
Abstract
This article explores two potential forms of institutional ageism within Norwegian General Practitioner (GP) services for older adults experiencing mental health and substance abuse challenges. Despite recent legislative developments - including anti-discrimination laws that prohibit age-based discrimination in healthcare - transformation appears to be unfolding in services for the population. Drawing on interviews with 17 systems-level stakeholders, this study examines their perceptions of potential institutional ageism in Norwegian GP services, their roles in addressing it, and the possibilities for legal recognition and intervention. Rather than offering a legal analysis, the article presents a sociological inquiry into cultural beliefs that may shape the interpretation and implementation of legislation. It identifies a web of underlying beliefs that inform stakeholders’ views and may contribute to systemic inertia. The findings suggest, that unless these beliefs are critically examined and challenged, legislation may fail to prevent institutional ageism and instead risk legitimizing inaction amid broader welfare state transformation.
Keywords
Introduction
Of adults aged 60 and over, approximately 14% have a mental disorder, and between 2 and 9% report abuse of alcohol or other substances. 1 Demands on mental health and substance abuse (MH/SA) services are expected to increase with the aging of the world´s population. Many effective treatments are available for older adults with MH/SA disorders. 2 Despite documented prevalence of need, and the availability of effective treatment, international research shows lower utilization of MH/SA services among older adults. 3 Ageism in MH/SA assessment and treatment may help explain these inequalities. 4
Legal protections against age discrimination have been strengthened in EU/EEA legislation in recent years. 5 While much of this legislation establishes protections around labor participation, 6 some states have also included more general prohibitions against age discrimination. In Norway the adoption of the Equality and Anti-Discrimination Act in 2017 established a prohibition against age-based discrimination in all areas of society. 7 A reasonable inference is therefore that it is prohibited to discriminate based on age when delivering MH/SA services. Additionally, the Health and Care Services Act from 2011 offers a legal commitment to ensure municipal health care provision is based on equality. A reasonable inference is that this includes age-based equality. 8
Scandinavian societies, including Norwegian, are traditionally known for their high level of socioeconomic equality, gender equality, and equality in access to services like healthcare, all of which are ascribed at least partially to the Scandinavian welfare model with its emphasis on universalism. 9 Scandinavian universalism has historically fared better than British universalism, 10 but concerns are rising about its erosions, possibly related to international welfare state convergence. 11 The current Norwegian welfare state context is therefore one where new equality-oriented legislation has been adopted in parallel with an ongoing equality-eroding welfare state transformation. This transformation is interesting because, as the organizational theorist Nils Brunsson argues, decisions like legislation may conceal and thus legitimize organizational or political inertia related to exactly the problems it aims to solve. 12 Martin Luther King wrote about the ”paper laws” that purported to protect equality for black Americans, but that were in practice left unenforced. A problem with unenforced discrimination legislation is that it may prevent other efforts to promote social inequality and combat discrimination, such as organized action. 13 For example, there are strong indications of disparities in access to healthcare services for older Norwegians with MH/SA problems, 14 which may be an expression of both prevailing ageist practices despite anti-discrimination legislation and of an ongoing, equality-eroding welfare state transformation. 15
In the Norwegian context, General Practitioners (GPs) are physicians with broad, comprehensive knowledge about the examination, treatment and prevention of disease who act as gatekeepers to specialist (including MH/SA) services.
16
Norwegian GP services are regulated by the “Regular General Practitioner Scheme” (GP scheme),
17
a 2001 policy which guarantees GP services to all citizens and regulates GP reimbursements.
18
A recent study indicates that certain structural aspects of this GP scheme may encourage and justify ageist practices in service provision to older people with MH/SA problems.
19
This previous study identified GPs’ descriptions of outcomes in Norwegian MH/SA services that we consider potential forms of institutional ageism,
20
though they did not use the term “ageism”. In the present article we present research findings from interviews with various systems-level stakeholders regarding the potential forms of institutional ageism identified in the previous study. Systems-level stakeholders include representatives from agencies and organizations assigned an overarching responsibility for the GP scheme and/or for receiving and handling complaints about inequality or discrimination in healthcare delivery. This article aims to address the following questions: • How do systems-level stakeholders perceive potential institutional ageism and ageist practices in MH/SA services for older adults? • How do systems-level stakeholders describe the role of their organizations/agencies in monitoring, sanctioning, and preventing ageist practices in MH/SA services for older adults? • What are the potential legal, political, or practice related changes that systems-level stakeholders posit may prevent ageist practices?
The article shows how systems-level stakeholders do not necessarily recognize potential forms of institutional ageism as valid or age discriminatory by legal standards. It also explains how, in cases where stakeholders do recognize these forms of institutional ageism as valid, their perceptions of their own roles may contribute to systemic inertia—making it unlikely that such practices will be effectively monitored, sanctioned, or prevented. Our findings highlight a potential web of cultural beliefs that may underpin systems-level stakeholders perceptions. Lastly, we discuss the implications this web of beliefs may have for the function of equality-oriented legislation (including anti-discrimination legislation) within an equality-eroding welfare state transformation.
Background
The concept of ageism
According to the WHO, “ageism” refers to “the stereotypes (how we think), prejudice (how we feel) and discrimination (how we act) towards people on the basis of their age”. 21 The WHO defines three types of ageism: (1) interpersonal (between two or more individuals), (2) self-directed or internalized ageism (where a society´s age stereotypes influence individuals’ own perceptions of self-worth due to their age), and (3) institutional ageism (laws, policies, practices, and social norms). 22 Experts claim that, globally, one in two persons hold ageist attitudes toward older people. 23 In a study of 28 European countries, age was the most frequently mentioned reason for those experiencing discrimination. 24
Ageism is often described as a complex and pervasive issue that manifests in various direct and indirect forms. 25 Direct ageism involves overt acts of bias, whereas indirect ageism comprises subtler biases and systemic practices that may go unnoticed by perpetrators. According to medical sociologist, Carroll Estes, ageist beliefs or stereotypes contribute to the development of social schemas and constructs that foster age-based disparities, especially in healthcare delivery. 26 Estes claims that the study of beliefs, values, and ideology is central to understanding competing constructions of reality regarding old age. 27 These constructions signal whether and how older adults are defined as valued and deserving in society. 28 The impact of legislation on reducing discrimination and inequality depends on several factors, such as the extent to which cultural beliefs support the law. 29
Some argue that ageist beliefs, rooted in stereotypes, may give rise to social schemas that categorize older individuals as inherently frail, dependent, burdensome, and undeserving. 30 The ageist belief that all older people are dependent may lead to the belief that they are a burden on, and a liability to, the sustainability of health care and welfare systems. Beliefs of this type may shape the perceptions and expectations of healthcare professionals and leaders when assessing the needs, capabilities, and deservingness of older people resulting in indirect and possibly unintentional ageism and age-based discrimination in healthcare services. 31
Norwegian legislation and structural protections meant to prevent ageism
Legislation occupies an important position in structures of the Norwegian welfare state meant for protection of universalism and equal access to services like healthcare. This aspect of the welfare state´s structure can be seen as a remnant of the Weberian governance paradigm that accompanied the expansion of the welfare state in the post-second world war decades. 32 A Weberian governance paradigm emphasises hierarchy and rule-based governance, where elected politicians made politics that public administrators implemented. 33 This paradigm differed from its successors, New Public Management and then New Public Governance. The currently dominant New Public Governance regime favours a division of labor between politicians and public adminstrators that differs from the one in the original Weberian regime. It emphasizes governance through collaboration between diverse stakeholders within and outside public organizations, and is associated with terms like “co-production” and “co-creation”. 34 A critique against New Public Governance has been that it implies willingness to negotiate goals with stakeholders who are not democratically elected, hereby possibly undermining concerns for the whole of society. 35 However, remnants of the Weberian paradigm – like the focus on legislation – still co-exists with elements from this governance paradigm currently.
The focus in this article is on ageism in GP services, which are regulated by the Norwegian Health and Care Services Act.
36
Additional protections for equality in GP services are provided through the Equality and Anti-Discrimination Act,
37
which includes both individual and structural protections. The law´s individual protections prohibit direct and indirect differential treatment on a series of grounds, including age (Section 6, 7 and 8).
38
“Direct differential treatment” means treatment of a person that is worse than the treatment that is, has been or would have been afforded to other persons in a corresponding situation because of age (or other protected categories). “Indirect differential treatment” means any apparently neutral provision, condition, practice, act or omission that results in persons being put in a worse situation than others based on age (or other protected categories). Further, section 9 states that differential treatment does not breach the prohibition in section 6 if it (a) has an objective purpose, (b) is necessary to achieve this purpose, and (c) does not have a disproportionate negative impact on the persons subject to the differential treatment. This Act´s structural protection obligates both public and private entities to promote equality and prevent discrimination. For example, the “activity and reporting obligation” establishes that, “Public authorities shall in all their activities make active, targeted and systematic efforts to promote equality and prevent discrimination as specified in section 6” (Section 24).
39
Similarly, section 24 also requires that, “Public authorities shall describe what they are doing to convert equality and non-discrimination principles, procedures and standards into action”.
40
In Norway, several agencies share responsibility for monitoring and enforcing the legal obligations related to the
In addition to the individual responsibility of practitioners, three categories of systems-level agencies have responsibility for enforcing the legal commitment to equal treatment under the
Additionally, two enforcement agencies are assigned responsibility for facilitating “access to justice” related to the ban on age discrimination in the
In addition to the enforcement apparatus related to legislation, a range of organizations and systems-level stakeholders may exert influence over how legislation ends up interpreted and sanctioned. Throughout the history of discrimination legislation civil society organizations have played important roles in influencing juridical practices. 46 In Norway, public and civil society stakeholder organizations of relevance to age discrimination in health care include the Norwegian Medical Association, the former Alliance of Human Rights (which did advocacy work prior to the adoption of Equality and Anti-Discrimination Act), research institutions, and consultant agencies, among others.
The prevalence of ageism in healthcare related to MH/SA problems
Although there are few Norwegian studies about healthcare where the term “ageism” figures, there are some reports indicating that Norwegian MH/SA services carry ageist traits. 47 Moreover, while the proportion of younger adults (18-39) accessing MH/SA services increased between 2016 and 2020, the proportion of older adults (40+) accessing the same services decreased over the same period. 48 These utilization statistics reflect a growing age-based disparity in access to MH/SA for older adults. A Norwegian study of 383 patients above 65 revealed that one in three suffered from moderate depression unrecognized by their GP. 49 In 2020, the Norwegian government identified both older people and patients with MH and SA problems as among those receiving inadequate GP services. 50
The Norwegian GP scheme and potential institutional ageism
Historically, Norwegian municipal health care services are organized as a public service. 51 However, GP services are a partial exception. Under the GP scheme, most GPs operate as private businesses, and only about one in five are publicly employed. 52 Still, all GPs – regardless of employment type - are reimbursed by the state. It is also a public responsibility to ensure that every citizen who wants a GP is assigned one, and that everyone has access to affordable, high quality GP services that meet legal obligations, including the commitment to equality. 53 Within this system, a large portion of state reimbursement to Norwegian GPs is regulated by a tariff system. 54 GPs can claim a refund from this system for each consultation and each service offered to a patient. The types and amounts of these tariffs are defined in a government regulation. 55 This regulation is the result of annual negotiations between the Medical Association, the Ministry of Health and Care Services, and the Norwegian Association of Local and Regional Authorities. 56 It is administered by the National Health Economics Administration (Helfo). 57 GPs receive regular reports from Helfo showing their use of each tariff compared to the national average. Substantial divergence from the average may trigger responses from the National Board of Health Supervision, including rejecting claims or, in rare cases, the withdrawal of authorization to practice. As a result, some GPs experience this oversight as a source of pressure, leading them to adjust their practice to align with average tariff use. 58
In recent decades, Norwegian health policy has repeatedly claimed that demographic change—specifically, a growing proportion of older adults—threatens the financial sustainability of the health care system by creating an overburdened service. 59 While this concern may have some basis, it may also be overstated and oversimplified, reflecting ageist assumptions and prevailing cultural beliefs. This narrative is not unique to Norway, similar claims appear in policy documents from international organizations like OECD 60 and are even embedded in research financing priorities. For instance, the Norwegian Research Council has issued calls for proposals aimed at developing interventions, innovations, and research to improve the sustainability of health and care services. 61 One consequence of this framing may be that very little research currently addresses ageism or age discrimination as legal issues within Norwegian health care. Nevertheless, the term “discrimination” is used openly in public discourse about older adults’ access to MH/SA services. 62
A previous Norwegian study attributed the healthcare system´s failure to prevent ageist practices in MH/SA services, in part, to a mechanism recognizable from the organizational theorist Nils Brunsson’s theory about 63 the “localization strategy”. This refers to the tendency to maintain established beliefs even when confronted with contradictory evidence. Experiences that challenge dominant assumptions are often dismissed as anomalies, misinterpretations, or irrelevant. In the Norwegian study of healthcare for older adults with MH/SA problems, this manifested as a persistent belief in the Norwegian welfare state´s universalism and commitment to equality – despite evidence of inequalities. 64 The ongoing lack of research on age discrimination in health care may help sustain this “localization strategy,” allowing ageist practices to remain unexamined and unchallenged.
This calls for reflection in the current context, where the Norwegian welfare state—once known for its strong commitment to equality—is undergoing transformation. 65 The inequalities experienced by older adults in need of MH/SA services may signal an early stage in the erosion of universalism, a principle traditionally linked to equality. 66 Due to the “localization strategy”, scarcity of research may contribute to societal inertia related to this transformation.
The previous study this article builds on described, among other things, what we in the present article see as two forms of potential institutional ageism in the GP scheme. First, it found that GPs often fail to detect mental health and substance abuse problems among older patients or ensure they receive adequate treatment. 67 This failure was understood to be rooted in structural conditions, 68 resulting in the use of the term “institutional ageism” in this article. The reason was that the tariff system created financial incentives for shorter consultations over longer ones. Several GPs, though not all, reported that their practices were influenced by pressure to conform to the standards set by the Norwegian Health Economics Administration (Helfo), and by fear of sanctions for unjustified deviations in tariff use. Because GPs must consider the economic viability of their practices, the tariff structure influences, according to them, how they prioritize and organize their workday.
This system may indirectly place older patients with MH/SA problems at risk of receiving lower-quality care and facing more limited access to specialist services. GPs noted that working effectively with older patients often requires more time, due to factors such as greater shame, reluctance to seek help, and the presence of multiple co-occurring conditions. 69 However, because the tariff system rewards brief consultations, it discourages the kind of time and engagement needed to detect and attend to older patients’ MH/SA problems.
The previous study also identified a second form of potential institutional ageism as affecting GP services for these older adults. GPs described how increasing workloads - driven by societal changes and healthcare reforms - created pressure to find practical ways to manage time. One such strategy involved de-prioritizing health issues that patients did not explicitly verbalize. As one GP described, “We squeeze [out] the ones who don´t shout.” 70
Formally, GPs may only charge for services when a patient initiates contact, 71 and informally, the system assumes that patients are responsible for presenting their own health concerns. GPs stated that older patients were less likely than younger patients to verbalize MH/SA issues, making these problems more likely to go undetected and untreated. 72 This reliance on patient-initiated contact and verbalization of problems may unintentionally produce ageist outcomes. While this practice may reflect liberal values such as autonomy, non-interference, freedom from prejudice or skepticism to paternalism 73 it risks reinforcing inequality when applied to vulnerable groups. Belief in autonomy is central to anti-discrimination legislation 74 and is echoed in more modern narratives of “successful aging” and older adults as independent and self-reliant, but may obscure the need for proactive care. 75
Recognition of the possibility of institutional ageism may be especially important in light of the recommended prioritization criteria outlined by the Norwegian Ministry of Health and Care in April 2025. 76 The criteria for prioritizing services include “benefit”, “resources”, and “severity”. While still in early stages of implementation, such efforts at prioritization of health care services could further institutionalize ageist practices and deepen existing inequalities.
Methods
The aim of this article is to explore how systems-level stakeholders perceive the two above-described potential forms of institutional ageism in GP services for older adults. It also examines how these stakeholders describe their agencies´/organizations’ roles in monitoring, sanctioning and preventing this potential institutional ageism, and what legal, political, or practical changes they believe could help prevent it. Through this examination we will aim to uncover underlying cultural beliefs that may influence the scope and potential societal function of equality-promoting legislation in the context of welfare state transformation. Thus, the aim of this article is not to conduct a legal analysis, but a sociological one. A key premise to it is the idea that underlying cultural beliefs will often impact on the scope and societal function legislation ends up having.
Individual interviews (n = 17) were conducted between September 2020 and May 2023 with systems-level stakeholders. Systems-level stakeholders were recruited (by phone or email) based on their positions in organizations/agencies assigned some form of responsibility for the GP scheme and/or for receiving and handling complaints about inequality or discrimination in healthcare delivery.
Study participants
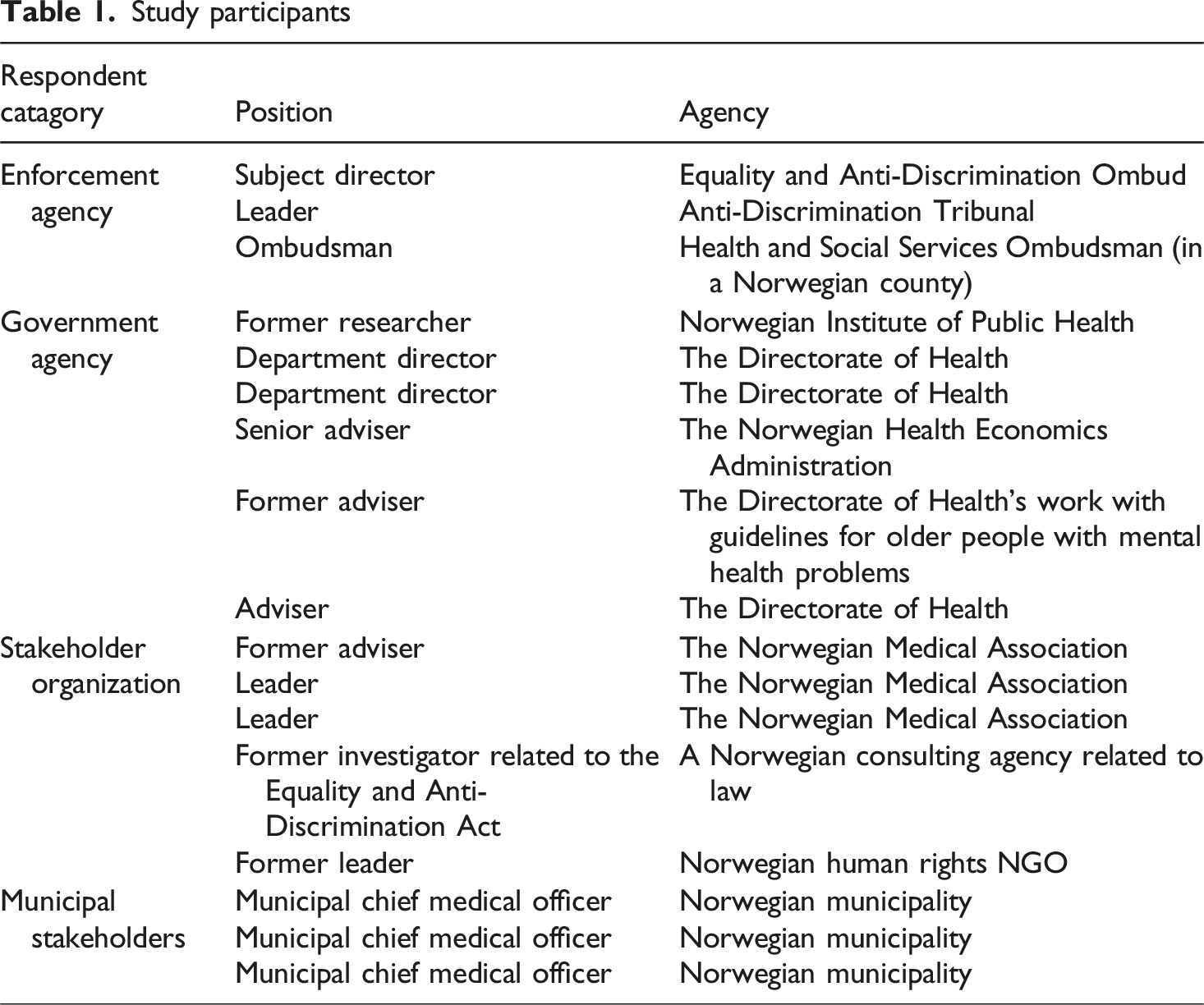
Notes were taken during interviews and interviews were recorded and transcribed verbatim when possible. Approval for human subject research was received from the Norwegian Agency for Shared Services and Research (reference code 598740). All participants were informed about the study and provided consent.
The sum of the qualitative data was thematically analyzed. 79 Interview transcripts and audio recordings were reviewed multiple times, with notes and highlights used to identify emerging themes. Through iterative writing and reflection, we uncovered connections across the data, revealing systems-level perceptions and beliefs that may influence practices—particularly legal ones—related to the GP scheme. However, we did not collect data on the practices themselves. Our analysis was informed by Carol Bacchi´s “What’s the Problem Represented to be?” (WPR) framework for critical policy analysis. 80 Interview findings were compared with current discrimination and healthcare legislation, including participants’ views on the enforceability of laws addressing institutional ageism.
Findings
Below we present key findings about systems-level stakeholders’ perceptions of the validity of findings about potential forms of institutional ageism in GP services to older MH/SA patients; their perceptions of the role of their organizations in monitoring, sanctioning, and preventing ageist practices in MH/SA services for older adults with MH/SA problems; and their ideas about potential legal, political, or practice related changes that may prevent ageist practices.
The Prevalence and validity of potential forms of institutional ageism
Several participants, including from government agencies, acknowledged the potentially inequality-producing effects of the GP tariff system. To some, however, this perception was combined with strong trust in the system. As one participant from a government agency said, “By and large, we must trust that the system works according to the intention.” This participant described a private experience with a GP who they saw as influenced by the tariff system in such ways that an older family member ended up with poorer GP services. When asked whether they interpreted this personal experience as an exception to how this tariff system normally worked, they responded, “I would believe that. I trust the system”. This understanding resonates with similar understandings, expressed in interviews, by other systems-level stakeholders. For instance, a municipal stakeholder said, when confronted with the findings about the potentially negative impact of the Helfo system on older MH/SA patients’ services, “I think this is not a topic”. Another participant from a government agency emphasized that the system was not intended to work the way GPs had reported it to work, and commented, “Is it the system that is skewed, or is this a practice that the GPs have acquired to be able to defend their own practice?”, apparently suggesting that there were good intentions behind the Helfo system, but that it might serve as a scapegoat to GPs, without necessarily being the real root of potential ageist practices.
At the same time, interviews revealed an alternative view among some stakeholders, who were more open to the possibility that the findings reflected broader patterns in GP services. A municipal stakeholder from a populous Norwegian municipality said, for instance, The way the earnings [of GPs] are structured, then, with Helfo and its tariff system… I believe it does not always support good clinical practice. And that applies related to [older MH/SA patients] in particular.
Different versions of this alternative perception became apparent in interviews with participants from government agencies and stakeholder organizations. For example, a participant from a government agency described the tariff system´s impact like this, “You get these five-minute “slots” that the doctor works with (…) before he has to attend to another patient. Or actually: to a different tariff. That’s how it’s designed: Thump, thump, thump, thump, thump.” A participant from a stakeholder organization added, “One could definitely raise a debate about how well-suited such a tariff system is for promoting quality”. Another described the tariff system as hampering the possibilities for the municipality to ensure that GP services provide equal access to all patient groups.
As we have seen, there were divergent perspectives on the prevalence and validity of the ageist impact of the tariff and control system on systems level. However, agreement appeared to prevail concerning the prevalence, in a GP setting with work pressure, of de-prioritization of non-verbalized needs. There also appeared to be agreement about the possibility that this might foster age-based inequalities harmful to older MH/SA patients. A participant from a government agency said, for example, “[These patients] will not enter the GP´s office saying “You know what? I will not surrender! (…) I want an answer before I leave”. They will always suffer from [referring to the tariff system] … Because it is designed to favor the strongest ones”. Several other participants voiced similar judgements.
Legislation was explicitly thematized more strongly in some interviews, typically in those where the respondent was educated in law or where legal issues were key to the relevant agency’s daily work. Below follows a series of data excerpts from interviews where legislation was particularly strongly emphasized. They concern whether and to what extent the two potential types of institutionalized ageism this article focuses on (1) the tariff and Helfo control system and (2) de-prioritizing non-verbalized issues) could be considered age discriminatory in a legal sense.
As we have seen, the Equality and Anti-Discrimination Act establishes, in section 8, that any apparently neutral provision, condition, practice, act or omission that results in persons being put in a worse situation than others (based on age, among other factors), reflects indirect differential treatment. 81 As such, indirect differential treatment based on age is discriminatory according to the law. Thus, an interesting question is whether older MH/SA patients’ poorer access to GP services resulting indirectly from de-prioritization of non-verbalized issues is age discriminatory in a legal sense. A consistent finding from our interviews was that it could not be considered age discriminatory. However, there were limits to that position. First, some claimed that it might be possible to see knowledge about the relevant forms of institutionalized ageism as unleashing the structural aspect of the Equality and Anti-Discrimination Act. Second, one respondent appeared open to the idea that if certain exceptional conditions were met, it could perhaps be considered discriminatory in a legal sense not to offer healthcare to someone who failed to report verbally about a need for it.
These perceptions can be illustrated by a statement from a participant who, as a lawyer in 2014 had provided guidance to the government regarding whether the (then planned-for) Equality and Anti-Discrimination Act
82
should mention age as a prohibited ground for discrimination. “It is This is a result of the individualized nature of legislation. We should perhaps look to the indirect legislation here. (…) According to (...) the Equality and Discrimination Act, public authorities are obliged to work structurally. So that could of course be an approach: To encourage information dissemination.
Also an academic and professional who had had a key role in the development of national guidelines related to older people´s MH, seemed to confirm that de-prioritizing non-verbalized issues could not be considered discrimination in a legal sense. Commenting on the low percentage of older people (compared to young) being referred to specialized mental health services, he said, “It could be that this is a result of discrimination. However, it is not certain (…) It could also reflect that older people do not ask for services”.
Below we have included an excerpt illustrating what the respondent from an enforcement agency portrayed as an exception to what he perceived as the main rule (implying that it was normally not legally discriminatory to de-prioritize non-verbalized health care needs), Of course, there are limits to this principle. For example, if I know that a person with such and such a condition is under my care [as a health care provider], then there´s a reasonable expectation that someone in my professional capacity would know: “Ok, a person with a motor problem is struggling in the swimming pool – I can´t let that person drown even though they are not calling out for help”.
Role of systems-level agencies in monitoring, sanctioning and preventing ageist practices
A key finding, particularly from the enforcement agencies, was that their perceived possibilities to monitor, sanction and prevent the potential forms of institutional ageism depended on two types of reports. The first type was verbal reports from patients, guardians or care partners. The second was reports in the form of authoritative knowledge. Both could, according to the perception they conveyed, legitimize a practice on their part where the relevant forms of institutional ageism were monitored, sanctioned or prevented. This perception was justified with reference to assumptions about people´s general inclination to report in this way when issues mean a lot to them. It was also justified with reference to liberal values like freedom from prejudice and respect for individual autonomy, and to resource constraints. Another key finding was that for various reasons the agencies rarely received such reports, which according to them led older people´s MH/SA issues to become a marginal issue to their agencies’ work.
This perception became apparent in several ways in interviews. A respondent from an enforcement agency said for instance, when explaining why older people´s MH/SA problems occupied a marginal position in their work, “My impression is that we have few complaints from older people…. I don´t think it is that they are not displeased with their GP. But they… do not think about contacting us about it.”
This perception also became apparent in their account for certain types of information that in their view did not provide legitimate ground for them to monitor, sanction or prevent. A respondent from a government agency confirmed having received similar reports from individual GPs about the effects of the tariff and Helfo control system, consistent with the findings from the previous study. However, he explained that such information did not give sufficient grounds for the agency to take action. Taking action would, he claimed, have required “good data indicating that ‘This is the way it is´”. It would, in other words, have required access to knowledge considered sufficiently authoritative.
A respondent from an enforcement agency expressed a slightly different perception for why the forms of institutional ageism affecting older MH/SA patients were marginal to the agency´s work. He explained that in those cases when age discrimination became an issue to the agency, it happened because of incoming complaints. These complaints typically concerned age discrimination in working life. When asked why he believed they concerned working life, he replied that it probably was because the complainants must be willing to participate in the agency´s case process: Respond to questions and write and read case documents. He reported that he believed people´s jobs were often so important to them that they were probably willing to participate in what could be an arduous process. A consequence was that discrimination in healthcare experienced by older people with MH/SA problems became a marginal issue to the agency.
A representative of another enforcement agency justified a similar perception (that the possibilities and responsibility for action on systems level depended on reports) with reference to liberal values like respect for individual autonomy and freedom from prejudice, as he said, If I don’t bring my needs to the attention of my employer or my service provider, then they´re not obliged to do anything about them. Because the alternative would be that they go around and make all sorts of assumptions about people. You might end up in a situation where they pathologize someone, or rely on stereotypical assumptions, like “Oh - there´s an older person. I bet he´s infirm” or “I bet he´s an alcoholic”. Not good, right? So instead, the law operates on a kind of ‘innocent until proven guilty’ principle.
Below follows a statement from a respondent from another enforcement agency providing yet another justification for such a role perception, and for the practice resulting from it. This justification is resource constraints, We are not rigged organizationally to do (…) outreach. We do it in some cases. And (…) get “fired up” when you [as a researcher] contact us because (…) we need (…) a factual base. We need findings (..). We do not have the capacity to find that (…). A lot of our capacity is spent on answering phone calls and inquiries, and on offering help in singular cases.
The findings also indicate that resource constraints in knowledge development organizations may influence whether enforcement agencies gain access to the authoritative knowledge they perceive their capacity for action depends on. Of interest related to this is a finding from our interview with a respondent from a government agency with responsibility for knowledge production. She explained that the national government had imposed austerity measures on her agency a few years ago. Austerity had prompted the agency to enter into an agreement with the Directorate of Health. The contract 83 established that her agency should from then on only develop knowledge reviews about narrow research questions, that is, only about the effects of measures. Further, the effect measures must be specific. This implied, according to the respondent, that only findings from RCT studies could be considered facts and as such, be included in the reviews. Thus, if resource constraints have a similar impact on other Norwegian knowledge development organizations, like universities, then it may have consequences for systems-level agencies. It may affect their capacity to develop that type of knowledge about institutionalized ageism the respondents saw themselves to depend on in order to monitor, sanction and prevent in the absence of individual reports.
Potential changes to the “institution”
We did not ask all interview objects about their views on changes that could be initiated to reduce the impact of potential institutional ageism on GP services to older MH/SA patients. However, this often arose from the interviews as an important consideration.
A common view that was put forth was for example that equality for older MH/SA patients in GP services would probably have been the result if GPs had received fixed salaries (rather than, as currently, often running businesses). One stakeholder organization favored, according to the interviewed leaders, the continuation of a system with private businesses and tariff use for GPs. However, the respondent from this organization also noted a shift in preferences among GPs, echoing comments from government agency representatives: “more and more [GPs]now want a fixed salary – and especially the young [GPs]”. Moreover, a respondent from a government agency suggested that a relevant measure in the face of the potential forms of institutional ageism could perhaps be to introduce new tariffs particularly suited for older adults with MH/SA problems. They mentioned that during the pandemic the national authorities had made changes in the tariff system that would have been more difficult to make outside of the pandemic. They also said, “It could be so serious, what you will be presenting [from interview with GPs and a survey among GPs about this topic], that it must be possible to consider: Should there be proper tariffs for this?”. They also mentioned as a possibility that new guidelines of relevance to older MH/SA patients perhaps could be developed, and said,“Is there anything we need to look at in relation to our guidelines? Do we need to create some more guidelines?”.
Participants from a government agency further suggested so-called “primary health teams” (part of a national effort being piloted when the interview took place) 84 as a relevant measure possibly suited for enabling GP services to attend better to non-verbalized issues, by including other professions, like nurses. “Personally, I strongly believe that could be a good tool for these groups”, one said, with reference to older MH/SA patients. Another respondent from a government agency recommended that Helfo´s figures concerning tariff use, key to its control regime, were used with great care, as they said, “Unless that information [the figures showing average tax use] is worked on, both in the way it is collected and also in the way it is communicated, then I would say: No. Then I would not use that information. Because it is false. It is a wrong picture”.
In some interviews it was thematized whether the whole tariff system could have been abolished. It was also thematized whether those tariffs that the GPs had said in interviews were most relevant to providing older MH/SA patients with good services, could be significantly raised to stimulate to equality. However, the respondents often discarded such measures as unrealistic and/or undesirable. This was partly due to productivity- and public finance-related concerns. For instance, a respondent from a stakeholder association said, “I sometimes think: Do we have to have a tariff system? But it is a very productive system. Research shows that productivity drops by 30% when you switch to fixed wages.” Partly, this was discarded also because it was perceived as very difficult for systems-level stakeholders to contribute to increases in concrete tariffs. This was because the size of the tariffs was decided in negotiations. A respondent from a government agency said, for example, “The tariff system is a result of negotiations. It is not at all (…) determined unilaterally by the authorities”, whereas another said, “I actually don´t know how they do that [the determination of the taxes and their size]: If the state could say, in those negotiations: “Now, we will focus on older people and depression. We will increase that tariff”.
Finally, some respondents with competence in law and/or for whom law was a particularly important part of their work, mentioned the possibility of enforcing the structural aspect of the Equality and Anti-Discrimination Act in the face of the relevant forms of institutional ageism. An enforcement officer said that knowledge about the potentially ageist outcomes of the tariff and control systems should perhaps trigger the legal “activity obligation” established by the Equality and Anti-Discrimination Act. He said in this connection, “that’s actually something that we in our capacity as agents of change should keep in mind – I definitely think that’s something that we should address”.
Discussion
It is perhaps not self-evident that cultural beliefs and their strength can impact on the extent to which legislation is used to prevent discrimination and/or reduce inequality. However, inspired by the sociologist Robin Stryker, our discussion below takes as its point of departure that it can. 85 Below we will therefore discuss what those cultural beliefs may be that underpin the perceptions of systems-level stakeholders outlined above. Then we will briefly discuss the possible implications for legislation and its function under welfare state transformation, of the web of underlying cultural beliefs that we may see the contours of here.
Institutional ageism and the role of belief systems
This study highlights how perceptions of institutional ageism in Norwegian GP services appear shaped by a complex web of cultural beliefs. These beliefs may influence how systems-level stakeholders interpret potential institutional ageism in GP services and their own roles in monitoring, sanctioning and preventing it. The effectiveness of legislation in reducing inequality depends not only on legal frameworks but also on the cultural beliefs that support or undermine them. 86
One dominant belief on the systems level appeared to be in the intactness and good intentions of the Norwegian welfare system. Some stakeholders expressed trust in the Norwegian health care system and GP scheme despite personal experiences or qualitative data suggesting they may disadvantage older adults with MH/SA needs. This may reflect what the organizational theorist Nils Brunsson calls the “localization strategy,” where established beliefs persist even when contradicted by experience. 87 For example, stakeholders often interpreted incidents potentially caused by structural disadvantages—such as by the economic incentives embedded in the GP tariff system—as isolated incidents rather than systemic problems. Such trust may contribute to inertia, preventing recognition of institutional ageism and delaying corrective action.
Conversely, some stakeholders recognized that the GP tariff system, along with its reliance on patients’ verbalized needs, may systematically disadvantage older adults. They noted that the system incentivizes short consultations, which can be particularly problematic for older patients who often require more time. At the systems level, this perception was linked to a sense of responsibility to implement corrective measures—such as tariff reforms, clinical guidelines, or the development of primary health teams—to promote more equitable access. However, suggestions about which measures could or could not be adopted also appeared to reflect underlying beliefs. Some measures, such as fixed salaries or radical changes to the tariff system, were dismissed due to concerns about financial cost and productivity. This tendency to prioritize cost-saving and efficiency—even when acknowledging that certain reforms could improve age-based equity—suggests a tension between values. On one hand, this could reflect cultural beliefs in fiscal responsibility. On the other, it may reveal ageist assumptions about the financial sustainability of the healthcare system in light of demographic changes.
The structure of Norwegian GP services places significant responsibility on patients to initiate contact and articulate their health concerns. This expectation is embedded both formally—through regulations that allow GPs to charge only when a patient has actively sought care—and informally, through cultural norms that frame help-seeking as a matter of individual autonomy. While this model aligns with liberal values such as freedom from prejudice and paternalism and respect for autonomy, it may inadvertently disadvantage older adults with MH/SA problems. These individuals are for various reasons often less likely to verbalize their needs. 88 As a result, their health issues may go undetected and untreated, not because of intentional ageism, but because the system is structured in a way that privileges verbal self-assertiveness. This reliance on patient-initiated contact thus may be seen to constitute a form of institutional ageism, where seemingly neutral practices produce unequal outcomes for older adults.
While most stakeholders did not consider the deprioritization of non-verbalized health needs to be legally discriminatory, some nuances emerged. One respondent gave a hypothetical scenario - where a person is drowning but does not call for help – that was used to illustrate how legal responsibility may shift under certain conditions. If specific criteria are met, such as the acuteness and seriousness of the situation, a clearly defined responsibility on the health provider´s part to provide care could, according to this interpretation, possibly prevail. Based on the hypothetical scenario´s content, other potentially relevant criteria seemed to be geographical proximity between the healthcare professional and patient, and the provider’s awareness of the patient’s disability. Although the respondent did not connect this line of reasoning directly to any legal provision, the line of reasoning implied here is interesting. It could be interpreted as a reference to, among others, section 8 of the Equality and Anti-Discrimination Act about indirect differential treatment. 89 In that case, it indicates that there may be some situations where the responsibility to initiate care may fall on the healthcare professional rather than the (older and verbally non-self-assertive patient). Neglecting to offer older MH/SA patients health assistance due to their “failure to shout” could, in certain exceptional cases, possibly be discriminatory according to the law, according to such an interpretation.
Perception of role, and of role related to legislation – in the face of potential institutional ageism
The study reveals that systems-level stakeholders often interpreted the relevant forms of potential institutional ageism as falling outside the scope of legal discrimination. Thus, the currently accepted legal interpretation limits the applicability of the Equality and Anti-Discrimination Act. Several systems-level stakeholders conveyed the perception that it was possible to monitor, sanction, and prevent the relevant forms of institutional ageism in GP practices. However, they also said that if they were to do that, they would often need to receive specific types of reports indicating a need for it. Among the enforcement agencies, the perception seemed to be that these reports should come from the patients themselves (or care partners). This resonates with findings from a previous study 90 where Norwegian State Administrators described their enforcement work as “governed by the ones who complained”. This led to the marginalization of older people´s MH as a topic to the State Administrators’ enforcement work related to healthcare legislation. Basing these agencies’ work on incoming complaints may perhaps appear like a reasonable approach to discovering these assumed exceptions, especially if combined with liberal beliefs that make human beings emerge as rational, autonomous individuals. But, it does not appear unreasonable to expect that the ones who lose out as a result of this “regime” may often be the ones with least resources, and thus in the weakest position, but perhaps the strongest need of help from enforcement agencies.
Policies that require individuals to self-report their own discrimination may result in underreporting. Ageist beliefs or stereotypes may be internalized and/or embedded in social schemas fostering age-based disparities. Low numbers of complaints from older MH/SA patients could reflect internalized or self-directed ageism of one´s own deservingness. Additionally, systems-level agencies’ failure to monitor, sanction or prevent institutional ageism of relevance to those uninclined to complain may reflect underlying belief in the generalizability or superiority of behavioral patterns or concerns that are more common among the young. The latter interpretation may also shed light on one enforcement agency´s experience with some older people complaining about age discrimination in working life but not in healthcare. This could have been interpreted as a likely result of beliefs rooted in an ageist social schema. These beliefs could for instance imply that arenas of importance to many older people, such as healthcare, are unimportant, whereas arenas of importance to many young people, such as working life, are important. Either way, enforcement agencies’ dependence on complaints to trigger action means that, as older adults may be less inclined or less able to report complaints, detection of ageism is as unlikely as the sanctioning or implementation of corrective measures to monitor, sanction or prevent institutional ageism.
These findings raise questions about how enforcement mechanisms might be strengthened to address institutional ageism. One possibility is that enforcement agencies could consider the possibility of acting in this field despite a lack of individual complaint. For example, the Long Term Care Ombudsman Program in the United states monitors quality through in-person observation, addresses systematic barriers to quality of care as well as individual complains, and accepts both patient initiated and ombudsman initiated complaints. 91
Although enforcement agencies are designed to serve as structural safeguards against age discrimination, our findings suggest that perceptions there about prioritization may reflect a belief system that values arenas typically associated with younger populations—such as working life—over those more relevant to older adults, like healthcare. Thus, it is possible to interpret the relevant stakeholder´s perception of his agency´s role in this field as informed by institutional ageism, possibly merging with a traditionally strong Norwegian welfare state belief in the value of labor market participation. 92 In the Norwegian context, high employment rates are seen as essential to sustaining the welfare model. This belief may inadvertently influence enforcement agencies to concentrate their efforts on protecting equality in employment, while overlooking systemic inequalities in healthcare access for older adults. A likely result may be that the structural protections intended to prevent ageism—particularly in MH/SA services—are rarely activated. The consequence could then be a pattern of social inertia, where ageism in healthcare is neither monitored, sanctioned or prevented, despite its prevalence and impact.
Some systems-level stakeholders explained that they could have monitored, prevented or sanctioned ageism in GP services despite lack of individual reports. This would, however, have required them to gain access to authoritative knowledge that indicated a need for them to act. However, as noted in the background and findings section, government and research funding agencies may prioritize RCTs and measurable outcomes over knowledge development about normative and legal issues. This perspective may be rooted in belief in the superior value of knowledge about models, medicines and measures capable of solving (what is framed as) a sustainability challenge, and/or in the subordinate value of knowledge about moral and legal issues like ageism and age discrimination. This finding may reflect deeper beliefs about what constitutes “valuable” knowledge—beliefs that deprioritize ageism as a research topic and hinder systemic change. Such beliefs may in turn be associated with the “localization strategy”. If believing in the intactness of the basic normative and legal structure of the welfare state, it may appear wasteful to prioritize knowledge development about discrimination within this structure. 93 In turn, the power of such beliefs about knowledge may be accentuated by other underlying beliefs impacting on research funding systems, like the potentially ageist belief in the threatened financial sustainability of the healthcare system caused by demographic change. This belief may also make it appear reasonable to spend resources on research projects that set out to develop the technological, organizational and medical innovations that can perhaps solve the (alleged) sustainability challenge. A consequence of this may be that the system-level agencies will never, or only to a limited extent, obtain the authoritative knowledge they consider themselves to need (in the absence of individual reports) to monitor and prevent institutional ageism, or perhaps to sanction it as age discriminatory according to the law.
Potential for change?
Another finding about role perception concerned the possibilities, on systems level, for changing or abolishing the tariff and control system to promote age-based equality. One stakeholder from a government agency noted that the COVID-19 pandemic had enabled national authorities to implement changes to the tariff system that would otherwise have been difficult. This observation implies that technically and legally speaking, the national authorities could still have made bold decisions about the tariff system in pursuit of the political goal of equality. However, the fact that such action was perceived as contingent on an exceptional and “extra-political” force like a pandemic suggests that this avenue is not currently seen as viable. This perception, voiced by several respondents, appears to be related to and nourished by perceptions about the tariff system being the result of negotiations. Consequently, the tariff system was perceived to require a cautious approach from national political leadership, despite its central importance to the widely shared political goal of ensuring age-based equality in access to healthcare.
The political authority that, technically speaking, could have been used to protect equality seems here to give way to a negotiation-based decision-making process. In this process, stakeholder organizations, like the Medical Association, appear to be offered decision-making roles equivalent to that of the democratically elected government. This partial abdication on the government´s part may be seen to reflect underlying beliefs in ideals associated with the prevailing New Public Governance paradigm, like in “co-production” and “co-creation”. As commented earlier in this article, this paradigm has been criticized for its willingness to negotiate goals with stakeholders who are not democratically elected, hereby possibly undermining concerns for the whole of society. 94 As a result, the authorities may face restricted possibilities for radically changing the tariff system in order to enable older MH/SA patients, among others, to gain more equal access to GP services.
Another perception surging from the interviews concerned the impossibility of substituting the tariff system with a system with fixed salaries for GPs, to promote more equal access to GP services for older MH/SA patients. This view was often accompanied by an implicit belief that equality-promoting measures must be sacrificed if they are financially too costly or present challenges to the ideal of productivity (according to a given understanding of productivity). While this may reflect a commitment to values like fiscal responsibility, it could also signal a potentially ageist belief in the threatened financial sustainability of the healthcare system as a result of demographic change. This may make it appear fair that older adults accept poorer healthcare services, which normalizes the idea that older adults should accept poorer healthcare services.
Some perceptions surged from interviews with those respondents who were educated in law or for whom law was particularly salient in their agencies’ work. One such perception was that it is difficult or impossible to sanction the potential forms of institutional ageism as illegal or age discriminatory according to the law. However, respondents acknowledged the possibility of invoking the structural provisions of the Equality and Anti-Discrimination Act. Some stakeholders suggested that knowledge about institutional ageism could activate the Act’s “activity obligation,” requiring public authorities to promote equality proactively.
Recognition of institutional ageism was occasionally accompanied by suggestions for reform, such as introducing new tariffs or expanding primary health teams. Yet, some of these proposals were dismissed due to concern about productivity and cost—concerns that may themselves be rooted in ageist beliefs about demographic threats to healthcare sustainability. The interviews with participants in government agencies seemed to reveal a slightly different perspective on proactivity versus reactivity in GP services than the one where proactivity is considerered a potential threat to liberal values like autonomy and freedom from prejudice. Although age discrimination was not explicitly thematized in interview with government agency stakeholders, their references to “primary health teams” suggested support for more proactive approaches to non-verbalized patient needs. Notably, their proposed measure for higher proactivity was not necessarily that GPs should become more “proactive”. Instead, proactivity was to be achieved by the introduction in GP services of other, more lowly waged professional groups. This may reflect adaptation to financial restraints, which in turn could be informed by a potentially ageist belief in the unsustainable burden of older adults on the healthcare system.
Implications for legislation and policy
Some of the above-mentioned beliefs appear rooted in ageist social schema. Among these we find beliefs in older people´s arenas and patterns of behavior as being subordinate to typical younger people´s arenas and patterns, and beliefs in the threats from demographic change to the financial sustainability of the healthcare system. Other beliefs appeared associated with the localization strategy, and with assumptions about and values related to the Norwegian welfare state. Among these we find beliefs in the intactness of the normative structure of the universalistic welfare model, making it appear natural to see and treat empirical examples of unjustified age-based inequality as trivial exceptions to a general rule. We also find beliefs about the value of labor market participation. Moreover, there are beliefs reflecting a concern for traditional liberal values like freedom from prejudice, respect for individual autonomy, non-intervention and skepticism to paternalism. Finally, we appear to find beliefs in co-creation and co-production rooted in the prevailing governance paradigm New Public Governance.
Taken together, these findings suggest that equality-oriented legislation may currently serve more as symbolic protection than as a mechanism for protection of equality in access to healthcare. The structural and cultural conditions surrounding GP services—economic incentives, liberal values of independence and autonomy, governance models, and research priorities—limit the law’s capacity to prevent institutional ageism in healthcare to older MH/SA patients. A web of underlying, partially interconnected cultural beliefs inform the perceptions on systems level of potential forms of institutional ageism affecting older MH/SA patients in GP services. These beliefs also inform the perceptions of systems-level stakeholders of their agencies’ role related to them. This web of beliefs may have important implications for how institutional ageism in healthcare is monitored, sanctioned and prevented on systems level in Norway, and for the factual scope of the law. Based on the findings presented in this article it appears unlikely that the potential forms of institutional ageism will be sanctioned as illegal or age discriminatory according to the law. It appears unlikely that equality-oriented legislation is applied as any kind of brake to slow the equality-eroding transformation of the welfare state. In many ways then, anti-discrimination legislation appears likely to serve as “paper law” related to older MH/SA patients in the GP scheme, possibly legitimizing systems level inertia related to transformation. 95
The findings do, however, indicate that this might change with time depending on the choices that are made on policy level, as well as on the direction of the societal and ideological development. If systems-level agencies were to prioritize knowledge development about moral and legal issues like age discrimination and age-based inequality, and if enforcement bodies adopted more proactive approaches, legislation could become a more relevant tool. This would require challenging dominant beliefs, including those about autonomy, fiscal sustainability, and the deservingness of older adults.
It could also depend on choices made in those systems-level agencies where legislation is most explicitly present, as in the National Board of Health Supervision (which was not part of this study), the Discrimination Tribunal and the ombudsman apparatus.
Limitations
Our sample includes only seventeen systems-level stakeholders. Although the potential sample of enforcement officers and other systems’ level stakeholders is limited, additional participants would strengthen the generalizability of our findings. Unfortunately, we were unable to recruit participants from the National Board of Health Supervision, represented by the Regional Governors, one of the most important systems-level agents in the field of study. It is also important to stress that our findings do not allow for conclusions about how the perceptions described in interviews reflect actual practices or services on systems level.
Conclusion
Our findings show that current interpretations of the Equality and Anti-Discrimination Act and the Health and Care Services Act, and current political prioritizations, may not indicate that these laws are used to counteract potential institutional ageism affecting older MH/SA patients in the Norwegian GP scheme. Despite the existence of legal protections, the findings suggest that these frameworks are interpreted in such ways that older MH/SA patients’ needs are often unlikely to be heard. A web of underlying cultural beliefs seems to contribute to that, informing perceptions on system level of practices, roles and change in such ways as to make systems level inertia related to age-based equalities appear a likely outcome. These beliefs—rooted in assumptions about autonomy, productivity, and the financial sustainability of the healthcare system—appear to limit the capacity of legislation to function as a corrective mechanism.
Given the backdrop of general equality-eroding transformation, it does not appear unlikely that legislation serves a legitimizing function currently for such inertia. This interpretation is particularly thought-provoking given the recognition of the inadequacies of the GP scheme in terms of services to older MH/SA patients, 96 and the expected increase in the population of older people in need of MH/SA services in years to come. If these cultural beliefs remain unchallenged, we may in years ahead witness an increase in institutional ageism in Norwegian GP services possibly forming part of a general equality-eroding welfare state transformation.
Legislation is not the only possible route to age-based equality for MH/SA patients in the GP scheme. While legal frameworks provide important structural protections, our findings suggest that broader systemic measures may require complementary strategies. The national and local authorities could opt for other approaches as well, rooted in alternative beliefs to the ones that currently appear dominating, or in alternative interpretations of these beliefs. Rather than relying on beliefs associated with the “localization strategy”, 97 age-based equality in healthcare could be seen and treated as a potentially threatened value. This would entail recognizing that structural ageism may persist despite formal legal protections, and that proactive measures may be needed to counteract it.
Rather than relying on potentially ageist beliefs about the need to de-prioritize age-based equality due to the threatened financial sustainability of the health care system, the pursuit of age-based equality could be prioritized despite the short-term costs it could imply. This shift could require a reorientation of policy and resource allocation, also in views about research and service design. Dominant research funding organizations could acknowledge the need to prioritize knowledge development about equality and other moral and legal values. Similarly, national governments could choose to make bold decisions aiming for the fulfillment of the democratically based goal of age-based equality in healthcare. Enforcement agencies and other systems-level stakeholders could also choose to look for and develop approaches better suited for capturing the needs and interests of verbally less self-assertive patients. In the case of such a scenario, equality-oriented legislation would not necessarily be seen so easily as “paper law” legitimizing inertia related to equality-eroding transformation. Instead, it could become a more dynamic tool for equality, embedded within a broader ecosystem where equality - in healthcare as elsewhere - is protected.
It remains uncertain which of the trends outlined will translate into concrete policy and practice. Much will depend on choice and prioritizations across sectors. A recent example from Norway illustrates the current policy ambivalence and the significance of such choices. In April 2025, a white paper on national prioritization guidelines for the municipal health and care sector 98 was published. It details the process by which criteria for service prioritization were established. Notably, the Ministry of Health and Care decided to exclude productivity-related societal effects (e.g. a patient’s ability to return to work) from these criteria, despite the majority of the expert panel recommending their inclusion in some cases. Given that older adults are less likely to return to work, this decision may reflect an effort to protect age-based equality. On one hand, this suggests that Norwegian authorities are willing to make decisions in favor of equity. On the other hand, it highlights the strength of competing pressures, including economic and productivity concerns, as well as prevailing ageists beliefs even among experts. This tension suggests that ageist beliefs and their policy implications will continue to pose challenges in the years ahead, but that a strong welfare state foundation and commitment to equality may play a protective role.
In conclusion, it is possible to choose inertia related to ongoing equality-eroding transformation in Norwegian welfare systems. However, it is also possible to choose an approach hinted at by one of our respondents, when confronted with findings about potential institutional ageism in the GP scheme, “That’s actually something that we in our capacity as agents of change should keep in mind – I definitely think that’s something that we should address”.
Footnotes
Acknowledgements
We appreciate our ROMEO project colleagues for their valuable insights, the interview subjects who have been generous with their time and perspectives, and Professor Carola Lingaas at VID Specialized University, for her invaluable legal assistance and editing.
Ethical considerations
Approval for human subject research was received from the Norwegian Agency for Shared Services and Research (reference code 598740) for the ten interviews that implied registration of personal data. Seven interviews did not imply registration of personal data, and it was clarified with the Norwegian Agency for Shared Services and Research that approval was not required.
Consent to participate
All participants were informed about the study and provided consent to participate.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Council of Norway under grant number 286611.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.