
Abstract
Renal artery stenosis (RAS) is an important cause of renal failure; however, the factors associated with loss of kidney function in patients with RAS are poorly described, as are the predictors of an improvement in kidney function after stenting. One hundred patients at seven centers undergoing renal stenting were randomly assigned to an embolic protection device or double-blind use of a platelet glycoprotein IIb/IIIa inhibitor. The glomerular filtration rate (GFR) was measured using the creatinine-derived modified Modification of Diet in Renal Disease (MDRD) equation, cystatin C, and iohexol clearance. In univariate and multivariate models, baseline MDRD and cystatin C GFR were associated with congestive heart failure (CHF) (p = 0.01), lesion length (p = 0.01), and percent stenosis (–0.27, p = 0.01). In multivariate models, MDRD-estimated GFR 1 month after stenting was associated with bilateral stenosis (p < 0.05) and lesion length (p < 0.05), whereas with cystatin C the multivariate model included angiotensin receptor blocker (ARB) (p < 0.05) and minimal luminal diameter (MLD) (p < 0.05). The improvement in GFR from baseline to 1 month, measured as percent change, was related to baseline MDRD (p = 0.009) and cystatin C (p = 0.03) GFR. For MDRD GFR combined treatment with abciximab and Angioguard® embolic protection (p = 0.02) remained significant in multivariate analysis as did CHF, which was also significant with cystatin C (p = 0.05). In conclusion, CHF and lesion characteristics (MLD, percent stenosis and lesion length) are determinants of renal function in patients with RAS. In contrast, the acute improvement in renal function after revascularization is most strongly influenced by baseline GFR, and to a lesser degree CHF and combined procedural treatment with abciximab and embolic protection but not lesion characteristics.
Introduction
The role of renal artery stenosis (RAS) in the genesis of renal dysfunction is controversial. A number of investigators have evaluated the basic mechanisms that may be involved in ischemic injury to the kidney. Gobe et al. described that a combination of necrosis and apoptosis are important in the loss of renal function during and after an ischemic insult. 1 In the clinical arena, the relationship between stenosis severity and loss of kidney function are less clear. Over 1–4 years atherosclerotic stenoses may progress anatomically; however, progression to occlusion is infrequent.2–5 In some patients, RAS is associated with loss of renal size, a crude measure of renal function. 5 In the setting of a significant RAS (60–99%), up to a quarter of kidneys demonstrate atrophy of > 1 cm in length,6,7 whereas loss of renal size is uncommon without RAS. 7
However, several investigators have been unable to demonstrate a relationship between stenosis severity and renal function.8–10 For some time there has been debate about the role of factors such as the severity of the stenosis, presence of diabetes and other factors that lead to loss of kidney function in patients with atherosclerotic RAS. Wright et al. described an apparent lack of relationship between the severity of RAS and the likelihood of recovery of renal function after intervention. 9 Similarly, the recently completed ASTRAL and STAR trials were unable to demonstrate an improvement in glomerular filtration rate (GFR) when stent treatment, a strategy that potentially relieves the kidney of the stenosis, was compared directly to medical therapy.11,12
It has been suggested that the failure of randomized trials to demonstrate an improvement in kidney function is explained by the enrollment of subjects who a priori were unlikely to benefit. 13 However, there is little data available that indicate the factor(s) responsible for the development of ischemic nephropathy or that predict a favorable outcome of stent revascularization. The purpose of the current analysis is to (1) describe the factor(s) that determine renal function before and after stent treatment, and (2) describe the factors that are predictive of an improvement in renal function after stenting.
Methods
The current study evaluated patients from the RESIST trial, a multi-center study of patients undergoing renal artery stenting that evaluated the utility of embolic protection and or abciximab (a platelet glycoprotein inhibitor) in a 2 × 2 randomization scheme. The methods of the RESIST trial have been described previously. 14 Briefly, the study (ClinicalTrials.gov identifier NCT00234585) was conducted by the Clinical Coordinating Center at the University of Toledo with funding provided by the sponsors, with study conduct, data analysis and reporting performed independently of the sponsors. ICH good clinical practice guidelines were followed, with patients providing informed consent in an IRB approved protocol. The major finding was an apparent benefit of abciximab on the post-procedural change in renal function, although the benefit appeared to be mostly attributable to patients randomly allocated to both abciximab and embolic protection.
One hundred randomized patients were recruited from seven sites. Inclusion required a history of hypertension, renal insufficiency, heart failure, or angina with poorly controlled hypertension and the presence of one or more renal artery stenoses, ≥ 50% and < 100%, treatable with the Angioguard® Short Tip (Cordis, Miami Lakes, FL, USA) embolic protection device (EPD). Exclusion criterion included age < 18, pregnancy, life expectancy ≤ 6 months, dialysis, history of kidney transplant, stenosis not amenable to stent, allergy to study agents, unrelated renal disease, untreated aortic aneurysm, kidney size < 8 cm, restenosis, vessel dimensions out of range for study devices, treatment of a side branch or distal stenosis, active bleeding, stroke within 2 years or with a residual neurologic deficit, INR > 1.2 times control, thrombocytopenia, major surgery or trauma within past 6 weeks, intracranial neoplasm, arteriovenous malformation or aneurysm, vasculitis, or a non-study procedure within 24 hours.
The use of pre-procedure hydration, with saline, sodium bicarbonate (n = 1) and/or acetylcysteine (n = 8) to prevent contrast-induced nephropathy, was at the discretion of each investigator. Prior to double-blinded administration of abciximab or placebo, systolic blood pressure was lowered to < 160 mmHg. The target activated clotting time (ACT) was 275 seconds, and if randomized to the EPD device an ACT of > 300 seconds was required. A bolus of 0.25 mg/kg abciximab (or placebo) was administered 5 minutes prior to crossing the lesion, followed by an infusion at 0.125 µg/kg/min (maximum 10 µg/min) for 12 hours. If necessary, pre-dilatation was permitted to facilitate delivery of the Angioguard Short Tip EPD. After positioning the EPD, pre-dilatation of the stenosis was performed prior to treatment with a Genesis™ stent (Cordis). The goal of stenting was to achieve 1:1 sizing of the treated lesion compared with a normal appearing distal segment.
All angiograms were analyzed at the University of Toledo Angiographic Core Lab, with staff blinded to study group or outcome. Angiograms were independently analyzed with lesion length, minimal luminal diameter (MLD), reference diameter and percent stenosis (%S) measured.
The CV Path core lab (Gaithersburg, MD, USA) performed the blinded analysis of EPD contents. Qualitative analysis of filter contents was also performed. The GFR was calculated using the modified Modification of Diet in Renal Disease (MDRD) equation. Creatinine was measured by a modified Jaffe reaction using the isotope dilution mass spectrometry–traceable assay at the University of Minnesota Core Laboratory. Cystatin C is determined nephelometrically in serum using the Dade Behring BN100, with an inter-assay laboratory CV of 4.7%. Lactate dehydrogense (LDH) is determined spectrophotometrically in serum using the Roche 911 Chemistry Analyzer with an inter-assay laboratory CV of 4.2%. Iohexol clearance was measured in plasma by ion-pair high-pressure liquid chromatography. Plasma is diluted to bring the concentration of iohexol into the range of the iohexol standards, then filtered by centrifugation through a microconcentrator to remove particulates and an aliquot of filtrate is injected onto the HPLC column. Iohexol in the sample is eluted via ion-pair reagent TBAP (ionate tetrabutylammonium phosphate) in sodium acetate buffer, with detection at 254 nm. A standard line of known iohexol concentration is constructed, against which the concentration of the unknown is read. Iohexol clearance is calculated by the formula: CL1 = dose/AUC, where AUC is the area under the plasma concentration curve. In a one-compartment model, the area under the curve is underestimated, making CL1 an overestimate of the true clearance value. The value is corrected according to Bröchner-Mortensen by the formula: GFR = (0.990778 × CL1) – (0.001218 × ). The GFR value is then normalized to body surface area.
Antihypertensive medications were continued during the evaluation of renal function except for diuretics, which were held that morning. Non-steroidal anti-inflammatory drugs (except aspirin), cimetidine, ranitidine, and trimethoprim were withheld for 7 days. Patients were instructed to drink 1 liter of water the day before and 500 ml of water on the morning of assessment.
Statistical analysis
Study data are presented as continuous (mean ± SD) and categorical data. Percent change was used as the primary analysis variable of GFR changes over time to approximate better a normal distribution of the study data. All analyses were performed in SAS. Univariate analyses of continuous data were compared with t-tests, ANOVA and Pearson’s correlation, and for categorical data the chi-square test. Multivariate models were created using the GLM (generalized linear model) program in SAS with application of stepwise model selection. Renal function at 1 month was defined as improved or declined. Probability plots were created using logistic regression for this categorical outcome at 1 month. Lesion characteristics from patients with multiple lesions are presented as the harmonic average; however, the analyses were repeated using the most severe lesion characteristics and the arithmetic averages.
Results
One hundred patients were included in the current analysis; complete data for MDRD GFR was available in 97 and 93 at baseline and follow-up, cystatin C in 97 and 93 at baseline and follow-up, and iohexol clearance in 70 at follow-up only. The MDRD and cystatin C methods for GFR determination were highly correlated (0.82, p < 0.0001). At 1 month the correlation between iohexol clearance with either MDRD or cystatin C were similar in strength (0.66 and 0.57 respectively, p < 0.0001 for both).
Baseline kidney function
By univariate analysis, baseline MDRD GFR was negatively associated with a high baseline LDH (–0.24, p = 0.02), presence of congestive heart failure (CHF) (p < 0.05), bilateral stenoses (p < 0.05), and percent stenosis (–0.27, p = 0.01), and was positively associated with lesion length (0.42, p < 0.0001) and MLD (0.34, p < 0.001) (Table 1). By multivariate analysis, CHF (p = 0.01), percent stenosis (p < 0.05) and lesion length remained significant (p = 0.0001) (Table 2). Baseline cystatin C-calculated GFR was associated with similar univariate factors, and the independent factors in a multivariate model included CHF (p = 0.01) and pre-treatment MLD (p = 0.0006).
Univariate factors with baseline MDRD estimated GFR in patients with renal artery stenosis

GFR, glomerular filtration rate; CC, correlation coefficient (for association with baseline MDRD GFR); BMI, body mass index; MDRD, modified diet in renal disease; LDL, low-density lipoprotein; HDL, high-density lipoprotein; DM, diabetes mellitus; CAD, coronary artery disease; CHF, congestive heart failure; HTN, hypertension; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker.
Multivariate predictors of baseline MDRD GFR in patients with renal artery stenosis
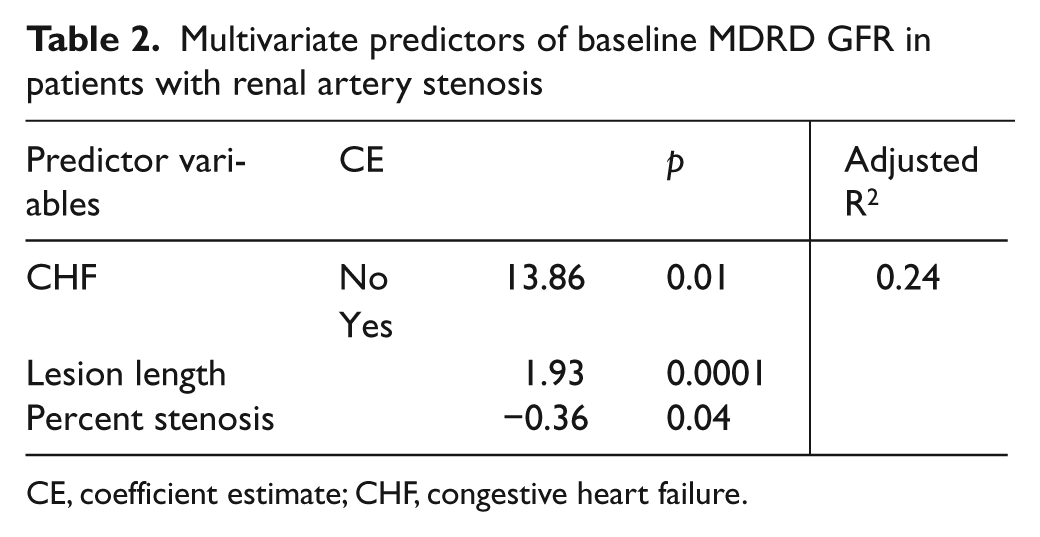
CE, coefficient estimate; CHF, congestive heart failure.
Kidney function 1 month after stenting
MDRD GFR 1 month after stenting was associated positively with ACE inhibitor use (p = 0.05), procedural contrast volume (0.27, p = 0.01), baseline lesion length (0.25, p < 0.05), baseline MLD (0.25, p < 0.05) and negatively with baseline presence of bilateral stenoses (p < 0.05). Cystatin C-calculated GFR 1 month after stenting was also positively associated with ACE inhibitor use (p < 0.05) and procedural contrast volume (0.24, p < 0.05). GFR measured by iohexol clearance 1 month after stenting was associated negatively with age (–0.29, p < 0.05) and baseline LDH (–0.23, p = 0.06), and positively with contrast volume (0.25, p = 0.05), baseline lesion length (0.24, p < 0.05), baseline reference diameter (0.28, p < 0.05), and baseline MLD (0.3, p = 0.01).
Multivariate analysis of 1-month MDRD GFR demonstrated that the presence of baseline bilateral stenoses (p < 0.05) and lesion length (p < 0.05) remained significant. Using 1-month cystatin C-estimated GFR, the significant independent factors in the multivariate model included angiotensin receptor blocker (ARB) use (p < 0.05) and baseline MLD (< 0.05). With 1-month iohexol GFR only, age (p = 0.07) and baseline MLD (p = 0.06) were close to significance in a multivariate model.
Change in kidney function after stenting
Univariate analysis of the percent change in GFR from baseline to 1 month, measured by MDRD estimate, was negatively related to baseline GFR (–0.32, p < 0.001), presence of diabetes (p < 0.05), and positively to combined use of abciximab and embolic protection (p = 0.01). The percent change in cystatin C-estimated GFR was related positively to smoking history (p < 0.05) and negatively to ARB use (p < 0.05) and baseline GFR (–0.25, p < 0.05).
Multivariate analysis of the change (%) in MDRD GFR suggested that combined treatment with abciximab and Angioguard embolic protection (p < 0.05) and baseline GFR (p = 0.009) remained significant in the model. The likelihood of a positive change (%) in MDRD GFR in relationship to baseline GFR and assignment to combined embolic protection and abciximab treatment are displayed in Figures 1 and 2. Multivariate analysis of the change (%) in cystatin C demonstrated that baseline GFR (p < 0.05), use of an ARB (p < 0.05) and baseline CHF (p = 0.05) were significant.
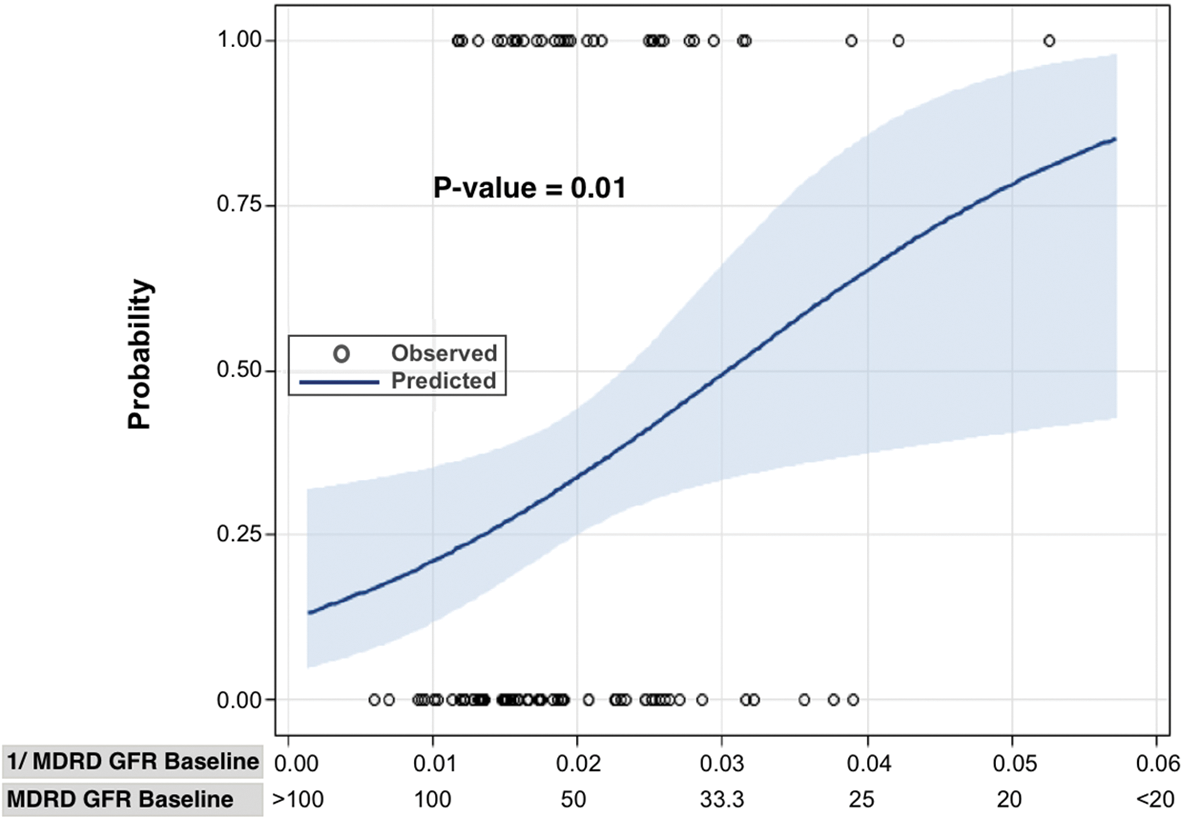
Probability plot displaying the likelihood of an improvement in change in GFR, calculated using the MDRD formula, from baseline to 1 month. The line indicates predicted probability and shading indicates 95% confidence intervals. (MDRD, medical diet in renal disease; GFR, glomerular filtration rate. The open circles at the top and bottom represent an occurrence of an improvement or lack of improvement in GFR for each study subject.)
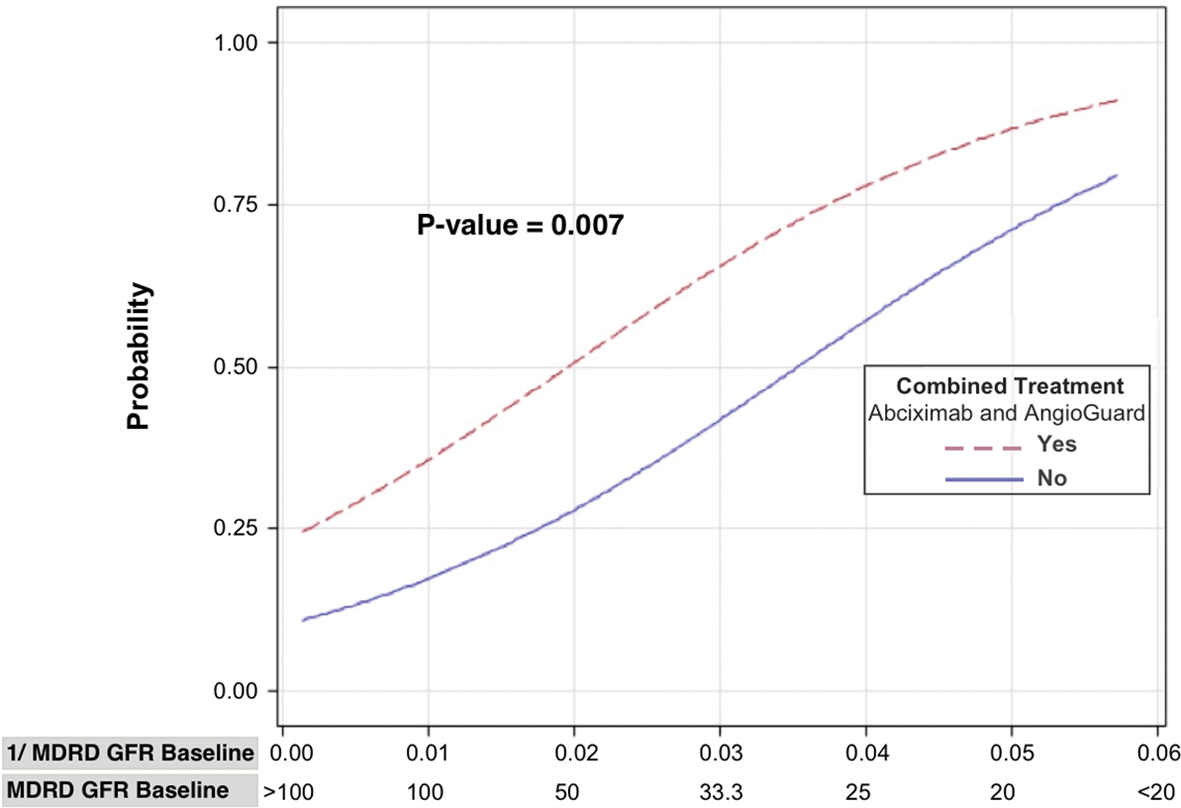
Probability plot displaying the likelihood of an improvement in change in GFR, calculated using the MDRD formula, from baseline to 1 month, categorized by treatment assignment. Combined treatment is randomly allocated assignment to both abciximab and Angioguard embolic protection device concurrently. ‘No’ indicates assignment to neither therapy, assignment to abciximab alone, or Angioguard alone. (MDRD, medical diet in renal disease; GFR, glomerular filtration rate. The open circles at the top and bottom represent an occurrence of an improvement or lack of improvement in GFR for each study subject.)
Discussion
A large body of experimental work has established that renal function may be lost as a consequence of stenoses occurring in an extraparenchymal renal artery, the syndrome of ischemic nephropathy. Stenoses may alter renal function hemodynamically by lowering glomerular pressure and filtration; biochemically through activation of inflammation, the renin-angiotensin system, and oxidative stress; or structurally by inducing cell death and fibrosis of the kidney.15–17
Several recent trials have failed to demonstrate a benefit of stent revascularization on renal function in patients with RAS.11,12 These studies had in common the idea that stenting would either improve renal function by improving renal blood flow in patients with ongoing ischemia, or prevent future declines in kidney function, presumably due to intermittent episodes of ischemia. Beyond a solid biologic basis, this idea was rational since prior authors such as Harden and Watson had demonstrated that stenting positively changed the rate of decline in kidney function in single-arm observational cohort series.18,19 In parallel, Hansen and colleagues have demonstrated the ability of surgical repair of ischemic nephropathy to improve kidney function in a substantial proportion, resulting in substantial dialysis-free survival in those who experience an improvement in renal function early after surgery. 20
On this background, the STAR and ASTRAL trials set out to test whether stenting could either prevent a 20% decline in creatinine clearance, or in the latter trial alter the slope of reciprocal creatinine that is a surrogate for GFR.11,12 Both trials were confounded by the inclusion of moderate numbers of subjects, presumably enrolled through non-invasive imaging studies, who were without a significant stenosis at the time of angiography. In this context, neither the STAR nor the ASTRAL trial was able to demonstrate an improvement in their pre-specified primary or secondary analyses of renal function. As a consequence, a reasonable conclusion of these trials is that stent revascularization does not improve renal function in patients with RAS.
However, a fundamental question that needs to be addressed is whether, in certain patient groups, it is a reasonable expectation that stenting should improve renal function. In specific, there are patients with resistant hypertension, but normal renal function, who undergo a stent procedure for blood pressure control not renal function. From a biologic perspective, it is entirely possible, or even plausible, that the severity of stenosis for inducing a blood pressure response 21 may be different than that required to injure or impair renal function. Unfortunately, little work has been done to understand what conditions predicate renal injury in patients with RAS, despite a substantive amount of animal work on the subject.
In the current study, we utilized a well-characterized group of patients with RAS who were enrolled in a prospective randomized trial 14 testing the utility of the Angioguard embolic protection device or abciximab, an inhibitor of the platelet glycoprotein IIb/IIIa receptor, to discern those factors that are predictive of renal function. We assessed renal function at two time periods and the difference between those. In addition, we were able to analyze renal function by several methods including a creatinine-based estimate of GFR using the MDRD formula, a cystatin C-based estimate, and finally iohexol clearance performed 1 month after the procedure.
From the current analysis several patterns emerged. Both prior to revascularization and 1 month after, a relationship was observed between stenosis severity (measured as MLD, percent stenosis, or bilateral stenoses) and GFR, irrespective of the method of GFR analysis, and this relationship persisted in the multivariate models. Of note, this finding stands somewhat in contrast to previous work that had suggested that stenosis severity, measured as a categorical variable, had no relationship to renal function.8–10 A difference with the current study was the use of a blinded core lab for the measurement of stenosis severity that may have allowed the precision necessary to discern this relationship. Admittedly, the relationship between stenosis severity and renal function was weak and explained a small minority of the differences in renal function observed within this heterogenous cohort of patients undergoing stenting.
While it may seem apparent that the relationship between ‘tight stenosis and worsened renal function’ implies ischemia-mediated injury, this may not necessarily be the circumstance. In the case of carotid artery stenoses, the severity of the lesion is predictive of stroke risk, primarily from an atheroembolic phenomenon, not occlusion per se. In a similar way, it is possible that more severe stenoses of the renal artery are either more likely to atheroembolize or embolize thrombotic material. On the latter note, a previous publication from this same cohort described a surprisingly high rate of capture of platelet-rich or fibrin-rich thrombi by the embolic protection system. 22 At this point it can only be concluded that stenosis severity does have some relationship with renal function in patients with RAS.
A limitation of the current study is the large number of baseline factors that were related to renal function that in turn was measured with several techniques, at two time points, and as a difference between time points. Given the large number of variables tested against several endpoints it should be expected that some factors may appear as significant simply because of chance association. Candidly, without confirmation in new cohorts, this concern should persist. Undoubtedly, some factors that were found to be statistically significant, especially those that were identified by only univariate analysis, with one method or at one time point, are chance associations. This has implications for treatment decisions that might be made based upon the current study. Having acknowledged this limitation, a reasonable algorithm to utilize to decide whether to revascularize a renal artery (if the goal is an improvement in GFR) would be to (1) identify if there is significant renal dysfunction, and (2) whether the patient is an appropriate candidate for treatment with embolic protection and a platelet glycoprotein IIb/IIIa inhibitor. If so, then based upon the current analyses, an improvement in GFR would be anticipated. However, such an approach should be viewed with some caution until this can be confirmed in future studies.
An additional limitation of the current work is that the pre-intervention hydration status and use of N-acetylcysteine was not strictly controlled in the study protocol, but was instead left to the discretion of the investigators. However, doubt has been raised about the clinical utility of acetylcysteine for the prevention of contrast nephropathy. 23
However, there were several relationships that were apparent across analytic methods or at certain time periods. In brief, at the baseline analysis, CHF was negatively related to GFR. MacDowall observed that in patients presenting with CHF the presence of RAS was associated with worsened renal function. 24 Certainly there is a large body of work describing the adverse consequences of CHF on renal function, in addition to studies suggesting that renal artery revascularization may be an effective strategy to improve CHF status.25–29 Of interest, in the current analysis, CHF no longer remained a significant predictor of renal function at the 1-month follow-up, irrespective of method of analysis.
In the current study, we were also able to explore the factors associated with an acute (1-month) improvement in renal function. Clearly, the most important factor was baseline renal function, with this factor alone contributing substantially to the likelihood of whether an improvement in renal function would be observed (Figure 1). In addition, assignment to treatment with the Angioguard embolic protection filter and concomitant use of abciximab, a monoclonal antibody to the platelet glycoprotein IIb/IIIa inhibitor, was also associated with an improvement in renal function (Figure 2). Interestingly, we were unable to demonstrate a significant contribution of baseline stenosis severity to the likelihood of an improvement of renal function by either univariate or multivariate analysis, despite the fact that lesion characteristics were significant in the prediction of baseline and 1-month GFR. Thus, while stenosis severity appears to be a predictor of overall renal function, at least in the short-term, it does not predict whether renal function will improve. In the current study we are unable to determine whether longer-term changes in renal function after revascularization are related to the severity of the stenosis since this was not measured. While the mechanisms of action are not clearly known, it is presumed that embolic protection captures material embolized from the lesion during the intervention, whereas the platelet glycoprotein IIb/IIIa inhibitor serves to limit platelet aggregation and/or activation which may be deleterious in patients with chronic renal injury. 30
In conclusion, the current study suggests that several factors may contribute to renal dysfunction in patients with RAS, including congestive heart failure, and to a modest degree stenosis severity. More importantly, a positive response of renal function to revascularization appears to be dictated most strongly by the severity of renal dysfunction prior to the procedure and to a lesser degree the presence of CHF and the adjunctive use of embolic protection and a platelet glycoprotein IIb/IIIa inhibitor during stenting.
Footnotes
The data utilized for the current study was collected in a clinical trial funded by unrestricted research grants from Centocor Inc. and Cordis Corporations that are Johnson & Johnson companies. Dr Cooper is funded by the National Heart, Lung and Blood Institute 5U01HL071556.