
Abstract
Peripheral artery disease (PAD) is an understudied chronic illness most prevalent in elderly individuals. PAD patients experience substantial walking impairment due to symptoms of limb ischemia that significantly diminishes quality of life (QOL). Cardiovascular disease (CVD) morbidity and mortality is increased in this population because of aggressive atherosclerosis resulting from untreated CVD risk factors. Despite current national guidelines recommending intensive CVD risk factor management for PAD patients, untreated CVD risk factors are common. Interventions that bridge this gap are imperative. The Vascular Insufficiency – Goals for Optimal Risk Reduction (VIGOR2) study is a randomized controlled trial (RCT) that examines the effectiveness of a long-term multifactor CVD risk reduction program on walking and quality of life in patients with PAD. The purpose of this article is to provide a detailed description of the design and methods of VIGOR2.
Keywords
Introduction
Peripheral artery disease (PAD) affects 8–10 million Americans and is associated with increased cardiovascular disease (CVD) events and death.1–3 Clinical presentation of PAD varies, but typically these individuals are elderly with multiple CVD risk factors including hypertension, diabetes, hyperlipidemia, smoking, obesity and physical inactivity due to limited walking ability resulting in poor quality of life (QOL).4–6 Current treatment options for PAD patients focus on limb salvage, reducing CVD events and death, and improving walking or functional capacity. 7 To attain these outcomes current clinical guidelines recommend aggressive CVD risk factor management inclusive of appropriate pharmacologic agents that have demonstrated efficacy in lowering CVD events including angiotensin-converting enzyme inhibitors (ACE-I), statins and antiplatelets. In conjunction with these agents, adoption of a healthy lifestyle with diet and exercise is recommended.8–10 Despite these recommendations, disparities in treatment and outcomes have been reported for this patient population compared with that for individuals with coronary artery disease.3,11,12
Background
Current treatment guidelines for PAD focus on optimal management of CVD risk factors. 7 Current recommendations include medications for improving individual risk factors as well as incorporating lifestyle modification including healthy diet and exercise regimens. In addition, exercise or a supervised walking program is recommended to improve walking impairment in this population.7,13 While reducing CVD risk factors is important for enhancing long-term outcomes such as CVD events and death, what is immediately meaningful to these patients’ quality of life is maintaining or improving physical function – specifically, walking. Our study focuses on examining the efficacy of patient-centered behavioral interventions to reduce CVD risk factors and their impact on improving walking ability. Walking was selected not only because of its clinical significance in this patient population, but also because of the known association between CVD risk factors and exercise. While the biological underpinnings for this association have not been conclusively demonstrated in PAD, there is evidence suggesting a relationship between CVD risk factors and endothelial function and the progression of atherosclerosis. Current studies show that CVD risk factors are associated with endothelial dysfunction and reduced nitric oxide (NO) bioavailability. This impairment is reversed with treatment. Additionally, there is a positive relationship between endothelial function, walking and CVD risk factors, including hypertension, diabetes, obesity, hyperlipidemia and PAD. Thus, while there is currently no direct evidence demonstrating that improving CVD risk factors alone (i.e. lowering blood pressure, lipids and glucose levels) enhances walking time, there is substantial evidence indicating a positive relationship between CVD risk factors, endothelial function and walking. Therefore, we propose that lowering CVD risk factors will improve vascular milieu, thereby restoring NO bioavailability that will translate into improved walking ability. This is further substantiated by the effect of exercise on improving a number of CVD risk factors.
Although evidence demonstrates the efficacy of pharmacological and non-pharmacological therapies for PAD, owing to the complexity of care regimens for multiple CVD risk factors and the age of this patient population, successful implementation and adherence to treatment recommendations are challenging. To address this issue, we incorporated a patient-centered behavioral intervention to address treatment adherence. For the purposes of our study, patient-centered care is defined according to the Institute of Medicine as ‘care that is respectful of and responsive to individual patient preferences, needs, and values’. We also expanded this to include patients as partners, involving them in planning their health care and encouraging them to take responsibility for their own health. Studies suggest that by using this approach, patients are more likely to adhere to medications, alter their diets and be more actively involved in their care.14–20
Thus, the Vascular Insufficiency – Goals for Optimal Risk Reduction (VIGOR2) study is a randomized controlled trial (RCT) that examines the efficacy of a 24-month, patient-centered, behavioral intervention focusing on lifestyle modification emphasizing exercise and healthy diet to increase peak treadmill walking time and self-reported walking impairment compared to enhanced usual care in men and women with PAD. A secondary objective is to assess the program’s effects on quality of life as measured by the SF-36 (ClinicalTrials.gov Identifier: NCT00537225). The purpose of this article is to provide a description of the design and methods of VIGOR2.
Theoretical foundation for behavioral intervention
The study intervention is based on three behavioral theoretical constructs: (1) the transtheoretical model recognizes an individual’s readiness for change or stages of change; 21 (2) cognitive behavioral therapy (CBT) assists a motivated individual to initiate, adopt and maintain healthy behaviors 22 ; and (3) self-efficacy from social cognitive theory that emphasizes the human capacity for self-directed change through an individuals’ own motivation and behavior. 23 These theoretical constructs will be implemented by study case managers using motivational interviewing, a therapeutic approach to facilitate behavioral change. 24 Previous studies report the effectiveness of these approaches in facilitating behavior change in a variety of clinical settings.22,25–29
The transtheoretical model describes change as occurring through a series of distinct stages (precontemplation, contemplation, preparation, action, maintenance) with interventions that are most appropriate and effective to facilitate change. 21 Processes that facilitate an individual to move from early stages of change (precontemplation, contemplation and preparation) to action include cognitive, affective, and evaluative strategies. Specific CBT activities in the precontemplation phase include: raising consciousness (increasing awareness), dramatic relief (emotional arousal), and environmental reevaluation (social reappraisal). Self-reevaluation (self-reappraisal) and social liberation (environmental opportunities) are key strategies during the contemplation and preparation stages.22,30 As an individual moves from preparation to action, CBT strategies include: commitment, conditioning, contingencies, environmental controls, and support. 31 The action phase involves self-liberation (commitment). Once behavior is adopted for at least 6 months, maintenance strategies emphasize reinforcement management (rewarding mechanism), counter-conditioning (substituting), stimulus control (re-engineering), and helping relationships (social support reinforcement management).21,32–34 Relapse prevention is emphasized throughout. 31
CBT views health behavior as acquired and maintained through a complex set of behavioral, cognitive, and environmental factors. 35 CBT focuses on restructuring attitudes, beliefs and misconceptions; identifying potential barriers; and assisting individuals in developing strategies to overcome them. The cognitive-behavioral assumption of the intervention is that durable change occurs temporally through a series of distinct stages beginning with problem identification and proceeding through building commitment, increasing awareness, developing an action plan, evaluating the results, and working to maintain specific goals.36–38 CBT strategies have been found to be effective across the lifespan, in a variety of health behaviors and with all stages of change.39,40
Motivational interviewing is a dynamic, patient-centered approach to facilitate behavior change by assisting individuals to explore and resolve ambivalence to change and identify discrepancies between present behavior and goals. 41 Motivation is defined as a situational state of readiness for change rather than a personality trait; thus, resistance or lack of motivation is amenable to change.42–44 Motivational interviewing is a narrative process involving respectful discussions to explore an individual’s perceptions.44,45 A key strategy in motivational interviewing is improving self-efficacy.
Self-efficacy (SE) is defined as an individual’s belief in their ability to successfully perform behaviors or take actions to achieve goals despite barriers and obstacles. 46 Specific to walking, self-efficacy theory suggests that an individual with high efficacy expectations will walk regularly and continue, despite barriers such as discomfort, compared to those with low efficacy expectations. In the VIGOR2 study, self-efficacy will be assessed at the time behavioral goals are developed and used to assess an individual’s level of confidence in their ability to achieve goals and to develop effective strategies to overcome barriers.
Based on the behavioral constructs described above, key behavioral strategies used in the VIGOR2 study intervention will include: (1) comprehensive assessment of CAD risk factors for goal-setting, monitoring progress and providing feedback; (2) matching intensity and prioritizing risk factor management with specific clinical needs; (3) recognizing behavioral interdependence of multiple risk factors; (4) explicit short and long-term goal-setting by patients, with guidance from care managers; (5) defining specific strategies for short-term goal attainment (including potential barriers and facilitators to goal attainment); (6) continuity and tracking of adherence to strategies and adjusting short-term goals as needed; (7) matching of patients with available and appropriate community resources; (8) focusing on patient adherence; and (9) engaging patients to be actively involved in their own care.
Materials/design
Study design
The study design is a randomized controlled trial (RCT) of 300 men and women aged 50 years and older who meet medical criteria. Following a baseline evaluation, subjects will be randomized into one of two groups: intervention (Int) or enhanced standard of care (ESC) for 24 months. Individuals in the intervention group will meet with one member of the care management team face to face or by telephone at minimum every 3 months or more frequently if needed. Individuals in the ESC group will receive limited contact with the care team at baseline, 12 months, and 24 months. These individuals will be invited to four group health education sessions a year. All subjects will be retained in their originally assigned condition for 24 months.
Ethics
Institutional review board approval was granted by the Committee on Human Research at the University of California, San Francisco (UCSF).
Study population and site
Inclusion criteria
Subjects eligible for this study include: (1) age 50 years or older with one or more CVD risk factors; (2) PAD secondary to atherosclerosis as documented by: (a) ankle–brachial index (ABI) < 0.90; (b) toe pressure < 70 mmHg in patients with diabetes; (c) ABI 1 minute after exercise at least 20% lower than index leg resting ABI; (3) capable of walking at least 50 feet (15.24 meters); and (4) difference of walking time between two consecutive (of four) baseline treadmill tests < 25%.
Exclusion criteria include: (1) active malignancy or tumor or other condition that would severely limit life expectancy; (2) any type of major surgery during the past 3 months (i.e. aortic or lower extremity artery surgery, angioplasty, or lumbar sympathectomy, leg amputation above the ankle); (3) residence in a long-term institutional setting; (4) psychiatric disorders with currently active manifestations; (5) uncontrolled metabolic disorders (renal failure, liver failure, thyrotoxicosis); (6) active symptoms suggestive of an acute coronary syndrome or decompensated heart failure; (7) lack of phone access (either by self or through neighbors/family members); (8) other specified circumstances incompatible with case management (i.e. plan to move away from area); (9) presence of another household member or first-degree relative already enrolled in the study; and (10) current enrollment in another clinical trial.
Recruitment
Three hundred men and women with PAD will be recruited using multiple strategies. The primary approach will be mass mailing to individuals over the age of 70 years by proximity to the medical facility. Other plans include: (1) advertising in local newspapers, health clinics, and senior centers; (2) sending letters and flyers to local primary care providers (PCP), vascular and cardiac surgery and cardiac rehabilitation services; and (3) providing free ABI screening at local community health fairs and senior centers.
Randomization procedures
After an individual is recruited and determined to be eligible, the participant will be randomized to one of two groups, stratified by sex. Prior to the randomization visit, project staff will contact the data manager who generates the treatment assignment. Confirmation of the treatment group assignment is then printed for the care manager containing the participant’s ID and group assignment. This algorithm tracks subject group assignment and ensures near-equal group sample size at all stages of randomization within each strata.
Study protocol
Individuals who are interested in the study will be asked to contact study staff via mail or telephone (PAD hotline). Individuals will be asked to undergo an initial telephone-screening questionnaire and those who meet inclusion criteria will be invited to a group or individual study information session. At this session, informed consent will be obtained by study staff in accordance with requirements of the Human Subjects Protection Committee, and ABI will be performed to determine eligibility (Figure 1).
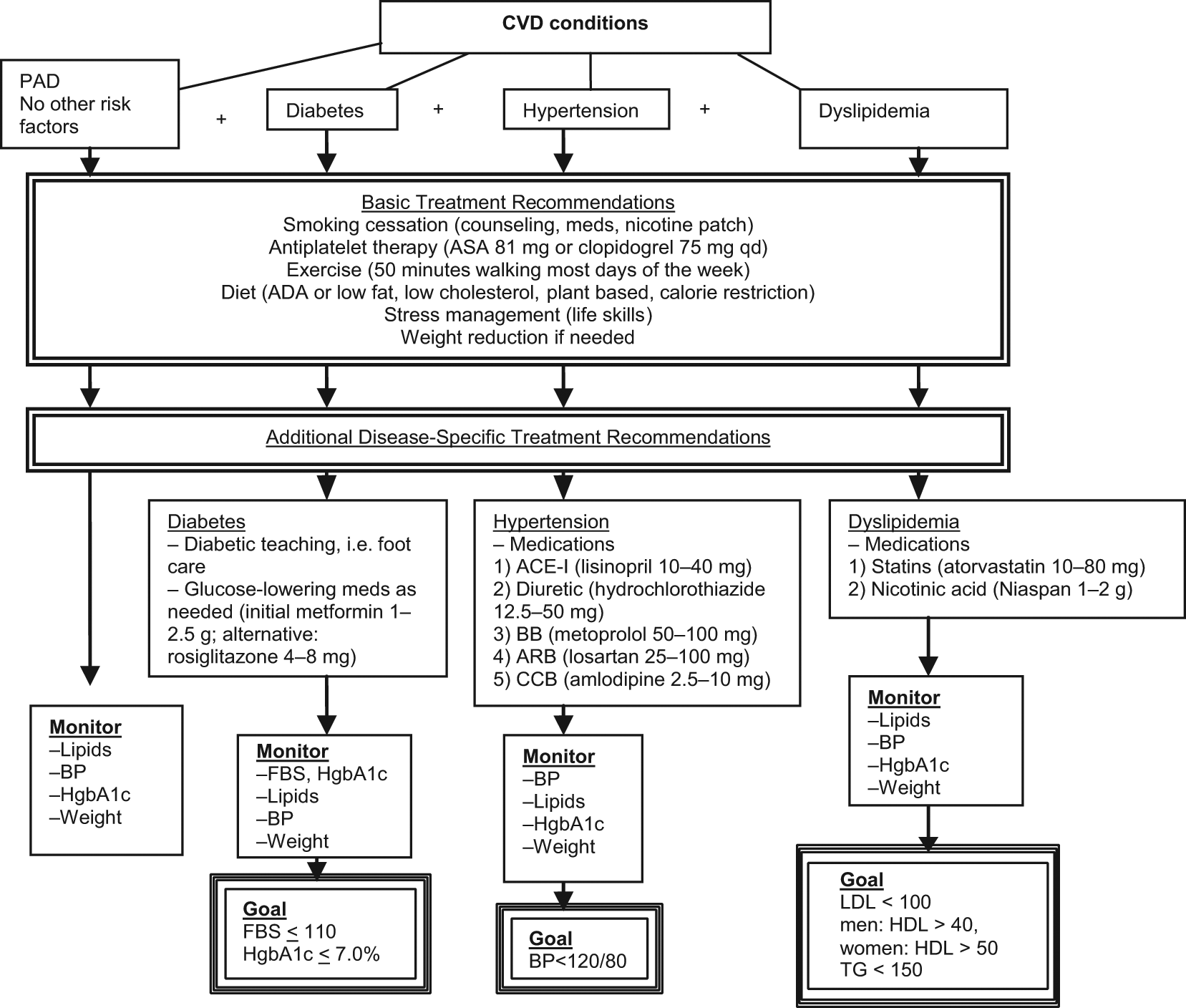
Algorithm for the management of CVD conditions and CV risk factors. All risk factors will be treated with lifestyle modification. The order of priority is smoking cessation, antiplatelet therapy, exercise, weight management, diet, and stress management. Depending on the individual’s CV risk factor profile, additional therapies will be implemented. These include diabetic teaching principles such as foot care and glucose lowering medications for diabetics. For hypertensive patients, blood pressure lowering medications will be prescribed. Dyslipidemia will be treated with lipid lowering medications such as statins. Monitoring will consist of laboratory analysis of risk factors as well as logs to assess weight, and BP measurement. Successful management will be determined by attainment of guideline goals. Interventions will be modified based on attainment of guideline goals. In the case of multiple comorbid conditions, recommendations and goals will be combined. (ACE-I, angiotensin-converting enzyme inhibitor; ADA, American Diabetes Association; ARB, angiotensin receptor blocker; ASA, aspirin; BB, beta-blocker; BP, blood pressure; CCB, calcium channel blockers; FBS, fasting blood sugar; LDL, low-density lipoprotein; HDL, high-density lipoprotein; TG, triglyceride.)
Eligible subjects will then be scheduled for a baseline evaluation at the General Clinical Research Center (GCRC) at UCSF or the Cardiology Clinic at Mt Zion Hospital to undergo a medical history and physical examination, height and weight measurements, blood pressure evaluation, and repeat resting ABI. Individuals who are eligible will perform an exercise treadmill test to determine peak walking time (PWT) and also a 1-minute post-exercise ABI. Those individuals who continue to be eligible will then enter a 2–4-week run-in period that will be used to minimize differences in exercise test performance due to learning effects. In order to qualify for randomization, a difference of < 25% between two consecutive treadmill tests must be achieved by the participant. Two treadmill tests will be performed on two separate days at least 24 hours apart but no more than 2 weeks apart. A third or fourth test may be required to qualify based on treadmill criteria.
A maximum of 30 days will be allowed for the run-in period to account for missed and rescheduled appointments. Study participants will also have completed self-administered questionnaires during this time. After all baseline assessments are completed, participants will be randomized to one of two groups: care management intervention (Int) or enhanced standard care (ESC) for 24 months. Testing will be repeated at 12 months (study midpoint) and 24 months (at conclusion of the study intervention).
Design elements of the intervention program
Guideline-based program goals
The delivery of care by team managers will be guided by evidence-based guidelines/goals for management of CAD risk factors, including cholesterol, 47 hypertension, 48 physical activity, 49 diabetes mellitus, 50 obesity, 51 smoking cessation 52 and secondary CAD prevention (Table 1).
CVD risk reduction strategies for individuals with CVD and other vascular diseases
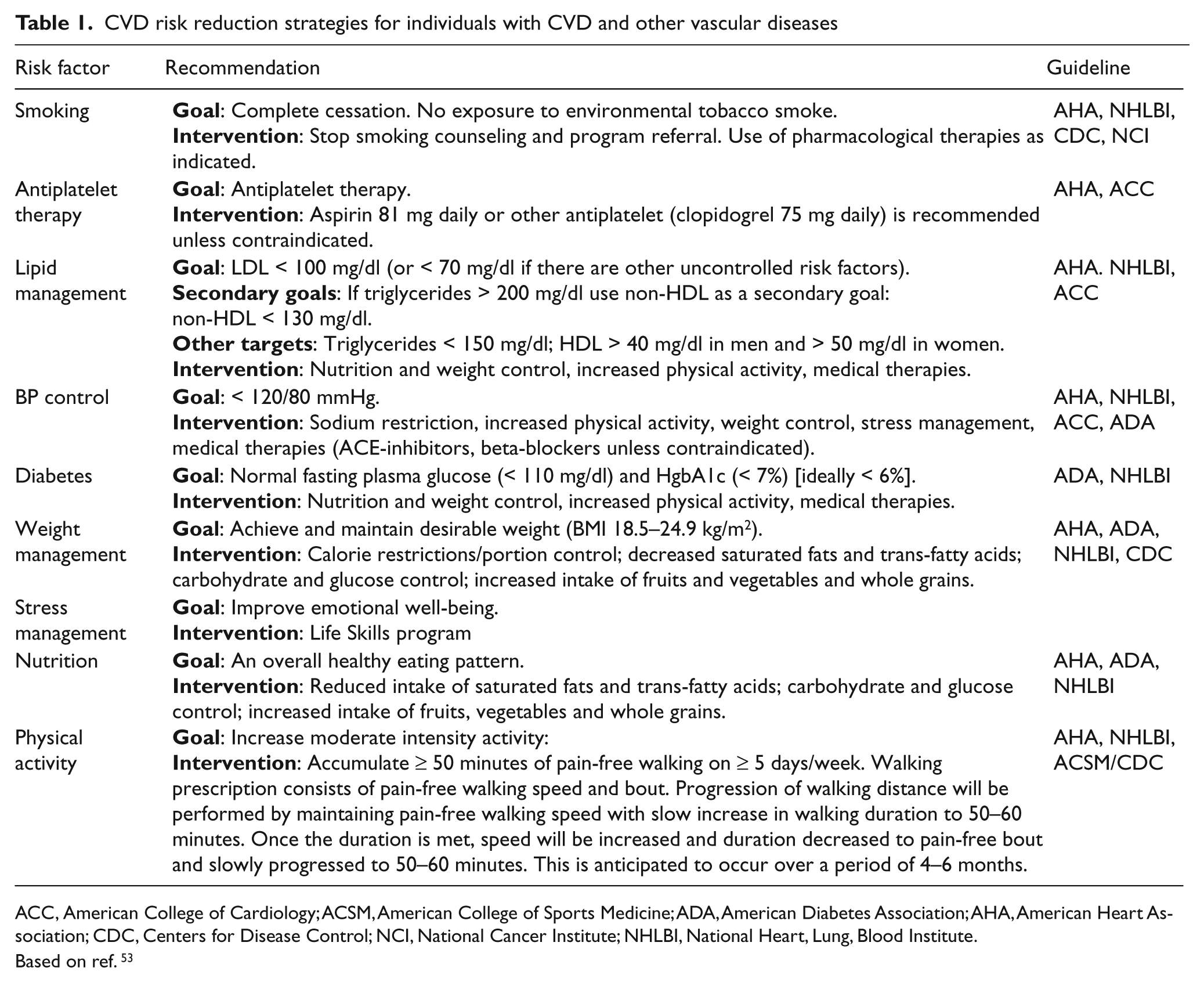
ACC, American College of Cardiology; ACSM, American College of Sports Medicine; ADA, American Diabetes Association; AHA, American Heart Association; CDC, Centers for Disease Control; NCI, National Cancer Institute; NHLBI, National Heart, Lung, Blood Institute.
Based on ref. 53
The cornerstone of the intervention is lifestyle modification (exercise and diet) as a partial, but critical, means of achieving CVD prevention goals. Home-based, patient-centered risk reduction is the core of the intervention. Subjects partnering with care managers will develop individualized, longitudinal strategies to achieve CVD risk factor reduction. The emphasis of intervention is long-term adherence to lifestyle modification and traditional medications. Medications, an important adjunct to lifestyle changes, will be provided by the participant’s PCP. Continuous monitoring of lifestyle change and adherence will be performed by care managers via telephone, email, and during clinic visits by review of adherence logs, pedometers and change in risk factor status. Behavioral interventions will be monitored and intensified as short-term goals are attained by study participants. In addition to counseling, participants will be referred to low-cost or free community services if deemed appropriate and consistent with study goals (i.e. smoking cessation programs, exercise classes, weight loss programs, nutrition education, etc).
Behavioral intervention
The skills required for adopting and maintaining lifestyle changes will be supported by the use of behavioral strategies that have been shown to be effective in CVD risk factor modification in a number of clinical settings.22,25–29 Fundamental principles of the intervention include individualized, tailored feedback based on cardiac risk assessment, goal-setting, self-monitoring, developing action plans, social support and rewards. At baseline, all subjects will be given a comprehensive cardiac risk assessment summarizing their individual CVD risk factors (including lipid profile, blood pressure, glycosylated hemoglobin levels, current medication regimen) compared with national guideline recommendations. These results will provide the basis for a dialogue between care managers and study participants on strategies to optimize treatment and lower risk factors. In the case of multiple risk factors, priorities for treatment will be identified by the care manager and discussed with the participant. The priorities will be based on importance for overall risk and the subject’s ability, interest and willingness to work on reducing the risk factor. In the case where medication management is inadequate, the care management team member will contact the PCP to recommend medication changes (in accord with national guidelines and recent evidence) to improve CVD risk factors. During this intensive discussion, short and long-term goals will be established and a realistic action plan will be developed by the care manager and the participant. The care manager will carefully craft goals so that they are small and achievable in a 1–2-week timeframe with actions that are very specific. The goal is to achieve success in a short period of time to improve the individual’s self-efficacy or confidence levels. If a participant’s goals are not behavioral in nature, too broad, long term or not achievable, further discussion will ensue to identify a more appropriate goal. An example of a general goal is lowering low-density lipoprotein (LDL) levels. In this instance, the care manager will discuss specific behaviors that will likely contribute to lowering LDL (i.e. walking) and set appropriate actions and goals for a 1–2-week period. The level of specificity for action plans will include time of day, days per week and route for the planned walk, including places to stop and the support of family or friends if appropriate. Other discussion items will include preparation for walking (i.e. type of shoes, safety issues and symptom awareness). Once goals are identified and an action plan is established, the individual will be asked to rank the level of confidence in their ability to accomplish this goal. If the score is low, the care manager will discuss barriers and strategies that would improve the individual’s confidence in being able to perform the behaviors as stated in the plan. If needed, goals and actions will be revised accordingly. Action plans will focus on one or two attainable goals. Importantly, as goals are accomplished (in 1–2-week intervals), new goals will be set with appropriate action plans to ensure that the participant is continuously working toward achieving longer-term risk reduction goals. To maximize participant commitment to the intervention, care manager–subject action plans will represent a concise summary of mutually agreed-upon goals and actions. Because of the emphasis on behavior change and progression during the first year of the intervention, frequent contact is anticipated between the individual and care managers via telephone and face-to-face channels.
Initial counseling visit
The initial in-depth care management visit will occur within 1–15 days after randomization. The visit is described in detail above. Subjects in the ESC group will receive appropriate educational materials with a follow-up contact within 3 months.
Medical risk factor management and monitoring care
The care manager under the supervision of the investigator and in collaboration with the subject’s PCP will be responsible for management and for monitoring the clinical and behavioral records of subjects in the intervention group. Healthcare providers will be contacted after each visit and provided with any relevant new clinical information obtained during the visit with recommendations (if appropriate) for optimizing medication management. This information will also be provided to participants with instructions for the patient to follow-up with their PCP if needed.
Strategies or tools to promote adherence to the intervention
Care managers will also have a ‘toolbox’ containing a variety of ‘tools’ to use in the event of relapse (i.e. weight gain, smoking relapse, discontinuation of exercise or consumption of a high-fat or high-calorie diet). The ‘toolbox’ concept was developed in the Diabetes Prevention Program Trial and was highly successful in achieving behavior change to diet and exercise in diabetic patients. 54 The ‘toolbox’ will contain strategies or ‘tools’ for promoting adherence to the intervention, and will be grouped into two types: reinforcers (tools that support adherence or success) or roblem-solving tools (used to identify alternative strategies or work to resolve barriers). 40 Tools will be used as a preventative strategy, with initial signs of problems or after long periods of lapse. Strategies may not be specific to one behavior and may be used for multiple behaviors if appropriate. Problem-solving tools include those that are specific to a problem (i.e. attendance at clinic visits, self-monitoring of diet, exercise, medications or weight). The care manager will decide which strategies in the toolbox are appropriate and the duration of implementation. Tools will be tailored to the individual so that reinforcers and problem-solving tools address specific individual barriers. Cost and time will be considered when selecting a tool, beginning with the least expensive and progressing to more intensive, expensive tools. The underlying principles for the toolbox include the following. (1) Creativity and responsiveness to the unique needs of the participants to increase adherence; (2) adherence to the intervention is important, but retention in the study is foremost 55 (the goal is 100% adherence but is translated as participants doing as much as they possibly can while remaining in the study); and (3) rewards will be individualized and structured to reinforce steps and to maintain long-term adherence. The process for monitoring and supporting adherence will be refined throughout the trial.
Examples of ‘tools’ for maintaining walking include: DVDs or videos for seniors; books on exercise and increasing physical activity; diaries; music CDs; walking distance competitions; and involving the participant’s significant other, family member or friend in walking. The ‘tools’ for maintaining diet goals include: specific meal plans tailored to the individual’s taste/preferences/lifestyle; dietary self-monitoring; purchasing cook books or food scales; cooking classes; and food shopping trips with the case manager to learn appropriate food choices, food substitutions and how to read food labels.
Other strategies to maximize adherence include regularly scheduled telephone calls (progressing from weekly to biweekly, monthly and bimonthly) and scheduled visits. The frequency of contact will be gradually decreased if it does not adversely affect maintenance. Intervention subjects will be asked to keep daily diet and exercise logs for the first 3 months after randomization, then for 2 weeks every 6 months. Pedometers will be used to provide motivational feedback to increase walking distance and as a means to track adherence. Dietary adherence will be assessed by the food frequency questionnaire and random 3-day food diaries. Newsletters and educational materials, recipes, and birthday cards will be regularly sent to retain interest and participation in the study.
Enhanced standard of care group
Subjects in the ESC group will meet with the care manager at baseline, 12 months, and 24 months for 30–45 minutes to discuss the individual’s risk factor profile and recommendations for lifestyle modifications and to set preliminary goals and develop action plans. These subjects will receive standard patient education brochures developed by the American Heart Association (AHA), American Diabetes Association (ADA), National Heart, Lung, and Blood Institute (NHLBI) on diet, exercise, weight loss, smoking cessation and stress reduction. Study participants will be instructed to continue to receive their health care, including CVD risk factor reduction, from their existing medical providers, consisting of a PCP and medical specialists when indicated. The care for these patients is considered ‘enhanced’ since both the patients and their physicians will be provided with (a) relevant study laboratory tests (BP, lipids, hemoglobin A1c, fasting blood sugar, treadmill test results and ABI) following the baseline, 12-month, and 24-month evaluation visits; and (b) recommendations for clinical management to meet current guideline goals. Guidelines will include the NCEP Adult Treatment Panel III, 55 Joint National Committee (JNC) VII on the treatment of hypertension 48 and the ADA guidelines for the treatment of diabetes. 50 Implementation of these guidelines on a patient-by-patient basis will be left to the discretion of the PCP. Subjects will also receive minimal telephone contact (approximately every 3 months) by project staff to update contact information, monitor the occurrence of medical events and maintain interest and participation in the study. Subjects will also be invited to participate in educational group sessions three times per year, presented by care managers on general health topics such as a healthy diet, exercise, diabetes, and weight management. ESC will consist of a combination of limited care management contact, telephone calls and group sessions as an adjunct to routine care from their PCP. Our goal is to ensure that the patients assigned to ESC have an opportunity to receive the best possible care using the existing healthcare delivery system. 56
Monitoring fidelity of intervention
The treatment fidelity plan for this study will be based on the comprehensive model described by the behavioral change consortium.57–59 Five areas of monitoring will include: (1) study design; (2) training providers; (3) delivery of treatment; (4) receipt of treatment; and (5) enactment of treatment skills. 60
Adverse events
Adverse events will be regularly assessed at each visit and during telephone contacts. All events whether elicited by the study staff or reported by the subject at clinic visits or via telephone contact will be recorded. Additionally, all participants will be asked to contact study staff in the case of hospitalization, emergency room visits or any unexpected medical event.
Measurement (Table 2)
Primary and secondary outcomes will be assessed at baseline, 12 months, and 24 months. All biological tests will be performed in the morning and performance testing will be scheduled at the same time of day for baseline, 12 months, and 24 months to control for circadian variation.61,62 The primary study outcome is walking time as measured by PWT during exercise treadmill test and self-reported walking impairment. Quality of life as measured by SF-36 is the secondary outcome of interest. Process variables will be measured every 3 months in the intervention group and include lipid levels for individuals who are hyperlipidemic, blood pressure for hypertensive participants, hemoglobin A1c for diabetics, weight for overweight and obese individuals, and smoking cessation for current smokers. These interim CVD risk markers will provide feedback to study participants, their clinicians, and the study team. These measures will be used to assess and monitor progress toward attainment of lowering risk factors.
Study procedures
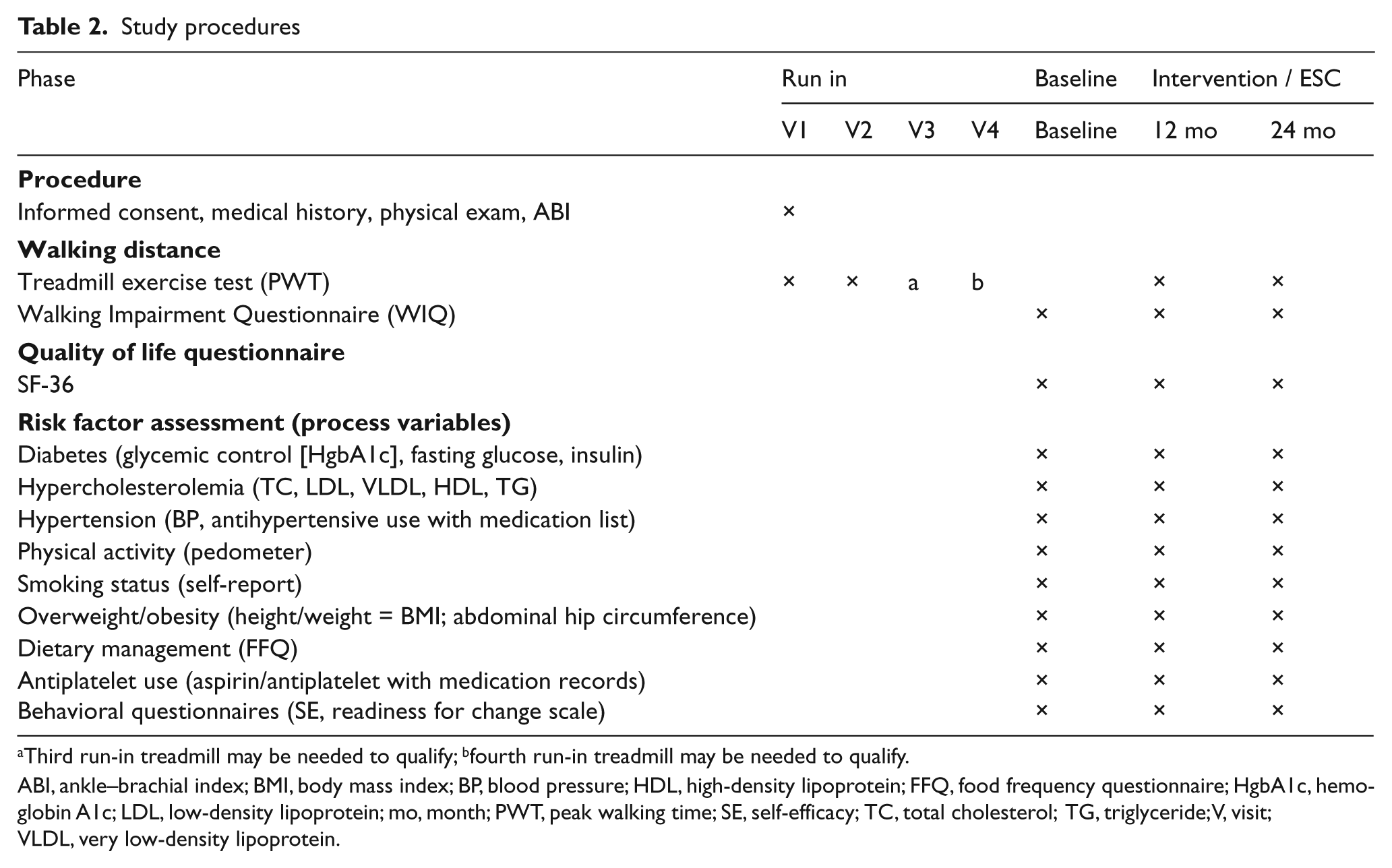
Third run-in treadmill may be needed to qualify; bfourth run-in treadmill may be needed to qualify.
ABI, ankle–brachial index; BMI, body mass index; BP, blood pressure; HDL, high-density lipoprotein; FFQ, food frequency questionnaire; HgbA1c, hemoglobin A1c; LDL, low-density lipoprotein; mo, month; PWT, peak walking time; SE, self-efficacy; TC, total cholesterol; TG, triglyceride; V, visit; VLDL, very low-density lipoprotein.
Statistical analysis
All variables will be summarized by appropriate descriptive statistics at each time point. The intervention group will be compared to the ESC group for homogeneity on demographic and baseline clinical variables via the chi-squared test or Student’s t-test (depending on the type of variable). Through stratified randomization, these variables are anticipated to be comparable in both groups. Data analyses are planned to compare those who did and did not drop from the study to determine if there was a differential bias. All analyses will be based on intention to treat (all participants randomized will be analyzed based upon their assigned group). The significance level will be preset at 0.05 and two-tailed tests will be performed.
To analyze both 12 and 24-month data, we will first consider the repeated measures analysis of variance (ANOVA) approach. To address dropouts, we will use the mixed models for longitudinal outcomes approach which provide unbiased estimates of the effects of covariates for data that are randomly missing. 66 Specifically, we will employ well-established methods such as the general linear mixed-effects models 67 and the generalized estimating equations (GEE) approach for marginal models. We will use a mixed model approach, accounting for within-subject correlation to model PWT, WIQ and quality of life, to compare their improvements over time between the two intervention groups, and to identify predictors of the outcomes. Random intercepts and slopes will be used to model the subject-specific improvement in the outcome measures and to accommodate the correlation structure.
Discussion
Summary
PAD is a systemic manifestation of atherosclerosis that is most prevalent in elderly people and those with CVD risk factors, including hypercholesterolemia, hypertension, obesity, diabetes and physical inactivity. Patients with PAD often report walking impairment due to symptoms of limb ischemia resulting in poor quality of life. Current national guidelines recommend intensive CVD risk factor management for PAD patients, including lifestyle modification and medications. Our study will examine the impact of a 24-month, patient-centered, behavioral, multiple CVD risk reduction program targeting exercise and diet on walking and quality of life in elderly patients with PAD.
Significance of the study and contribution to knowledge development
This study will be one of the first to examine the efficacy of a long-term, patient-centered, behavioral intervention to improve walking in elderly PAD patients. The foundation of the behavioral intervention is lifestyle modification; specifically, exercise and diet as the cornerstone of risk reduction. In addition, project staff will work with the participant’s primary care or specialty practice provider to optimize the medical treatment of chronic disease conditions in accordance with national guidelines, including diabetes, hypertension, and hypercholesterolemia.
One of the unique aspects of our study is the implementation of a patient-centered approach to focus and prioritize the treatment of multiple CVD risk factors and maximize adherence to our study program. While patient-centered interventions have demonstrated efficacy in patients with diabetes and more recently in improving hypercholesterolemia in PAD patients, 68 our study will be one of the first that we are aware of, that is patient-centered, includes long-term follow-up, and manages multiple CVD risk factors in elderly patients with PAD.68–70
In a recent study, McDermott et al. (2011) 68 reported that a telephone counseling intervention successfully increased patient activation as demonstrated by a patient’s ability to request more intensive lipid-lowering treatment. This resulted in markedly lower LDL levels in the activated group. Our study, in contrast to McDermott et al., will be longer in duration, 24 months versus 12 months, includes a variety of approaches to risk factor reduction such as face-to-face counseling, telephone calls and email, and monitoring and management of other CVD risk factors including hypertension, diabetes, smoking cessation and weight management. Our study is also unique in incorporating the principle of collaboration and partnership, including shared decision-making with study participants. Study staff and participants will work together on developing plans for care, including the use of short and long-term goals and action items and incorporating behavioral strategies to achieve progress. While both studies include process biological markers, our study will incorporate modification of goals and action items to tackle other CVD risk factors as appropriate.
The duration of our study will also allow care managers to successively intervene on multiple CVD risk factors in this patient population. For example, initially the highest priority for one study participant may be to lower glucose levels by improving medication adherence. Other less urgent but equally important concerns for this patient may include management of hypertension, hypercholesterolemia and obesity, all of which will be addressed over the study period.
The significance of using a patient-centered approach is the collaborative environment created between the study staff and participants as clinical problems and solutions are discussed and prioritized. It considers the participant’s state of readiness for change and self-efficacy for making those changes. Our approach will also be based on communication between the study participant and the staff in identifying barriers and practicing strategies to ensure successful behavior change. Problem-solving techniques will be supported and shared. The study staff will provide guidance in setting realistic and achievable goals that are modified according to whether goals are met.
Participants will learn new self-management skills and strategies as well as communication skills. The study staff will facilitate the exchange of information with the participant’s healthcare provider. Prior to a clinic visit, study participants will be coached on questions to ask their providers regarding medication changes, information about laboratory tests, referrals, and consultations. We hypothesize that close follow-up with study staff will encourage study participants to be more actively involved in their care and ultimately reduce CVD risk factors.
Our approach differs from the usual risk factor management and case management approach because it requires active engagement by the participant. The study intervention will be tailored to the needs and interests of the participant while considering priorities for the study. While this approach is unique, it has several limitations. The first is the time required to train providers in the skills needed to deliver a patient-centered behavioral intervention. Motivational interviewing skills require additional training and practice as well as a shift in the normal approach to clinical care and patient interactions. Second, individuals who are unfamiliar with the patient-centered model of care may be reluctant to actively engage in decision-making and self-management, requiring additional coaching and staff time. Finally, the clinical interactions in our study may require a longer period of time than might be allotted during a usual office visit and currently may not be reimbursed by third party payers, limiting portability of the intervention into clinical settings. We hypothesize that the increased interactions between study staff and participants will contribute significantly to improvement in CVD risk factors and change in lifestyle required to increase walking performance. To address this concern, the study intervention was delivered by a multidisciplinary team (nurse, exercise physiologist, registered dietician) who in a team or teamlet model patient care environment may be able to implement the proposed intervention.
Another important aspect of this study is the interaction between study staff and the participant’s primary care providers and specialists. All test results will be provided to the participant’s primary care providers and specialists. The longitudinal nature of the study and the many diagnostic tests that will be performed for monitoring risk factor reduction (i.e. lipid panels, 71 inflammatory markers, exercise tests, and ABIs) lend themselves to repeated interactions, follow-up, and opportunities to reinforce the importance of aggressive treatment and options to reduce CVD risk factors. These interactions may lead to increased awareness of PAD management and more active medical and surgical intervention in our study population. We anticipate that the intervention group will receive more attention by their providers since clinical data will be sent to providers and follow-up will be provided to the intervention group.
The cornerstone of the study intervention is optimal medication management and lifestyle modification; specifically, a home-based supervised walking program and a healthy diet. At the time the study was funded, there was little evidence that home-based walking would improve walking ability. Most evidence pointed to supervised exercise programs such as cardiac rehabilitation programs. A recent study has shown that home-based walking was as effective as supervised exercise in patients with intermittent claudication. 72 Our trial will provide further evidence for supervised home-based walking in conjunction with other CVD risk reduction strategies to improve walking time in patients with PAD. It is possible that behavioral factors such as improving depression, enhanced self-efficacy for walking, social support and increased self-management skills will contribute to increased walking ability and quality of life. Although not measured in this study, adherence to a walking program may also improve muscle strength and balance. With increased walking ability, quality of life is enhanced in this patient population.
Additional limitations of study/design/methods
In addition to the constraints attributed to the intervention described above, other limitations include the use of pedometers and self-report for walking and 3-day diet recall for dietary adherence. Previous studies suggest that exercise self-report tends to over-estimate activity and underestimate dietary intake.73–77 Additionally, medication adherence is self-reported as is dosage of medications. Every attempt will be made to verify prescribed medications by having study participants bring in their medication bottles at clinic visits and obtaining medical health records. Other limitations include the use of exercise treadmill testing to assess walking impairment. PWT is a subjective endpoint and although standardized instructions and encouragement will be provided for all study participants, PWT is influenced by an individual’s level of effort and can also be influenced by pain tolerance. Our study is also limited to those who are English speaking or have a reasonable command of the English language.
Conclusion
This study will be an important first step in examining the efficacy of patient-centered, behavior change strategies targeting multiple CVD risk factors; specifically, exercise and dietary habits as a means to improve walking ability and quality of life in elderly PAD patients.
Footnotes
Acknowledgements
The investigators wish to thank all the individuals and their families who participated in this study. We would also like to thank the staff of the UCSF Moffitt and Mt Zion CTSI centers and the staff of the Mt Zion Cardiology Laboratory.
This publication was made possible by grant numbers 5RO1NR9197, 3RO1NR009197-04S1, 3RO1NR009197-04S2, and 3RO1NR009 197-04S3 from September 2005 to 31 March 2011; the UCSF School of Nursing Intramural Fund; a UCSF Academic Senate Grant; and a Society of Vascular Nursing Research Grant.
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.