
Abstract
Aim
Investigate the role of mobile stroke unit (MSU) and rendezvous transport with emergency medical service (EMS) in timely large vessel occlusion (LVO) identification and direct transfer to the comprehensive stroke center.
Methods
The fifth-generation MSU (5G-MSU) program was first implemented in 2019, directly dispatched through the 120 emergency medical services. The rendezvous transport was initiated in 2020. We report the first case of rendezvous transport plus prehospital computed tomography angiography (CTA) on 5G-MSU for endovascular treatment of LVO.
Results
A 5G-MSU was dispatched for a patient with reported right-sided hemiparesis and reduced consciousness at a primary stroke center, located at a distance of 106 km. The 5G-MSU and EMS coordinated a rendezvous transport to transfer the patient. CTA performed on the 5G-MSU revealed basilar artery occlusion, prompting immediate contact with the main hospital's angiography suite. Upon arrival, the patient was directly transferred to the angiography suite for endovascular therapy, achieving successful recanalization. Consequently, the call-to-puncture time was successfully achieved within 103 min, across a distance of 106 km.
Discussion
Rendezvous transport combined with prehospital CTA on the 5G-MSU in rural areas is feasible. This approach allows the MSU to extend beyond its conventional treatment coverage, rapidly identify large vessel occlusions, and thereby significantly reduce call-to-treatment time.
Introduction
For patients with large vessel occlusion (LVO), endovascular treatment (EVT) currently represents the most effective reperfusion approach,1–5 where earlier recanalization significantly improves clinical outcomes. 6 Computed tomography angiography (CTA) serves as the pivotal diagnostic tool for LVO identification and subsequent EVT decision-making. 7 The critical challenge in stroke emergency care lies in achieving rapid prehospital LVO recognition and ensuring timely transfer to comprehensive stroke centers (CSCs) capable of thrombectomy.8–11
The fifth-generation mobile stroke unit (5G-MSU) is an advanced ambulance equipped with a compact 16-slice computed tomography (CT) scanner, laboratory testing devices, monitoring equipment, and a 5G-enabled telemedicine system. It supports real-time remote consultation with hospital specialists, enabling prehospital CTA to identify LVO and streamlining direct transfer to the angiography suite upon hospital arrival. Consequently, it effectively eliminates in-hospital CTA-related delays in EVT initiation. 12
From 2017 to 2025, 29 5G-MSUs were established. Notably, all 29 operational 5G-MSUs are primarily deployed in urban areas. For rural regions with limited medical resources, preserving therapeutic time windows through efficient patient transfer is critical. 13 The innovative rendezvous transport addresses this challenge by 5G-MSU can meet standard emergency medical service (EMS) transporting stroke patients from beyond the conventional MSU service area en route to the stroke center. This paradigm doubles the range of operations and the number of patients treated by an MSU in an urban area, significantly improving timely stroke care in underserved rural areas. 14 We report the first case of integrating rendezvous transport with prehospital CTA on a 5G-MSU for LVO diagnosis and treatment.
Methods
The 5G-MSU was officially commissioned on 30 September 2020. The 5G-MSU is staffed with a neurologist, an emergency nurse, and a driver. The CTA capability was added to the 5G-MSU on 15 March 2025. Once the nonenhanced CT of the brain and neurological assessment are completed, the neurologist on board may be instructed to proceed with a CTA if findings are suggestive of a suspected LVO by the vascular neurologist performing the telemedicine evaluation. Suspected LVO criteria of an NIH Stroke Scale/Score (NIHSS) ≥ 6, fluctuation of symptoms, a single focal deficit that may suggest LVO, and hyperdense vessels on non-contrast CT. And after verifying the absence of contraindications for the use of contrast agents, including assessments for allergies, hyperthyroidism, recent metformin use within the past 48 h, and renal failure (by point-of-care creatinine measurements), the onboard neurologist will be instructed to perform a CTA.
The following parameters were used for non-contrast CT scans: voltage, 120 kV; scan current, 8 mA; slice thickness, 4.4 mm. The parameters for CTA were as follows: 80 mL of nonionic contrast agent, injected at a rate of 4.5 mL/s, with a delay of 16 s; helical scan, 120 kV, 8 mA, 1.1 mm. With a 5G network, the images are transmitted to the hospital within 5 min. The radiologist performed image reconstruction, while the vascular neurologist interpreted the images and formulated treatment decisions based on the findings.
Results
5G-MSU was dispatched for reported right hemiparesis and reduced consciousness in a 64-year-old male with a history of hypertension, diabetes, and smoking. His symptoms began at 12:00 with persistent dizziness, and were subsequently accompanied by vomiting of coffee-ground emesis. He presented to a primary stroke center (106 km away from the main hospital) at 17:00, where a non-contrast CT demonstrated hypodense lesions in the bilateral occipital lobes (Figure 1(a)). Intravenous thrombolysis was not administered. His symptoms include progressive neurological deterioration, manifesting as right-sided hemiplegia and reduced consciousness. At 20:04, an urgent call was made to the 5G-MSU, and a rendezvous transport was employed. The EMS and 5G-MSU coordinated to meet and transfer the patient. The 5G-MSU successfully rendezvoused with the EMS and took over the patient at 20:43.
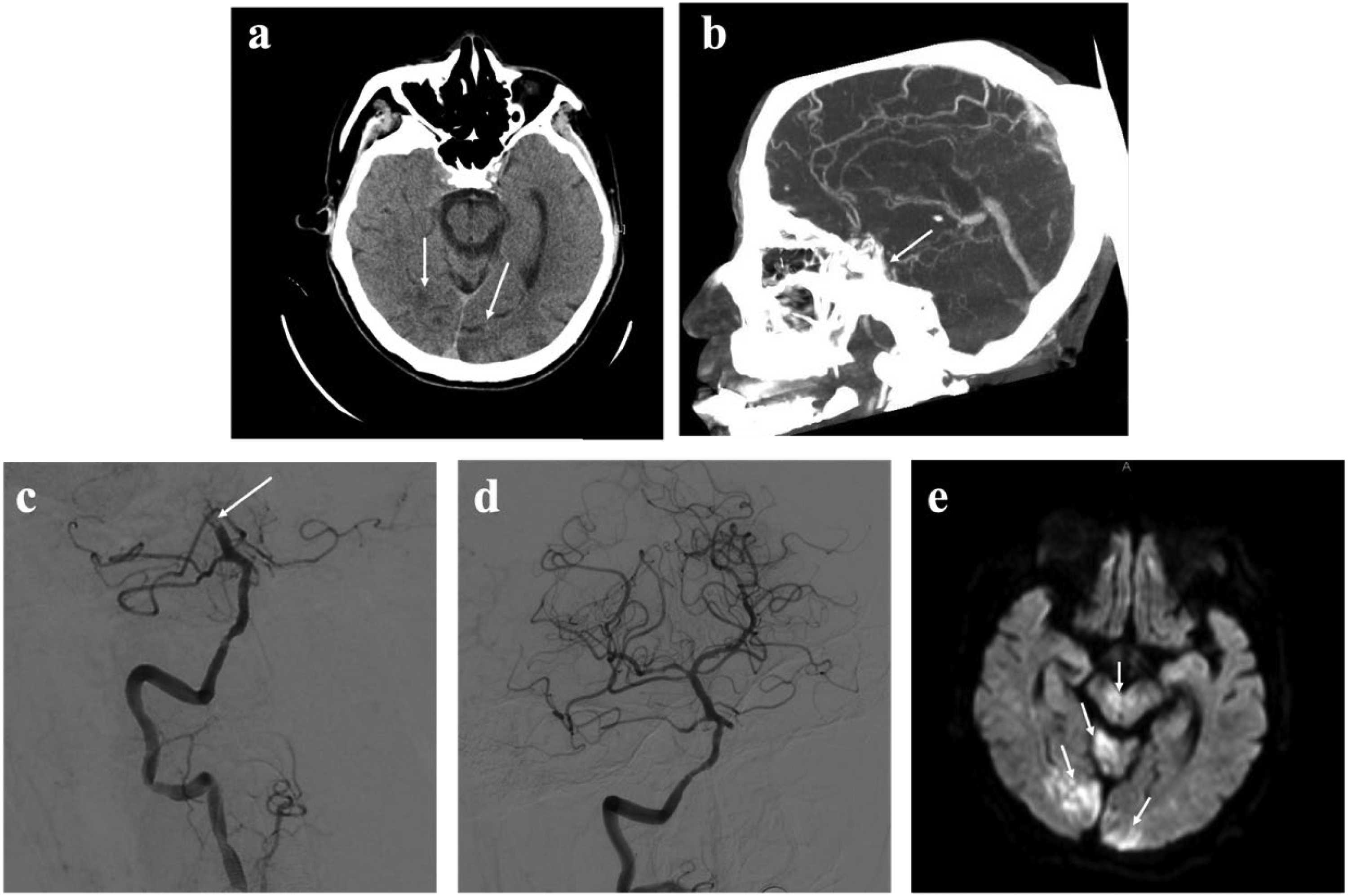
Baseline CT in the primary stroke center (a) demonstrated hypodense lesions in the bilateral occipital lobes (arrow). Mobile CTA (b) showed basilar artery thrombosis (arrow). Pre- (c) and postintervention (d) digital subtraction angiography images showed occlusion of the basilar artery (arrow), with subsequent recanalization in cerebral infarction 2b grade. Axial-diffusion-weighted images from the acute MRI (e) show restricted diffusion in the bilateral occipital lobes, cerebellum, and midbrain (arrow).
Upon neurological examination, the patient was comatose with anisocoria (left 4 mm with an absent pupillary light reflex, right 2 mm), absent spontaneous limb movements, and only reflexive activities (NIHSS score, 35; Glasgow Coma Scale score, 8). The MSU-CTA image (21:00) revealed occlusion of the basilar artery (Figure 1(b)). Then the imaging data were transmitted to the hospital via the 5G network (21:04). Following a multidisciplinary teleconsultation with in-hospital stroke specialists, the angiography suite was immediately activated.
Upon arrival at the main hospital (21:17), the patient was immediately transferred to the angiography suite (21:20). He underwent endovascular therapy (groin puncture at 21:47), during which successful recanalization of the completely occluded basilar artery was achieved (22:25) (Figure 1(c) and (d)). Figure 2 illustrates the patient treatment timeline. On postoperative day 5, axial diffusion-weighted images from the magnetic resonance imaging (MRI) showed restricted diffusion in the bilateral occipital lobes, cerebellum, and midbrain (Figure 1(e)). By postoperative day 12, the patient was discharged, exhibiting somnolence, right-sided hemiplegia, and dysarthria (NIHSS score 10).
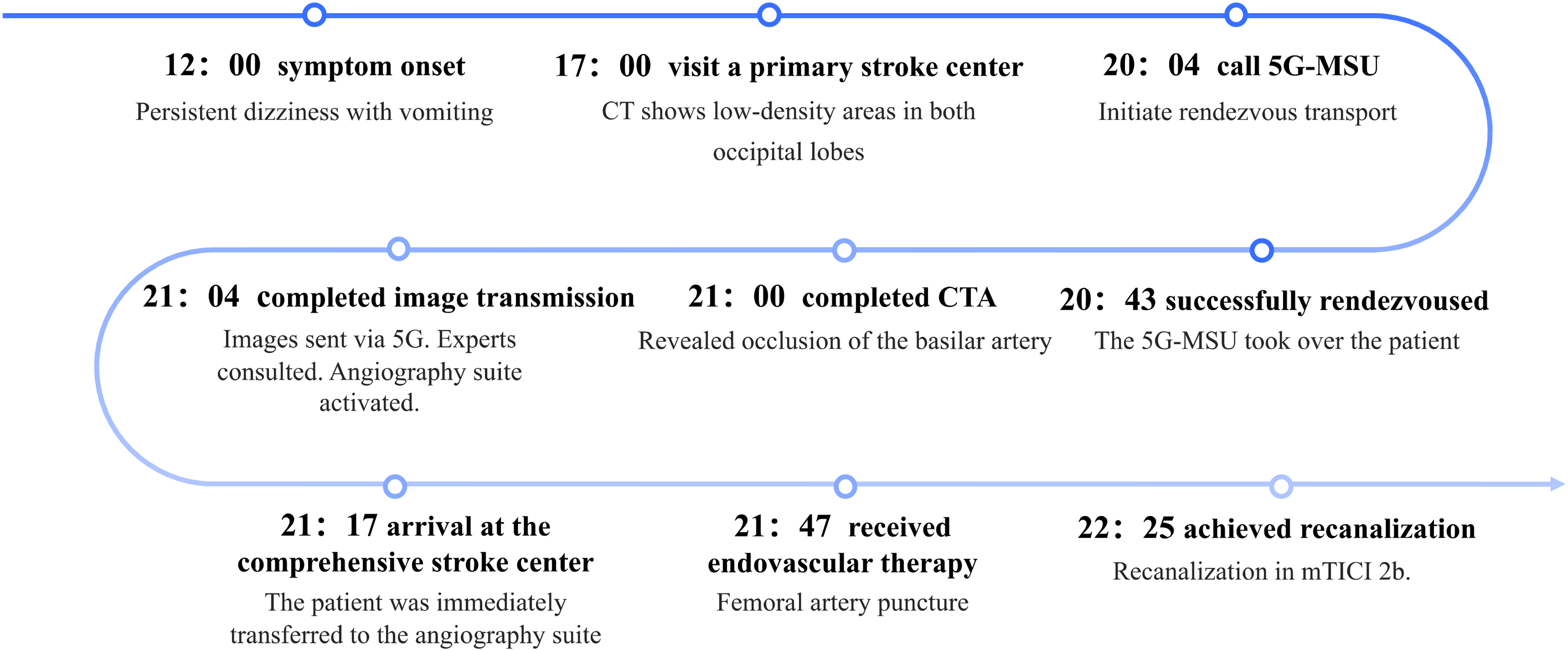
Patient treatment timeline.
Discussion
In this study, we successfully achieved the first case of rendezvous transport combined with prehospital CTA on a 5G-MSU for LVO, reaching a call-to-puncture time of 103 min over a distance of 106 km. Prehospital CTA significantly reduced the time from hospital arrival to puncture, while rendezvous transport minimized the time from call to MSU arrival. In stroke treatment, time is brain, as any time saved can potentially translate into improved neurological outcomes for patients.15–17 Therefore, optimizing the stroke emergency process and minimizing unnecessary delays are essential for improving patient outcomes.
In this study, with a 106-km distance between the two hospitals, the rendezvous transport system enabled a call-to-MSU arrival time of just 39 min, far quicker than the time required for direct MSU transport. In Hinggan League, which covers an area of 60,000 km2 and has only one CSC, the CSC is equipped with only one MSU (Figure 3). The conventional treatment radius of an MSU is 20 km. The rendezvous transport system significantly expanded the coverage area of the MSU. 14 In China, low thrombolysis (5.64%) and thrombectomy (1.45%) rates are primarily attributed to prehospital delays, with only 11.8% of patients arriving at the hospital within 3 h of symptom onset. To address this challenge, we propose a “1-h golden time rescue circle” strategy, aiming to achieve call-to-needle time within 1 h for patients within 3 h of symptom onset. This involves direct MSU dispatch for cases within 20 km and rendezvous transportation for distances over 20 km (Figure 4). The innovative rendezvous process between the MSU and rural EMS agencies effectively bridges the gap in stroke care in rural communities, reducing the disability and mortality rates of rural stroke patients caused by delays and optimizing the utilization of patients, institutions, and EMS resources. 18
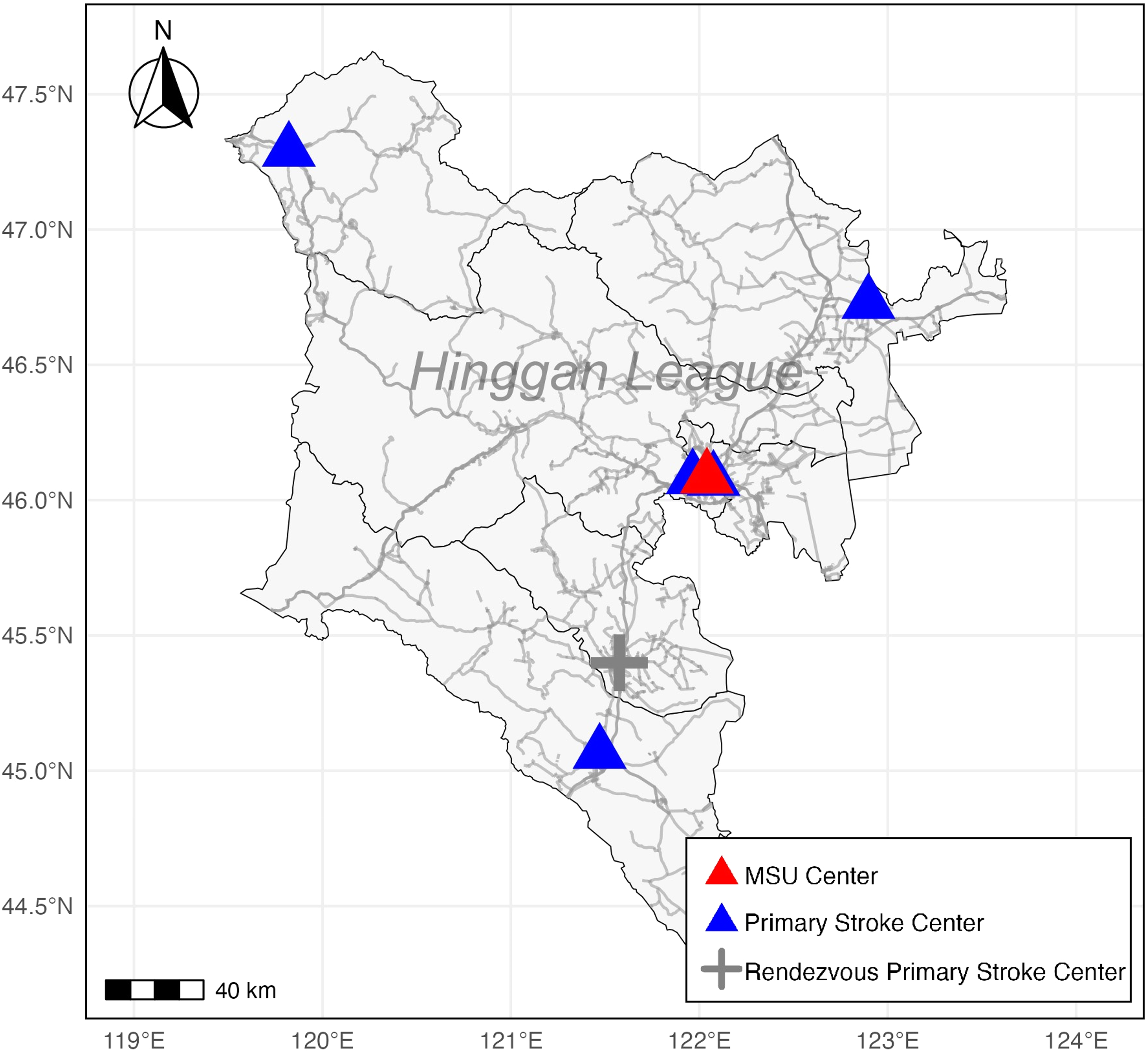
Route map of primary stroke centers, rendezvous primary stroke centers, and mobile stroke unit (MSU) centers in the Hinggan league.
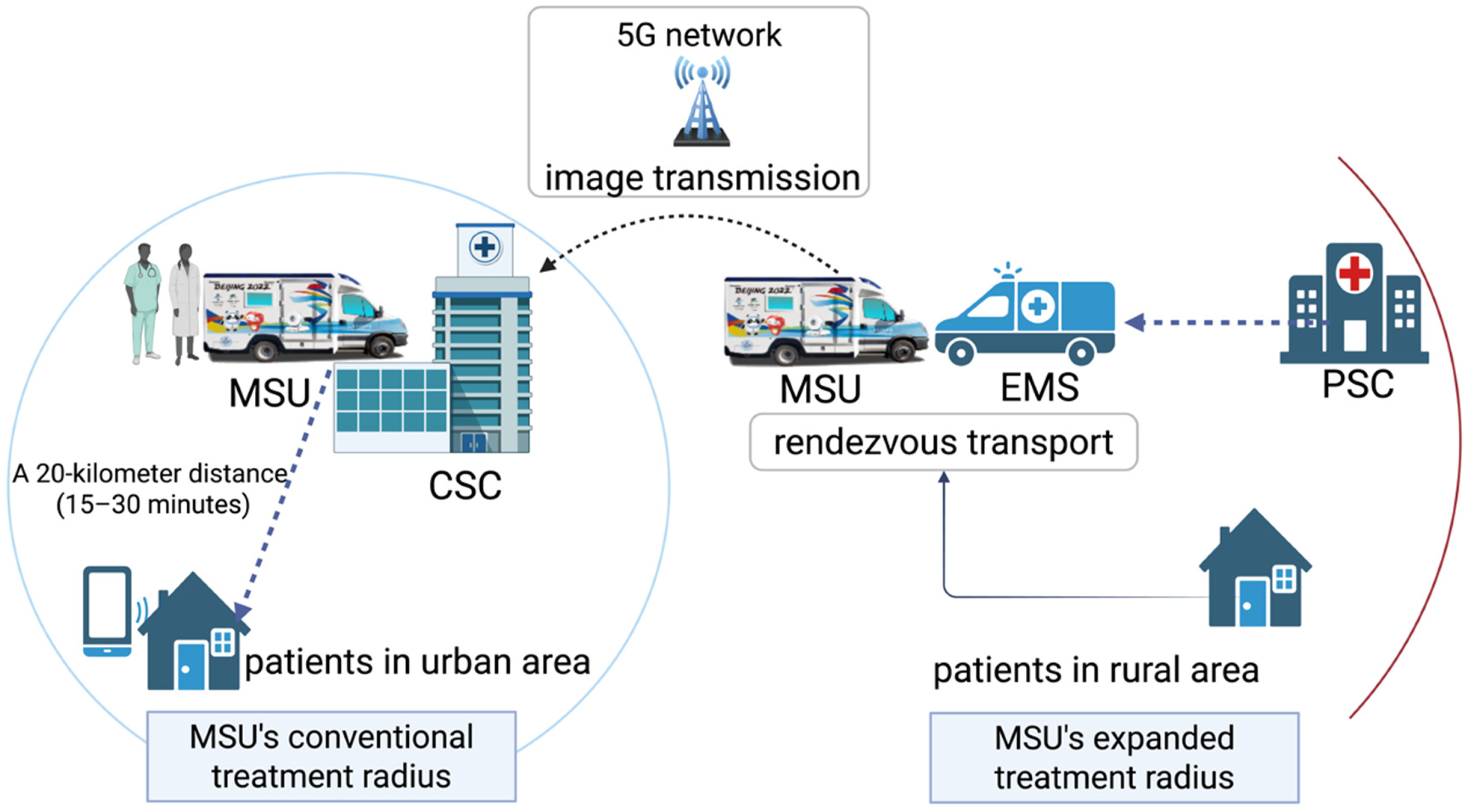
Schematic of the 1 h golden time rescue circle.
Our study demonstrated that performing CTA on the MSU is feasible and effective. Upon arrival at the hospital, the patient was directly taken to the angiography suite, attaining a door-to-puncture time of 30 min. The Benefits of Emergency Stroke Treatment using a MSU substudy indicated that CTA performed on the MSU can substantially reduce door-to-puncture time by approximately 1 h. 19 Additionally, unlike the traditional model of sending patients with unknown causes to the nearest hospital, performing CTA at the emergency site helps to reasonably triage patients with extensive cerebrovascular disease. 20 For patients with LVO, prehospital CTA enables the MSU team to directly transfer patients to CSCs for EVT. For patients with hemorrhagic stroke, the “spot sign” detected by CTA indicates ongoing hemorrhage enlargement, which is an unfavorable prognostic marker and supports decisions regarding neurosurgery or neonatal intensive care unit care at the CSC. 21 For patients with subarachnoid hemorrhage, prehospital CTA can immediately determine the etiology, ruptured aneurysm. 22
Our country has developed the world's largest 5G network, surpassing all others in scale and coverage, with a total of 3.748 million 5G base stations, covering all administrative villages. Additionally, 29,000 5G industry virtual private networks have been constructed. 23 This infrastructure makes 5G mobile stroke management highly promising. However, in this case, the data transmission speed was comparatively slow (an average speed of 1.12 MB/s), primarily due to the remote location of the transmission site from the nearest 5G base station.
The success of the rendezvous model relies not only on technological advancement but also on seamless coordination between referring physicians and the MSU team. To fully leverage the time-saving benefits of prehospital CTA and rendezvous transfers, it is essential to educate healthcare providers at primary stroke centers and emergency medical services within the catchment area regarding the indications and activation protocols for MSU deployment. Key educational priorities include the recognition of clinical signs highly suggestive of LVO, understanding the time-sensitive nature of endovascular thrombectomy (EVT), and familiarization with rendezvous logistics. In regions where CTA is not routinely available, MSU medical directors should develop and disseminate standardized educational programs and activation pathways to facilitate timely and appropriate deployment of MSU resources. This approach enhances the likelihood of delivering reperfusion therapy within the therapeutic window, thereby improving clinical outcomes.
Regrettably, this patient's outcome was poor, primarily due to the prolonged onset-to-call time (>8 h), which exceeded the therapeutic window. Thus, this case serves as a proof-of-concept for the process feasibility. For patients identified earlier, this protocol could translate time savings into meaningful recovery. Additionally, we found that even with 5G transmission, CTA imaging still took 4 min to transfer. But this did not affect subsequent patient treatment. China's network advantages have not been fully utilized and need to be enhanced to ensure the efficient and secure transmission of patient data and medical images through a dedicated medical network.
Conclusion
The rendezvous transport for patients in rural areas, combined with prehospital CTA on the 5G-MSU to rapidly identify LVO and be directly transferred to the angiography suite, is feasible. This represents the optimal model for patient care in regions with limited medical resources, which significantly reduces the time from call to treatment. Further experience is needed to explore the feasibility of routine use of this new protocol.
Footnotes
Ethical considerations
This study was approved by Xuanwu Hospital, Capital Medical University ethics committee (Approval Number: [2024]288, Approval Date: 11 September 2024).
Consent to participate
The patient signed an informed consent for participation in the study and authorized the publication of the article.
Consent for publication
The patient has provided written informed consent for publication of their data in this study. The consent form has been retained in the patient's hospital record in accordance.
Authors’ contributions
All authors contributed to the study conception and design. LW and XHG drafted and revised the manuscript for content. All authors have read and approved the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Science and Technology Major Project (2023ZD0503806), National Nature Science Foundation of China (82171302), and Capital's Funds for Health Improvement and Research (2024-1-2011).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data collected for the study may be made available from the corresponding author to others upon reasonable request.