
Abstract
Inferior vena cava (IVC) thrombosis remains under-recognised as it is often not pursued as a primary diagnosis. The aetiology of IVC thrombosis can be divided into congenital versus acquired, with all aetiological factors found among Virchow’s triad of stasis, injury and hypercoagulability. Signs and symptoms are related to aetiology and range from no symptoms to cardiovascular collapse. Painful lower limb swelling combined with lower back pain, pyrexia, dilatation of cutaneous abdominal wall veins and a concurrent rise in inflammatory markers are suggestive of IVC thrombosis. Following initial lower limb venous duplex, magnetic resonance imaging (MRI) is the optimal non-invasive imaging tool. Aetiology directs treatment, which ranges from anticoagulation and lower limb compression to open surgery, with endovascular therapies increasingly favoured. The objective of this review is to assess current literature on the aetiology, presentation, investigation, treatment, prognosis and other factors pertaining to IVC thrombosis.
Introduction
Inferior vena cava (IVC) thrombosis is related to the pathological and clinical spectrum of deep venous thrombosis (DVT). IVC thrombosis remains under-recognised, as it is not commonly pursued or identified. 1 Consequently, IVC thrombosis can present the clinician with a diagnostic and therapeutic challenge rarely discussed as a separate entity. Despite sparse Level I evidence, this review aims to heighten clinicians’ awareness of IVC thrombosis – summarising the epidemiology, aetiology, clinical presentation, investigation, treatment, prognosis and patient outcome in IVC thrombosis.
Methods
A comprehensive literature search was conducted using PubMed/MEDLINE/OVID and the Cochrane Database with the key words ‘inferior vena cava’, ‘thrombosis’, ‘epidemiology’, ‘pathology’, ‘presentation’, ‘diagnosis’, ‘investigation’, ‘treatment’, ‘surgery’, ‘prognosis’ and ‘outcome’. The search was limited to the English language and to papers published between 1950 and 2012.
Epidemiology
Lifetime incidence of DVT is 0.1% with a 4–15% incidence of IVC thrombosis in patients with a confirmed DVT.2,3 Stein et al. reported a 1.3% (99,000 of 7,902,000) rate of superior and inferior vena cava thrombosis in all hospitalised patients with venous thrombosis from their review of the US National Hospital Discharge Survey (NHDS) between 1979 and 2005. From 2000 to 2005, they identified an annual incidence of vena cava thrombosis of 5000 patients, which constituted 1.5% of all hospitalised venous thrombosis patients, where 78% had an isolated vena cava thrombosis presumed to affect the inferior rather than superior vena cava, while 22% had additional venous thrombotic sites. 4 Other researchers have reported vena cava thrombosis incidence rates between 1.4 and 1.8 per 100,000, with higher rates associated with increased age, while no significant difference was attributed between sexes (male 1.7 vs female 1.8 per 100,000) or ethnicity (white individuals 1.4 vs African American 1.7 per 100,000).3 –5 However, similar to DVT, the incidence was significantly lower in Asian Americans.3,4,6
Vena cava thrombosis is frequently associated with neoplastic disease. Stein et al. reported carcinomas in 37,000 of 99,000 (37.4%) patients diagnosed with a vena cava thrombosis. 4 Renal, tracheal and bronchopulmonary carcinomas were the most frequently observed. Carcinomas were diagnosed significantly less frequently (895,000 out of 7,825,000) in patients with identified isolated lower limb DVT compared with vena cava thrombosis patients (11.4% vs 37.4%, p = 0.0001). Despite the neoplastic association, vena cava thrombosis still remains rare and is identified in only 0.07% of hospitalised patients with neoplasms.
Aetiology
IVC thrombosis aetiology can be divided into congenital versus acquired. Most congenital IVC abnormalities remain asymptomatic owing to well-developed collaterals. Acquired thrombosis of the IVC can be caused by spontaneous thrombosis within a normal vessel wall, thrombosis secondary to external compression or thrombosis owing to pathological changes within the vein wall. 7 Aetiological overlap and synergy can exist between congenital and acquired pathologies and between different elements of Virchow’s triad.
Congenital IVC anomalies
Congenital IVC thrombosis aetiologies are more easily understood with an appreciation of the complex nature of the embryological development of the IVC. The infrahepatic IVC develops between the sixth and eighth weeks of embryonic life as a composite structure formed from three paired embryonic veins: the posterior cardinal, the subcardinal, and the supracardinal veins (Figure 1). 8
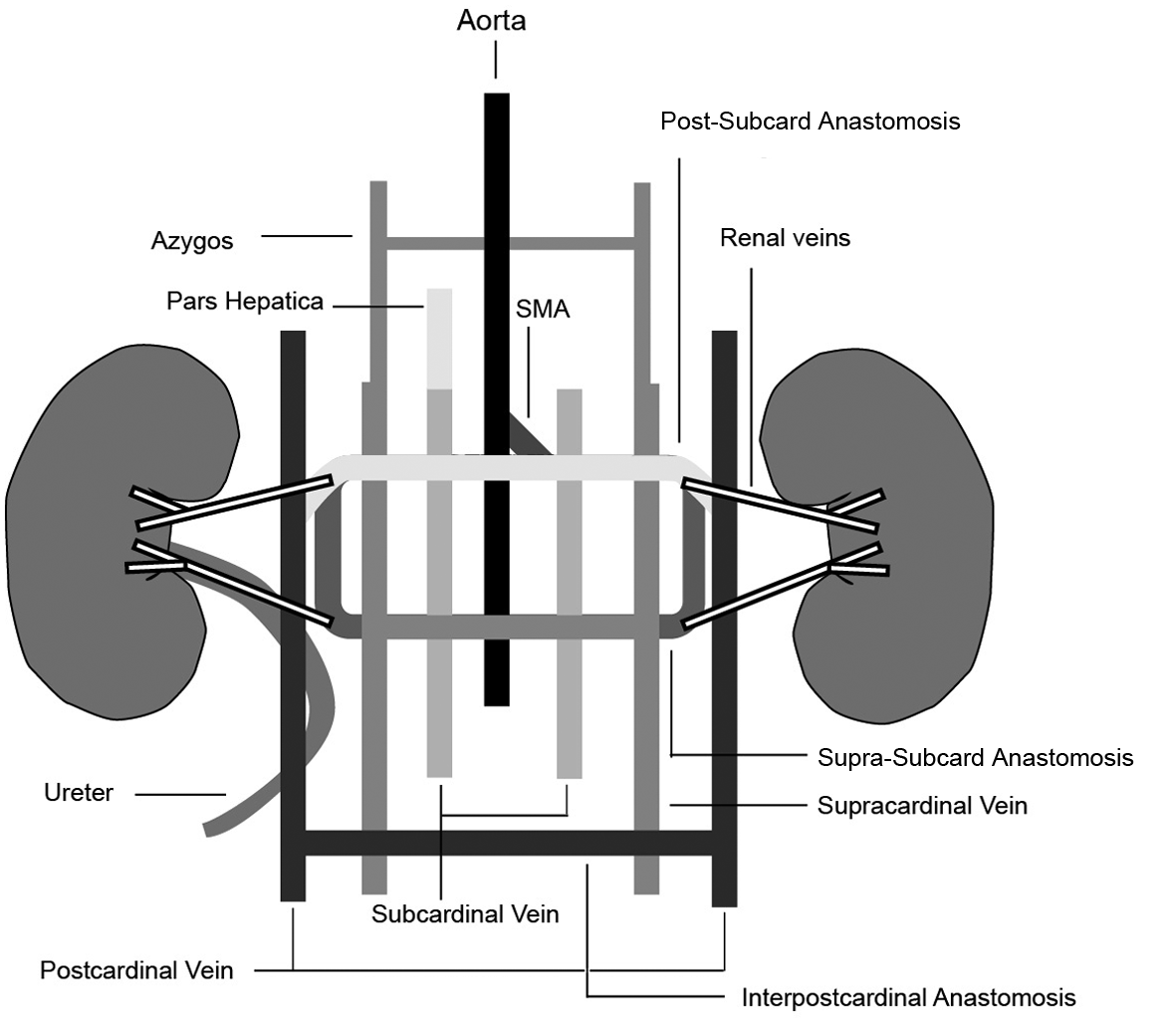
Conceptual framework showing the relative positions and interrelationships of the three paired embryonic vessels that contribute to development of the IVC (the pictured veins are not all present simultaneously). Under ordinary circumstances, the prerenal division is formed from union of the hepatic segment (pars hepatica – a vitelline vein derivative) and the right subcardinal vein. The renal segment is formed from the suprasubcardinal anastomosis and the post-subcardinal anastomosis. The infrarenal segment is derived from the right supracardinal vein. The iliac veins form from the posterior cardinal veins. 8 (SMA, superior mesenteric artery.) Reproduced from ref. 8 with permission from the Radiological Society of North America.
Although congenital anomalies of the IVC are infrequent, they are probably more common than current estimates owing to a predominantly subclinical presentation. Prevalence rates are between 0.3% and 0.6% in the general population. 9 This increases to 2.0% in those with other congenital cardiovascular defects such as dextrocardia, transposition of the great vessels, pulmonary artery stenosis or a single atrium. 10 IVC anomalies are most commonly identified in young males, invariably remaining subclinical for many years, usually presenting in the third or fourth decade. DVT or chronic venous insufficiency (CVI) are often the first indicators of a congenital IVC anomaly. 11
Congenital IVC anomalies can be divided into three anatomical types:8,12
infrarenal: left-sided IVC (prevalence 0.2–0.5%), a double (right and left) IVC (prevalence 0.2–3%), a double right IVC or absence of the infrarenal IVC.
renal: retroaortic left renal vein (prevalence 1.7–3.4%) and circumaortic venous ring (prevalence 2.4–8.7%).
suprarenal: an azygos continuation of the inferior vena cava (also termed absent hepatic segment of IVC with azygos continuation) (prevalence 0.6%) (Figures 2 and 3) 13 and left-sided IVC with hemi-azygos continuation and congenital membranes.
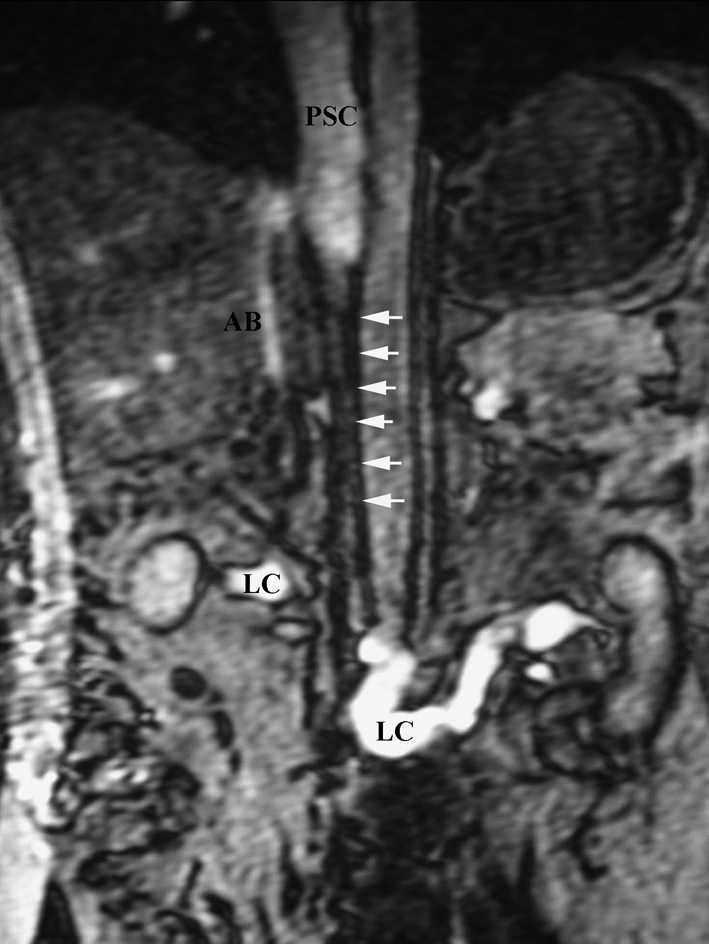
Coronal gradient echo MRI showing atresia of IVC between renal and hepatic segments (sequential white arrows) with a patent hepatic and suprahepatic IVC (PSC). Extensive well developed collateralisation is identified through ascending lumbar veins (LC), azygous branches and collaterals (AB) and anterior abdominal wall subcutaneous veins. Reproduced from ref. 13 with permission from The Ulster Medical Journal.
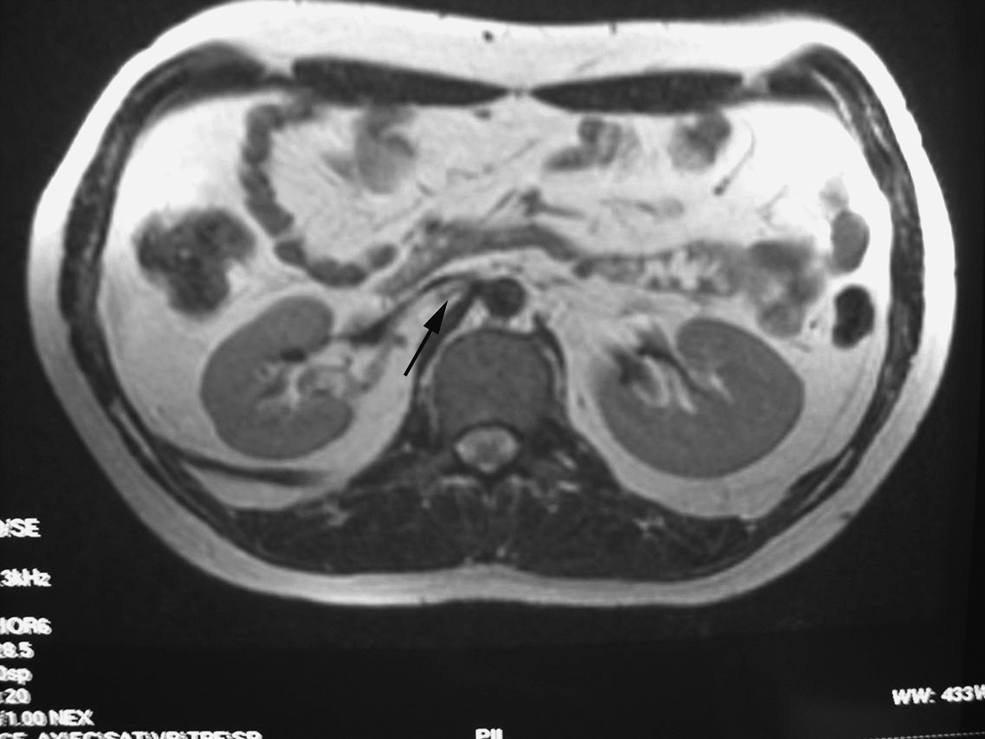
T2-weighted axial MRI showing stenosis of IVC at renal level (black arrow). Reproduced from ref. 13 with permission from The Ulster Medical Journal.
IVC aneurysms are thought to be congenital, developing at anastomoses of the embryological venous systems.14,15 More commonly saccular, often associated with other congenital cardiovascular abnormalities, they may remain subclinical or present with pain, rupture, DVT (usually bilateral) or IVC thrombosis. 15
These anomalies cause IVC thrombosis via volume restriction of channels returning blood to the heart, which despite prominent collaterals, cause venous hypertension, stasis and subsequent venous thrombosis.16,17 Bilateral ilio-femoral DVT is reported in over 60% of patients with IVC anomalies and when bilateral ilio-femoral DVT is present, the IVC is normal in only 10% of patients.16 –18 IVC anomalies are associated with thrombophilic disorders.17,19 As Gayer et al. reported a high prevalence of thrombophilia in their series of congenital IVC anomalies, they suggested an interaction between stasis and hypercoagulability in the pathogenesis of DVT/IVC thrombosis in patients with IVC anomalies. 17 Hereditary thrombophilias (activated protein-C resistance, protein-C and S deficiencies, antithrombin deficiency, prothrombin gene mutation and dysfibrinogenaemia) increase the risk of venous thromboembolism. 19 Current evidence suggests a thrombophilia screen is prudent in patients with IVC anomalies associated with IVC thrombosis.17,20 –23
Acquired IVC thrombosis
Acquired IVC thrombosis is caused by spontaneous thrombosis in an otherwise normal vessel, thrombosis secondary to external compression or thrombosis consequent upon pathological changes in the vessel wall. 7
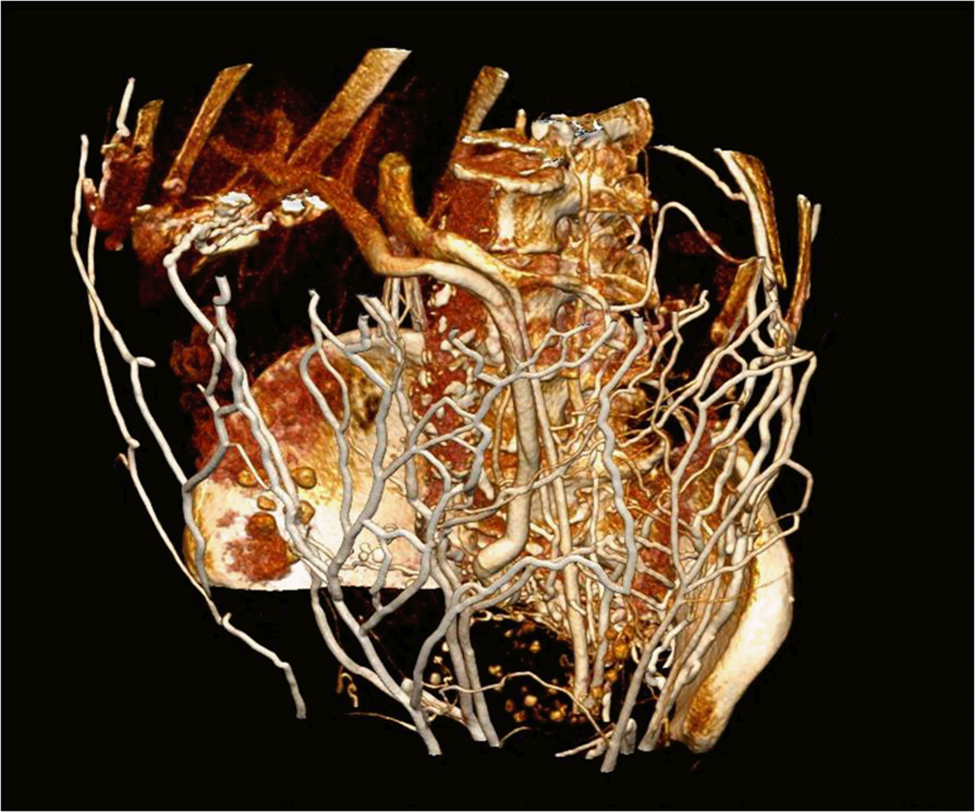
Spontaneous IVC thrombosis is associated with malignancy where the prothrombotic potential of the tumour state may combine with the consequent chemotherapy or radiotherapy treatment to enhance the risk of IVC thrombosis (Figure 4). A primary IVC tumour and secondary malignancies such as renal cell carcinomas may also infiltrate or adhere to the IVC wall, leading to endothelial damage and subsequent thrombosis.7,12,24,25 Intravascular tumour/thrombus invasion may extend intraluminally along the renal vein into the IVC and can propagate as far as the heart, resulting in an occluding thrombosis or tumour emboli (Figure 5). 3

Contrast-enhanced computed tomography (CT) scan of the abdomen demonstrating thrombus (white arrow) in a young male patient with a history of testicular malignancy.
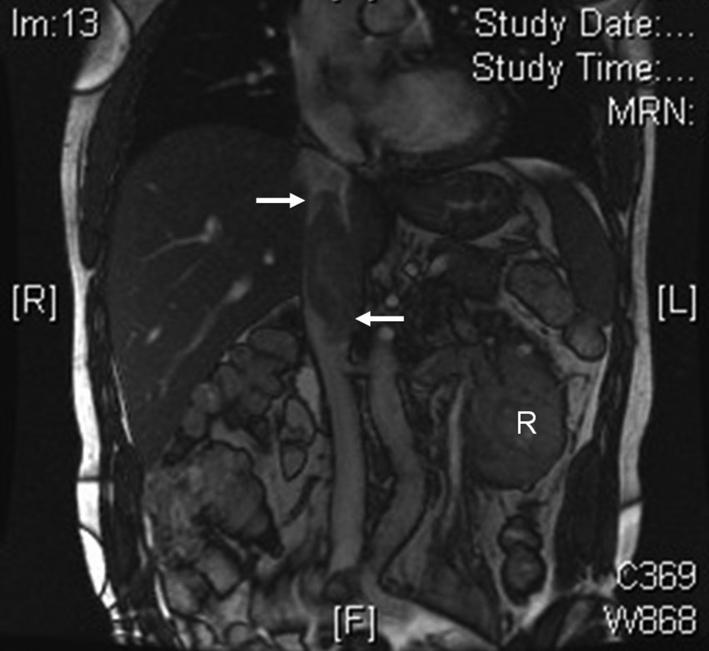
Coronal MRI of the abdomen, using 2-D fast imaging employing steady-state acquisition sequence (FIESTA), demonstrating thrombus within the IVC extending from the left renal vein to near the right atrium (white arrows) secondary to a left renal cell carcinoma (white ‘R’).
Following interventional procedures, IVC thrombosis may result from extension of ilio-femoral DVT into the vena cava either in isolation or in association with DVT elsewhere. 7 IVC thrombosis secondary to endovenous intervention may result from direct IVC/iliac vein injury, pressure effects from an iatrogenic retroperitoneal haematoma or owing to propagation of a pre-existing ilio-femoral or distal DVT.26 –28 Laparoscopic surgery may cause IVC thrombosis via similar mechanisms. 5 Hepatic transplantation can cause IVC thrombosis via direct IVC instrumentation, iatrogenic haematoma and formation of retro-hepatic IVC stenoses. 29
Placement of foreign bodies such as IVC filters (Figures 6 and 7) or venous catheters may promote thrombus formation.30 –32 Occlusion of IVC filters remains their most frequent complication, with IVC thrombosis reported in 2.7% of patients owing to new local thrombus formation/thrombogenicity of the device, trapped embolus from a more distant site, or cephalad extension of distal DVT.31 –33 Current underestimation of IVC thrombosis following filter insertion is suggested by the PREPIC study, which quotes rates from 13% at 8 years’ follow-up, with 30% demonstrated in longer-term studies.34 –38

Coronal computed tomography (CT) scan showing IVC thrombosis (white arrow) distal to an IVC filter (black arrow).
Re-formatted computed tomography (CT) images of the patient in Figure 6 displaying a large number of sizable superficial venous collaterals.
IVC thrombosis secondary to abdominal trauma may result from endothelial injury secondary to compression or shearing forces, direct IVC vessel wall damage because of blunt or penetrating injury, indirect trauma leading to vessel bruising and tearing from spinal fractures or from extrinsic compression from adjacent haematoma formation.7,39 –42 Minor trauma or apparently innocuous injuries acquired during the changing of a car tyre, tumbling exercises and even lengthy bicycle rides can trigger IVC thrombosis.43 –45
Compressive distortions of the IVC generate both turbulent flow and venous stasis, thereby facilitating the formation of thrombus. 7 Such secondary IVC thrombosis can be caused by lymphadenopathy, retroperitoneal fibrosis, aortic aneurysms, large abdominal malignant tumours and ascites.
Other acquired predispositions to DVT and hence IVC thrombosis include acquired thrombophilias (antiphospholipid antibody syndrome), as well as environmental factors (combined oral contraceptive pill, hormone replacement therapy, pregnancy, obesity, malignancy and chronic inflammatory conditions).20,46 Inflammatory bowel disease, nephrotic syndrome and sepsis predispose to venous thromboses owing to associated risks of severe dehydration, protein/anticoagulant loss and elevated inflammatory response.47 –50
A further variant of primary IVC thrombosis, occasionally termed obliterative or membranous hepatocavopathy, most commonly occurs in the hepatic portion (as the name suggests), and is characterised by a thrombus organising into a fibrous, membranous obstruction of the IVC. The cause of such primary IVC thrombosis is often idiopathic. Although this version of primary IVC thrombosis is rare in Western countries, it is endemic in Nepal where considerable evidence now suggests an acquired infective aetiology which results in thrombophlebitis leading to thrombus formation and a subsequent fibrotic stenosis. 51 Causative infective organisms include Staphalococcus aureus and gram-negative enteric organisms where the resultant bacteraemia causes a transient protein-S deficiency. 51 Other causes of IVC thrombosis include May–Thurner syndrome, which causes ilio-femoral thrombosis because of an intraluminal web or stenosis of the left common iliac vein, likely due to the direct mechanical impingement of the right common iliac artery on the left common iliac vein. 52 Although Budd–Chiari syndrome (primary hepatic vein thrombosis) is a hypertensive syndrome of the hepatic veins, it has features in common with IVC thrombosis owing to altered haemodynamics of the hepatic veins, IVC and portal vein. 53
Clinical presentation
Clinical presentation of IVC thrombosis varies from an incidental radiological finding in an asymptomatic patient through to severe haemodynamic compromise and cardiovascular collapse. Rapid onset of symptoms suggests acute IVC thrombosis while gradual symptomatic deterioration may be related to an increasing compression of the IVC or thrombotic IVC occlusion with associated venous collateralisation and peripheral chronic venous insufficiency. 7
Acute IVC thrombosis
An acute IVC thrombosis may appear spontaneously as a result of an identifiable risk factor such as a chronic debilitating illness, or as a consequence of pre-existing chronic IVC obstruction. 7 Patients often complain of low back and/or buttock pain. Sciatica-type pain and cauda equina symptoms have been described secondary to IVC thrombosis. 54 Renal vein involvement may result in loin pain and haematuria, while bilateral renal vein thrombosis can lead to oliguria, anuria and uraemic symptomatology. Anterior abdominal pain or tenderness is uncommon. Chest pain and shortness of breath may be indicative of pulmonary embolism (PE), which is reported in 12% of patients with isolated IVC thrombosis. 55
Clinical presentation of IVC thrombosis may vary according to the level of thrombosis (from the iliac confluence to the right atrium) and degree of occlusion of the cava. 56 Classically, patients present with bilateral lower extremity swelling and dilatation of superficial abdominal vessels. In reality, this only occurs in around half of patients presenting with symptomatic IVC thrombosis. If the thrombus is confined to the IVC and does not involve the iliac or femoral system, collateral pathways form along the posterior abdominal wall. If these more distal systems are involved dilated veins can appear on the abdominal wall between the groins and the axillae within days of thrombosis. Abdominal swelling can result from ascites or secondary to an intra-abdominal abnormality causing the IVC compression. Non-tender, pitting oedema associated with blue discoloration can occur in the lower limbs within 6–12 hours if the thrombus occludes the IVC. If IVC thrombosis extends to the pelvic and femoral veins there is an increased risk of phlegmasia cerulae dolens (PCD) and hence venous gangrene. 7 Pyrexia can be present, as described by Tsuji et al., who reported a series of 10 patients where 40% were pyrexic at presentation. 57
Chronic IVC thrombosis
Symptoms and signs of a slowly progressive thrombosis are similar to those of an acute thrombosis but with a different time course. 58 There may be a history of serious illness, trauma or surgery, even years earlier. This may have been asymptomatic or have caused a degree of leg swelling at the time, which regressed rapidly and spontaneously. IVC thrombosis may be uncovered coincidentally during a routine examination when collateral veins are noted on the abdominal wall, or identified following cross-sectional radiological imaging. 7
Chronic IVC thrombosis can cause a dull aching pain in both lower limbs as well as symptoms of venous claudication, where lower limb swelling and discomfort is precipitated by exercise and relieved by rest and elevation. The majority of patients with congenital IVC anomalies have few symptoms or clinical signs because venous compensation takes place through well-developed collaterals, masking the clinical presentation. 7 Symptoms may later ensue owing to gradual decompensation or further thrombosis, often between the age of 20 and 30 years.
IVC interruption or IVC stenosis is commonly asymptomatic if it is associated with the presence of a well-developed azygos/hemiazygos continuation. However, absence of the azygos/hemiazygos leads to significant symptoms. 59 Patients with absent segments of IVC may present with symptoms of lower extremity venous insufficiency or DVT. 8 Other IVC anomalies may cause different clinical findings depending on the variant drainage patterns or collaterals. Lower limb swelling predominates in these patients, combined with lower limb and abdominal wall varicosities in the superficial inferior epigastric and superficial external iliac distribution. Swelling often becomes gross and may extend into the buttocks and lower abdominal wall. Normal caudal direction of blood flow to the sapheno-femoral junction is reversed in these veins, while Harvey’s test elicits cranial to superior vena cava flow in abdominal wall varices. Post-thrombotic syndrome (PTS) with skin pigmentation, eczema, lipodermatosclerosis and ulceration is associated with the chronicity of IVC thrombosis. General examination may also reveal evidence of the underlying cause of an IVC compression causing IVC thrombosis such as an abdominal mass or generalised lymph node enlargement. 7
Investigations
Haematological
Tsuji et al. reported a series of 10 patients with IVC thrombosis who had elevated d-dimer levels and inflammatory markers at presentation (white cell count (WCC) and C-reactive protein (CRP)). 57 A raised erythrocyte sedimentation rate (ESR) may also suggest a systemic pathology or retroperitoneal fibrosis whilst abnormalities in haemoglobin concentration (Hb) and WCC can be related to an underlying systemic disease or infection. Biochemical renal dysfunction may suggest ureteric obstruction secondary to retroperitoneal fibrosis or renal vein thrombosis. 57 Though largely directed from Level IV evidence, it would appear prudent to perform a thrombophilia screen, especially in young patients without other risk factors. This should include: protein C, antithrombin, free protein S, activated protein-C resistance, IgG anticardiolipins, lupus anticoagulant and homocysteine levels as well as a PT (20210) FII gene mutation screen. 17 A thrombophilia screen should be acquired prior to heparinisation, though should not delay the latter.
Radiological
Recent advances in the utilisation of the ultrasound scan (USS), computed tomography (CT) and magnetic resonance imaging (MRI), as well as endovascular procedures, have resulted in an increase in the detection rates of both IVC anomalies and venous thrombosis. 57
Duplex USS provides an accurate non-invasive method of diagnosing IVC thrombosis and is often the first-line investigative modality. 1 Normality includes a continuous waveform with respiratory variations which become more pulsatile as the IVC empties into the right atrium. Thrombosis can cause the IVC waveform to appear monophasic, with high velocities giving it a ‘choppy’ appearance. 60 However, duplex USS is operator-dependent and can be limited by body habitus and the presence of bowel gas, and may occasionally fail to identify any IVC anomaly.1,61 Duplex USS also has diminished diagnostic reliability within the abdomen owing to difficulty in assessing venous compressibility combined with loss of respiratory phasicity above the renal veins because of retrograde transmission of the cardiac cycle through the valveless IVC. 61 USS may identify aetiologies causing extrinsic compression of the IVC or IVC anomalies.
Contrast venography remains the historical standard for the diagnosis of IVC thrombosis, with a low false-positive rate and with the advantage of access for immediate intervention and treatment. Local thrombolysis, IVC filters, angioplasty and stenting can be performed concurrently. 1 However, it is invasive, occasionally requiring proximal supraclavicular access in addition to distal femoral, to delineate cranial and caudal thrombus limits and is itself associated with a 2–10% incidence of post-procedural DVT. 1 It is limited to endoluminal imaging.
Computerised tomography imaging is rapid, non-invasive and can accurately diagnose and assess the extent of thrombus and the presence of associated abdominal or pelvic abnormalities. 1 The most common true filling defect of the IVC is bland thrombus, which may be idiopathic or reflect a hypercoagulable state, venous stasis, or the presence of a foreign body. 24 Benign distal ‘bland’ thrombus may coexist with upstream malignant thrombus more superiorly in the IVC. Malignant thrombus can be differentiated from bland thrombus on CT through the presence of a contiguous adjacent mass and enhancement of a filling defect. 12 Should an adjacent tumour not be identified, an enhancing mass may be the result of primary intraluminal sarcoma. It should be noted that pseudothrombosis of the infrarenal vena cava is a frequent finding during post-contrast helical CT studies of the abdomen. Pseudothrombosis, particularly of the infrarenal IVC, is generally thought to result from the variable amounts of contrast in the cava above and below the renal veins compounded by collapse of the diaphragmatic IVC while patients lie supine for the investigation. 62
Magnetic resonance imaging is replacing CT as the optimal non-invasive imaging tool. 63 MRI avoids radiation and provides more accurate delineation of thrombus, including proximal and distal extent and its age, as well as any IVC anomaly. 63 It is used to follow up patients to determine morphological thrombus changes after therapy. Disadvantages include cost and accessibility, and there remains a risk of nephrogenic systemic fibrosis if gadolinium-based contrast agents are administered in patients with renal dysfunction.25,62 Theoretically, IVC filter migration could also result from MRI but this has not been reported. Nevertheless, MRI should not be performed if there is any possibility that the IVC filter is not positioned correctly or is not firmly in place. 64
Treatment
IVC thrombosis treatment is determined by aetiology, timescale (acute vs chronic) and patient-specific factors. Similar to other types of venous thromboembolus (VTE), immediate treatment strategies for IVC thrombosis revolve around minimising the risk of pulmonary embolisation and reducing the local sequelae of lower limb swelling and pain.7,65 Medical, endovascular and surgical options are available. Long-term goals are to prevent symptoms and signs of CVI and minimise or prevent PTS. 65
The 2012 guidelines for antithrombotic therapy of VTE from the American College of Chest Physicians (ACCP) recommend, for patients with acute DVT, low-molecular weight heparin (LMWH) or fondaparinux over intravenous unfractionated heparin (IV UFH) (Grade 2C evidence) and over subcutaneous UFH (SC UFH) (Grade 2B evidence for LMWH; Grade 2C for fondaparinux). These recommendations, though largely based on lower limb DVT, include the treatment of IVC thrombosis. In patients with acute DVT of the leg treated with LMWH, the ACCP suggest once- over twice-daily administration (where total dose is the same in 24 hours) (Grade 2C). 66
Anticoagulant therapy reduces thrombus propagation, but does not produce clot lysis, thus risking PTS, which occurs after proximal DVT in up to 50% of patients within 2 years.67,68 Rapid thrombus removal is felt by many to be essential to preserve valvular function, thereby minimising CVI and PTS.33,65 However, it is necessary to determine whether IVC thrombosis is spontaneous (idiopathic) or secondary, as removal of thrombus will not result in long-lasting patency if the cause (e.g. external compression) has not been corrected. Elastic compression stockings are also used to minimise long-term PTS. Although the timing of initiating compression remains varied, Arpaia et al. reported that elastic compression applied immediately at diagnosis of DVT was safe, with a significantly higher re-canalisation rate in venous segments and popliteal veins in the early compression group compared to application at day 14. 69 The ACCP recommend the use of compression stockings for 2 years (Grade 2B) in patients with acute symptomatic DVT to prevent PTS. 66
Acute IVC thrombosis treatment
In acute idiopathic IVC thrombosis, where no abnormality is detected other than caval thrombosis, treatment options are threefold: remove thrombus through pharmacological, endovascular or surgical modalities; reduce the risk of thrombus propagation with anticoagulation; and confine thrombus to the IVC to reduce the risk of PE. Thrombus removal is preferred by many in the management of IVC thrombosis as it is thought likely to minimise the long-term complications of CVI and PTS. Where acute thrombosis is a secondary event, treatment depends on whether the causative pathology can be resolved. Many compressive pathologies precipitating IVC thrombosis are unsuitable for intervention. Thrombus in a compressed or infiltrated IVC is usually adherent and without a propagating tail. In such cases where there is no contraindication, anticoagulation to minimise thrombus propagation combined with a proximal filter to minimise embolisation risk are the mainstays of treatment. Where the primary aetiology is reversible, a combination of these treatment options is employed to address cause while treating the acute IVC thrombosis. 7
Unfractionated or LMWHs are commonly used to reduce the risk of embolisation and propagation of thrombus from the time of diagnosis. 70 However, they do not lead to a rapid resolution of IVC thrombosis, thought likely to preserve distal venous valvular function, and reduce the long-term risk of CVI and PTS. Only 6% of patients treated with anticoagulation alone achieve clot lysis within 10 days of treatment and thrombus propagation is identified in up to 40% of patients despite adequate treatment. 65
Systemic thrombolysis with urokinase, streptokinase or tissue plasminogen activator is more effective than heparinisation for IVC thrombosis. However, thrombolysis does not always lead to rapid resolution of clot and carries an increased risk of haemorrhage.65,71 Thery et al. prospectively assessed 174 patients with extensive proximal DVT and reported complete lysis with systemic thrombolyis in 60% of patients with non-occlusive thrombus versus 14% amongst those with occlusion. 72 Systemic thrombolysis is likely suboptimal treatment for occlusive IVC thrombosis, where treatment merits should be balanced against the risks of haemorrhagic or cardiovascular complications. A recent Cochrane review by Watson and Armon concluded that thrombolysis (including systemic and local) is advantageous over anticoagulation alone in the treatment of DVT. However, the optimum drug, dose and route of administration has yet to be determined. 73
Endovascular modalities facilitate local delivery of therapeutic agents including thrombolytics, thereby minimising systemic effects, and permitting angioplasty, stent insertion and deployment of proximal filters.65,71 Although timing is debated, the majority of reports suggest that thrombolytic therapy, delivered locally using catheter-directed thrombolysis (CDT; with or without a pulse-spray and/or a pharmacomechanical adjunct), should be administered as soon as possible after the patient becomes symptomatic and ideally within 14 days of onset of symptoms.65,71 Successful treatment has also been reported up to 30 days after onset of symptoms. CDT appears valuable in the early treatment of venous thromboses where preservation of distal venous valvular function leads to significant reduction in both CVI and PTS.74,75 Alesh et al. reported 28% recanalisation and 56% PTS for occluded veins following systemic thrombolysis compared to 90% and 26%, respectively, with CDT. 76 The Trellis-8® (Covidien plc, Dublin 2, Ireland) pharmacomechanical thrombectomy catheter deploys thrombolytic agent between two balloons allowing localisation of treatment, limiting systemic effects. 77 Other modalities include pulse-spray pharmacomechanical thrombolysis (PSPT), which consists of brief high-pressure pulsed injections of a concentrated fibrinolytic agent throughout the clot via a multi-side-hole catheter. In addition to CDT, PSPT leads to clot maceration and an increased thrombus contact area for thrombolytic activity via numerous penetrating intra-thrombus injections. PSPT minimises systemic thrombolytic concentration owing to an enhanced local lytic effect combined with a reduced dilutional tendency through direct intra-thrombus activity. 65 Dose reductions in urokinase therapy from 7.8 million IU, with an 11% major bleeding complication rate, to 1.71 million IU have been reported with PSPT, where the reduced dose was sufficient to lyse thrombus and recanalise occluded vein with virtually no bleeding complications. 65 Although, PSPT appears superior to conventional CDT in fragmenting and lysing clot, randomised controlled trials are still required.
The use of IVC filters, to minimise the risk of PE in IVC thrombosis, in combination with local thrombolytic procedures, remains a subject for debate. Yamada et al. and Protack et al. reported that CDT without universal filter placement was safe except for patients with poor cardiovascular reserve or those with large, free-floating IVC thrombosis.65,78 In contrast, Kolbel et al. retrospectively reviewed 40 venograms in patients with IVC filters treated with CDT for ilio-caval thrombosis and reported that embolisation to the filter was visible in 45% of patients. 79 They concluded that placement of a retrievable IVC filter during CDT can prevent both silent and symptomatic PE. However, the British Committee for Standards in Haematology state that vena cava filters have not been shown to reduce the incidence of fatal PE during thrombolysis (systemic or catheter-directed) and hence are not mandatory with such thrombolysis. 64 When deployed these filters should ideally be retrievable. Yamada et al. have reported a higher frequency of non-permanent IVC filter insertion following PSPT because of a perceived higher risk of emboli caused by fragmentation of thrombus when compared to CDT. 65 Insertion of IVC filters may also precipitate venous thrombosis, with IVC thrombosis a recognised late complication of IVC filters, occurring in up to 30% of cases (Figures 6 and 7).33,35 The British Committee for Standards in Haematology recommends that patients with permanent caval filters should receive routine follow-up for complications associated with caval filters or VTE. Most manufacturers recommend that retrievable filters should be removed within 10–14 days of implantation, although some have been successfully removed more than 1 month after placement. 80 The US Food and Drug Administration (FDA) recommends that implanting physicians and clinicians responsible for the ongoing care of patients with retrievable IVC filters should consider removing the filter as soon as protection from PE is no longer needed and consider the risks and benefits of filter removal for each patient. 81
Angioplasty and stenting may be used to complement thrombolysis where improvements in medium- to long-term patency rates combined with minimal additional procedural co-morbidity have been reported in patients with residual stenosis and ilio-caval obstructive lesions.65,79,82,83 Patients unfit for major intervention or with contraindications to thrombolysis should be considered for caval blockade with permanent IVC filter to minimise risk of embolisation. 7
Surgical interventions including thrombectomy, bypass, reconstruction/replacement and interruption/ligation are used infrequently owing to inherent morbidity and mortality.84 –86 Thrombectomy may be indicated for acute or septic IVC thrombosis and PCD but these procedures are less commonly performed because of high rates of re-thrombosis. 7 Such procedures are typically completed in conjunction with a distal arteriovenous (AV) fistula to maintain high flow. Neglen et al. demonstrated a successful thrombectomy combined with construction of an AV fistula and anticoagulation in 27 out of 52 patients diagnosed with ilio-femoral thromboses extending into the IVC. None of these patients developed features of PTS on long-term follow-up, whereas 20% of non-thrombectomised patients developed ulceration. Successful thrombectomy, with low morbidity and mortality, was achieved in patients with recent onset symptoms and associated fresh thrombus. 86 Others report operative mortality rates of 2% with morbidity rates of 30%.82,84 Thrombectomy combined with stenting, ligation or external clipping of the IVC have also been performed with varied success rates.82,84
Chronic IVC thrombosis and IVC stenosis/occlusion treatment
Chronic obstructive venous lesions can be divided into two categories: non-thrombotic venous lesions (e.g. external compression) and post-thrombotic lesions. 7 Until the mid-1990s chronic venous thromboses/obstructive lesions were treated medically with anticoagulation and compression hosiery, or treated surgically. 82 Endovenous angioplasty combined with stenting has emerged as the method of choice for the treatment of isolated caval and ilio-caval obstructive lesions.82,87,88 Results of angioplasty alone are disappointing in chronic venous stenoses owing to venous recoil, low flow state and re-thrombosis. 89 Stent insertion can improve the outcome of endoluminal interventions by preventing recoil therefore maintaining a large venous conduit to promote patency. 90 In patients with an unresectable underlying malignancy, treatments are commonly palliative. However, endoluminal treatment can relieve profound IVC obstructive/thrombotic symptoms, avoiding distressing and debilitating lower limb symptoms. In such patients, endovascular intervention should be considered urgent first-line treatment. 90
Benign causes of chronic IVC thrombosis with stenosis/occlusion pose a different clinical challenge, as maintenance of IVC patency and relief of symptoms are required long term. Razavi et al. reported a series of 17 patients with long-term IVC occlusions, suggesting promising medium-term results with angioplasty and stenting. 90 Riele et al. also reported that angioplasty and stenting is potentially efficacious in patients with long-segment (> 5 cm) as well as shorter IVC occlusions. 89 Currently, endovascular stent placement in combination with angioplasty is recognised as the treatment of choice for chronic ilio-caval/IVC stenotic and occlusive lesions. 91
IVC bypass surgery has a high failure rate. 7 Graft material for large vein reconstruction continues to be problematic. External compression of graft and length limitations, restrict use of spiral vein grafts for ilio-caval and femoro-caval applications. Expanded polytetrafluoroethylene (PTFE) is the current optimal prosthetic material. 90 However, Gloviczki et al. reported low short-medium term patency rates of 64% (n = 7/11) at 9 months in patients with abdominal or pelvic PTFE bypass grafts. 85 Jost et al. reported similar findings and also suggests the use of an arteriovenous fistula to improve patency may not be appropriate. 84 Donor homografts may provide a potential source of bypass conduit, but as yet are unassessed.
Aggressive surgical management with reconstruction or replacement of the affected segment may offer the only chance for cure or palliation of symptoms for patients with primary or secondary IVC tumours, the majority of whom will become symptomatic from subsequent IVC thrombosis. Bower et al. performed successful vena cava replacement in 29 patients with low graft-related morbidity and good patency, in carefully selected patients. 92
Thrombosis treatment in congenital IVC anomaly
Anticoagulation therapy and compression hosiery are likely to ameliorate symptoms in patients with congenital IVC anomalies and symptomatic IVC thrombosis. Treatment duration is widely debated. As caval anomalies remain permanent risk factors for venous stasis and thrombosis, life-long anticoagulation appears acceptable; however, there are no explicit guidelines.18,93 Endovascular intervention including thrombolysis may be considered in severe venous claudication, while stent insertion can be used to treat congenital occlusions dependent upon anatomical variance.89,93 Broholm et al. report promising results from CDT in 11 patients with segmental IVC agenesis presenting with ilio-femoral DVT/IVC thrombosis at a median follow-up of 37 months. 94 Surgical bypass with interposition PTFE graft has also been performed, though experience is minimal.95,96
Continuing medical treatment in IVC thrombosis
Whether or not patients have endovascular or surgical intervention, unfractionated or LMWH treatments, where not contraindicated, are the mainstays of treatment to minimise the risks of thrombus propagation, PE and recurrent thrombosis following IVC thrombosis. They can be used concurrently with other acute interventional treatments with conversion after a minimum of 5 days’ treatment to oral therapies such as warfarin, which should be initiated early with treatment overlap as per ACCP guidelines.66,70 Length of treatment with warfarin is dependent upon aetiology and patient-specific factors. There is no specific literature describing the ideal duration of anticoagulation for the differing pathologies causing IVC thrombosis. However, current ACCP guidelines indicate that where a secondary cause is reversed without concurrent thrombophilia, oral anticoagulation should be maintained for 3 months. 66 Where there is co-existent or causative thrombophilia, the cause is non-reversible, such as an IVC anomaly, or if the treatment involves an IVC stent, patients are likely to benefit from life-long oral anticoagulation. Newer oral anticoagulants such as rivaroxaban or dabigatran are not recommended as first-line, long-term anticoagulation in the 2012 ACCP guidelines and are currently third line after warfarin and LMWH. 66
Prognosis and outcome
The prognosis for patients with IVC thrombosis is determined by aetiology, whether and when a diagnosis is made, the cranial and caudal extent of thrombus, whether thrombus causes stenosis or occlusion, and the success of treatment.
The immediate risk from IVC thrombosis is PE, which occurs in over 30% of cases. 4 Significant long-term complications of IVC thrombosis are CVI and PTS, occurring in up to 20% of non-resolved IVC thrombosis. Over 50% of patients with a DVT may develop PTS, with 6% progressing to venous ulceration despite compression. In rare cases, limb-threatening venous gangrene may result. 68
Conclusion
IVC thrombosis is associated with significant acute and chronic morbidity. It presents a diagnostic challenge to the clinician and requires a high index of suspicion. Pain and swelling of lower limbs, lower back pain, dilatation of superficial abdominal veins and a concurrent rise in inflammatory markers and pyrexia are diagnostic indicators. Further investigational modalities are mandatory following ultrasound identification of ilio-femoral thrombosis, especially if bilateral. Where IVC thrombosis is idiopathic, especially in younger patients, a complete thrombophilia screen should precede but not delay heparinisation. CT and more so MRI are increasingly adept at delineation of IVC anatomy and assessment of thrombus extent, with the advantage of highlighting many causes of secondary IVC thrombosis. In appropriate cases, locally directed thrombolysis is the most efficacious treatment, minimising long-term complications of IVC thrombosis.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors report no conflicts of interest.