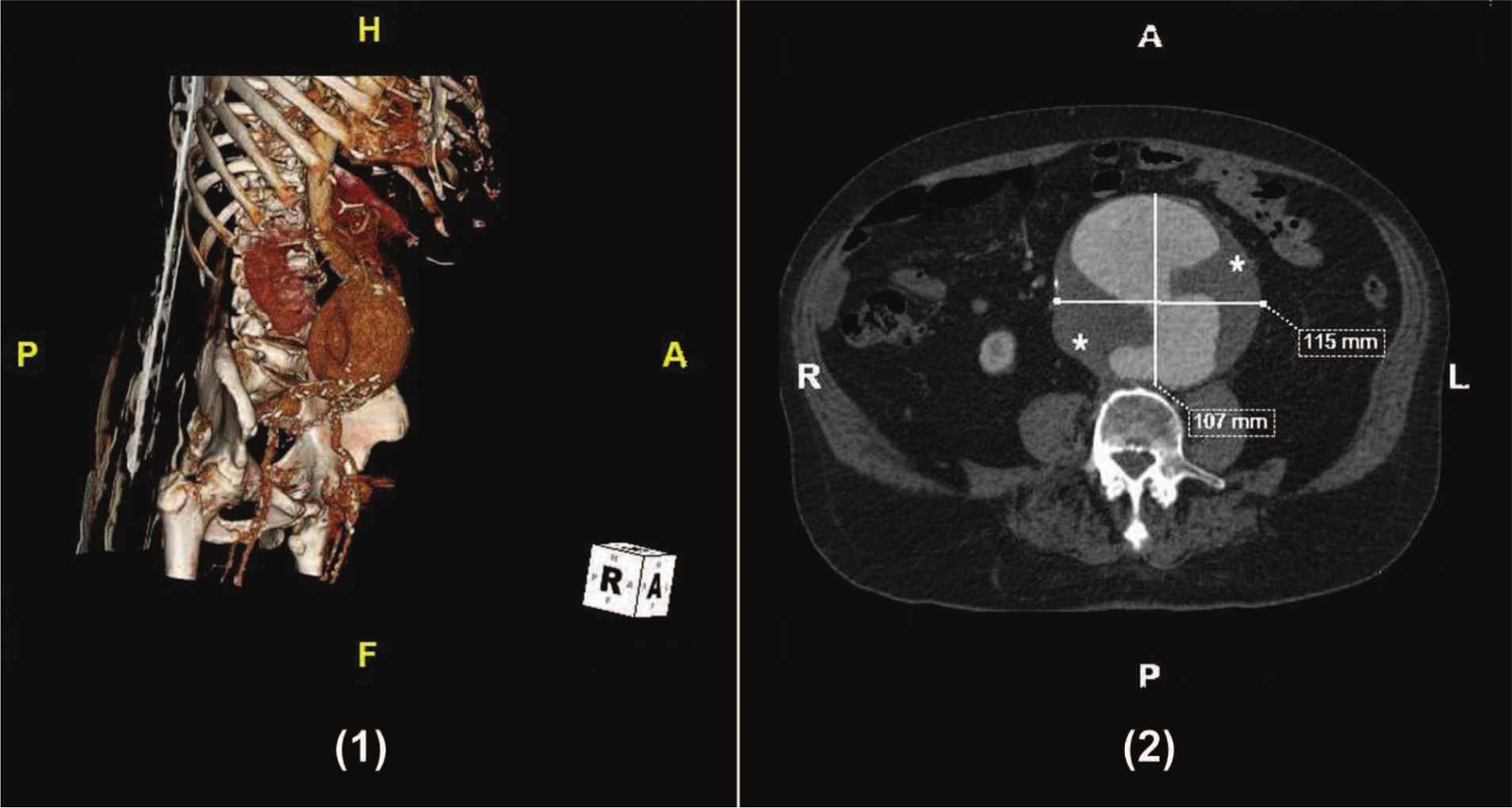
The patient was immediately transferred to hospital where a color Doppler ultrasound and subsequent contrast-enhanced computed tomography (CT) scan of the abdomen showed a giant, non-ruptured, infrarenal abdominal aortic aneurysm (AAA) (Panel A1), which extended to the aortic bifurcation, measured 10.7 × 11.5 cm and demonstrated extensive mural thrombosis (Panel A2; asterisks). Moreover, the CT scan revealed a small aneurysm of the right common iliac artery with a maximal diameter of 2.5 cm.
Laboratory parameters were normal. The patient underwent open surgical repair of the abdominal aortic aneurysm the following day (Panel B) with aorto-bifemoral reconstruction using a 16 × 8-mm expanded polytetrafluoroethylene (ePTFE) bifurcated graft. Recovery was uneventful and he was discharged from hospital on postoperative day 12.

Abdominal aortic aneurysm prevalence among men older than 65 years of age has been reported to be as high as 8% in Western countries. 1 Important risk factors for AAA development are smoking, hypertension and hypercholesterolemia. A larger initial aneurysm diameter is a significant and independent risk factor for AAA rupture: the 12-month rupture risk is about 30–33% for AAAs > 7.0 cm in size. 2 Patients with giant AAAs require urgent treatment. Open surgical repair is often the only viable treatment because aneurysm size implicates an adverse neck anatomy that makes these AAAs not suitable for endovascular aneurysm repair. 3
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Mark A Creager, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Conflict of interest
All authors have no conflicts of interest or financial ties to disclose.
Funding
This research received no specific grant from any agency in the public, commercial, or not-for-profit sectors.