
Abstract
Patients with peripheral artery disease (PAD) have higher cardiovascular event rates than patients with established coronary artery disease (CAD) and abnormal endothelial function predicts cardiovascular risk in PAD and CAD. We investigated the hypothesis that PAD is associated with a greater degree of impairment in vascular function than CAD. We used several non-invasive tests to evaluate endothelial function in 1320 men and women with combined PAD and CAD (n = 198), PAD alone (n = 179), CAD alone (n = 466), or controls aged > 45 years without CAD or PAD (n = 477). Patients with PAD had lower brachial artery flow-mediated dilation (5.1 ± 3.9% PAD and CAD, 5.9 ± 4.4% PAD alone) compared to patients with CAD alone (7.0 ± 4.5%) and no PAD or CAD (8.1 ± 5.1%, p < 0.0001). In multivariable models adjusting for clinical covariates and the presence of CAD, PAD remained associated with lower flow-mediated dilation (p < 0.0001). PAD was associated also with lower nitroglycerin-mediated dilation and reactive hyperemia. Patients with both PAD and CAD had a lower digital pulse amplitude tonometry (PAT) ratio in unadjusted models but not in adjusted models. Flow-mediated dilation was modestly associated with PAT ratio in patients with atherosclerotic disease (r = 0.23, p < 0.0001) but not among control participants (r = 0.008, p = 0.93). Our findings indicate that patients with PAD have greater impairment of vasodilator function and are consistent with the possibility that endothelial dysfunction may contribute to adverse cardiovascular prognosis in PAD.
Introduction
Peripheral artery disease (PAD) affects over 8 million people in the United States with a rising prevalence driven by population aging. 1 In addition to the lower extremity manifestations, PAD confers a markedly increased risk of cardiovascular complications. 2 Compared to patients with CAD, PAD patients have even higher rates of cardiovascular mortality and events. 3 The mechanisms underlying the elevated risk in PAD patients remain incompletely understood.
It is well-established that endothelial dysfunction is a potent mediator of atherogenesis.4,5 Decreased nitric oxide bioavailability promotes inflammation, thrombosis and vasoconstriction, all of which contribute to the development and clinical manifestations of atherosclerosis. 6 In PAD patients, the presence of endothelial dysfunction redicts the occurrence of cardiovascular events.7–10 Endothelial function has also been associated with the severity of lower extremity arterial obstruction. 11 Further, beneficial interventions including supervised exercise improve endothelial function in PAD patients. 12
Importantly, the risk factors and clinical course of PAD are not identical to CAD, raising the possibility that there may be distinct aspects of pathophysiology.13–15 Thus, in the present study, we investigated the hypothesis that PAD is associated with a greater degree of impairment in vascular function than CAD. We evaluated flow-mediated dilation in a large cohort including patients with clinically established PAD, CAD, and controls without clinical PAD or CAD.
Methods
Study participants
Baseline ultrasound and risk factor data were pooled from 1320 participants who had participated in published and unpublished studies of endothelial function at Boston Medical Center between 1994 and 2011. For the present study, we included all individuals with available flow-mediated dilation testing from four groups: (1) patients with clinically established PAD; (2) patients with stable CAD without clinically evident PAD; (3) patients with both CAD and PAD; and (4) individuals with age ≥ 45 years without PAD or CAD. Patients with CAD and/or PAD were enrolled from inpatient and outpatient cardiovascular and vascular surgery services. CAD was defined based on prior angiography, exercise test, or documented history of myocardial infarction. Of the 377 patients with PAD, 27% had critical limb ischemia, 70% had claudication, and 3% were asymptomatic with prior revascularization. All participants gave written informed consent, and the Boston Medical Center Institutional Review Board approved all study protocols.
Study protocol
We evaluated risk factors and vascular function in a consistent fashion across the study period.16,17 Clinical history and relevant clinical covariates were compiled from participant interviews and medical records. Blood pressure was assessed with an automatic recorder (Dinamap; General Electric Healthcare). Body mass index was calculated from measured weight and height. Measurement of cholesterol levels and fasting glucose were available in 1226 and 980 participants, respectively.
Brachial measures of vascular function
After a 10-minute rest period, we evaluated the brachial artery diameter using high-resolution ultrasound before and 1-minute following induction of reactive hyperemia by a 5-minute upper arm cuff occlusion. Brachial artery flow velocity was assessed using pulsed Doppler at rest and for 15 seconds after cuff release, as previously described. 16 We measured the brachial artery diameter before and 3 minutes after administration of 0.4 mg sublingual nitroglycerin. Nitroglycerin was not given if the participant declined or had previous adverse reactions to nitroglycerin, migraine headaches, severe carotid stenosis, systolic blood pressure < 100 mmHg, or had used sildenafil, tadalafil, or vardenafil within 1 week of the study. Therefore, nitroglycerin-mediated dilation measurement was available in 559 participants (n = 232 no CAD or PAD, n = 198 CAD alone, n = 63 PAD alone, n = 66 PAD and CAD). We measured brachial artery diameters in a blinded manner with commercially available software that uses automated border detection (Medical Imaging Applications, LLC, Coralville, IA, USA). 17
Digital measures of vascular function
In 2003, we began assessing microvessel endothelial function in the fingertip with pulse amplitude tonometry (EndoPAT; Itamar Medical, Caesarea, Israel). Thus, we have available simultaneous flow-mediated dilation and PAT studies in 497 participants (n = 135 no CAD or PAD, n = 152 CAD alone, n = 88 PAD alone, n = 122 PAD and CAD). We express the PAT result as the natural logarithm of the ratio of the pulse amplitude during the 90–120 second period after cuff release in the test finger to the baseline amplitude divided by the similar ratio from the contralateral control finger (lnPAT ratio).18,19
Statistical analysis
We compared clinical characteristics between the four groups (no PAD or CAD, CAD alone, PAD alone, PAD and CAD) using one-way ANOVA or chi-squared testing for continuous or categorical data, respectively. We compared vascular responses across the four groups using one-way ANOVA with post hoc testing by Tukey’s test. We performed multivariable linear regression models to evaluate the association of cardiovascular risk factors with brachial and digital vascular measures in patients with CAD alone compared to PAD (PAD alone and PAD with CAD). We performed two multivariable linear regression models comparing the relation of PAD to vascular function measures. The first adjusted for age, sex, and the presence of CAD. The second additionally adjusted for cardiovascular risk factors including: black race, diabetes mellitus, hypertension, hypercholesterolemia, smoking history, and family history of CAD. In secondary analyses, measured lipid values, glucose, blood pressure, and body mass index or cardiovascular medications were included as covariates. Data are reported as mean ± SD, unless otherwise specified. Two-sided p < 0.05 was considered statistically significant. Analyses were performed using IBM SPSS Statistics 20.
Results
Study population
Clinical characteristics are summarized in Table 1. Overall, the cohort had a mean age of 62 ± 11 years with 35% women and 24% black race. As would be anticipated, the prevalence of cardiovascular risk factors was higher in the participants with clinical CAD and/or PAD. Use of cardiovascular medications also differed across the groups of participants.
Clinical characteristics.
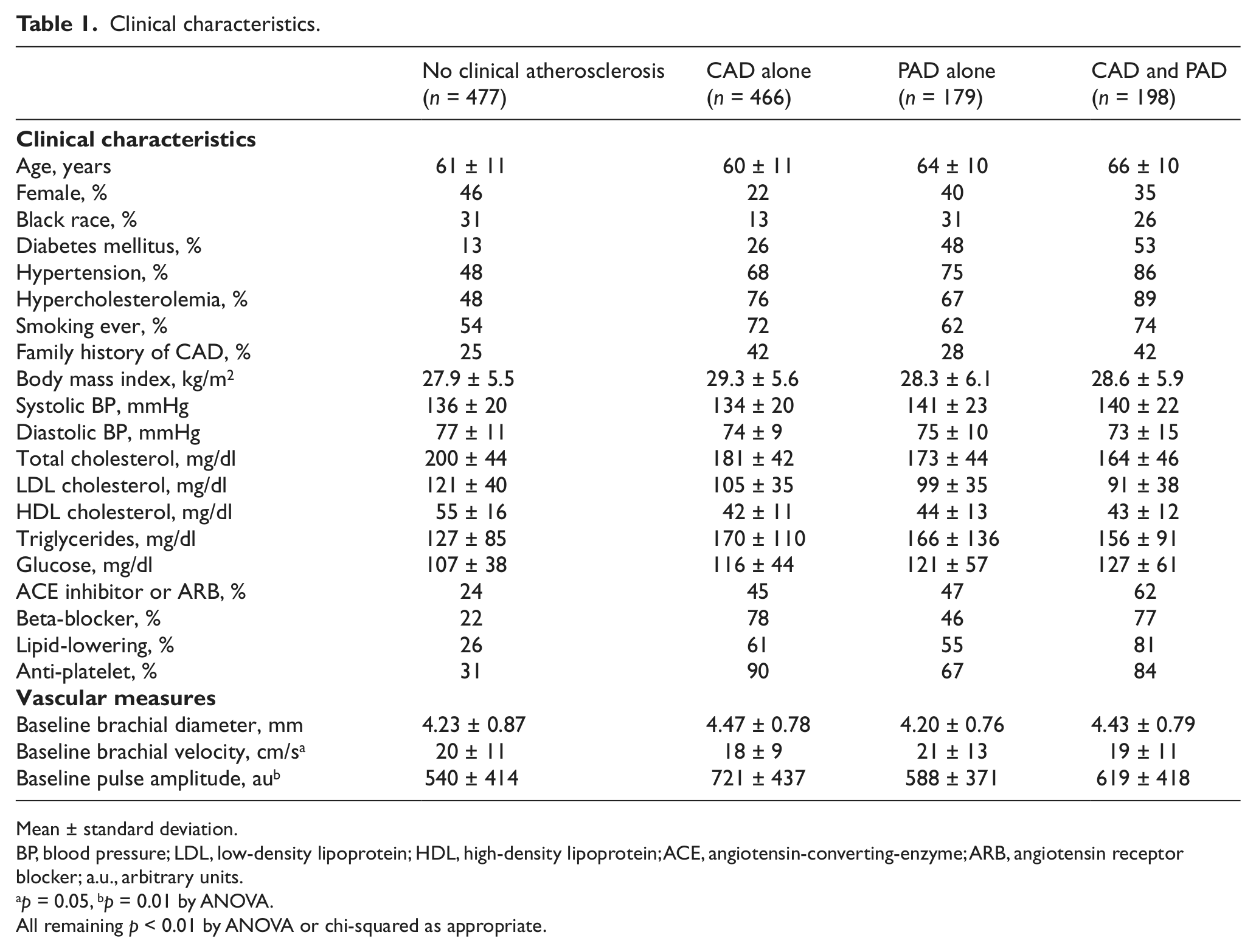
Mean ± standard deviation.
BP, blood pressure; LDL, low-density lipoprotein; HDL, high-density lipoprotein; ACE, angiotensin-converting-enzyme; ARB, angiotensin receptor blocker; a.u., arbitrary units.
p = 0.05, bp = 0.01 by ANOVA.
All remaining p < 0.01 by ANOVA or chi-squared as appropriate.
Brachial measures of vascular function
As shown in Figure 1, flow-mediated dilation of the brachial artery was lower in the patients with PAD as compared to both patients with CAD and control participants without atherosclerosis. Patients with PAD combined with CAD had similar flow-mediated dilation responses to patients with PAD alone.
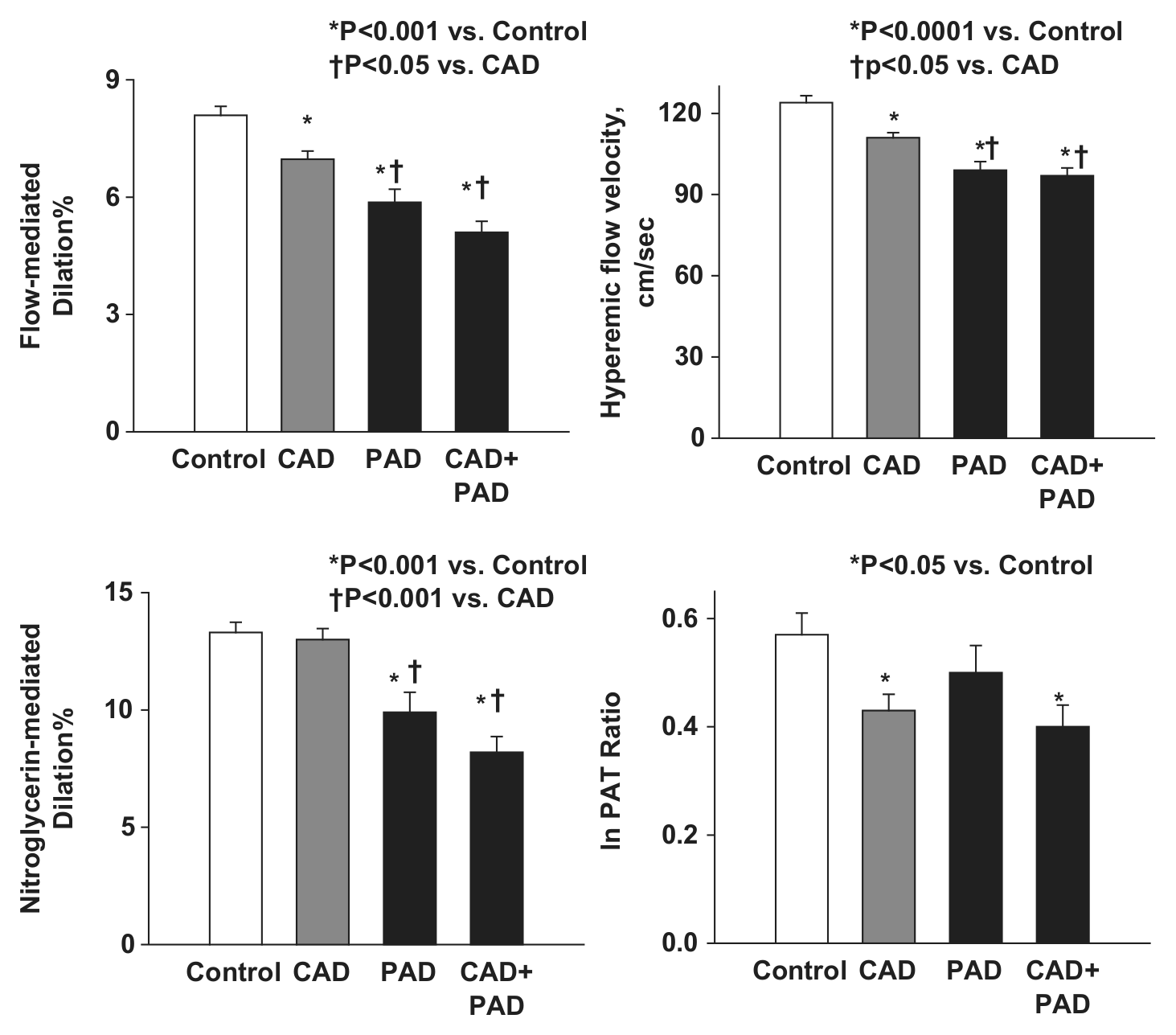
Displayed are mean (± standard error of the mean) flow-mediated dilation (n = 1320), nitroglycerin-mediated dilation (n = 559), hyperemic flow velocity (n = 1239), and lnPAT ratio (n = 497) by the four study groups: controls without CAD or PAD, CAD alone, PAD alone, and PAD combined with CAD. Overall ANOVA p < 0.01 for all four measures. The p-values detailed in the figure are from post hoc between-group testing by Tukey’s test.
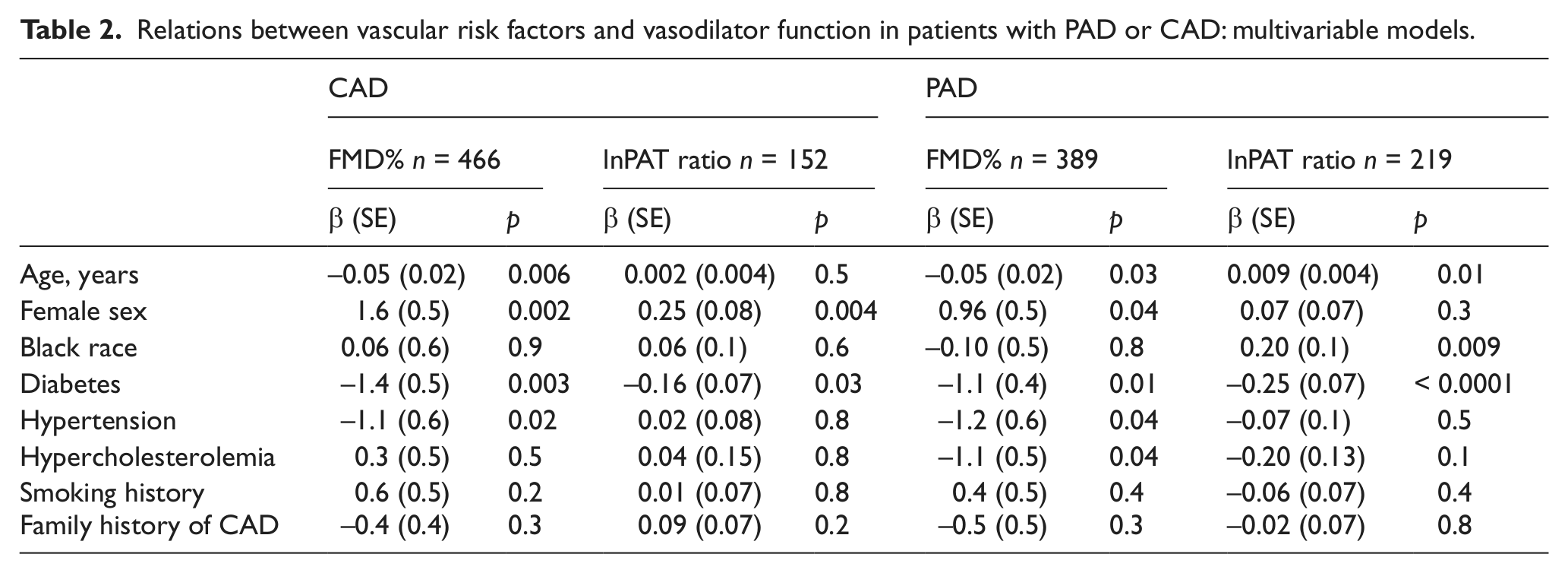
As shown in Table 2, advancing age, male sex, diabetes, and hypertension were associated with lower flow-mediated dilation in patients with CAD alone and in patients with PAD.
Relations between vascular risk factors and vasodilator function in patients with PAD or CAD: multivariable models.
The association of PAD with lower flow-mediated dilation persisted in multivariable models as shown in Table 3. In secondary analyses including serum lipids, glucose, measured blood pressure, and body mass index as covariates, the results were similar. In secondary analyses including cardiovascular medications as covariates, the results were similar. In secondary analyses excluding patients with critical limb ischemia, the results were similar.
Relation of PAD and vascular function: multivariable models.
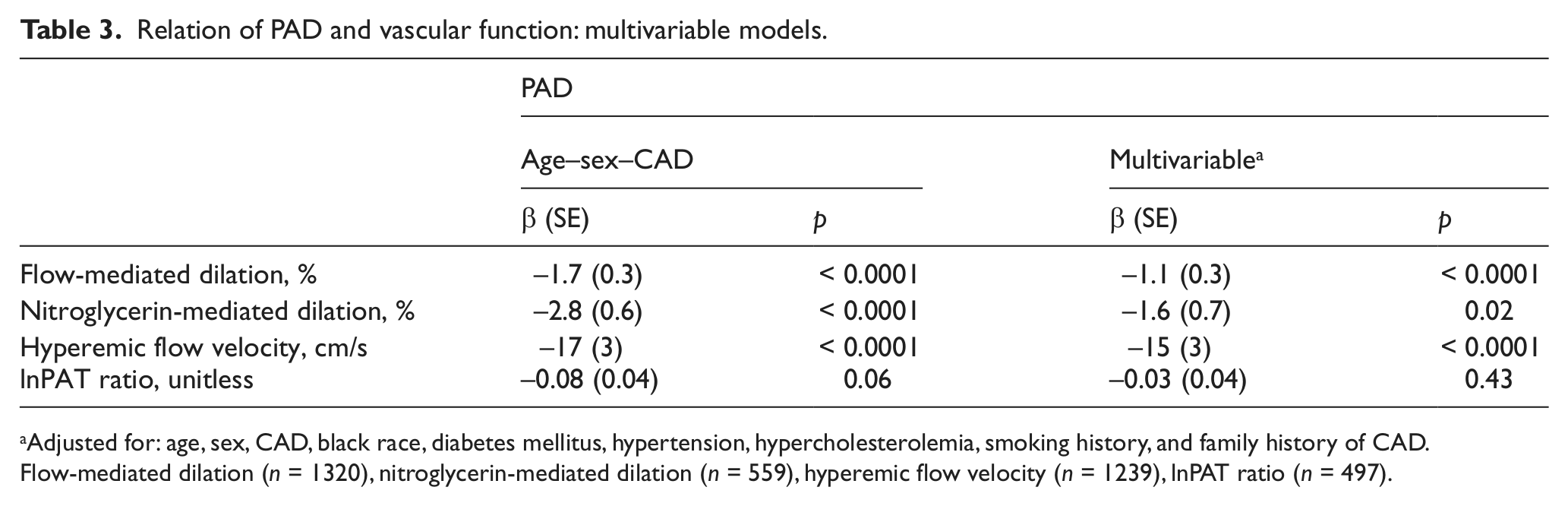
Adjusted for: age, sex, CAD, black race, diabetes mellitus, hypertension, hypercholesterolemia, smoking history, and family history of CAD.
Flow-mediated dilation (n = 1320), nitroglycerin-mediated dilation (n = 559), hyperemic flow velocity (n = 1239), lnPAT ratio (n = 497).
The extent of reactive hyperemia, a measure of microvascular dilation, was also lower in patients with PAD compared to both CAD and control participants in both unadjusted (Figure 1) and multivariable models (Table 3). In the full multivariable model additionally adjusted for hyperemic flow velocity, PAD remained associated with lower flow-mediated dilation (β = −0.96, p = 0.001).
In the participants with measurement of nitroglycerin-mediated dilation, PAD patients had a lower extent of dilation compared to CAD patients and control participants in unadjusted analyses (Figure 1). In the full multivariable model, the association of PAD with nitroglycerin-mediated dilation was attenuated but persisted (Table 3), suggesting that abnormal endothelium-independent vasodilator function in PAD may be attributable, in part, to concomitant risk factors.
Digital measures of vascular function
As shown in Figure 1, in the subset of participants with digital vascular testing, patients with combined PAD and CAD had lower digital vessel hyperemic response compared to control patients but were similar to CAD patients. As shown in Table 2, diabetes was associated with lower PAT response in patients with CAD and patients with PAD. Female sex was associated with higher PAT response in the patients with CAD and black race was associated with higher PAT response in the patients with PAD. In multivariable models, PAD was not associated with lower PAT hyperemic response (Table 3).
Comparison of brachial and digital measures of vascular function
As shown in Table 4, in the overall group of participants with simultaneous measurement of brachial and digital vasodilator function, there was a modest association of higher flow-mediated dilation with higher PAT response that persisted when adjusting for cardiovascular risk factors. When we separately evaluated the participants without clinical PAD or CAD from the patients with CAD and/or PAD, the association between brachial and digital vascular function persisted only in the presence of clinical atherosclerotic disease. There was not a significant association between reactive hyperemia measured in the brachial artery and the PAT hyperemic response in the entire cohort, or the group with clinical PAD and/or CAD.
Relation of digital and brachial vascular function.
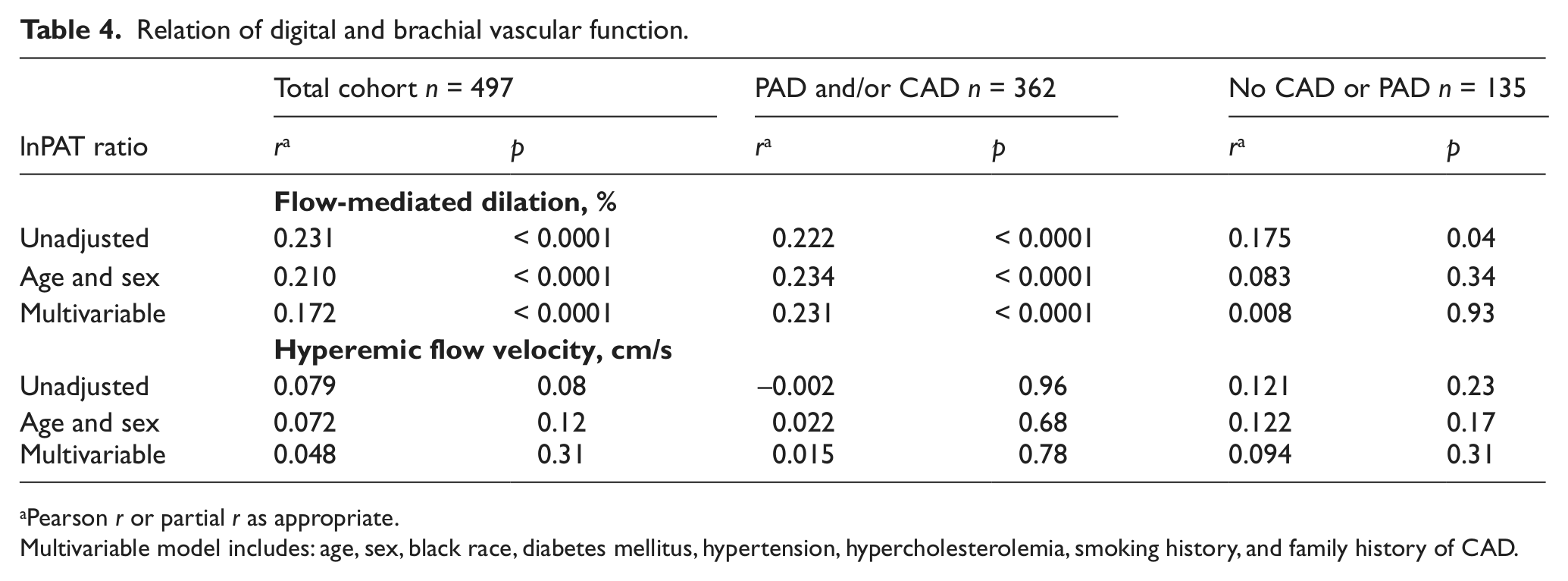
Pearson r or partial r as appropriate.
Multivariable model includes: age, sex, black race, diabetes mellitus, hypertension, hypercholesterolemia, smoking history, and family history of CAD.
Discussion
In a large cohort of patients, we found that patients with clinical PAD have impaired vasodilator function. Flow-mediated dilation, a measure of conduit artery dilation, and reactive hyperemia, a measure of microvessel dilation, were worse in the presence of PAD after adjusting for the presence of CAD and cardiovascular risk factors. We also observed lower nitroglycerin-mediated dilation in patients with PAD. PAD combined with CAD was associated with lower digital vasodilator response in unadjusted but not risk factor adjusted models. The association of digital and brachial vascular measures was isolated to patients with established atherosclerosis. Taken together, our findings demonstrate a pronounced abnormality of vascular function that may be relevant to the elevated cardiovascular event rate in PAD patients.
Prior studies with much smaller patient samples (n = 50 to 131) have linked PAD to endothelial dysfunction. 20 Compared to individuals without atherosclerosis, PAD patients have been shown to have lower flow-mediated dilation of the brachial artery, indicating loss of nitric oxide activity.21–24 Attenuated flow-mediated dilation has also been associated with the severity of PAD measured by ankle–brachial index. 11 Functional status in PAD patients has been associated with measures of endothelial function. 25 Exercise interventions that have been shown to improve symptoms in PAD results in a concomitant augmentation of endothelial function. 12 Importantly, abnormal vascular function measured by flow-mediated dilation is associated with future cardiovascular events in PAD patients.7,9,10 Decreased nitric oxide bioactivity has the potential to contribute to the clinical expression of PAD by promoting plaque rupture, inflammation, and thrombosis. 20 Thus, vascular function has relevance to clinical status and outcomes in PAD.
In the present study, we extend these findings by demonstrating that vascular dysfunction is more severe in PAD patients compared with CAD patients in a much larger cohort enabling us to adjust for the confounding effects of risk factors. Despite a similar atherogenic process in both coronary and peripheral obstructive lesions, risk factors and clinical trajectories differ based on disease location.3,13–15 Patients with PAD have higher rates of adverse cardiovascular outcomes compared to CAD patients, yet the underlying mechanisms for such differences remain incompletely understood. 3 The present study indicates that PAD is associated with a greater degree of systemic vascular abnormalities. The association of lower flow-mediated dilation with PAD was not accounted for fully by differences in risk factor profiles or medication use. The greater extent of vascular dysfunction in PAD patients may reflect a higher burden of atherosclerotic disease. It is also possible that PAD has distinct vascular consequences reflected in reduced vasodilator function.
Reactive hyperemia is a pivotal vascular response that enhances blood flow after ischemia. Hyperemic blood flow depends on multiple substances including nitric oxide that produce microvascular dilation.26–28 Prior studies demonstrate an association of reactive hyperemia measured in the brachial artery with cardiovascular risk factors, inflammatory markers, and vascular stiffness.29–32 Hyperemic response provides incremental information regarding cardiovascular risk beyond flow-mediated dilation in patients with PAD. 8 In the present study, we show that reactive hyperemia is lower in PAD patients than in CAD patients, indicating that vascular dysfunction extends to the microvessels.
In addition to impaired flow-mediated dilation, PAD patients exhibited diminished response to nitroglycerin that was partially attributable to differences in risk factor profile. Prior studies have reported abnormal response to nitroprusside in atherosclerotic superficial femoral arteries in PAD patients and an association between impaired nitroglycerin response and higher cardiovascular risk in PAD patients.8,33 Attenuated nitroglycerin-mediated dilation may reflect dysfunction at the level of the vascular smooth muscle. Alternatively, nitric oxide activity may be reduced by increased inactivation by reactive oxygen species. Similar findings have been observed in patients with risk factors, including diabetes. 34
The association of PAD combined with CAD with reduced digital vasodilator responses was attenuated in adjusted analyses. These findings indicate that for digital vascular measures, but not brachial measures, the abnormalities observed in PAD patients may be attributable to differences in risk factor profiles. Both brachial flow-mediated dilation and PAT are non-invasive indicators of endothelial function.16,35,36 However, prior studies have had inconsistent results regarding the association of flow-mediated dilation with the PAT hyperemic response.18,37–39 The present study provides a potential basis for reconciling the conflicting reports. We observed a modest association between higher flow-mediated dilation and PAT hyperemic response in patients with established atherosclerosis but not in control individuals. However, we did not observe an association between the hyperemic response measured in the brachial artery and the PAT response, suggesting that the small vessels in the finger respond differently compared to the forearm microvasculature. Thus, in patients with clinical atherosclerotic disease there are parallel alterations in vasodilator function in the brachial and digital vessels.
Several limitations of our study are notable. The cross-sectional design of the study prevents conclusions about causality. The presence of PAD was determined by clinical diagnosis. It is likely that some patients classified as having CAD only, have peripheral atherosclerotic disease that has not yet manifest in clinical symptoms. 40 However, underdetection of PAD would be expected to diminish differences between the CAD and PAD group. In addition, it is possible that patients with asymptomatic PAD have different vascular function than patients with clinically evident PAD. Further, patients with PAD may have been at a more advanced disease state compared with CAD patients. Patients with atherosclerosis are taking multiple medications that may influence vascular responses. All vasoactive medications were withheld before testing and models that adjusted for medication use showed similar results. It is possible that participants in one of the included studies consumed food or smoked less than 8 hours before the vascular test. When we excluded these participants from the analysis, the results were similar. Measurements of nitroglycerin-mediated dilation and digital vascular function were available in a limited sample that may have influenced the detection of differences related to the presence of PAD. We elected to maximize the number of individuals studied by including all participants with available flow-mediated dilation.
In conclusion, our study demonstrated that patients with PAD have multiple defects in vasodilator function. Vascular dysfunction in PAD patients is more severe and extensive than in CAD patients. Our study supports the presence of a deleterious vascular phenotype that may contribute to heightened cardiovascular risk in PAD patients.
Footnotes
Conflict of interest
The authors declare no conflicts of interest in preparing this article.
Funding
This work was supported by grants from the National Institutes of Health (HL102299, HL109790, HL081587, HL075795). Drs Tabit and LeLeiko are supported by the Boston University Leadership Program in Vascular Medicine (K12 HL083781). Dr Gokce is supported by grants from the National Institutes for Health (HL081587 and HL084213).