
Abstract
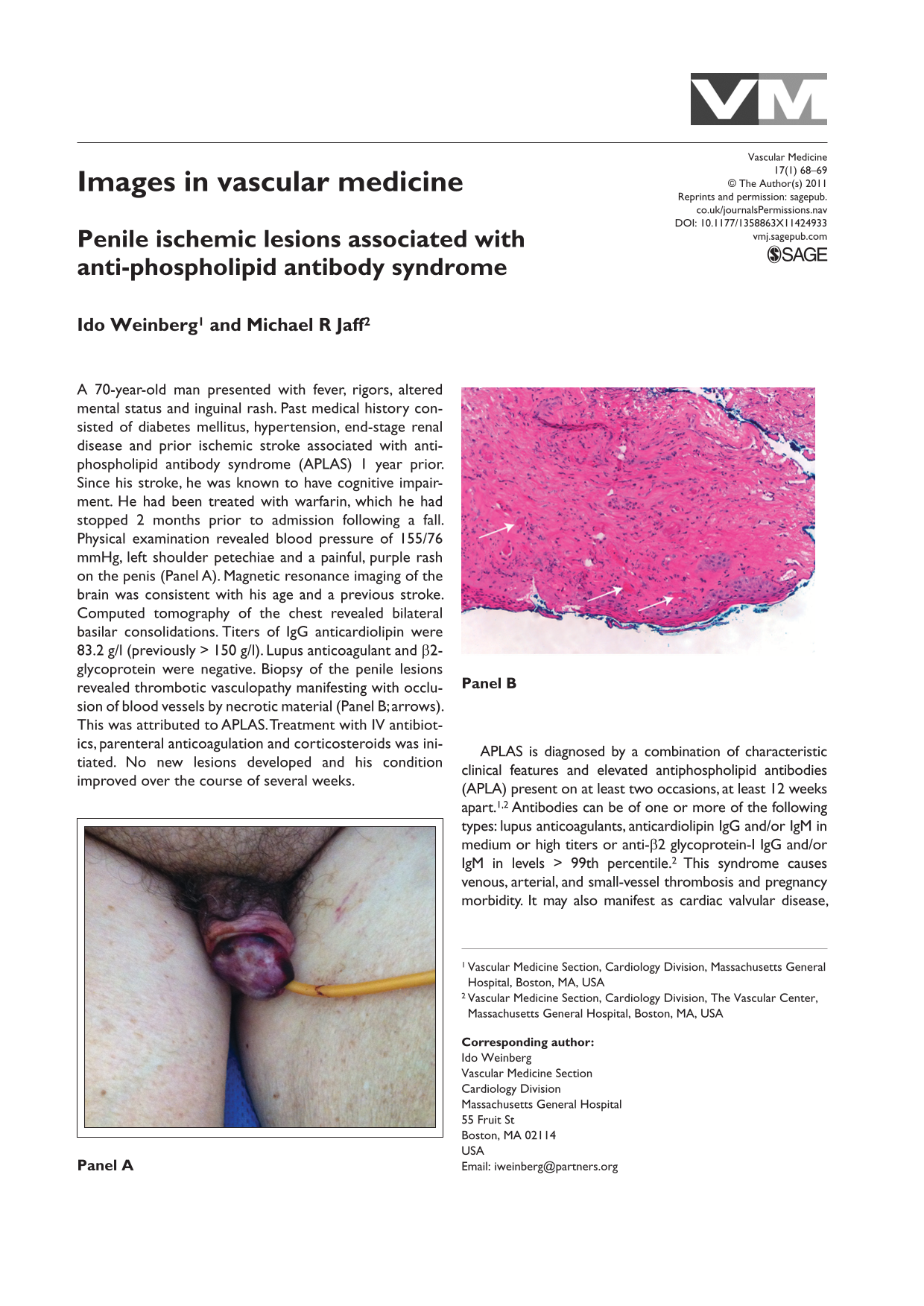
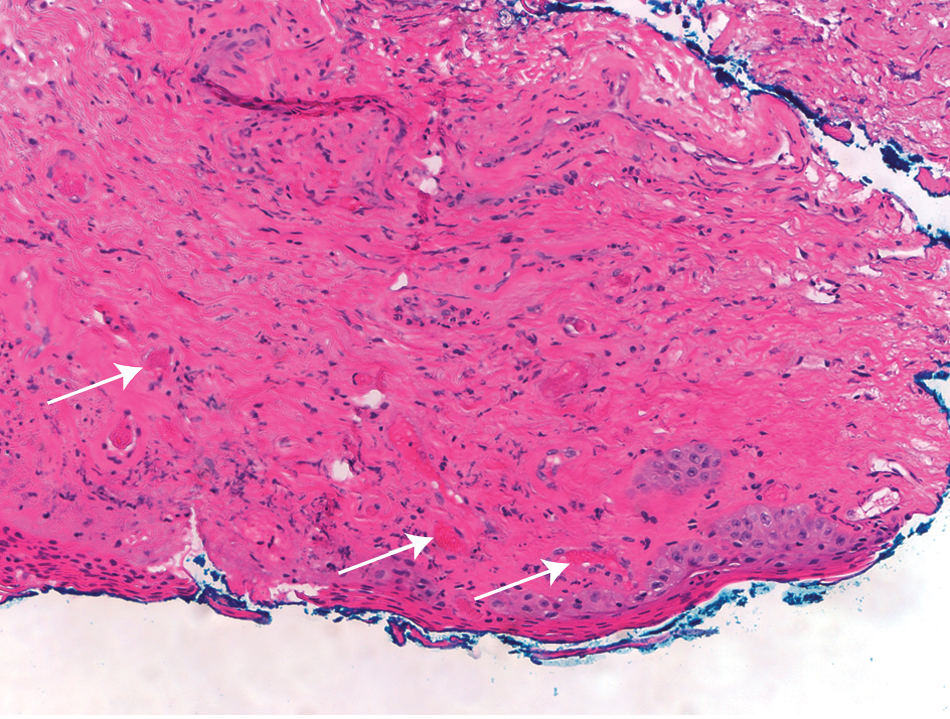
A 70-year-old man presented with fever, rigors, altered mental status and inguinal rash. Past medical history consisted of diabetes mellitus, hypertension, end-stage renal disease and prior ischemic stroke associated with anti-phospholipid antibody syndrome (APLAS) 1 year prior. Since his stroke, he was known to have cognitive impairment. He had been treated with warfarin, which he had stopped 2 months prior to admission following a fall. Physical examination revealed blood pressure of 155/76 mmHg, left shoulder petechiae and a painful, purple rash on the penis (Panel A). Magnetic resonance imaging of the brain was consistent with his age and a previous stroke. Computed tomography of the chest revealed bilateral basilar consolidations. Titers of IgG anticardiolipin were 83.2 g/l (previously > 150 g/l). Lupus anticoagulant and β2-glycoprotein were negative. Biopsy of the penile lesions revealed thrombotic vasculopathy manifesting with occlusion of blood vessels by necrotic material (Panel B; arrows). This was attributed to APLAS. Treatment with IV antibiotics, parenteral anticoagulation and corticosteroids was initiated. No new lesions developed and his condition improved over the course of several weeks.

APLAS is diagnosed by a combination of characteristic clinical features and elevated antiphospholipid antibodies (APLA) present on at least two occasions, at least 12 weeks apart.1,2 Antibodies can be of one or more of the following types: lupus anticoagulants, anticardiolipin IgG and/or IgM in medium or high titers or anti-β2 glycoprotein-I IgG and/or IgM in levels > 99th percentile. 2 This syndrome causes venous, arterial, and small-vessel thrombosis and pregnancy morbidity. It may also manifest as cardiac valvular disease, renal thrombotic microangiopathy, hemolytic anemia, thrombocytopenia, and cognitive impairment. 3 Cutaneous manifestations of APLAS include livedo reticularis, skin ulcerations and rarely widespread cutaneous necrosis. 4 While penile ischemia with full recovery has been described in patients with APLAS, 5 this is a rare complication. It should be identified promptly as it can offer a diagnostic clue to the syndrome and direct treatment.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Mark A Creager, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Dr. Weinberg has no conflicts of interests to declare. Dr. Jaff is a Member, Board of Trustees, VIVA Physicians, Inc, a 501(c) 3 not for profit physician education and research organization.