
Abstract
Thoracic aortic aneurysm formation is a known complication of late syphilis. Large aneurysms may cause symptoms via mass effect. When aneurysms compress the pulmonary artery, pulmonary arterial hypertension and right heart failure may result. We report the case of a 76-year-old man who presented with right heart failure secondary to an 11-cm syphilitic thoracic aortic aneurysm, and discuss the evolving epidemiology, complications, diagnosis and management of syphilitic aortitis.
Introduction
Thoracic aortic aneurysm formation is a known complication of late syphilis. Large aneurysms may cause symptoms via mass effect on neighboring mediastinal structures. When aneurysms compress the pulmonary artery, pulmonary arterial hypertension and right heart failure may result. Images from a case were recently displayed; 1 here, we fully describe the clinical presentation and pathologic findings of this 76-year-old man who presented with right heart failure resulting from a massive syphilitic thoracic aortic aneurysm.
Case history
A 76-year-old man presented via an urgent care center with two episodes of near syncope over 48 hours, both while bending to tie his shoes. He described 6 months of worsening dyspnea on exertion and a weight gain of 40 pounds (18 kg). One month prior to presentation, he had begun oral furosemide, prescribed by his primary care physician for worsening leg edema. Past history included prostate cancer treated with androgen suppression and choroidal degeneration leading to legal blindness. He had emigrated from Dominica 5 years prior to presentation. He denied excess alcohol use and admitted to remote smoking. He recounted many sexual partners and reported, “I have many children.” He had no family history of aneurysmal disease or bicuspid aortic valve. His only medications were bicalutamide and furosemide. A review of symptoms disclosed mild, progressive dysphagia.
Examination revealed an ill-appearing man with blood pressure of 119/76 mmHg, heart rate 76 bpm, respiratory rate 18 bpm and oxygen saturation 96% on 4 liters of oxygen. A side-to-side head bob was evident. The jugular venous pressure exceeded 20 cm of water. The precordium was highly active with a right ventricular heave, an enlarged, displaced apical impulse and a pronounced impulse at the upper sternal border. Auscultation revealed a regular rhythm with a loud pulmonic component to the second heart sound, a III/VI holosystolic murmur best appreciated at the lower sternal border, a II/VI systolic ejection murmur noted at the left upper sternal border and left scapula, and a II/IV high-pitched early diastolic murmur heard at the left sternal border. Breath sounds were diminished at the lung bases. The abdomen was distended with bulging flanks and hepatomegaly. Symmetric edema was present in the pretibial regions. Peripheral pulses were all normal without delay.
An electrocardiogram suggested right ventricular strain (Figure 1). A chest radiograph showed a markedly enlarged aortic contour with rightward displacement of the trachea, a prominent right heart border and small bilateral pleural effusions (Figure 2). Computed tomographic angiography (Figure 3) demonstrated extensive thoracic aortic calcification and aneurysm dimensions of 11.5 × 11.4 cm in short axis and 18 cm in length. The aneurysm compressed the left main stem bronchus and main pulmonary artery. Transthoracic echocardiography demonstrated right ventricular systolic failure, elevated right atrial pressure and severe pulmonary hypertension with estimated right ventricular systolic pressure of 72 mmHg. The aortic valve was trileaflet with moderate insufficiency and no stenosis. The left ventricle appeared underfilled, with grossly normal systolic function, and associated mild left atrial enlargement.
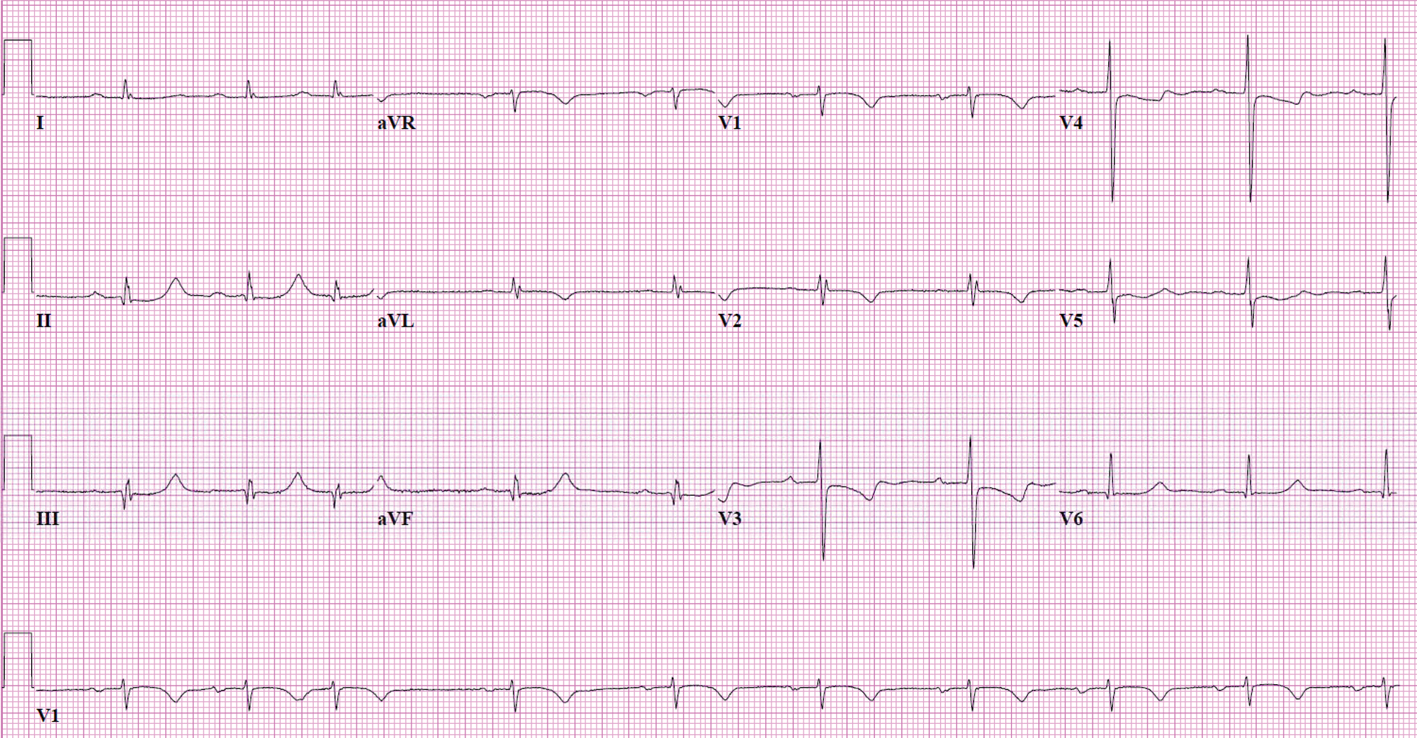
Electrocardiogram showed sinus bradycardia at 58 beats per minute with sinus arrhythmia, first-degree atrioventricular block, septal Q waves in inferior leads and repolarization abnormalities in leads V1–V4 compatible with right ventricular strain.
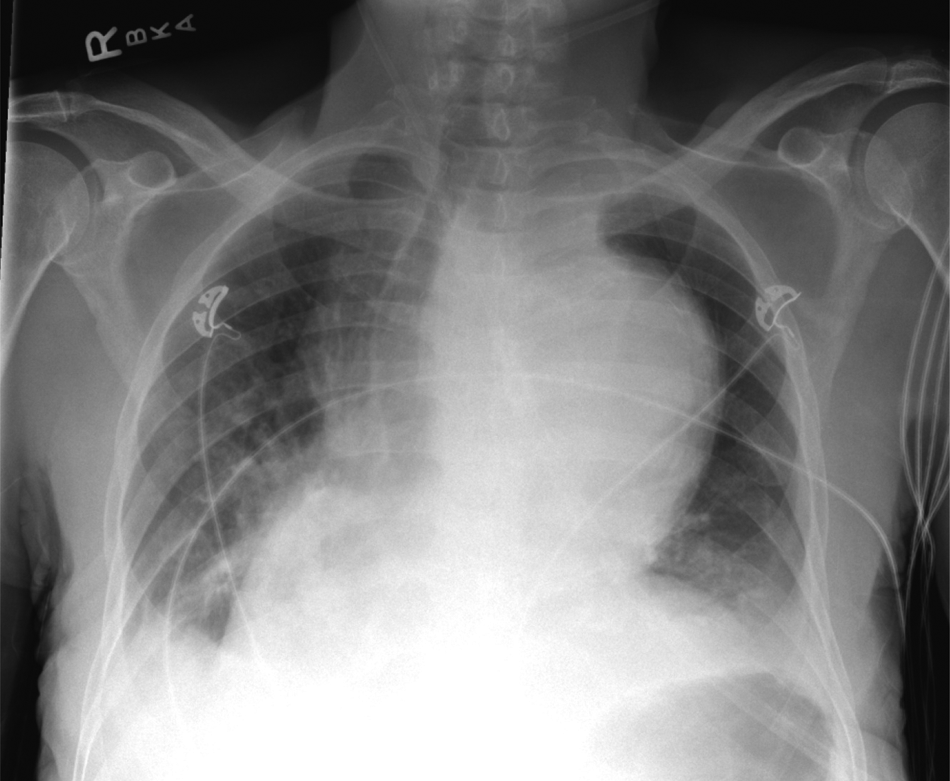
Chest radiograph showed a markedly enlarged aortic contour with rightward displacement of the trachea. A prominent right heart border suggested right atrial enlargement. Small bilateral pleural effusions are present.
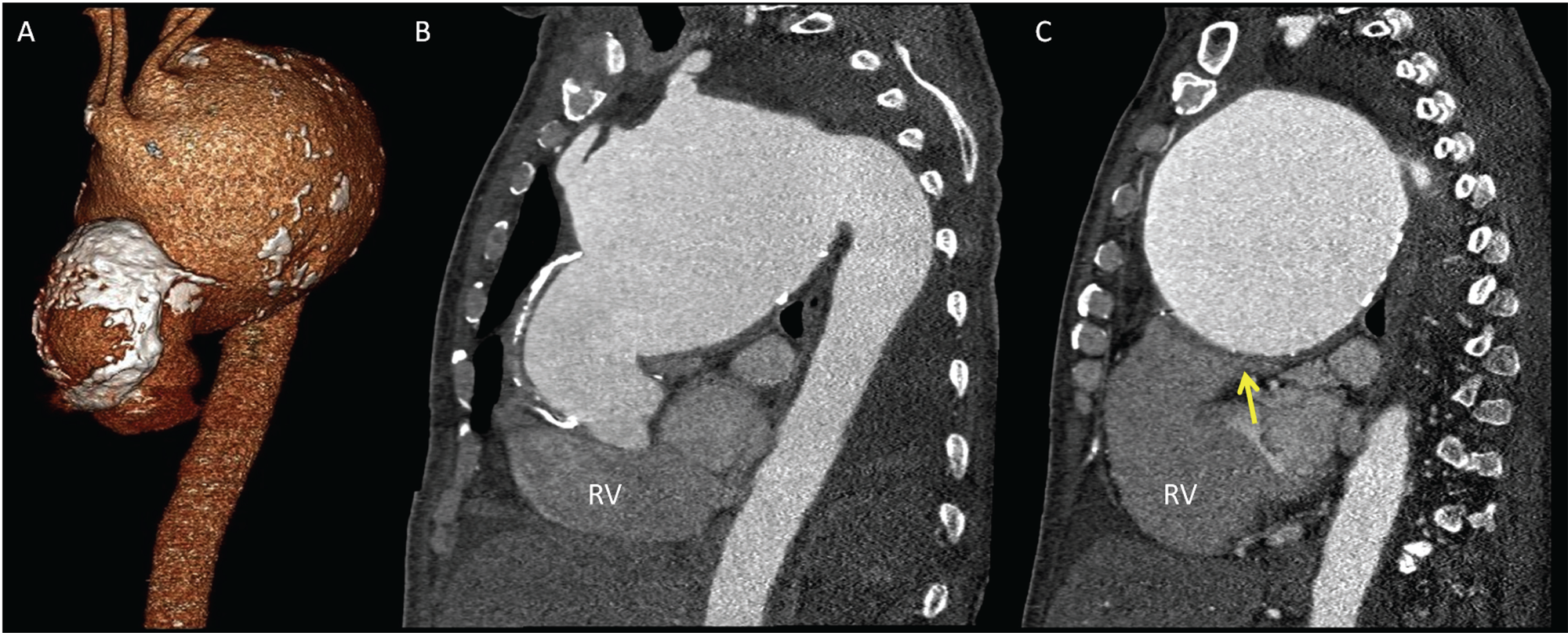
Volume rendered (A) and oblique maximum intensity projections (B, C) from computed tomographic angiography of the chest revealed an extensively calcified thoracic aortic aneurysm, sparing the sinuses of Valsalva, measuring 11.5 × 11.4 cm in short axis and 18 cm in length. The aneurysm caused substantial mass effect resulting in rightward tracheal deviation, moderate compression of the left main stem bronchus and severe compression of the main pulmonary artery (arrow).
Laboratory investigations revealed mild pancytopenia and synthetic liver dysfunction but normal serum transaminase levels and erythrocyte sedimentation rate. Rapid plasma reagin was positive with a titer of 1:4. Confirmatory fluorescent treponemal antibody was positive. Cerebrospinal fluid Venereal Disease Research Laboratory testing was negative. Studies for tuberculosis and HIV were negative.
Low-dose nicardipine and nitroglycerin infusions were initiated to decrease aneurysm wall stress. These were discontinued because of systemic hypotension requiring intravenous volume resuscitation revealing preload dependency due to fixed, severe pulmonary hypertension with advanced right ventricular failure. Antibiotic therapy with intravenous penicillin was also begun.
In light of the aneurysm size and progressive nature of the patient’s symptoms, surgical repair was recommended. Owing to the complexity of the operation, the patient was advised of a substantial risk of perioperative mortality and adverse neurologic events. The prognosis without surgery was felt to be poor with limited ability to ameliorate his progressive symptoms given his intolerance of both diuretics and vasodilators. Consensus was reached to proceed with surgery. After a challenging dissection, aneurysm resection and graft repair, there was an initial observation of normal cardiac function. However, bleeding was noted from a leak at the aortic root. Despite extensive efforts at repair and resuscitation, hemostasis could not be achieved. The patient expired.
Histopathology revealed aortitis with an adventitial lymphoplasmacytic infiltrate focally extending into the media. Extensive medial scarring was noted along with a paucity of medium-sized adventitial vessels and complex atherosclerosis (Figure 4). This constellation of findings is most compatible with syphilitic aortitis. 2
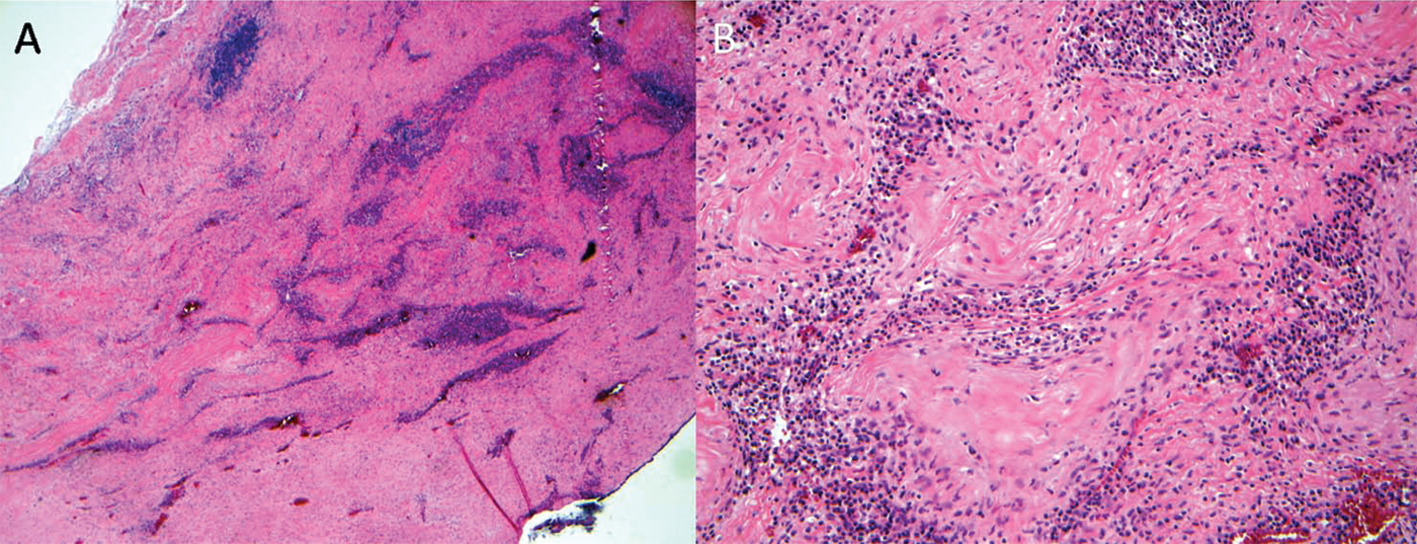
Low (A) and high-power (B) sections of the aortic aneurysm showed aortitis with an adventitial lymphoplasmacytic infiltrate focally extending into the media. Extensive medial scarring was noted along with a paucity of medium-sized adventitial vessels and complex atherosclerosis.
Discussion
This patient was felt to have progressive right heart failure resulting from mass effect from a giant thoracic aortic aneurysm of syphilitic origin.
Thoracic aortic aneurysms are a significant source of morbidity and mortality. Aortic aneurysmal disease classified as thoracic, thoracoabdominal or unspecified accounted for 12,545 discharges, or 0.4% of total discharges, from a large consortium of academic medical centers in 2006–2007. 3 Annually, dissection of the aorta (any part), thoracic aortic aneurysms, thoracoabdominal aneurysms and aortic aneurysms of unspecified site (ruptured or without mention of rupture) account for over 7000 deaths in the United States, based on query of Centers for Disease Control and Prevention (CDC) mortality data for the years 1999–2006. 4 These data, relying on the International Statistical Classification of Disease and Related Health Problems, Ninth Revision and Tenth Revision (ICD-9 and ICD-10) codes, respectively, likely underestimate the true burden of thoracic aortic aneurysmal disease, as they fail to include cases in which aneurysmal disease was unrecognized or misdiagnosed.
Thoracic aortic aneurysm formation is associated with several conditions, including atherosclerosis, hypertension, smoking, chronic obstructive pulmonary disease, congenital anomalies (bicuspid aortic valve, coarctation of the aorta, aberrant right subclavian artery, and right aortic arch), familial syndromes (Marfan, Loeys-Dietz, vascular Ehlers-Danlos, and Turner), inflammatory disease (Takayasu arteritis, giant cell arteritis, Behçet disease, and HLA B-27 positive spondyloarthropathies) and infections, including bacteria (in particular, Staphylococcus aureus, Salmonella, pneumococci, and Escherichia coli), fungi (in particular, Candida and Aspergillus), tuberculosis, HIV, and syphilis. 3 Vascular involvement in late syphilis is due to an obliterative small vessel endarteritis, usually of the vasa vasorum of the thoracic aorta, fostering loss of structural integrity of the tunica media and subsequent fibrosis and calcification. Recognition of cardiovascular syphilis is important, as, in addition to broader management of aneurysmal disease, it warrants antibiotic therapy, for which penicillin is preferred.
Although far rarer than in decades past, syphilis remains relevant as a potential source of aneurysmal disease. Rates of syphilis declined sharply following the initial reporting of surveillance statistics in 1941, capped by a 90% fall in incidence of primary and secondary syphilis in the 1990s to a nadir of 5979 reported cases in 2000. Over the years 2001–2008, however, incidence of primary and secondary syphilis more than doubled, with a majority of new cases occurring in men who have sex with men. 5 These data likely do not capture a large number of individuals who do not seek medical attention for the painless chancre of primary infection, the non-specific rash of secondary syphilis, or the silence of latent illness. Accordingly, the observed rise in early syphilis forebodes a parallel resurgence in late disease, including cardiovascular syphilis, in years to come.
Definitive diagnosis of syphilitic aortitis can be challenging owing to long latency from primary infection to aneurysmal dilatation and the inability to culture Treponema pallidum on standard media. Clinical diagnosis is most often made based upon serologic confirmation of syphilis and a characteristic pattern of vascular involvement. Aortitis typically involves the tubular portion of the ascending aorta, aortic arch and descending thoracic aorta, sparing the sinuses of Valsalva. 6 Clinically relevant aortic valve insufficiency is unusual. Exceptional cases have been reported, however, describing aortic insufficiency 7 and ostial coronary artery stenosis. 8 Syphilitic vasculitis and aneurysmal disease affecting the abdominal aorta, 9 pulmonary arteries, 10 coronary arteries, 11 and aortic arch branch vessels have also been reported. 12
Large syphilitic thoracic aortic aneurysms may cause symptoms via mass effect on neighboring mediastinal structures, including the trachea, esophagus and pulmonary artery,13–15 as in our patient. Additional reported complications include compression of the superior vena cava, 16 erosion into the chest wall 17 and thoracic spinal bodies, 18 erosion into the airways 19 and esophagus, 20 and fistulization to the pulmonary artery. 21 As with aneurysms of other etiologies, patients with syphilitic aortitis are at risk for dissection and rupture.
Thoracic aortic aneurysms grow at a rate upwards of 0.10 cm per year, with risk of complications, including dissection and rupture, increasing sharply as the aneurysm diameter surpasses 6.0 cm. 22 Consensus guidelines advise surgical evaluation for all patients with symptoms suggestive of thoracic aortic aneurysm expansion, regardless of size, as well as asymptomatic individuals with an ascending aortic or aortic sinus diameter of 5.5 cm or greater. 3 Our patient’s case illustrates how, for individuals with giant thoracic aortic aneurysms, management may obligate a choice between Scylla and Charybdis: high-risk surgery or the inevitable progression of disease. A multidisciplinary approach is paramount, and a patient’s personal values must be carefully assessed.
Conclusion
This case demonstrates the potential of large thoracic aneurysms to cause pulmonary hypertension and right heart failure, and how, in advanced stages, massive aneurysms may obligate difficult management decisions for physicians and patients. Ascertaining the etiology of aneurysmal disease is important. Syphilis, though far less common today, continues to be a relevant source of aneurysmal disease, and may indeed grow in prevalence in decades to come.
Footnotes
Dr Murthy is supported in part by a grant from the National Institutes of Health (T32 HL094301-01A1).
The authors declare that there is no conflict of interest.