
Abstract
Assessment of collateral circulation to the hand is required prior to invasive procedures or harvesting of the radial artery (RA). A modified Allen’s test (MAT) is commonly used to assess palmar arch collaterals. A variety of non-invasive methods including digital pressures, plethysmography, pulse oximetry and duplex ultrasonography are available to supplement physical examination. However, no consensus exists about the proper role of the MAT and the most appropriate non-invasive test (NIT) in this situation. Interpretation of the MAT and NIT findings are also controversial. This paper reviews the anatomy and the physiologic basis for the MAT and various NITs, the pros and cons of various NITs and recommendations for the assessment of collateral circulation to the hand prior to interventions directed at the RA.
Introduction
The radial artery has become the third most frequent conduit for use in coronary artery bypass graft (CABG) operations owing to modification of harvesting techniques leading to good, long-term results. 1 Although the incidence of clinically significant hand ischemia following radial artery harvest is uncommon, the consequences can be disastrous.2,3
In addition to radial artery harvesting, prolonged cannulation of the radial artery and resulting thrombosis also creates some risk of hand ischemia. Although radial artery access for catheterization of the coronary arteries accounts for < 2% of all catheterizations in the US, the frequency is on the rise because of reduced morbidity and quicker return to normal activities. 4 One of the complications of radial artery access is hand ischemia. In a review of complications following radial artery catheterization, permanent hand ischemic damage was reported in 0.09%. 5 Some studies have reported a 25–33% incidence of flow reduction or thrombosis after radial artery cannulation and, although any hand ischemia after radial artery cannulation is 1 in 500 in another series, the consequences of an ischemic hand have been emphasized.6,7 Radial artery occlusion specifically following radial artery access for coronary angiography varies between 5% and 38%. 8 Factors associated with greater occlusion rates include: prolonged circulatory failure, hypotension, high-dose vasopressor therapy, duration of cannulation, number of puncture attempts, larger arterial sheaths (> 5 French), peripheral arterial occlusive disease, younger age and female sex.8,9 Symptoms can vary from numbness, stiffness and coolness of the hand or digits to rarely rest pain from acute ischemia. It is important to note that not all patients found to have radial artery occlusions become symptomatic. Of 455 patients prospectively scanned by ultrasound after radial artery access for coronary angiograms, 97 (21%) were shown to have occluded radial arteries. 8 However, 42.5% of these patients were symptomatic within 24 hours and another 7.1% became symptomatic up to 8 days following the procedure. Although none of the patients developed critical ischemia, if 10% (half of 21%) of all patients undergoing radial artery access for coronary catheterization develop symptoms, a screening examination is clearly warranted.
The first objective for some form of objective evaluation prior to harvesting the radial artery is that collateral circulation via the ulnar artery is adequate to perfuse the hand. The second objective is choosing an adequate size conduit free of atherosclerosis. About one of four radial arteries in some series is reported as being unusable for grafting due to size, anatomic absence, plaque or inadequate collateral circulation to the hand.10,11 Therefore, a thorough knowledge of the anatomy and physiology of the palmar arch, variations in anatomy and the pros and cons of a variety of methods to assess the collateral circulation of the hand is required. Because of the variability of the Allen’s test and the subjectivity associated with it, an additional objective testing modality is necessary for assessing hand collateral circulation. This paper reviews the normal anatomy and common variations of the palmar arch, Allen’s test and the pros and cons of various non-invasive tests available for determining adequate collateral circulation to the hand.
Normal anatomy, variations, and vessel diameters
Arterial supply to the hand is provided by the superficial and deep palmar arches. However, there have been a number of anatomic variations reported for the arterial patterns of the hand. The superficial arch is usually formed by direct continuity between the ulnar artery and the superficial branch of the radial artery. 12 Four common palmar digital arteries then arise from the superficial arch, with each common palmar digital artery giving rise to two proper palmar digital arteries (Figures 1 and 2).
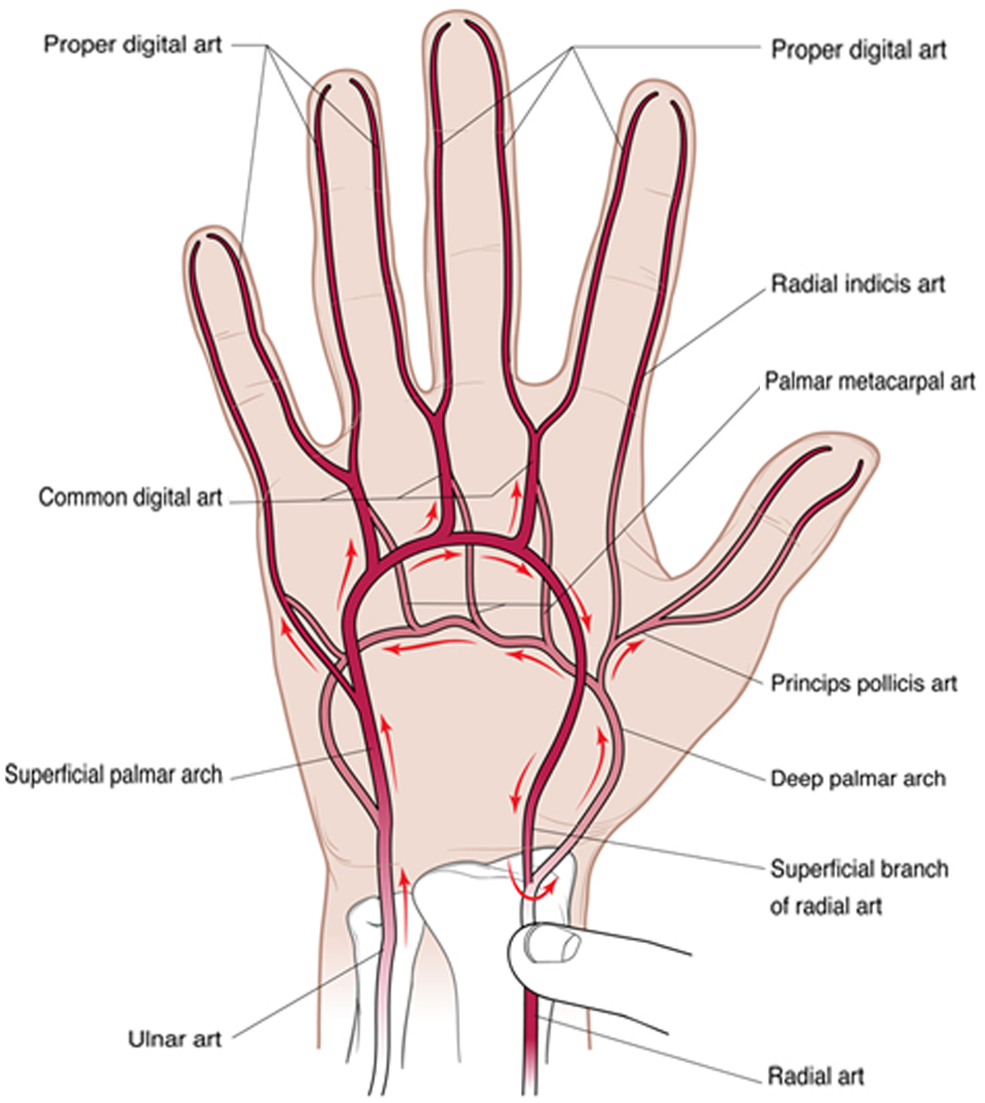
Arterial anatomy of the hand with direction of blood flow with manual occlusion of the radial artery.
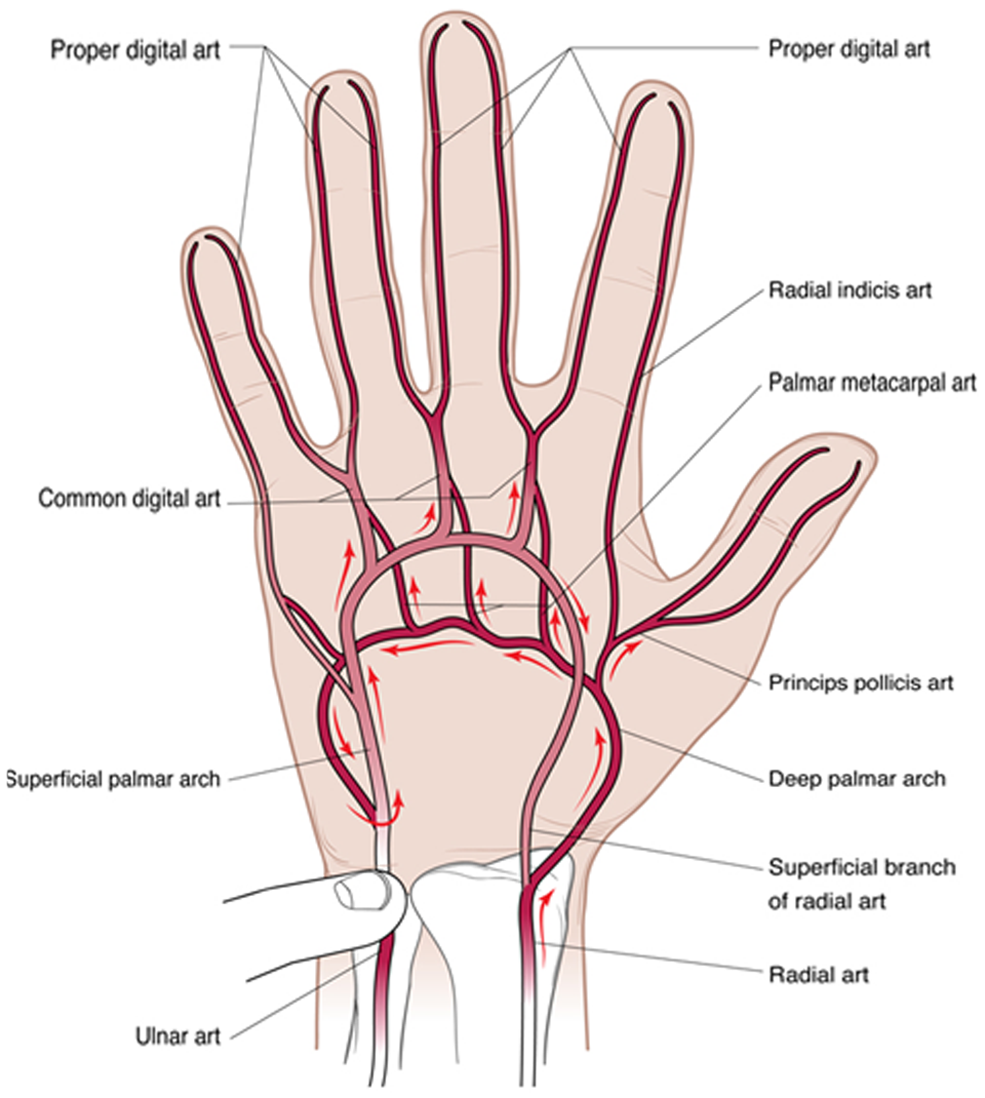
Arterial anatomy of the hand with direction of blood flow with manual occlusion of the ulnar artery.
The deep palmar arch is most often formed by an anastomosis between the deep palmar branch of the ulnar artery and the dorsal radial artery 13 (Figures 1 and 2). Four palmar metacarpal arteries arise from the deep palmar arch and give a contribution to each common palmar digital artery arising from the superficial arch. The princeps pollicis artery and radial indicis artery also arise from the deep arch.
The superficial arch can be classified as either complete or incomplete. To be classified as a complete arch an anastomosis must be present between the vessels constituting it. 14 Fortunately, the majority of superficial arches are complete.13,14
There have been no incomplete deep palmar arches identified in the literature. Three types of complete deep palmar arches have been identified. In the most common pattern the deep arch is formed by an anastomosis between the deep volar branch of the radial artery and the inferior deep branch of the ulnar artery. The second type is where there is an anastomosis between the deep volar branch of the radial artery and the superior deep branch of the ulnar artery. The third type is where the anastomosis is formed by the deep volar branch of the radial artery with both superior and inferior deep branches of the ulnar artery.13,14
The mean diameter of the radial artery at the wrist differs depending on whether the superficial palmar arch is complete or incomplete. Radial artery diameter at the wrist in hands with a complete palmar arch is reported to be 3.1 ± 0.2 mm, whereas for the incomplete arch the mean diameter is 2.6 ± 0.3 mm. 14 The mean diameter for the ulnar artery at the wrist in hands with a complete arch is 2.5 ± 0.2 mm and for the incomplete arch the diameter is 2.6 ± 0.2 mm. The mean diameter of the median artery at the wrist is 1.7 ± 0.3 mm.
Allen’s test
The Allen’s test was first described in 1929 in three patients with thromboangiitis obliterans by Dr Edgar V Allen. 15 His description entailed making a fist with the radial artery occluded for 1 minute followed by extending the fingers and watching for return of color. The original technique has been altered and is called the modified Allen’s test. 16 The test is conducted by having the patient make a fist for 30 seconds. Pressure is applied over the radial and ulnar arteries to occlude them. The patient is then instructed to open the fist and the ulnar artery is selectively released (Figures 1 and 2). Care is taken to avoid a false-positive (abnormal) test by hyperextension of the hand or wide separation of the digits. If sufficient collateral circulation is present there should be normal return of color to the hand within about 3–12 seconds. If return of color does not occur this is called a positive modified Allen’s test and is thought to preclude radial artery harvest. In the original description, no time limit for blushing of the palm is described and to date there is no consensus regarding the optimum cut-off time for a positive modified Allen’s test.
The modified Allen’s test is often used in the preoperative evaluation of the radial artery for coronary artery bypass graft to determine whether sufficient collateral circulation is present throughout the hand to allow harvesting. In a study of 1000 patients undergoing cardiac catheterization, 49% had a normal modified Allen’s test (< 5 seconds), 24% borderline (5–9 seconds) and 27% abnormal (> 10 seconds). 17 However, an abnormal modified Allen’s test does not necessarily imply that hand ischemia will result if the radial artery is harvested. An angiographic study of patients with indwelling radial artery catheters showed complete or partial radial artery thrombosis in 76% and yet none of the hands was clinically symptomatic. 18 With regard to using the modified Allen’s test prior to radial artery access for coronary catheterization or prolonged radial artery lines, the data are certainly not convincing. There is lack of incontrovertible evidence that it can predict hand ischemia and there have been cases of hand ischemia following observance of a normal modified Allen’s test. 9 Part of the explanation may be that digital embolization is the etiology, which can lead to digit and hand ischemia in the setting of anatomically normal arteries as well as a normal modified Allen’s test. 9
While the modified Allen’s test has been used reliably prior to coronary artery bypass grafting as well as percutaneous procedures, there are some limitations to using the test exclusively. Pallor, an uncooperative or unconscious patient or other anatomic factors makes the test highly subjective in nature. The modified Allen’s test may be misleading because of anatomic anomalies within the forearm arteries. False-positives and negatives can also occur because there are observer biases in deciding when the normal return of color to the hand occurs. In addition, if the radial artery is not completely occluded during the test it can lead to false-negatives. Conversely, false-positives may occur if the wrist is hyperextended. 19
Various non-invasive tests have therefore been added to the modified Allen’s test to improve the reliability of the test and avoid hand ischemia. 20 Jarvis and colleagues compared a modified Allen’s test to a Doppler ultrasound assessment of collateral ulnar flow in 93 coronary artery bypass graft patients. 19 By using the receiver operating characteristics, a cut-off of 6 seconds resulted in a sensitivity of 54.5% and a specificity of 91.7%. If a cut-off of 5 seconds was used, the sensitivity increased to 75.8% but the specificity dropped to 81.7%. For a cut-off of 3 seconds the sensitivity was 100% but the specificity dropped to 27%. The authors proposed that the modified Allen’s test should be abandoned and replaced with more objective tests such as Doppler ultrasound. However, Meharwal et al. reported no acute ischemic hand symptoms in a large series of 4172 harvests in 3977 patients. 2 They utilized a cut-off of 3–12 seconds of a palmar flush to indicate a positive modified Allen’s test along with intraoperative pulse oximetry and the only adverse finding was a 5.2% incidence of hand ‘weakness’ at 4 weeks. Ruengsakulrach and colleagues also validated the modified Allen’s test with a 10 second cut-off in a series of 71 patients undergoing coronary artery bypass grafting. 21 An abnormal modified Allen’s test was noted in four (5.6%). All patients with a recovery time of < 10 seconds had uneventful harvesting of their radial arteries.
Starnes compared the modified Allen’s test with Doppler ultrasound and to digital blood pressures before and after radial artery compression. They identified a false-positive (abnormal modified Allen’s test rate of 50% in their series), and radial artery harvest was performed in 52/129 patients with no ischemic sequelae. 22 Because of the limitations of the Allen’s test, some experts have reported harvesting the radial artery despite an abnormal Allen’s test 23 (Table 1).
Literature review of Allen’s test
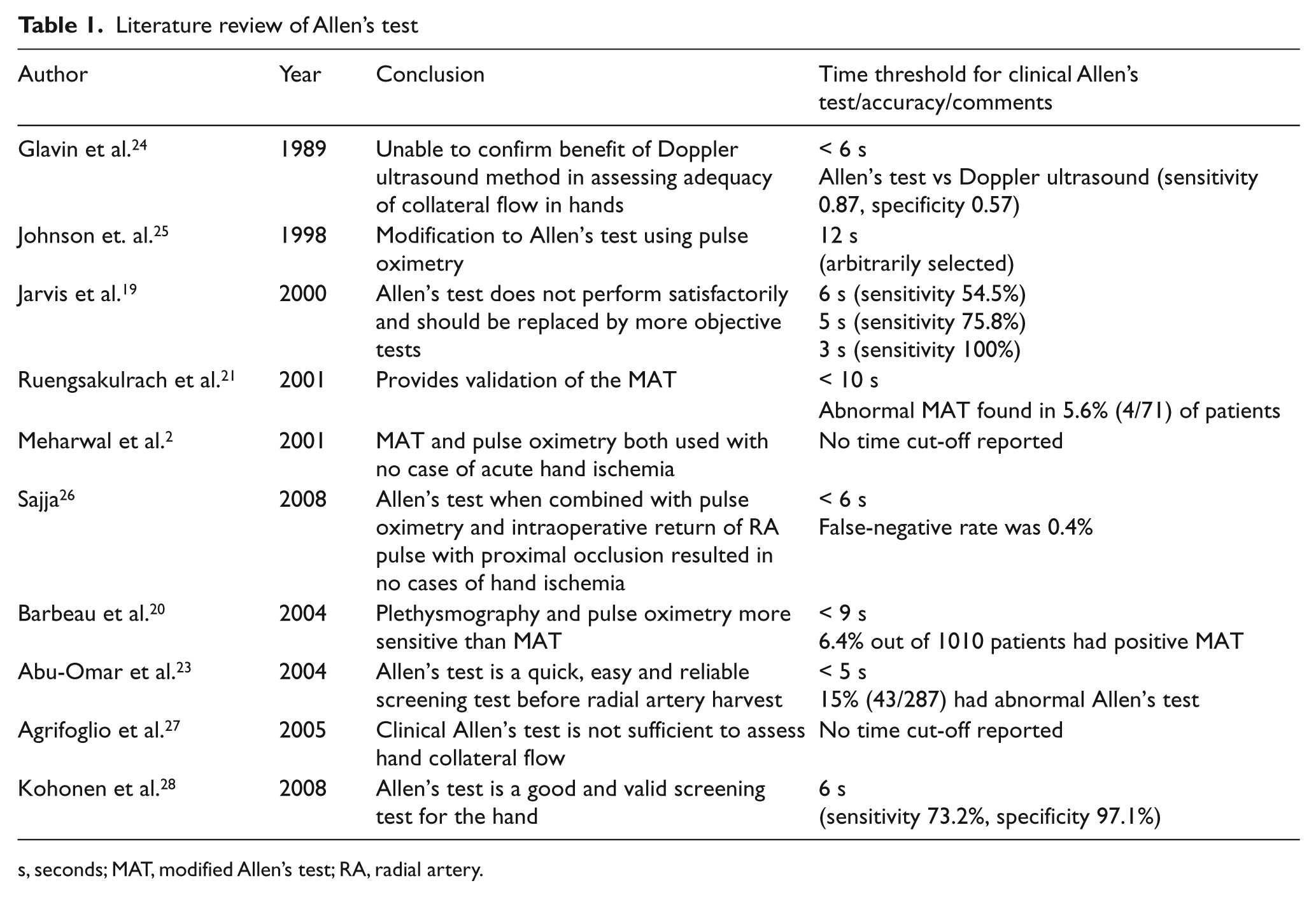
s, seconds; MAT, modified Allen’s test; RA, radial artery.
Non-invasive determination of adequate collateral circulation
There is no consensus in the literature on the most appropriate pre-operative non-invasive testing modality prior to radial artery harvest for coronary artery bypass grafting. We now explore some of the most frequently used non-invasive methods to evaluate the radial artery for possible use in coronary artery bypass graft procedures.
Digital plethysmography
Digital plethysmography can be performed using photoplethysmography or pulse volume recordings.
A photoplethysmography sensor is placed on the tip of the finger using double-sided tape to help hold the sensor in place and a 3–4 cm cuff is placed at the base of the finger (Figure 3). The hand needs to be resting flat palm side up with the patient in a supine position to allow for minimal movement. It is important for the hand to be steady so a reliable tracing can be obtained. Once a reliable tracing is noted, free of motion artifacts, a minimum of at least three cardiac cycles should be captured. Our protocol is to record baseline waveforms of the first, second and fifth digits. If the baseline waveforms are of normal contour, compression maneuvers are then performed. Compression maneuvers are performed for each digit examined with the radial artery compressed while a photoplethysmography tracing is captured and then a tracing is taken with the ulnar artery compressed.

Photoplethysmography sensor placed on the tip of the finger using double-sided tape and a 3–4 cm cuff is placed at the base of the finger.
Interpretation
The photoplethysmography tracings should be classified as either normal or abnormal. Normal photoplethysmography tracings should have the following characteristics: a sharp upstroke during peak systole, a prolonged downstroke with a dicrotic notch and the waveform should downslope towards the baseline (Figure 4). In contrast, an abnormal photoplethysmography waveform is suggested by a prolonged onset to peak with a rounded appearance at the peak. The waveform then bows away from the baseline and the overall amplitude is decreased (Figure 4).
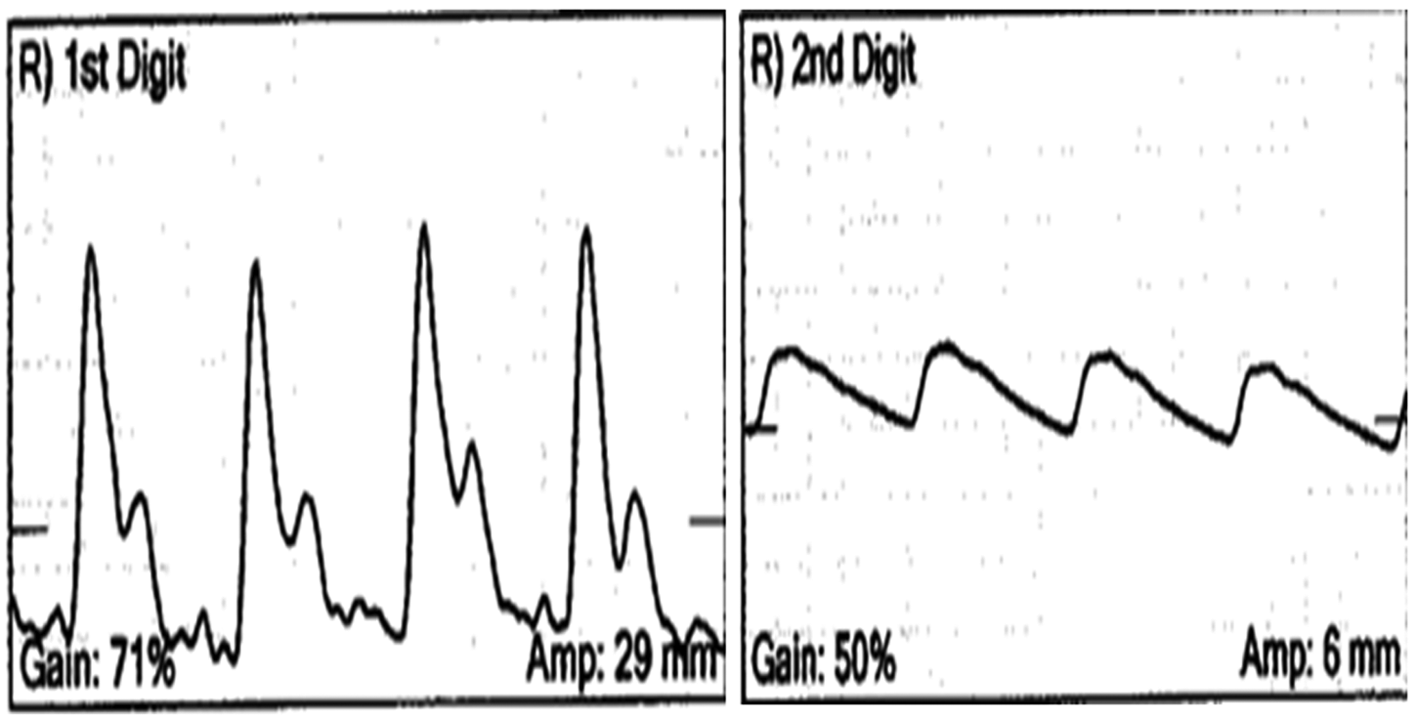
(Left) A normal photoplethysmography tracing showing a sharp upstroke during peak systole, a prolonged downstroke with a dicrotic notch. (Right) An abnormal photoplethysmography waveform shows a prolonged onset to peak and has a rounded appearance at the peak. The waveform then bows away from the baseline and the overall amplitude is decreased.
If there is no noticeable decrease in amplitude of the waveforms with compression maneuvers, a good collateral circulation to the hand is presumed. A complete disappearance of the oscillations clearly suggests inadequate arterial circulation to the finger being evaluated.
Fronek used photoplethysmography sensors attached to the tips of the first, third, and fifth digits to help objectively evaluate the patency of the radial and ulnar arteries. 29 Pulse volume oscillations were recorded in the first, third, and fifth fingers after sequential compression of the radial and ulnar arteries. In 25 normal subjects, they found that there was a 35% reduction in the pulse volume recording with compression of either artery. In patients with an occluded ulnar artery, compression of the radial artery resulted in a disappearance of the pulse volume recording. A pulse volume drop of > 55% was found in patients with varying degrees of ulnar and radial artery stenosis. 29 However, there appears to be no absolute value for a normal response to radial artery compression in the amplitude of the waveform since the change in oscillation is subjective and not easily quantifiable.
Digital Doppler waveforms and pressures
Digital pressures are obtained by cuff inflation at the base of the digit until the signal is obliterated then slowly released to obtain a pressure. The same method is used with the radial artery and then the ulnar compressed to evaluate the patency of the palmar arch.
Interpretation
Normal values for digital pressures are considered to be a finger–brachial index of > 0.90 using the brachial artery pressure of the ipsilateral arm. 30 There is no agreement on what is considered a significant drop in pressure. Starnes et al. suggest a 40 mmHg pressure drop after radial artery compression is significant. 22 They showed a poor correlation between a modified Allen’s test and a decrease in digit pressures after radial artery compression in normal volunteers. They also observed that 50% of extremities with an abnormal modified Allen’s test had a change in digit pressures of 40 mmHg with radial artery compression. Therefore, these patients would have been excluded from radial artery harvest if the modified Allen’s test had been the sole criterion. Also, 9% of limbs with a negative modified Allen’s test had a reduction in digit pressure of 40 mmHg or more with radial artery compression. This latter group of patients may have been exposed to the risk if digit ischemia after radial artery harvest.
Based upon experience with a steal syndrome associated with dialysis grafts, Rodriguez and colleagues consider a 40% decrease in the digital systolic pressure in the first and fifth digits after radial artery compression to be abnormal. 10 They evaluated 346 arms in 187 patients with Doppler ultrasound imaging and digital plethysmography. A total of 27% were excluded from harvest based on either anatomic or physiologic criteria. Nineteen arms demonstrated > 40% decrease in systolic pressures with an average of 71% from baseline pressures. Based on this protocol, no digit ischemia developed after harvesting of the radial artery. It is notable that they also excluded from harvest a small group (5.5%) of patients with low baseline digit pressures despite normal palmar arch reversal and ulnar increases with radial compression. Another important point emphasized by the authors is that more than half the limbs excluded from harvest were because of anatomic abnormalities such as calcification, which would not have been observed with an Allen’s test or digit pressures and waveforms.
Duplex ultrasonography
Duplex ultrasonography is a useful tool to evaluate the radial artery in addition to indirect methods. A high-frequency transducer between 8 and 15 MHz is selected for better wall definition since the arteries in the arm are usually superficial. Ultrasonic gel is applied to the forearm. The transducer is aligned in the proximal forearm in the transverse plane to the radial artery. The radial artery diameter is measured in the proximal, mid and distal segments. Additional measurements are taken if there is the presence of a branch, a reduction in diameter is visualized or if any pathology is noted.
The transducer is then turned 90 degrees to obtain a long axis view of the radial artery. A Doppler waveform is obtained using a 60 degree angle in the middle of the vessel parallel to the walls. A peak systolic velocity is recorded. Color Doppler is also applied to assist with evaluating the velocity and direction of flow in the radial artery.
Interpretation
There is no consensus with regard to the acceptable diameter of the radial artery for use in a coronary artery bypass grafting procedure. The normal diameter range of the radial artery is between 2.3 mm and 5 mm. 14 It is suggested that a diameter of < 2.0 mm makes the radial artery less than ideal for use as a coronary artery bypass graft conduit. Visualizing calcification within the radial artery wall and identifying a significant stenosis are contraindications for use in coronary artery bypass grafts. Rodriguez et al. excluded radial arteries if they were < 2 mm in diameter, had diffuse calcifications or had anatomic variants. 10 They defined diffuse calcification as multiple echogenic foci with shadowing or diffusely increased echogenicity of the vessel wall with luminal narrowing. Agrifoglio et al. excluded patients from radial artery harvest when the radial artery peak systolic flow velocity is < 0.20 m/s, or the radial artery diameter is < 2.0 mm, or if there are radial artery calcifications and atherosclerotic plaques. 27
In terms of hemodynamic parameters, a peak systolic velocity of between 40 and 90 cm/s is considered to be within a normal value range in the radial artery. 31 A triphasic Doppler waveform in the radial artery also indicates good arterial perfusion. However, many factors may affect the characteristics of the Doppler waveform, such as room temperature and clenching the fist. 31
Measurement of flow velocities and waveform analysis of the radial artery and ulnar artery have been used with duplex ultrasonography alone or in conjunction with the modified Allen’s test to assess collateral circulation to the hand. Abu-Omar and co-authors reported using a modified Allen’s test and duplex ultrasonography in 287 patients undergoing coronary artery bypass graft. Forty-three (15%) had an abnormal modified Allen’s test and were then subjected to duplex ultrasonography. 23 The authors reported on their ability to use the radial artery conduit in 99% of instances. Normal findings (patent vessel, normal waveforms and velocities) were noted in 38 patients whereas five had abnormal radial artery or ulnar artery findings (occlusion or a doubling of systolic velocities suggesting > 50% diameter stenosis).
Sullivan et al. have reported no correlation between ulnar artery velocity changes and digit pressure change during radial artery compression in 40 normal subjects. 32 They concluded that velocity changes cannot be used to determine potential digit ischemia following radial artery harvesting and therefore recommend using digital pressure measurement with radial artery compression as the preoperative screening tool prior to radial artery harvest.
Advantages of duplex ultrasonography include the ability to map the entire vessel for size and morphology, note calcified or stenotic areas, and observe common anatomic variants of the radial artery such as a high takeoff and record hemodynamic parameters in the forearm and hand.
Duplex ultrasonography dynamic test
Dynamic tests using duplex ultrasonography can be performed to assess hand collateral circulation. The duplex ultrasonography dynamic test is performed in the following fashion. A 10 MHz transducer is used to determine the peak systolic velocity in the ulnar artery at the wrist, the superficial palmar branch of the radial artery and the dorsal digital thumb artery. In one version of the dynamic Allen’s test performed with duplex scanning, the ulnar artery peak systolic velocity at the wrist is measured before and after radial artery compression. An increase in velocity after radial artery compression is a sign of adequate collateral perfusion. Radial artery flow reversal after radial artery compression is also evidence of good collateral circulation (Figure 5).
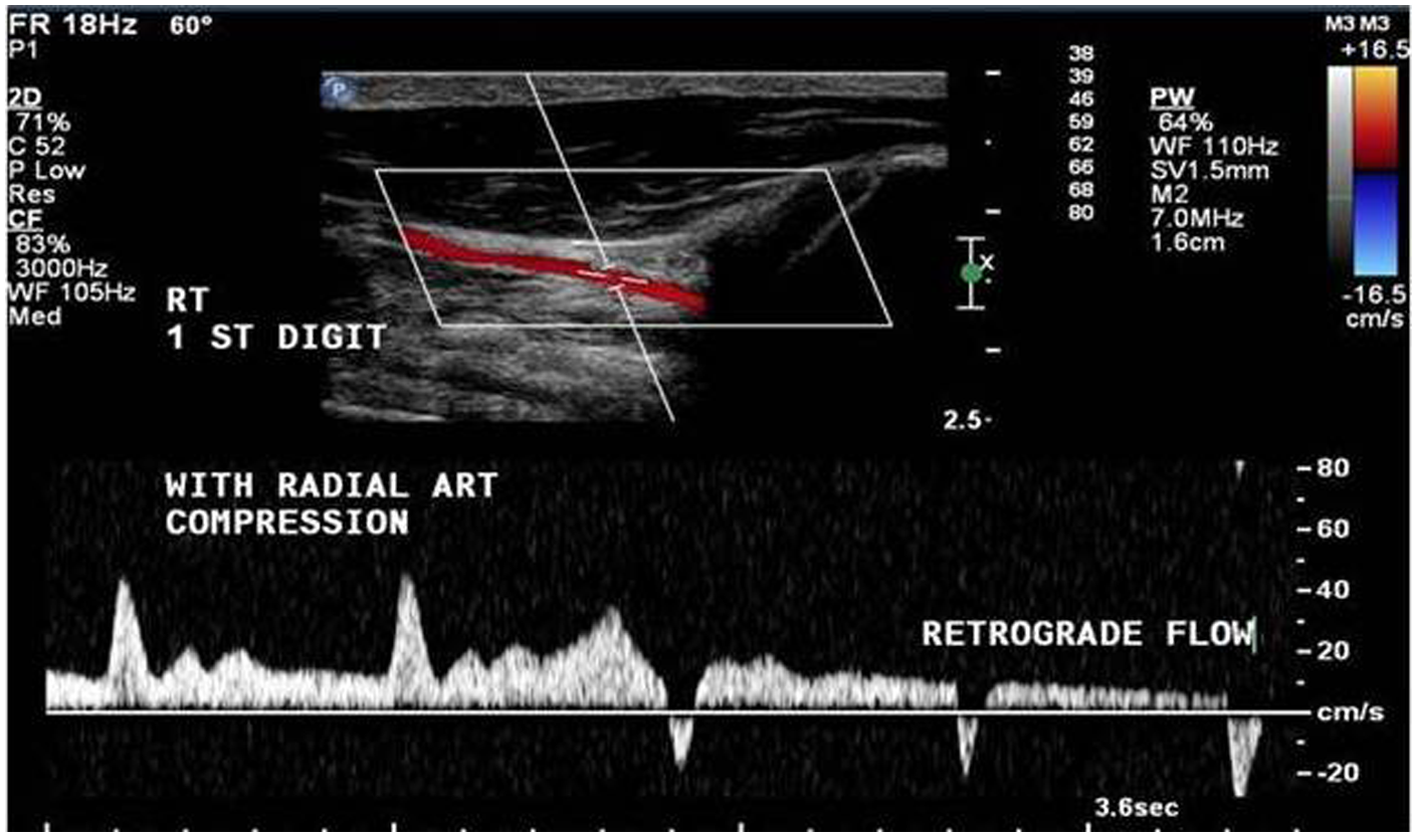
Duplex ultrasound of the first digit with manual compression of the radial artery showing reversal (retrograde) of flow indicating adequate collateral circulation to the hand.
Rodriguez et al. used color flow duplex ultrasonography to determine radial artery reversal of flow during radial artery compression in the mid or proximal forearm and also to detect stenoses. 10 A doubling of the velocity from the pre-stenotic to the stenotic area was defined as a significant stenosis. Velocity in the ulnar artery with radial artery compression was also determined with Doppler. An increase in ulnar artery velocity less than 20% from baseline with radial artery compression was considered abnormal.
The palmar arch test is where the probe is positioned on the thenar eminence to measure the superficial palmar artery flow direction during radial artery compression. Backward flow here indicates good perfusion of the superficial palmar arch. In a patient with an incomplete palmar arch, no flow reversal in the radial artery occurs. Instead, there is very low-flow antegrade flow (Figure 6). The test can also be conducted by placing the Doppler probe in the anatomic snuffbox.
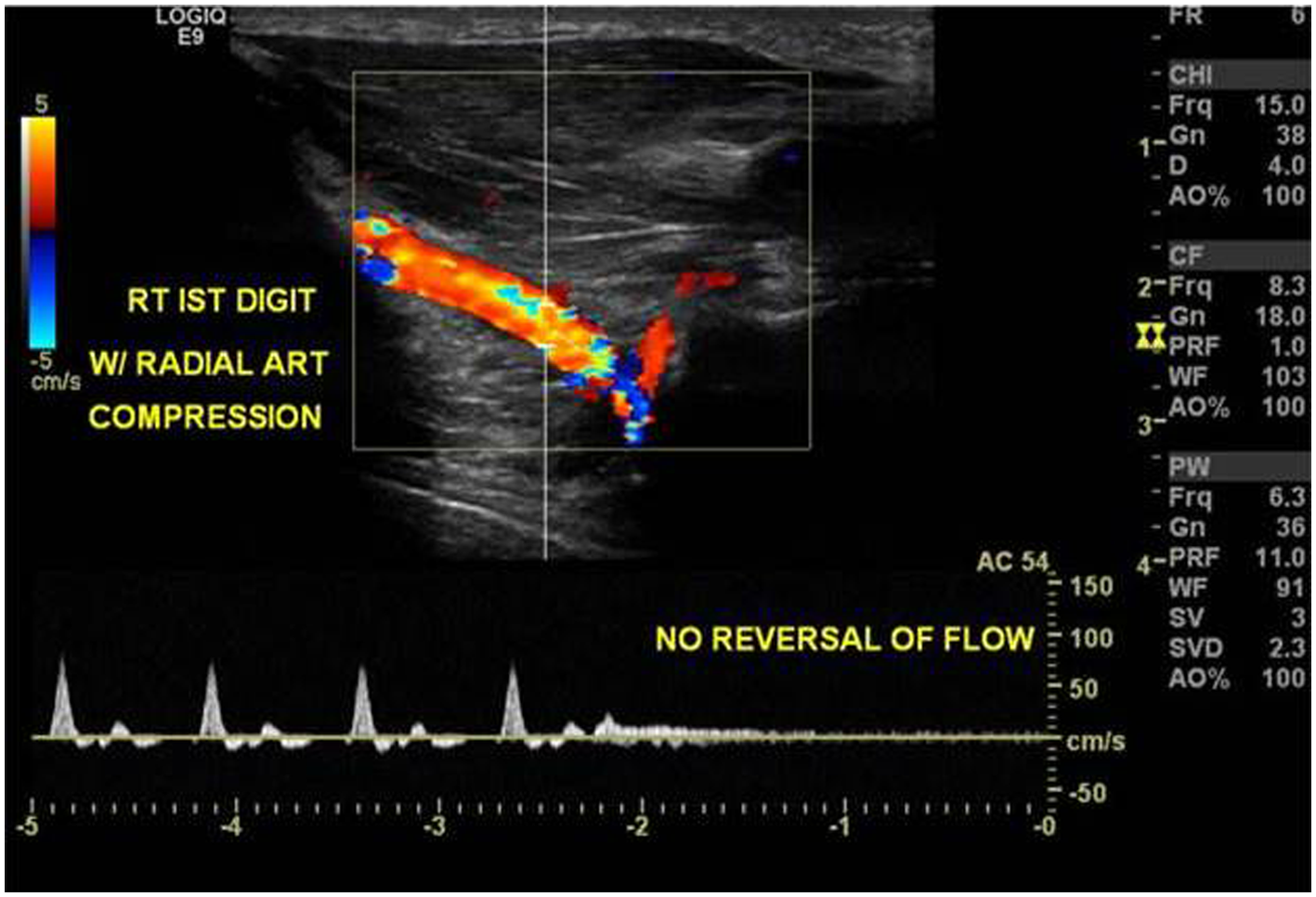
Duplex ultrasound of the first digit with manual compression of the radial artery showing no appreciable flow and also no reversal of flow.
Pola and his colleagues described their experience using dynamic duplex ultrasonography in identifying 11 of 188 patients in whom the collateral circulation to the hand was deemed inadequate. 33 One of the criteria used was an absence of increase in blood follow velocity in the ulnar artery following flow disappearance in the superficial palmar arch during radial artery compression. The authors contended that an increase in blood flow in the ulnar artery after radial artery occlusion was expected due to an increase in the pressure gradient between the ulnar artery and the capillary bed of the palm. An absence of flow in the dorsal digital artery to the thumb during radial artery compression was considered an absolute contraindication to radial artery harvesting.
In another report, no ischemic events developed in 142 patients undergoing radial artery harvest when echo color Doppler was performed during static and dynamic tests. 27
Pulse oximetry
This technique consists of attaching a pulse oximeter sensor on the thumb or forefinger and measuring first the baseline oxygen saturation and waveform. Following this, both the radial artery and the ulnar artery are compressed until the saturation reaches zero. The pressure on the ulnar artery is then released and the time to reach baseline saturation and the waveform is recorded.
Although the test has not usually been utilized as the sole method of assessing collateral circulation to the hand, intraoperative pulse oximetry has been used to supplement a preoperative Allen’s or a modified Allen’s test. 2 Johnson used pulse oximetry to identify return of perfusion to control levels during an Allen’s test in 452 forearms using an arbitrary 12 second cut-off time. 25 In the same time period, the authors identified 21 patients (5%) with radial artery dominance in whom the radial artery was not harvested. In another series of 241 patients undergoing coronary artery bypass grafting, a modified Allen’s test was used along with pulse oximetry. No adverse consequences were noted utilizing a cut-off of 6 seconds for reappearance of the pulse wave on pulse oximetry. 26 Glavin, using 6 seconds as a cut-off, showed that the test was associated with both false-positives and false-negatives. 24 Limitations of the test include the fact that the amplitude of the waveform may vary depending on which finger the probe is placed as well as the proximity of the probe to the patent arterial source. 34
Contraindications to radial artery harvesting
Contraindications to radial artery harvesting can be determined by a modified Allen’s test, Doppler ultrasound, plethysmography or duplex ultrasonography. Contraindications may be classified as morphological or circulatory. Morphological contraindications include a radial artery inner diameter < 2 mm, diffuse intimal or medial calcification or anatomical anomaly. 10 Circulatory contraindications include the absence of flow reversal in the radial artery during radial artery compression or < 20% increase of ulnar peak systolic flow during radial artery compression.32,33 Contraindication by plethysmography includes a > 40% decrease in digital pressure during radial artery compression. When there is a contraindication for radial artery harvest in the non-dominant hand, the risk of having a non-harvestable artery in the dominant hand is doubled. 28
Patients with hand ischemia after radial artery harvest can present with a variety of symptoms ranging from hand fatigue, to resting pain and gangrene. Severe ischemia has been reported to develop in up to 0.03%, whereas mild ischemia may develop in up to 10%. 35 Ischemia after radial artery harvest may result from occlusive artery disease in the forearm or poor ulnar artery flow reserve. Scanning of the ulnar artery and examining flow during the Allen’s test may be useful as a preoperative screening test. 36 According to Manabe, severe hand ischemia has not been documented as a result of an incomplete palmar arch. 36
Conclusions
A complete palmar arch and a normal ulnar artery are essential prior to procedures that risk radial artery continuity. Between 15% and 23% of patients being considered for coronary artery bypass grafting appear to have an abnormal modified Allen’s test.19,25 The specificity of the modified Allen’s test is in the 97% range with a 6 second cut-off. Therefore, if the modified Allen’s test is abnormal an additional non-invasive test is appropriate since the relatively lower sensitivity of the modified Allen’s test means that the radial artery may be safe to harvest in many patients. 25
The prevalence of patients at risk for hand ischemia following radial artery harvest can be extrapolated. There are approximately 183,000 coronary artery bypass graft operations performed in the US annually. 37 Of these, 15% can be expected to have an abnormal modified Allen’s test and about 11.6% of those with an abnormal modified Allen’s test will have an abnormal duplex ultrasound examination. 23 Exactly how many actual ischemic hands would have resulted after harvesting of the radial artery is hard to extrapolate from available data since most centers use some form of pre-operative screening test.
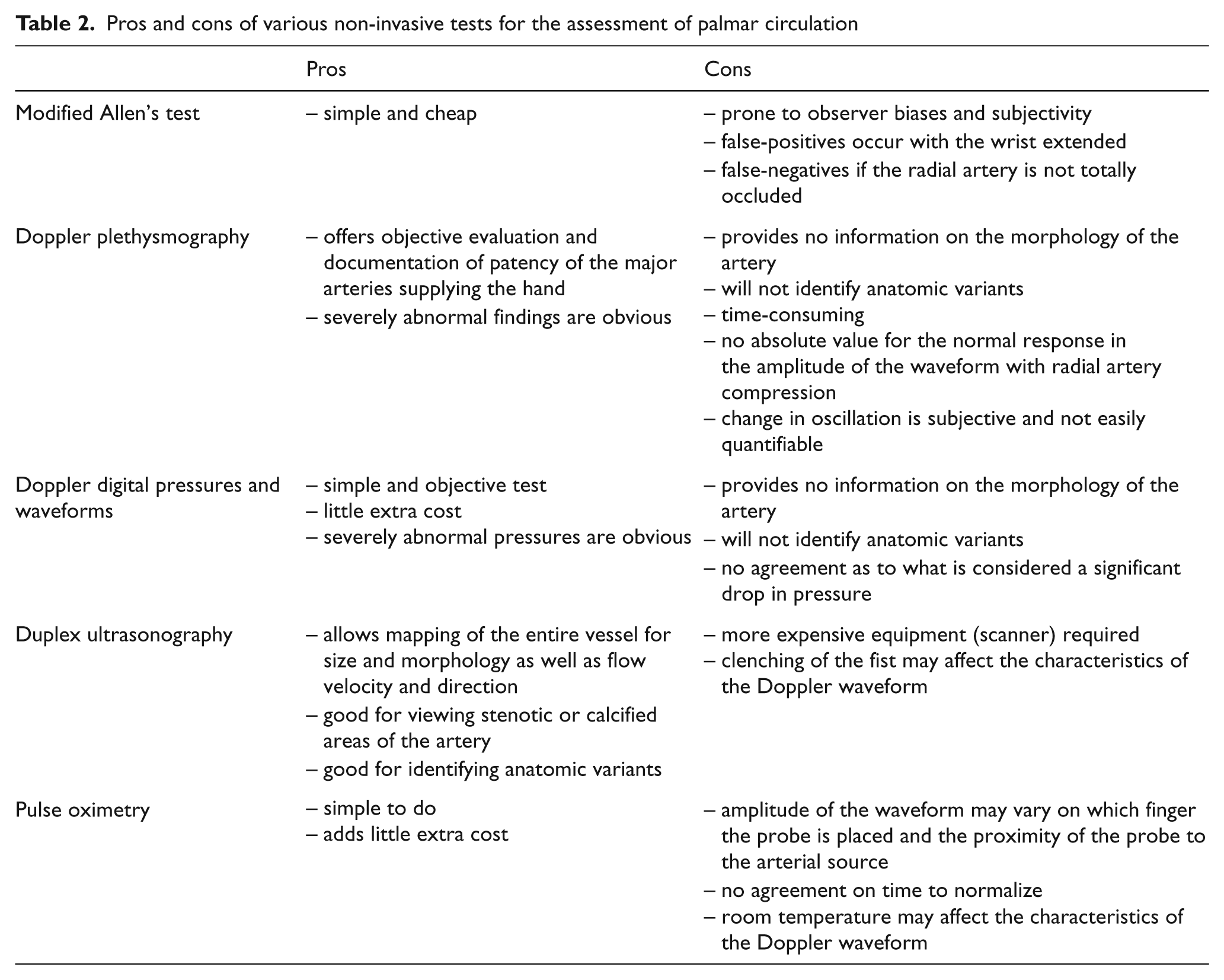
There is no consensus on the best test for assessing collateral circulation of the hand and the choice of non-invasive test depends upon the preference of the individual vascular laboratory or surgeon. To date, no guidelines have been published for differentiating between normal and abnormal Doppler ultrasonographic results. Similarly, no standard set of plethysmography pressure measurements have been established for radial artery harvest. Digital Doppler waveforms, pressures, pulse oximetry and duplex ultrasonography with systolic velocity measurements all have their advantages and disadvantages (Table 2). The major limitation of the physiologic, non-imaging methods is that they cannot provide information about the size and morphology of the radial artery in assisting the surgeon who is deciding whether to utilize the radial artery for coronary artery bypass grafting. In addition, plethysmography waveforms can be highly subjective and digital pressures even in ‘normal’ hands can vary significantly from digit to digit, often providing conflicting information.
Pros and cons of various non-invasive tests for the assessment of palmar circulation
For patients being evaluated for arterial blood gases, blood draws and short-term arterial lines, a modified Allen’s test that shows adequate collateral flow may be all that is necessary. For patients subjected to cardiac catheterization or long-term lines or radial artery harvest, a dynamic duplex ultrasonography can provide anatomic, morphologic and physiologic information and it may be the best available non-invasive test to supplement the modified Allen’s test, particularly if the latter is abnormal. From a physiologic standpoint, the absence of reverse flow in the superficial palmar branch in the hand upon radial artery occlusion or an absence of flow in the dorsal digital artery to the thumb during radial artery compression appear to represent contraindications to radial artery harvest.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.