
Abstract
Introduction
Telemedicine has been shown to be a safe and effective modality to assess and treat patients with acute stroke who present to a community hospital. There are no previous reports on using telemedicine to treat patients with acute stroke who present to a comprehensive stroke center. We report here the outcomes of patients with acute stroke treated in 2021 at our comprehensive stroke center using telemedicine versus an in-person assessment.
Methods
Patients with acute ischemic stroke who were treated after either a telemedicine or in-person assessment at our hospital in 2021 were identified by a retrospective chart review. The primary outcomes collected were door-to-needle (DTN) time for alteplase (tPA) administration, door-to-puncture (DTP) time for endovascular thrombectomy, symptomatic intracranial hemorrhage (sICH) rates and 3-month mortality.
Results
There were 302 patients with acute stroke treated at our hospital in 2021. Of these, 18.2% (n = 55/302) were treated using telemedicine. There were no differences in any of the outcomes between patients treated using telemedicine versus an in-person assessment: DTN (35.5 min (n = 42) vs 33 min (n = 182), p < 0.76), DTP (86.5 min (n = 30) vs 85 min (n = 134), p < 0.97), sICH (0% (n = 0/55) vs 1.6% (n = 4/245, p < 0.59) or 3-month mortality (20.6% (n = 7/34) vs 22.1% (n = 40/181), p < 0.29).
Discussion
To the best of our knowledge, this is the first study to report on outcomes for acute stroke patients treated using telemedicine at a comprehensive stroke center. In this study, there were no differences in outcomes between patients treated using telemedicine versus an in-person assessment.
Introduction
The use of telemedicine by a stroke specialist to assess and treat patients presenting with acute stroke at another location is commonly known as telestroke. telestroke is typically used in “hub-and-spoke” models of care, in which a tertiary care comprehensive stroke center specialist is connected to a peripheral primary stroke center. 1 In 2002, the Canadian province of Ontario established a telestroke “hub-and-spoke” network to address low treatment rates of patients with acute ischemic stroke in underserved areas. Previous studies have reported that telestroke assessments in a “hub-and-spoke” model have a high inter-rater agreement with in-person National Institute of Health Stroke Scale (NIHSS) score assessment, 2 enhance safe decision making when compared with telephone-only consultation, 3 are as safe and effective as in-person assessments and are cost-effective.4,5 In Ontario, telestroke has improved access to endovascular thrombectomy (EVT) for stroke, increased the number of patients with stroke discharged home, reduced the costs of stroke borne by network hospitals, and improved long-term patient outcomes.6–10 Overall, the efficacy and safety of telestroke in a “hub-and-spoke” model is well established.
Our hospital (Trillium Health Partners, Mississauga, Ontario, Canada) is the only comprehensive stroke center for our local health network, which is approximately 1500 km2 and serves 1.6 million residents. In 2019 to 2020, 1049 patients presented by EMS to our center for acute stroke assessment, and 171 patients were treated with tissue plasminogen activator (tPA) and 123 with thrombectomy. 11 During the early stages of the COVID-19 pandemic, our stroke neurology group worried that the pandemic would threaten our ability to provide timely in-person acute stroke assessments, especially when patients presented after-hours when a neurologist was not in-house. Our concerns included physicians becoming COVID positive and not being able to participate in call, strict infection controls at hospital entrances and the emergency department (ED), and our ED being on COVID outbreak. Prior to the COVID-19 pandemic, we did not use telestroke locally at our hospital. We would typically receive one to two patients per month from outside hospital transfers through the Ontario telestroke program.
In 2020, we developed a local telestroke system that allowed our hospital's stroke neurologists to virtually assess and treat patients who presented to our institution as code strokes. This involved consultations with our hospital's stroke neurologists, information technology specialists, and administration. We also worked with the Ontario telestroke Network to take advantage of their existing telestroke infrastructure. We trialed a few videoconferencing devices but ended up using a custom-built telemedicine cart with a 23” monitor, HD camera, microphone, and WiFi router. We chose WiFi, instead of a physical connection, because our patients are assessed in several rooms in our ED. Installing physical connections in each room would have taken more time and more money than using WiFi. The local hospital network connection was configured to provide dedicated bandwidth to ensure stable audio and visual performance. We used the Ontario Stroke Network to remotely connect to our local hospital network. “Vidyo” videoconferencing software connected the cart in the ED to the remote stroke physician. Both the Vidyo software and the Ontario Stroke Network were previously vetted to ensure that our local hospital, provincial and federal government privacy requirements were met. From our review of the literature, this is the first time that telestroke has been used to assess and treat patients with acute stroke who present to a comprehensive stroke center.
The protocol for telestroke assessments was similar to in-person assessments. We used a co-management model with our ED physicians. The stroke neurologist's role was to assess patients to determine if they were candidates for acute therapy with thrombolytics or thrombectomy, and to order the administration of tPA if the patient was a candidate. At the start of a code stroke, the ED charge nurse would call the stroke neurologist when EMS per-notified the hospital that a code stroke was on route. The neurologist would then decide to either come to the ED for an in-person assessment or to use telestroke. telestroke was usually used for after-hours and weekend assessments, when the neurologist was not already on-site. For telestroke, the stroke neurologist would ask the ED charge nurse to have the telestroke cart connected in the patient's room. The cart would usually be set up in the assessment room before the patient arrived. The cart was setup to automatically login to the hospital network via WiFi and the videoconferencing software on start-up. The neurologist would then remotely assess the patient with the assistance of a previously stroke-trained ED nurse. Because the cart was set up before the patient arrived, the stroke neurologist would also be able to get a history directly from EMS. Protocols to get the patient acute stroke imaging were not changed or different from in-person assessments. Computed tomography (CT)/CT angiography (CTA) images were reviewed remotely, and orders would be entered remotely through our electronic medical record system (Epic). If needed, thrombectomy would be arranged over the phone by the stroke neurologist consulting with the neuro-interventionalist. There was always an ED physician on-site in the ED. The ED physician's role was to ensure that the patient remained stable and to assess and treat for any medical issues, including complications of thrombolysis.
In this study, we report the efficacy and safety outcomes of patients with acute ischemic stroke who presented to our comprehensive stroke center in 2021 and who were treated with either telestroke or in-person assessments. Our null hypothesis was that there will be no difference in efficacy or safety outcomes between patients who were treated using telestroke versus in-person assessments.
Methods
We performed a retrospective chart review of patients treated for acute ischemic stroke at our comprehensive stroke center. Study patients were identified from a pre-existing registry that our stroke program maintains. Patients were included in the study only if they were treated with tPA, EVT, or both. Patients were confirmed to have been treated using telestroke after a chart review and by tracking telestroke utilization dates and times through our telestroke provider (Ontario telestroke Network). Data that was collected included patient age, gender, initial NIHSS, arrival time in the emergency department, treatment type (tPA only, EVT only, both tPA and EVT), time of tPA administration, time of arterial puncture for EVT, treating neurologist's name, symptomatic intracerebral hemorrhage (sICH) identified on imaging after treatment and 3-month mortality. Door-to-needle time (DTN) was defined as the time from patient's arrival to the time the tPA bolus was administered. Door-to-puncture (DTP) time for embolectomy was defined as the time from arrival in the ED to the time of arterial puncture at the start of EVT. The sICH was defined as: a hematoma occupying ≥30% of the infarcted brain tissue with substantial space occupation on imaging 22 to 36 h after treatment and combined with a neurological deterioration of ≥4 NIHSS points from baseline. 3-month mortality was determined through local chart review and through a provincial medical record review. If patients were not confirmed to be either alive after 3 months or dead before 3 months, then this field was left blank. After-hours patients were defined as patients who presented before 8 am, or after 5 pm on Monday to Friday, or anytime Saturday or Sunday.
Study data were collected from January to December 2021 and January to June 2018. Control data from 2018 was collected to see if the pandemic affected 2021 in-person assessments. Study patients were divided into three groups: those treated in 2018, those treated using telestroke in 2021, and those treated after an in-person assessment in 2021.
Patient data were collected using a database program (Microsoft Access) and stored on a password-protected local hospital server. This study was approved by our hospital's local research ethics board.
We then compared efficacy (DTN and DTP) and safety (sICH, 3-month mortality) outcomes between patients treated using telestroke versus in-person assessments. Efficacy and safety outcomes were co-primary objectives. Data were compared using a Student's t-test, one factor analysis of variance with Bonferroni correction or a chi-square test for proportions where appropriate using Microsoft Excel.
Results
Patient characteristics are summarized in Table 1. There were 455 patients identified during the chart review. From January to June 2018, there were 153 patients treated for acute ischemic stroke at our center (72 treated with just tPA, 43 treated with just EVT, 38 who received both). In 2021, there were 247 patients treated using in-person assessments (113 treated with just tPA, 66 treated with just EVT, 68 patients treated with both) and 55 patients were treated using telestroke (25 treated with just tPA, 17 treated with just EVT, and 17 treated with both). telestroke was used to treat 18.2% of patients in 2021 (55 of 302) and 91% (n = 50) of telestroke patients were treated after-hours.
Patient characteristics.
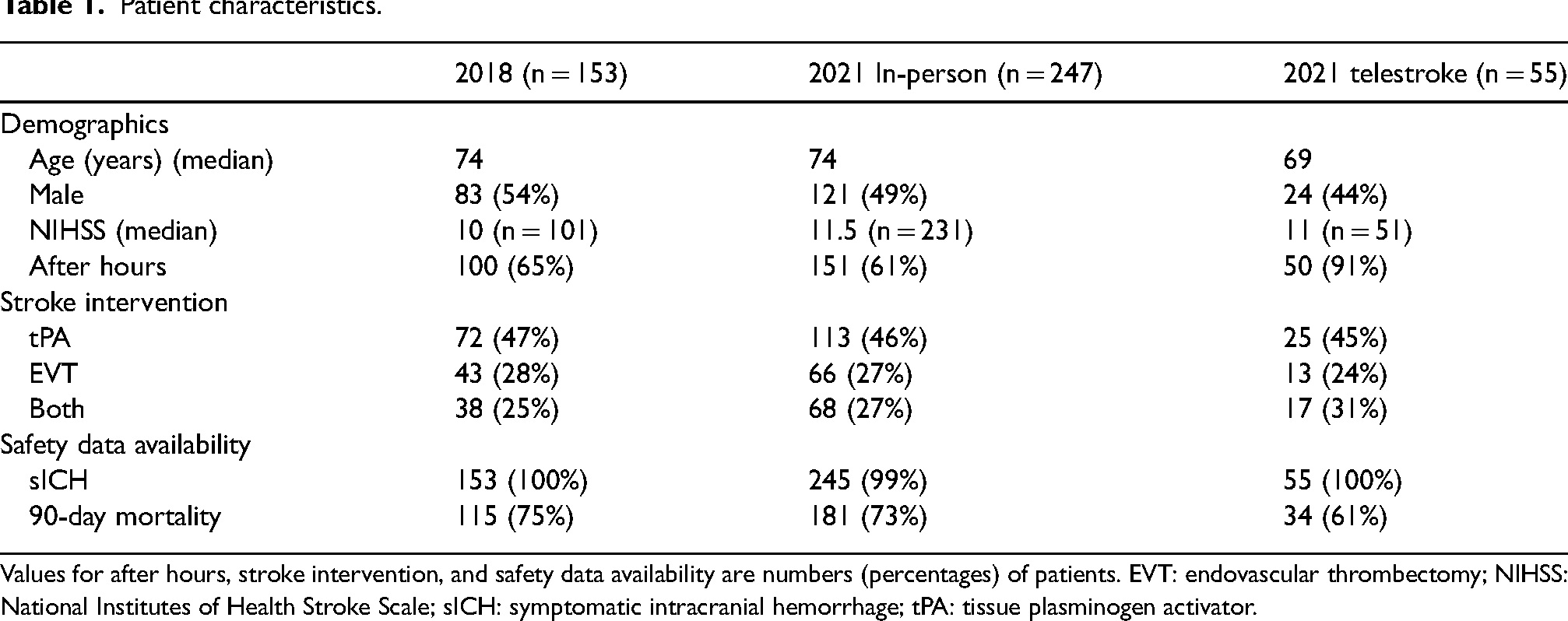
Values for after hours, stroke intervention, and safety data availability are numbers (percentages) of patients. EVT: endovascular thrombectomy; NIHSS: National Institutes of Health Stroke Scale; sICH: symptomatic intracranial hemorrhage; tPA: tissue plasminogen activator.
In terms of efficacy, there was no difference between median DTN for patients treated using telestroke versus in-person assessments (35.5 min ± 12.7 (n = 42) vs 33 ± 17.5 min (n = 182), p < 0.76, see Figure 1) or in median DTP (86.5 ± 19.3 min (n = 30) vs 85 ± 35.4 min (n = 134), p < 0.97, see Figure 2). There was a significant difference in median DTN between patients treated after an in-person assessment in 2018 versus 2021 (40 ± 21.1 min (n = 111) vs 33 ± 17.5 min (n = 182), F 6.55, p < 0.0007). There was no difference between in-person assessment DTN in 2018 vs 2021 when patients were treated during regular hours (40.4 ± 15.6 min (n = 35) vs 37.8 ± 15.3 min (n = 52), p = 0.45). However, there was a difference between in-person assessment DTN between 2018 versus 2021 when patients were treated after-hours (47.8 ± 42.0 min (n = 76) vs 37.9 ± 18.4 min (n = 111), p = 0.001). The difference between in-person assessment DTN in 2018 and 2021 was therefore attributed to a difference in after-hours DTNs. For comparison, the DTN of after-hours telestroke cases was 37.7 ± 12.0 min (n = 38).
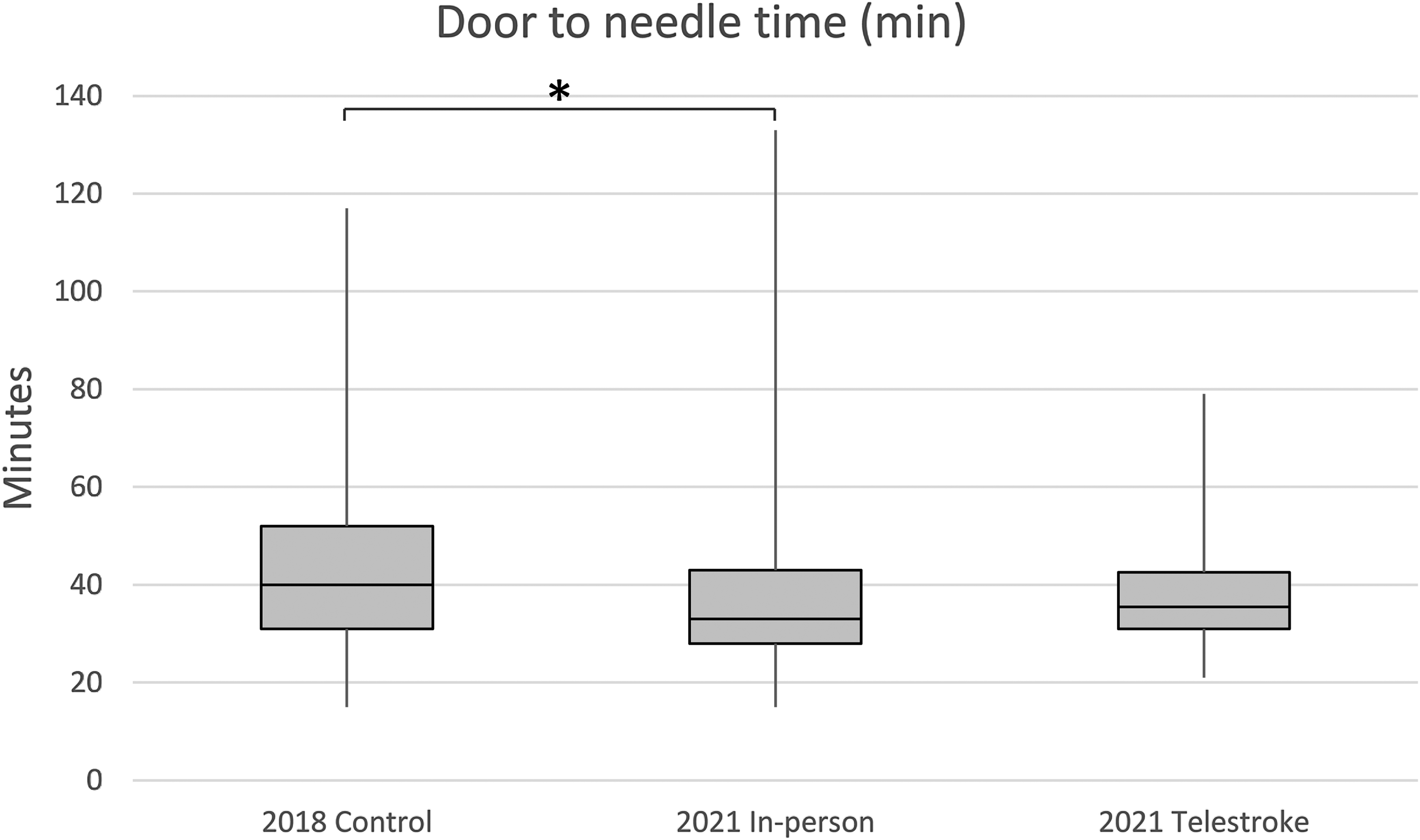
DTN times for tPA administration. Box and whisker plot of DTN times (minutes) for tPA administration for the 2018 in-person control group, 2021 in-person assessments, and 2021 telestroke assessments. Boxes show the first quartile, median, and third quartile values. Whiskers show the minimum and maximum values. *There was a difference in DTN time between 2018 and 2021 in-person assessments (p < 0.0007). DTN: door-to-needle; tPA: tissue plasminogen activator.
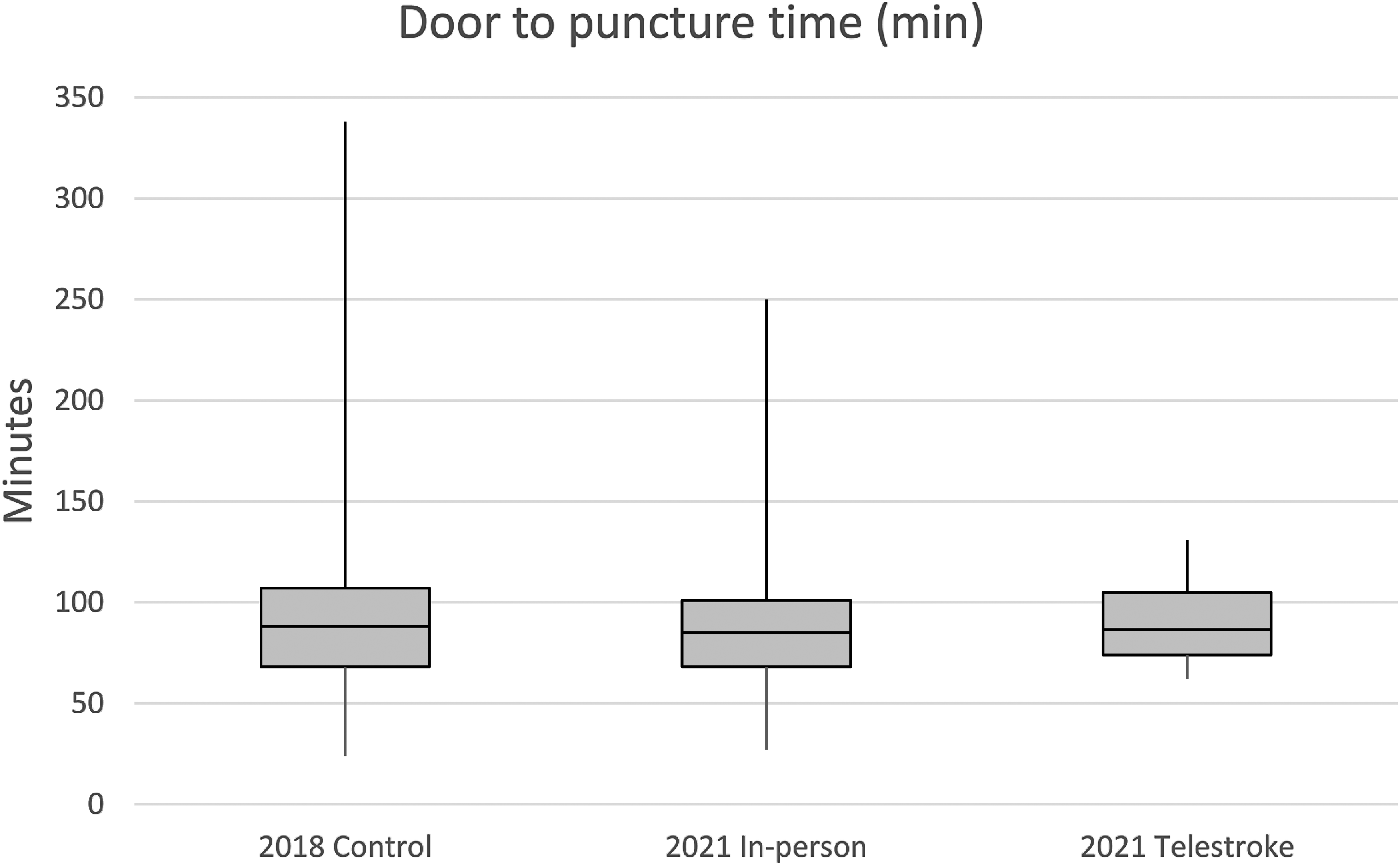
DTP times for EVT. Box and whisker plot of DTP times (minutes) for EVT for 2018 in-person control group, 2021 in-person assessments, and 2021 telestroke assessments. Boxes show the first quartile, median, and third quartile values. Whiskers show the minimum and maximum values. There was no difference in DTP times between the three groups. DTP: door-to-puncture; EVT: endovascular thrombectomy.
Eleven neurologists took acute stroke call at our hospital in 2021. Of those, 63% (7 of 11) chose to use telestroke for some of their assessments. For neurologists who treated patients using either telestroke or in-person assessments, there was no difference in telestroke versus in-patient efficiency outcomes with either DTN (35.5 ± 12.7 min (n = 42) vs 34 ± 15.9 min (n = 111), p < 0.69) or DTP (88 ± 18.5 min (n = 25) vs 81.5 ± 36.0 min (n = 80), p < 0.06).
For safety metrics, sICH data was available for 100% (153 of 153) of 2018 patients, 100% (n = 55 of 55) of telestroke patients and 99% (n = 245/247) of patients treated using in-person assessments. There was no difference in sICH between the three groups: 1.96% (n = 3/153) in 2018, 0% (n = 0/55) 2021 telestroke, and 1.63% (n = 4/245) 2021 in-person assessments (p < 0.59). Patients could be confirmed to be either alive or dead at 3 months for 75% (n = 115 of 153) of 2018 patients, 61% (n = 34 of 55) of telestroke patients and 73% (n = 181 of 247) of patients treated after an in-person assessment. There was no difference in 3-month mortality between the three groups (p < 0.29): 14.8% (n = 17 of 115) in 2018 patients, 20.6% (n = 7 of 34) in telestroke patients, and 22.1% (n = 40 of 181) of patients treated in 2021 after in-person assessments.
Discussion
In this retrospective, single center study at our comprehensive stroke center, there was no difference in efficacy (DTN and DTP) or safety (3-month mortality, sICH) outcomes between patients treated for acute ischemic stroke in 2021 during the COVID-19 pandemic using telestroke versus in-person assessments. Our results are consistent with other studies that have reported on the efficacy and safety of using telestroke in hub-and-spoke models of care.8,12,13 To our knowledge, this is the first study to report on clinical outcomes using telestroke for patients with acute ischemic stroke who present to a comprehensive stroke center.
In this study, the only differences in median DTN were between patients treated with in-person assessments in 2018 versus 2021. This difference was most likely due to worse DTN times for patients who presented after-hours in 2018 versus 2021. We hypothesize that the after-hours DTN times for in-person patients in 2021 were better than those in 2018 because of telestroke. In 2018, neurologists would have had to come from home for every after-hours acute stroke activations, which can take time depending on the time of day, traffic, weather, the distance the neurologist lives from the hospital, etc. In 2021, neurologists could use telestroke to assess and treat after-hours patients if they thought that their travel time could adversely affect the DTN time. The patients treated after-hours with an in-person assessment in 2021 would therefore have been a subset of the patients treated after-hours in 2018 and they would have been selected to have a lower DTN than the 2018 after-hours patients.
Retrospective, single center cohort studies are prone to selection bias, incomplete records, and confounders. In this trial, selection bias was possible because the treating neurologist knew some clinical information about the patient from the patch nurse before making the decision to treat with telestroke or not. However, the effect of this selection bias is likely small because the biggest determining factor for if telestroke was used was whether the patient came in after-hours or not (91% of telestroke cases presented after-hours). Our patient database did have some missing data for mortality (Table 1). The proportion of missing data was similar across the three groups. Differences between the missing mortality data could result in a difference in mortality rates between the groups, but this is unfortunately hard to control for in this retrospective study. One confounder was that only 63% (7 of 11) of the neurologists in this study used telestroke. However, when we looked at outcomes for only the neurologists who used telestroke, there was no difference in their safety or efficacy outcomes between telestroke versus in-person care. This was a moderate-sized study (n = 455), so the lack of a significant difference between telestroke and in-person care could be from a lack of power. However, the absolute differences in the clinical outcomes between the three groups were small. Even if statistical significance were demonstrated with a larger trial the clinical significance of this result would be low. Finally, this study was done during the COVID-19 pandemic. The pandemic has been previously shown to have decreased the rates of patients presenting with stroke, 14 lower ED volumes, 15 and increase the necessity of infection prevention and control measures. 16 However, despite these differences, the outcomes for patients treated at our hospital in 2021 were similar to pre-pandemic patient outcomes from 2018. For this reason, it is our opinion that this study's results will be generalizable to patients with stroke treated with telestroke at other comprehensive stroke centers beyond the pandemic.
As stroke neurologists, ED staff, and hospital networks become more comfortable with virtual care, we anticipate telestroke assessments will become more commonplace even in urban tertiary care centers like ours. At that point, larger case series could give a better estimate of telestroke's safety, efficacy, and feasibility. In the future, quality improvement studies using feedback from healthcare providers could optimize telestroke-delivered care. For example, in this study we did not examine patient or physician satisfaction. Future studies could examine this to improve patient-centered outcomes and help find ways to make patients more comfortable speaking to a physician virtually. Finally, stroke neurologist burnout is a growing concern. telestroke is an option to reduce provider burnout by decreasing travel times, allowing one provider to cover multiple sites to reduce call frequency and make being on-call for acute stroke assessments less onerous. In the future, quality of life studies could assess if telestroke is an effective way to address stroke neurologist burnout.
In summary, the results of this study found that there were no differences in the clinical outcomes for patients with acute stroke who were treated at our comprehensive stroke center using telestroke versus in-person assessments during the COVID pandemic. The demand for acute stroke assessments will increase in the future with our ageing population, 17 increasing prevalence of vascular risk factors and expanding indications for acute stroke therapy. The results of this paper suggest that this increased demand can be met effectively and safely at comprehensive stroke centers though the expanded use of telestroke.
Footnotes
Acknowledgements
We thank Dr Nazia Sharfuddin and Mr Jonathan Hersh for their help in organizing this project as part of the Quality Improvement Experiential Student Training (QuEST) Program at the University of Toronto Temerty Faculty of Medicine and Ms Nicole Pageau, Dr Yael Perez and Mr Lauren Bauer from Trillium Health Partners for their support of this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.