
Abstract
Introduction
The COVID-19 pandemic has instigated the development of telemedicine-mediated provision of medications for opioid use disorder such as buprenorphine and methadone, referred to as TMOUD in this study. As services start to return to pre-pandemic norms, there is a debate around the role of TMOUD as addition to or replacement of the conventional cascade of care for people with opioid use disorder (PWOUD). This scoping review is designed to characterize existing TMOUD services and provide insights to enable a more nuanced discussion on the role of telemedicine in the care of PWOUD.
Methods
The literature search was conducted in OVID Medline, CINAHL, and PsycINFO, from inception up to and including April 2023, using the Joanna Briggs Institute methodology for scoping reviews. The review considered any study design that detailed sufficient descriptive information on a given TMOUD service. A data extraction form was developed to collect and categorize a range of descriptive characteristics of each discrete TMOUD model identified from the obtained articles.
Results
A total of 45 articles met the inclusion criteria, and from this, 40 discrete TMOUD services were identified. In total, 33 services were US-based, three from Canada, and one each from India, Ireland, the UK, and Norway. Through a detailed analysis of TMOUD service characteristics, four models of care were identified. These were TMOUD to facilitate inclusion health, to facilitate transitions in care, to meet complex healthcare needs, and to maintain opioid use disorder (OUD) service resilience.
Conclusions
Characterizing TMOUD according to its functional benefits to PWOUD and OUD services will help support evidence-based policy and practice. Additionally, particular attention is given to how digital exclusion of PWOUD can be mitigated against.
Keywords
Introduction
Opioid use disorder (OUD) is defined as a persistent and problematic pattern of opioid use resulting in negative impacts on the individual's daily life and/or functioning. 1 OUD affects more than 26.8 million people worldwide and accounts for two-thirds of deaths directly caused by drug use disorders. 2 The COVID-19 pandemic has significantly impacted people with OUD (PWOUD) for example through social isolation, increasing the likelihood of solitary opioid use, increased mental health challenges and gender-based violence, and reduced access to health and social care.3–7 There is evidence that PWOUD in the US, particularly African Americans, were at increased risk of COVID-19 and associated adverse outcomes. 8 Indeed, the COVID-19 pandemic has significantly magnified existing structural and health inequalities that disproportionately impacted people from Black and ethnic minority groups, geographically deprived and/or remote regions, poorer socioeconomic backgrounds, and other marginalized social groups.9,10 PWOUD, through their intersecting experiences of social exclusion, discrimination, stigma, and homelessness, are over-represented among these marginalized groups.11,12
There is a parallel narrative that the COVID-19 pandemic has introduced several policy and regulatory and technological changes and innovations that has improved the delivery of and access to medications for OUD (MOUD) such as methadone and buprenorphine.13–15 Examples of these changes have included the provision of more take-home doses, longer prescriptions, and home delivery of MOUD, mobile methadone dispensing units, 16 and the provision of MOUD through telemedicine termed TMOUD in this paper.14,15,17As pre-pandemic norms of healthcare delivery return, there are calls to retain, invest in, and expand upon TMOUD to increase the efficiency and cost-effectiveness of OUD services, extend the reach of limited numbers of addiction specialists and qualified prescribers, and reduce overdose deaths and other OUD sequelae.15,18 There is a robust and comprehensive international evidence base in support of the effectiveness of MOUD such as buprenorphine and methadone to reduce opioid related all-cause mortality, overdose risk, and blood-borne virus transmission.19,20 There is also an acknowledgment that urgent systems-wide strategies are required to remove barriers to MOUD,21–24 increasing the appeal of TMOUD as a viable intervention in countries experiencing overdose crises. 25
Nevertheless, within a resource-constrained context, 26 and applying the lessons learnt during the COVID-19 pandemic,3,13,25 there are compelling reasons to apply a critical lens when examining the role of TMOUD in meeting the care needs of PWOUD. Firstly, PWOUD often have multiple and complex unmet care needs including housing, legal and income support, the treatment of co-morbid physical and mental health conditions, and harm reduction interventions to prevent blood-borne virus transmission. 19 Indeed, a recent Scotland-based study by Lowrie et al., 27 where per capita drug-related deaths are similar to the US, found that people experiencing homelessness repeatedly overdosed despite having access to MOUD. The authors attributed this to the inadequacy of single condition care models for PWOUD common in Scotland and worldwide, which may provide MOUD without also considering multimorbidity, frailty, and social determinants of health. 27
Similarly, Hedden et al., 28 raise concerns over the displacement of care that occurred during the COVID-19 pandemic, when key services to address PWOUD needs became inaccessible. For example, in the US, there was a 43% reduction and 25% cessation of syringe service programs (SSPs) nationally at the onset of the pandemic. Emergency departments, a common point of urgent care for PWOUD 29 and consistent primary care, known to improve health outcomes for this group,28,30 both had to restrict access in response to the pandemic. Eaves et al., 31 make the point that improved MOUD provision through telemedicine will not adequately mitigate against the structural drivers of drug use and risks, and the loss of wraparound services such as sterile injection equipment, wound care, blood-borne virus screening, pre-exposure prophylaxis, antiviral treatment, and naloxone offered by many community-based SSPs.16,32
The adequacy of telehealth to fully meet PWOUD care needs and through this, reduce high-risk opioid use and associated morbidity and mortality is one of the key unknowns in current TMOUD research. 18 More specifically, are there models of TMOUD that can improve access to wraparound and holistic person-centered care, and are there aspects of this care that are best delivered virtually or in person? The question of telehealth and access to care is further muddied by increasing evidence that Black and ethnic minorities and displaced people experiencing homelessness disproportionately under-utilized TMOUD, yet experienced opioid overdoses more frequently.18,33 An expansion of TMOUD services, which occurs at the expense of in-person care for PWOUD, will likely lead to the further marginalization of people who struggle to engage with technology due to affordability, skills, literacy, or other aspects of digital exclusion. 34
While digital exclusion may explain some of the observed inequality in uptake of TMOUD, there may be another more concerning explanation. There was evidence that clinicians delivering MOUD through telemedicine excluded prospective patients perceived to carry more liability risk due to greater complexity in their care needs. 33 This included people not already receiving MOUD, those who were taking multiple substances, had significant co-morbidities and/or were experiencing homelessness.35,36 Models of telemedicine that encourages the cherry-picking of patients with lower intensity needs may result in widening already unequal OUD care access to those who most need it, thus exacerbating racial and socioeconomic inequality. 37
There is therefore an argument for a more nuanced approach to capitalizing on the growth of telemedicine and its use in delivering MOUD to improve care for PWOUD. With this in mind, we conducted this scoping review to answer the following questions:
What models of TMOUD are currently described in the peer-reviewed literature? How do available TMOUD models cater for the diverse care needs of PWOUD? What are the knowledge gaps in developing TMOUD models, which equitably improve access to OUD care?
Methods
This study was conducted according to the Joanna Briggs Institute methodology for scoping reviews. 38 The review findings are reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (known as PRISMA) extension for scoping reviews. 39
Search strategy and selection criteria
Searches were conducted in three databases, OVID Medline, CINAHL, and PsycINFO, from inception up to and including 6 April 2023. Search terms for OUD, problematic opioid use, and medications for OUD such as methadone and buprenorphine were combined with terms for telemedicine, such as telepsychiatry, telehealth, videoconferencing, and remote consultation. An example of the search strategy and terms are included in the Supplemental material. The search strategy was intended to capture a diverse range of TMOUD services reported in the peer-reviewed literature. Consequently, articles were included if they were peer-reviewed, in English, and described service or systems level implementation, or the adaptation of existing services to deliver TMOUD in any setting and involving any population needing care for OUD. The review considered any study design provided sufficient descriptive information of the TMOUD service was available. Articles without abstracts, not peer-reviewed such as commentaries and/or letters, from the grey literature, or describing the use of technology but not directly connected to the delivery of MOUD were excluded. Zotero, an open-source bibliography management tool (v6.0.23) for Mac was used to manage references and remove duplicates.
Data extraction and synthesis
The retrieved records were screened by title and abstract using the review-management tool, Rayyan, by one author (JT). Full-text articles of the records passing this initial screen were obtained and reviewed for suitability for inclusion (JT). A second reviewer (AB) reviewed randomly selected 10 articles to independently verify their suitability according to the established inclusion criteria. Discrepancies between the two authors on whether an article should be included were resolved by consulting a third reviewer (JB). The final selection of papers was downloaded into the qualitative analysis platform Atlas.ti for Mac (v22.1.0).
Basic data were captured such as the year of publication, the country where the intervention was carried out, whether it was implemented in response to the COVID-19 pandemic, and the study design used. A more detailed data extraction form based on work by Lagisetty et al., 40 and Tang et al., 41 was developed to collect and categorize specific descriptive characteristics of each discrete TMOUD model identified. This included the treatment setting, existing in-person treatment model, the target population, threshold for care, whether the service was adapted or designed to be virtual, whether there was a hybrid offer (both in person and virtual), exclusion and inclusion criteria for enrollment, medications offered, and contingencies for care continuity. The data were extracted by one reviewer (JT) into a Microsoft Excel spreadsheet. Where possible, missing descriptive data of each TMOUD service was obtained either by contacting the article's author(s) or by looking at the service website. The findings of this review are reported in a narrative format.
Results
The search conducted on 6 April 2023, identified 195 records. Deduplication left 183 records screened by title and abstract, of which 100 were excluded due to irrelevance to the topic. A total of 83 full-text articles were then screened, of which 45 met our inclusion criteria (Figure 1).
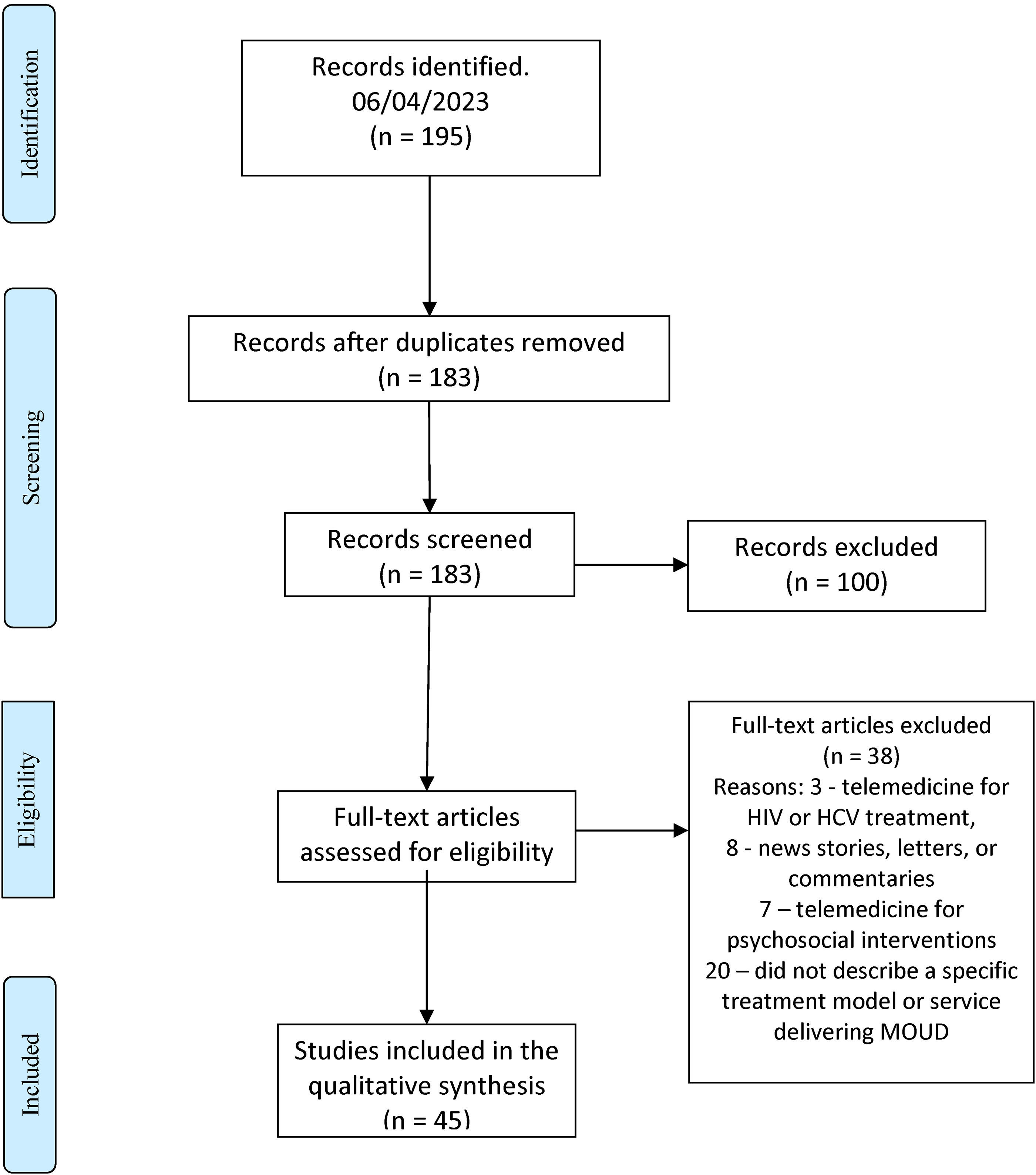
PRISMA diagram.
Characteristics of the included articles
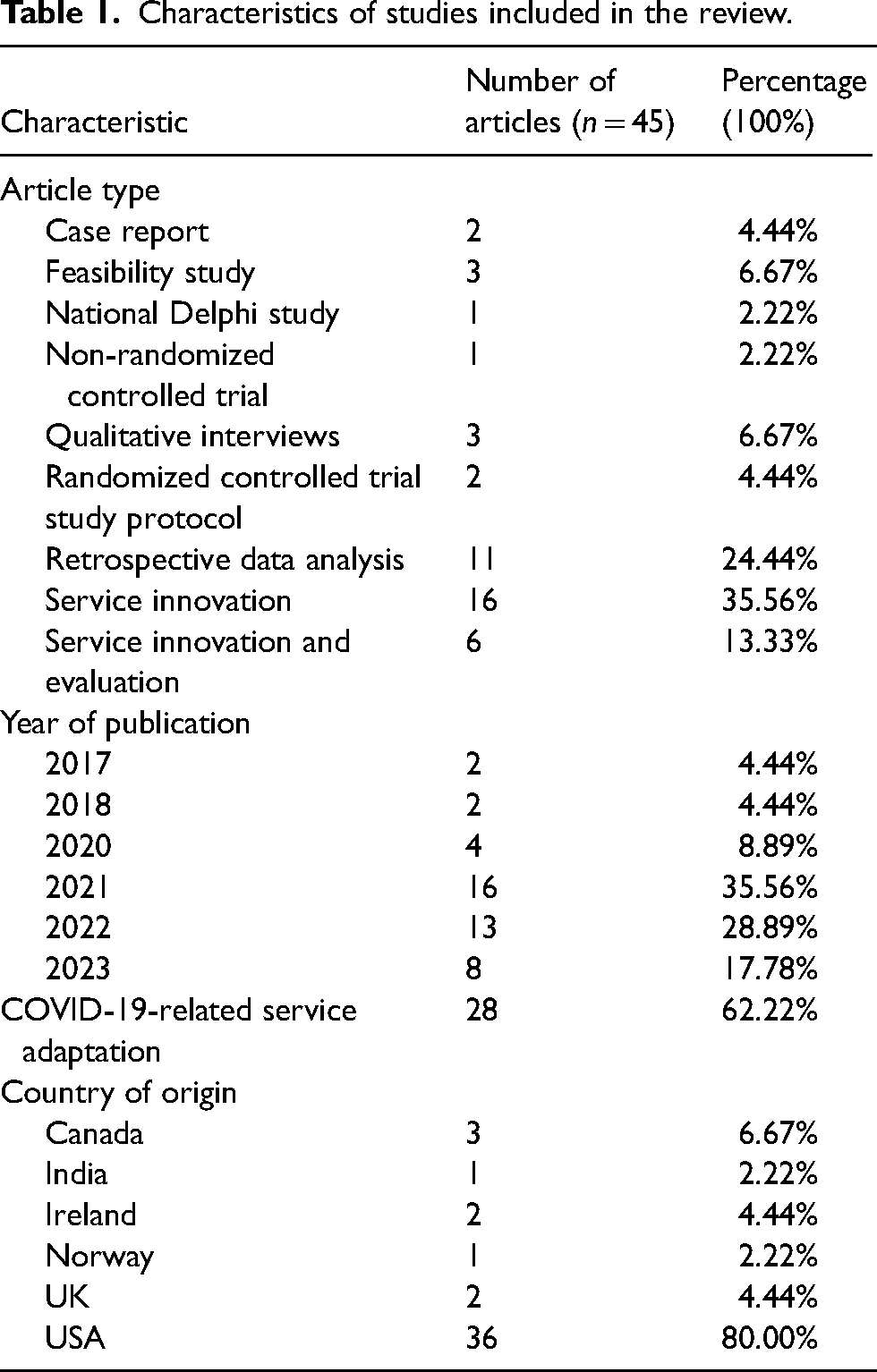
Table 1 summarizes the key characteristics of the included papers, and their contribution to this review can be found in the Supplemental Table 1. A total of 36 out of 45 papers (80%) were from the US, and 16 of the included papers described service innovation (16/45; 35%), or service innovation and evaluation (6/45; 13%), making up 49% of the included studies. There were 28 of the 45 papers (62%) that described service innovations in response to the COVID-19 pandemic.
Characteristics of studies included in the review.
Services identified in this review
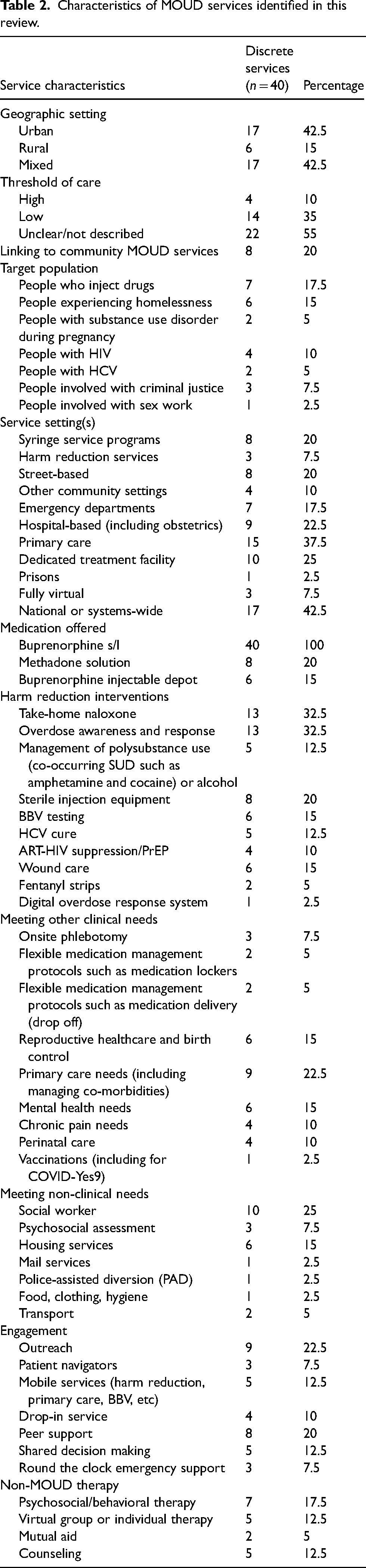
We identified 40 discrete services described across the 45 included studies. Table 2 summarizes some of the key characteristics of these services, and more detailed information on each service is provided in the Supplemental Tables 2–5. A total of 17 (17/40; 42.5%) services provided care for urban communities, 17 (17/40; 42.5%) for mixed urban-rural settings, and 6 (6/40; 15%) served rural settings exclusively. Most services were from the US (33/40; 82%), and within this, there was a diverse range of service settings from which TMOUD was delivered, including SSPs (8/33; 24%), harm reduction and street-based services (11/33; 33%), emergency departments (7/33; 21%), and hospital-based including perinatal services (9/33; 27%) and primary care (13/33; 39%).
Characteristics of MOUD services identified in this review.
Ten (10/33; 27%) of the US services identified in this review were national or systems-wide services, delivering care across state boundaries or across a large geographic area within a state. This included the Veterans Health Administration,42,43 the NYC Health + Hospitals system, 44 and the Los Angeles County Department of Health Services. 45 State-wide services covering South Carolina 46 and Pennsylvania47,48 were also represented. Two of the nationwide services were virtual only providers, one available in 30 US states 49 and the other in 14 US states. 50
All seven non-US services were national or systems-wide providers. Specifically, the Irish national model of remote care for opioid agonist treatment51,52 and the Norwegian national OUD treatment services 53 were represented in this review. Two of the three Canadian services covered the province of Ontario.54,55 The third identified Canadian service covered the province of Alberta and is the only non-US example of a virtual only TMOUD service. 56 One service provided care for OUD across a semi-rural county in England,57,58 and one is a publicly funded addiction treatment and research center catering to several northern and western states of India. 59
All 40 services offered sublingual buprenorphine as a MOUD option. Among the US services in this review, only the NYC Health + Hospitals system offered methadone through four hospital-based Opioid Treatment Programs (OTPs). 44 These OTPs did not provide telemedicine for patients already prescribed/taking methadone, despite the US regulatory changes allowing this provision. 44 All 33 US services in this review offered buprenorphine via telemedicine, dubbed tele-buprenorphine in some articles.60–62 A small number of patients from services in Pennsylvania were offered buprenorphine depot injection. 47 Among the seven non-US services, the Drug De-addiction and Treatment Center, in Chandigarh, India, was unable to provide MOUD without face-to-face contact with patients due to national regulatory restrictions on the prescribing of controlled drugs. 59 The remaining six non-US services offered both buprenorphine and methadone via telemedicine.
In Ireland, England, and Ontario, the tendency has been for methadone prescribing to be more common than buprenorphine.63–65 The Virtual Opioid Dependency Program (VODP) in Alberta, Canada, did not offer patients induction to methadone in its pilot phase in 2017 but did introduce this from 2018 onwards. 56 This makes VODP the only fully virtual TMOUD service in this review offering both buprenorphine and methadone inductions. 56 In Norway, as of 2021, 75% of patients prescribed with MOUD were provided predominantly sublingual buprenorphine, and increasingly since 2019, buprenorphine depot injection. 66 Indeed, 15% of patients on MOUD in Norway were provided monthly buprenorphine depot injections. 66
Telemedicine-specific challenges and solutions
Table 3 describes key telemedicine delivery processes undertaken by the services in this review. More than half the services (23/40; 57.5%) were fully hybridized, offering virtual and in-person access to both clinical and non-clinical interventions. Seven of these services allowed patients to determine for themselves whether they wished to have virtual or in-person contact. A small number of services were more restricted in how they used telemedicine. For example, four services had fixed criteria for whom they permitted the use of telemedicine for, determined by measures of stability, according to threshold of care needs or an agreement to engage in a certain number or pattern of clinical contacts.47,53,67,68 Similarly, while more than half of the services here (21/40; 52.5%) permitted induction onto MOUD through telemedicine, a small number provided virtual care for patients on established treatment only (5/40; 12.5%).
Telemedicine-specific service characteristics.
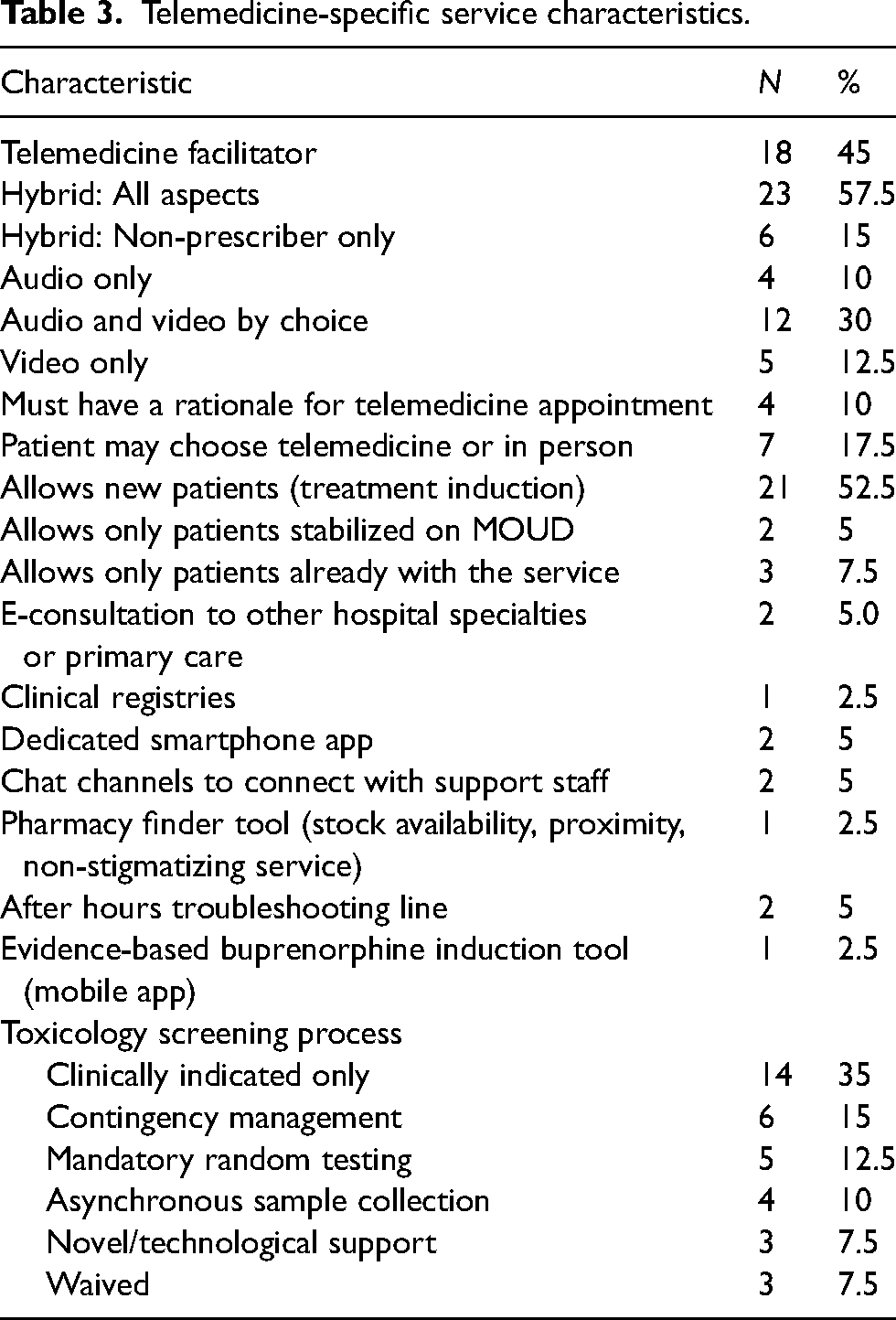
Almost half the services (18/40; 45%) provided telehealth facilitation to support engagement with TMOUD consultations, and bridge potential digital literacy or access issues. In recognition that many patients were unable to afford a smartphone or internet connectivity, 16 services offered an audio option (16/40; 40%), making telemedicine accessible to those with access to a standard handset or fixed line phone.
A key issue in providing TMOUD has been how near patient drug testing was to occur. Drug testing, to aid in OUD diagnosis, screening for polysubstance use, monitoring progress and stability, and confirming compliance with or detecting potential diversion of medication, is typically considered standard practice by treatment services.52,69–71 While guidance were produced to ensure that drug testing did not become a barrier to accessing MOUD during the pandemic,70,72 many services continued to place an arguably excessive importance in retaining this practice. Fourteen services (14/40; 35%) expected patients to provide samples for drug testing where clinically indicated for example if there were concerns around stability or diversion of MOUD. Five services (5/40; 12.5%) continued with mandatory drug testing as part of a formal treatment program, and six (6/40; 15%) used drug testing to support contingency management decisions where proof of abstinence would result in more entitlement to take-home doses of MOUD. Three services provided novel drug testing approaches that included posting out urine kits to the patient's home so a drug test could be carried out on demand during a virtual consult, 49 or the use of saliva-based drug testing kits where the clinician observed the test being taken live during a video consult. 47
Finally, the extended capabilities of a digital medium were capitalized upon by small number of services that provided dedicated apps to manage appointments and consults,17,49 chatroom channels to interact with support staff,17,49 a pharmacy finder with stock checking and stigma rating functionality, 49 a mobile phone-based buprenorphine induction tool, 49 and a digital overdose response system. 56
Defining TMOUD models of care
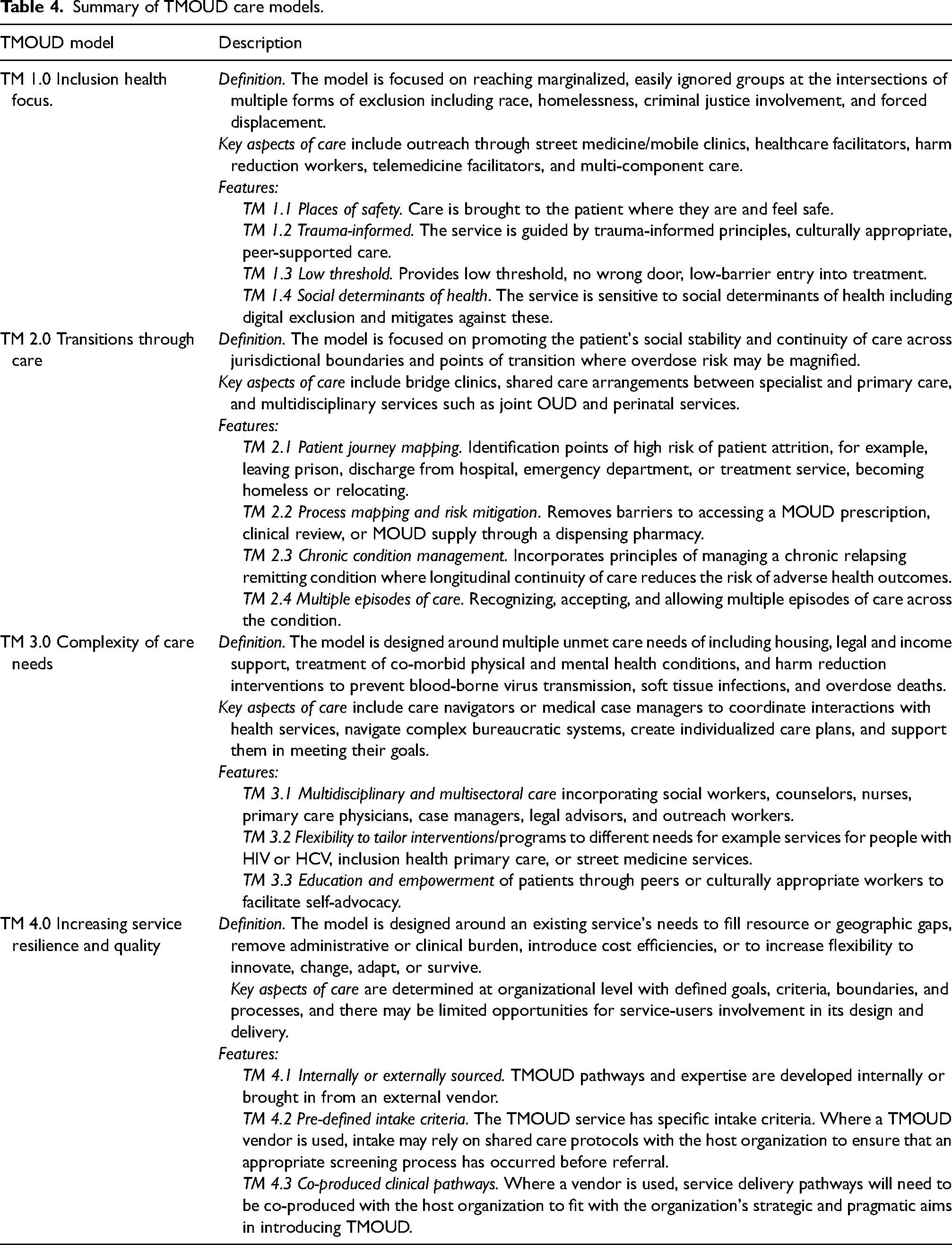
Through our analysis of the 40 services identified in this review, detailed in the Supplemental Tables 2–5, we have defined four TMOUD models of care that are described in this section. Table 4 provides a summary of each care model described below. These are TMOUD provided in the context of improving health inclusion, facilitating transitions through care, supporting complex care needs, and increasing service resilience. The models of care described here are not mutually exclusive and do have overlapping characteristics.
Summary of TMOUD care models.
TMOUD within inclusion health focused services
Inclusion health target populations refer to people who are disproportionately affected by inequalities in the social determinants of health, due to intersecting experiences of marginalization from homelessness, forced displacement, sex work, or criminal justice involvement, frequently underpinned by problematic drug and alcohol use.11,73 Among inclusion health populations, the mortality rate is almost 8 times the male average and nearly 12 times the female average, significantly greater than accounted for by the social gradient in health. 74 Twelve of the services in this review (12/40; 30%) had an inclusion health focus targeting easily ignored groups such as people experiencing homelessness,45,75–82 involved with criminal justice75,79,80,83 or with sex work. 84
These services offered a low threshold (minimal barrier) for entry typically characterized by same-day treatment entry45,51,52,56,60–62,76–81,85–87 and permitting treatment induction at home rather than exclusively at a dispensing pharmacy.45,49,56,60,61,76–81,86,87 In keeping with trauma-informed principles in providing care to people who use drugs (PWUD), 88 a non-judgmental attitude respectful of the patients goals in engagement with treatment were prioritized,45,49,56,60,61,76–81,86,87 including a reduction in illicit substance use as opposed to a commitment to abstinence.56,60,75–77,79,81,87
The cornerstone of this model involved making OUD care available in non-traditional sites, where the patient felt safe and more likely to attend. This is demonstrated by the provision of TMOUD at SSPs, which are community-based interventions offering sterile injecting equipment and blood-borne virus preventative strategies such as testing and treatment. 89 Eight (8/40; 20%) of the services in this review provided TMOUD via SSPs,75–80,82,84,87,90 and three also worked through overlapping harm reduction services.75,84,85 Barriers were broken down further by delivering TMOUD directly to people on the street. Examples of this have included the Los Angeles County Department of Health Services low-barrier telephone service 45 that used community health workers entering homelessness encampments and linking patients directly with providers, or volunteer delivered foot or bicycle-based street outreach through the Harm Reduction and BRidges to Care (HRBR) Clinic, in Portland, Oregon. 90
A further key characteristic of this TMOUD model was a nuanced perspective on digital exclusion. 75 For example, Aronowitz et al., highlighted that the remote clinician's attitude toward risk, expectations, and measures of patient stability and consequent judgment on suitability for telemedicine consults ran counter to in-person observations of non-clinical support workers in SSPs. 75 In this context, digital exclusion was not caused by a lack of access to technology, but to clinician discomfort in the use of this technology for a specific patient group. 75 Other examples of a nuanced understanding of digital exclusion was demonstrated by the Infectious Disease Elimination Act (IDEA) Syringe Services Program (SSP) in Miami, Florida, 76 and the associated Telehealth Solution for HIV and Addiction-Related Problems among People who inject drugs (T-SHARP)77,78,81 research project. Specifically, while the telemedicine consult was a critical element of care, there were several other essential components needed to translate it into successful engagement in MOUD. The IDEA SSP service for example invested in the provision of flexible medication management protocols that allowed for fixed location lockers or street-based medication drop-offs to ensure that people experiencing homelessness were able to safeguard their prescription medications supply. 77 Similarly, the STAMINA study at three SSP sites in Chicago, Illinois, incorporated transport for patients to attend the pharmacy to obtain their supply of buprenorphine following a telemedicine consult, or to access an OTP, should they opt for methadone as their MOUD option. 87
Finally, digital exclusion cannot be divorced from the individual's overall socioeconomic deprivation and disadvantage. 91 In other words, where the individual is unable to meet housing, financial, and nutritional needs, it is unlikely for them to be concerned about owning and maintaining a digital device to utilize telemedicine. Examples to mitigate against this included the telephone booth model of TMOUD by the Centre for Harm Reduction, Homeless Health Care Los Angeles. 82 Further, several services providing TMOUD also extended supports to address social determinants of health including housing,75,77,81,82,92,93 food, clothing, and hygiene. 82
Several services recognized the importance of building trust and creating a sense of psychological safety among PWOUD in need of treatment through the use of peer outreach workers.49,60,75–77,79–81,84,92 Nevertheless, there was evidence to show that Latinx and Black PWUD were less likely than White PWUD to access SSPs, harm reduction interventions, and OUD services more generally. 94 Indeed, this was the reflection of the Los Angeles County Department of Health Services low-barrier telephone service that continued to find disparities in Black and Latinx populations access of MOUD despite their healthcare worker outreach approach. 45 One service, the Honoring Individual Power & Strength (HIPS) clinic, in Washington, DC, bucked the trend with predominantly Black (90.6%), male (74.4%) clients with a mean age of 53 years old. Most HIPS clinic staff originated from the same community and shared lived experiences with clients, including recovery from substance use, which contributed to the effectiveness of their TMOUD model in addressing racial inequalities to access. 84
TMOUD facilitating transitions through care
A key aspect of the provision of MOUD is continuity through key periods of transition across or between services and jurisdictions. 19 Examples of key transition points include people entering or leaving the criminal justice system, 19 leaving an emergency department following a non-fatal opioid overdose,29,95 moving from specialist treatment programs to community-based maintenance services, 96 leaving an inpatient hospital ward on completion of medical treatment, 19 or an unplanned departure from an OTP for non-adherence to a treatment plan. 97 These periods of transition represent key touchpoints where substance use-related harms are more likely to occur, and overlap with opportunities to modify this risk. 19
Ten services in this review described bridge clinic models designed specifically to provide low-barrier, transitional MOUD services to reduce the increased risk associated with periods of care transition.17,47,56,60–62,85,86,90 These services became particularly important with the onset of the COVID-19 pandemic due to policies of rapid reductions in prison populations, resulting in a large number of people leaving incarceration with urgent MOUD needs. 98 Six of these 10 TMOUD bridge services provided care to people leaving emergency departments.17,47,60,85 An emergency department in Rhode Island conducted a callback pilot to extend the reach of the bridge model of care, contacting people who suffered a non-fatal opioid overdose for a follow up telephone call on discharge, offering harm reduction resources and access to TMOUD. 60 The Faster Paths Low-barrier bridge clinic offered through The Grayken Center for Addiction at the Boston Medical Center not only provided care to patients identified through the emergency department, but also permitted direct walk-in access for patients. 85 The NYC Public Hospital System Low-Threshold Tele-Buprenorphine bridge clinic was able to provide care to patients referred by hospital and clinic staff, correctional health services, community organizations supporting reentry, homeless shelters, social service, community organizations, and harm reduction programs, as well as self-referrals from patients hearing about the service by word of mouth and online searches. 61
In addition to the bridge clinic model, this review identified two services designed to offer specialist transitional telemedicine care to women with OUD and going through pregnancy.68,93 These services were particularly important to maximize the engagement with both perinatal and OUD care, both of which improve health and social outcomes before, during, and after pregnancy.68,93 Five shared care models through telemedicine were identified, where specialty services like addiction psychiatry carried out diagnosis, assessment, MOUD induction, and handed off to community-based services or primary care for longer term chronic care management.25,42,43,46,51–53,62,99,100
The VODP in Alberta, Canada, exemplified the full potential of telemedicine in delivering treatment continuity through periods of transition and increased risk. 56 VODP was fully integrated into the Alberta Health Service and used the province-wide telehealth network and health insurance. 56 This enabled access to TMOUD to any qualifying individual, practitioner, or service (including criminal justice, harm reduction, and hospitals) in Alberta through a single toll free number. 56 Reciprocally, a broad range of Alberta-wide community-based resources such as laboratories for urine drug screening, pharmacies for observed MOUD dosing, and unscheduled care telephone lines were available to VODP staff and patients. 56
TMOUD supporting complex care needs
Several TMOUD services identified in this review evolved to address the complex health and social care needs of PWOUD. Examples included those providing care for people with or at risk of HIV,75–81 HCV,79,80,92 multi-morbid health conditions best addressed by primary or generalist care42,43,47,48,61,62,85,100 including through street medicine, 79 and co-morbid mental health conditions.55,71 The provision of care navigators to help patients to coordinate complex bureaucratic systems of health and social care was a key component in addressing complex care needs.45,61,62,92 Embedding TMOUD within primary care allowed for cultivation of long term, longitudinal relationships, and provision of resources and expertise to manage chronic co-morbid medical conditions including chronic pain and cardiovascular and respiratory disease, another critical feature of this model.42,43,47,51,62,66,85,100
Other key needs addressed by services supporting patients with complex needs included the provision of onsite phlebotomy,78,79 hepatitis C testing and cure,75,78,79,85 HIV testing, and antiretroviral therapy for suppression,78,79,85 wound care including incision and drainage,75–78,82,85 and reproductive care needs.68,75–78,85 Mental health needs were met through telepsychiatry, virtual psychology or counseling, and mobile app-based chatrooms.47,49,55,68,71,76–78,85,93 In order to educate and empower patients to prioritize their own health needs and goals, some services prioritized shared decision making to develop individualized care plans.17,75,78,93
Some services provided access to crisis care through stabilization units to support people in acute withdrawals or intoxication, 17 or through round the clock telephone or app-based emergency support.50,56,68 New avenues of meeting complex health needs were made possible in the Substance Treatment and Recovery (STAR) clinic in South Carolina, following COVID-19-related transitioning to TMOUD, where a new range of cross-specialty and cross-disciplinary e-consults were introduced. 46 The Norwegian national OUD treatment service identified improvements in liaising with non-medical colleagues in social and housing services through multidisciplinary case management facilitated by telemedicine. 53
TMOUD to increase service resilience
The term “TMOUD vendors” has been used to describe the outsourcing of MOUD provision to specific telemedicine providers to expand community-based access to this form of treatment. 101 Hser et al., described a feasibility study looking at the use of TMOUD vendors to expand MOUD availability to rural primary care services for example. Participating rural practices screened for OUD and directed appropriate patients to a telemedicine consult for buprenorphine induction and stabilization before taking on their longer term management. 101 Both Bicycle Health 49 and Ophelia Health 50 offered opportunities to work with health systems and providers to offer tele-buprenorphine to patients meeting pre-determined criteria. Other examples included the STAMINA study at three SSP sites in Chicago, where a national TMOUD vendor remotely assessed potential patients and either inducted suitable patients unto buprenorphine or facilitated their attendance at an OTP that offered methadone. 87 Critically, the intake criteria TMOUD vendors used had the potential of excluding patients with complex needs or those perceived as having significant social or clinical instability. 50
The VODP service, fully integrated into the existing healthcare infrastructure in Alberta, Canada, 56 supported mainstream community OUD service resilience through the provision of flexible continuity of care. Indeed, a fully integrated virtual model offering seamless transitions through care may ultimately contribute to overall treatment system resilience by reducing demand on traditional services to respond to acute crises and high-risk situations among PWOUD. VODP provided bridging MOUD services, allowed for repeated treatment episodes, and was able to provide ongoing medical case management if there is no local capacity to take over patient care. 56 Similarly, the US Veteran Health Administration funded regional tele-mental health hubs, which facilitated the sharing of clinical cover to less well-resourced areas, a facility that was adapted to deliver TMOUD during the pandemic. 43
The effectiveness of this model is contingent on the TMOUD vendor understanding and engaging with the system and organizational needs of the host service,50,101 the community, and individual patient care needs. 49 For example, one vendor supporting a high threshold abstinence focused rural service reflected on the disadvantages in being unable to influence other critical programmatic components such as the patient discharge policy and obligations to attend counseling.102,103 Additionally, fully virtual TMOUD services in this review were not explicit in how key harm reduction services such as take-home naloxone, overdose awareness and response training, sterile injecting equipment, and fentanyl test strips were to be provided.87,104 The exception was VODP that provided access to an Alberta-wide app-based digital overdose response system. 56 Exclusively, virtual services may need to be increasingly intentional, proactive, and innovative in ensuring that high quality harm reduction interventions are incorporated into their delivery of TMOUD.
Discussion
To our knowledge, this systematic scoping review is the first exploration of the international peer-reviewed literature to identify models of TMOUD delivery. Through the identification and characterization of discrete services within our data set, we have been able to empirically define four over-arching models of TMOUD. Three of these models addressed some of the complexities inherent in providing care to PWOUD, for example, the need to actively reach marginalized individuals, to minimize breaks in MOUD provision during periods of transition, and to opportunistically address holistic care needs beyond OUD. The final TMOUD model of care, arguably the dominant focus of post-pandemic policy discussions, related to improving and preserving service resiliency and efficiency.
By defining these four overlapping models of care, we hope to contribute to a more nuanced discussion on the policy challenges involved in designing telemedicine for PWOUD. This has relevance for healthcare jurisdictions examining alternative reimbursement models such as bundled payments (expected costs for a defined episode of care) as opposed to fee per service or capitation (a standard fee per patient regardless of services provided) models. 105 Specifically, the TMOUD models described here provide context to define clinical episodes of care matched to the needs of PWOUD. By defining what these PWOUD-focused episodes of care look like, we also hope to influence the quality standards of this care and future outcome and evaluation measures.
Further, alternative payment models that allows the flexible use of in-person and telemedicine tools 106 to fit specific functional deliverables, for example, inclusion health, care transitions, complex co-morbidities, and service resilience, may lead to innovative approaches that reach marginalized groups, rather than being accessible only to those with a higher level of health cover or digital competence. Such an approach may mitigate against exclusively virtual TMOUD services cherry-picking higher-margin patients, leaving hybrid or traditional providers grappling with increased health inequity and negative financial impacts. 41
The importance of a nuanced understanding of digital exclusion when applying TMOUD models of care has been highlighted in this review. For example, there is currently a debate on whether audio only telemedicine should be reimbursed in the same way as video consultations, 106 with policymakers leaning toward disallowing this in the longer term. This is partly due to concerns that audio only services will result in increased costs without improvements in efficiency or workload. Nevertheless, some of the more successful TMOUD services identified in this review, which have engaged people at the extreme margins of society, have been audio only services.45,84 It is possible therefore that current thinking that devalues audio only telemedicine may contribute to worsening digital exclusion. The growing evidence base for audio only TMOUD in populations most vulnerable to digital exclusion may serve to temper this debate 107 and lead the way toward future prospective randomized controlled trials for this treatment modality.
Another concern is that digital exclusion may become conflated with other structural causes of social exclusion and inequality. More specifically, the reasons why some TMOUD services were not successful in attracting Black and Latinx PWOUD may be connected to an entrenched mistrust of authorities and services rather than due to a lack of digital competence or resources. 94 Strategies to address digital exclusion that focuses on access to technology or improving digital literacy alone 34 may therefore miss the mark and fail to engage these groups in TMOUD. A particular challenge lies in identifying how cultural competence, trust building, and breaking down barriers caused by structural violence may be embedded within telemedicine approaches offered to marginalized and oppressed communities.
The main limitation of this review is that it is dominated by US studies, which may impact on its applicability to other countries and health systems. Further, as TMOUD in the US has mainly provided sublingual buprenorphine, information is limited on how methadone or injectable depot buprenorphine may be provided through telemedicine. This gap does need to be addressed considering the lower retention in treatment of patients on buprenorphine (46%) compared to methadone (74%), 108 and the different safety concerns relating to the two medications. 70 Both Irish 52 and Canadian 70 guidance on TMOUD provide detail on how methadone inductions and maintenance can be conducted, and risk managed, and future research should consider more diverse use of different medication options. Additionally, concerns over medication diversion, the need for frequent pharmacy attendance, and problems with identifying pharmacies to dispense buprenorphine may be addressed by exploring the more extensive use of injectable depot buprenorphine, as was done in the national Norwegian OUD service. 53
Finally, both in the US, and internationally, there are likely to be private and public entities that have carried out intentional or ad hoc TMOUD activities that will not have been captured by this review. There is therefore a need to understand the lack of peer-reviewed literature on TMOUD from other countries and within that, from treatment providers not typically captured by conventional research approaches. The UK, for example, is said to have introduced telemedicine to facilitate more widespread induction of patients to MOUD in response to the pandemic,109,110 yet there is limited peer-reviewed or grey literature to verify this claim, or to support local best practice guidance on practice and implementation of TMOUD.
Conclusion
In this review, we have detailed how services providing OUD care have incorporated telemedicine to facilitate the provision of medications such as methadone or buprenorphine. Specifically, we have characterized four models of TMOUD that includes its use to facilitate inclusion health, transitions through care, the management of complex care needs, and maintaining the resilience of in-person high acuity OUD services. This characterization supports a more nuanced discussion around the role of telemedicine in delivering care for PWOUD, with implications for how such services are funded and avoiding the risk of worsening digital exclusion among already marginalized and vulnerable groups. Further, our characterization of TMOUD models may guide the development of service evaluation metrics that link more directly to the different but overlapping constellations of PWOUD need. This may lead to incentivizing the retention and strengthening of TMOUD programmatic components that breaks down structural barriers to treatment access for PWOUD.
Supplemental Material
sj-pdf-1-jtt-10.1177_1357633X231195607 - Supplemental material for Understanding the use of telemedicine across different opioid use disorder treatment models: A scoping review
Supplemental material, sj-pdf-1-jtt-10.1177_1357633X231195607 for Understanding the use of telemedicine across different opioid use disorder treatment models: A scoping review by Joseph Tay Wee Teck, Jenna L Butner, and Alex Baldacchino in Journal of Telemedicine and Telecare
Footnotes
Acknowledgments
We would like to acknowledge the support of the Scottish Government Drug Deaths Task Force in the development of the DigitAS Project in St Andrews University.
Author contributions
JT and AB conceived the project. JT extracted data. AB supervised research activities. All authors contributed to data analyses and verification. JT drafted the manuscript and managed subsequent iterations following additions and edits from co-authors. All authors critically reviewed the manuscript and interpreted findings.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JB has previously worked at Ophelia Health which is cited in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.