
Abstract
Background
Telemonitoring and telerehabilitation can support home-based pulmonary rehabilitation (PR) and benefit patients with lung diseases or COVID-19. This study aimed to (1) identify which telemonitoring and telerehabilitation interventions (e.g. videoconferencing) are used to provide telehealth care for people with chronic respiratory conditions or COVID-19, and (2) provide an overview of the effects of telemonitoring and telerehabilitation on exercise capacity, physical activity, health-related QoL (HRQoL), and healthcare use in patients with lung diseases or COVID-19.
Methods
A search was performed in the electronic databases of Ovid MEDLINE, EMBASE, and Cinahl through 15 June 2021. Subject heading and keywords were used to reflect the concepts of telemonitoring, telerehabilitation, chronic lung diseases, and COVID-19. Studies that explored the effect of a telerehabilitation and/or telemonitoring intervention, in patients with a chronic lung disease such as asthma, chronic obstructive pulmonary diseases (COPD), or COVID-19, and reported the effect of the intervention in one or more of our outcomes of interest were included. Excluding criteria included evaluation of new technological components, teleconsultation or one-time patient assessment.
Results
This scoping review included 44 publications reporting the effect of telemonitoring (25 studies), telerehabilitation (8 studies) or both (11 studies) on patients with COPD (35 studies), asthma (5 studies), COPD and asthma (1 study), and COVID-19 (2 studies). Patients who received telemonitoring and/or telerehabilitation had improvements in exercise capacity in 9 out of 11 (82%) articles, better HRQoL in 21 out of 25 (84%), and fewer health care use in 3 out of 3 (100%) articles compared to pre-intervention. Compared to controls, no statistically significant differences were found in the intervention groups’ exercise capacity in 5 out 6 (83%) articles, physical activity in 3 out of 3 (100%) articles, HRQoL in 21 out of 25 (84%) articles, and healthcare use in 15 out of 20 (75%) articles. The main limitation of the study was the high variability between the characteristics of the studies, such as the number and age of the patients, the outcome measures, the duration of the intervention, the technological components involved, and the additional elements included in the interventions that may influence the generalization of the results.
Conclusion
Telemonitoring and telerehabilitation interventions had a positive effect on patient outcomes and appeared to be as effective as standard care. Therefore, they are promising alternatives to support remote home-based rehabilitation in patients with chronic lung diseases or COVID-19.
Introduction
Chronic lung diseases and COVID-19 are leading causes of disease, death and disability globally1–4 which entail a substantial burden on the individual5–7 and healthcare systems.8,9 Pulmonary rehabilitation (PR) is defined by the “National Heart, Lung, And Blood Institute” as a “supervised program that includes exercise training, health education, and breathing techniques for people who have certain lung conditions or lung problems due to other conditions” 10 is widely recognized as an important treatment for patients suffering from chronic respiratory diseases,11,12 and has been recommended as a potential beneficial intervention for post-COVID-19 patients. 13 PR has been shown to provide statistically and clinically significant improvements in physical activity, exercise capacity, self-efficacy, and health-related quality of life (HRQoL), and a decrease in healthcare use in patients with lung diseases.11,14 Despite the multiple benefits identified, it has been estimated that less than 3% of people with chronic lung diseases accessed PR programs 15 which are also hampered by low participation, insufficient attendance, and high dropout rates.16–19 Home-based PR programs seem to offer a promising alternative20,21 to overcome well-known PR barriers including, but not limited to, symptom severity, acute exacerbations, transportation, financial difficulties, disruption of daily routines and access to care in remote locations.17,18,22–25 In addition, the COVID-19 pandemic has highlighted the need for delivering PR programs remotely, safely, and efficiently. 15
Advances in technology have boosted at-home health service delivery26,27 and popularized telehealth for those with chronic diseases.27–30 Telehealth can be described as the use of electronic information and communication technology by professional health care providers to provide and support at-home health care to patients in case of long distances. 31 Evidence indicates that telehealth can enhance healthcare use,32,33 especially among the populations who cannot otherwise access care. 34 There are several terms used to describe telehealth systems based on their applications. Telerehabilitation is defined as the delivery of rehabilitation services (e.g. assessment, prevention, treatment, education, and counseling) via information and communication technologies. 35 It has been associated with lower healthcare costs compared with traditional inpatient or person-to-person rehabilitation.36,37 Recent advances in sensor technology have also enabled remote patient telemonitoring, which is the transmission of physiological and other noninvasive data (e.g. heart rate, blood pressure, oxygen saturation, weight, symptoms, etc.) directly to care providers via Bluetooth or digital/broadband/wireless.36,38 Telemonitoring can be used to recognize and treat changes in the patient's health status as a stand-alone approach (e.g. early detection) or as part of a telerehabilitation intervention. This paper focuses on telemonitoring and telerehabilitation as types of telehealth that can support home-based PR and benefit patients with lung diseases or COVID-19. The purpose of this paper is to depict the use of telemonitoring and telerehabilitation interventions in patients with chronic lung diseases, such as asthma, chronic obstructive pulmonary diseases (COPD), or COVID-19 patients and their association with patient health outcomes. The objectives of this paper were to (1) identify which telemonitoring and telerehabilitation interventions (e.g. videoconferencing) are used to provide telehealth care for people with chronic respiratory conditions or COVID-19, and (2) provide an overview of the effects of telemonitoring and telerehabilitation on exercise capacity, physical activity, HRQoL, and healthcare use in patients with lung diseases or COVID-19.
Methods
A health sciences librarian (HL), in consultation with the research team, developed and performed a search in the electronic databases of Ovid MEDLINE, EMBASE, and Cinahl through 15 June 2021. Subject heading and keywords were used to reflect the concepts of telemonitoring, telerehabilitation, chronic lung diseases, and COVID-19 (see supplement 1 for the OVID Medline search). The search was limited to full-text articles published in the English language with full text available. This scoping review of the literature, which has not been registered, was conducted using Preferred Items for Systematic Reviews and Meta-Analysis (PRISMA) (Figure 1). The search retrieved 3013 references. After removing the duplicates, two researchers screened 2941 titles and abstracts and read in full the text of 227 articles. Both researchers reviewed independently the articles and selected 44 publications that met the inclusion criteria of (1) the study explored the effect of a telerehabilitation and/or telemonitoring intervention, (2) in patients with a chronic lung diseases, such as asthma, COPD, or COVID-19 patients, (3) and reported the effect of the intervention in one or more of the following outcomes: exercise capacity, physical activity, HRQoL, or healthcare use. The main reasons for exclusion of the studies included: (1) the study aimed to validate a new technological component instead of evaluating an intervention, (2) the intervention was only teleconsultation or one-time assessment, or the effect of the intervention in one of the (3) populations or (4) outcomes of interest were not reported.
PRISMA—Literature selection process.
Data extraction and synthesis
Information from the 44 articles was summarized in Table 1, which presented: (1) author(s)’ name, (2) country of the study, (3) type of study, (4) intervention group and control group, (5) technology used in the study, (6) duration of the intervention, (7) participants’ condition, and (8) description of the study population. The effect of telemonitoring and telerehabilitation on physical activity, exercise capacity, health-related quality of life and healthcare use in patients with chronic lung diseases or COVID-19 was extracted and compiled in Tables 2–4.
Main characteristics of the studies included.
SD: standard deviation; PR: pulmonary rehabilitation; SBP: standard best practice; N/A: not applicable; NR: not reported.
Effect of telemonitoring and/or telerehabilitation on physical activity and exercise capacity in patients with lung diseases or COVID-19.
IG: Intervention group; CG: control group; 6MWT: 6-min walking test NA: not applicable. ↑: significantly better outcome; =: no significant difference in outcome change between groups. not reported. NR: data and/or significance level not reported.
Effect of telemonitoring and/or telerehabilitation on health-related quality of life and/or health status in patients with lung diseases or COVID-19.
IG: Intervention group; CG: control group. NA: not applicable. EQ-VAS: EuroQol-visual analogue scales; CAT: COPD assessment test; SGRQ: St George's Respiratory Questionnaire; CRQ: chronic respiratory disease questionnaire; ↑: significantly better outcome; =: no significant difference in outcome change between groups. NR: data and/or significance level not reported.
Effect of telemonitoring and/or telerehabilitation on healthcare use in patients with lung diseases.
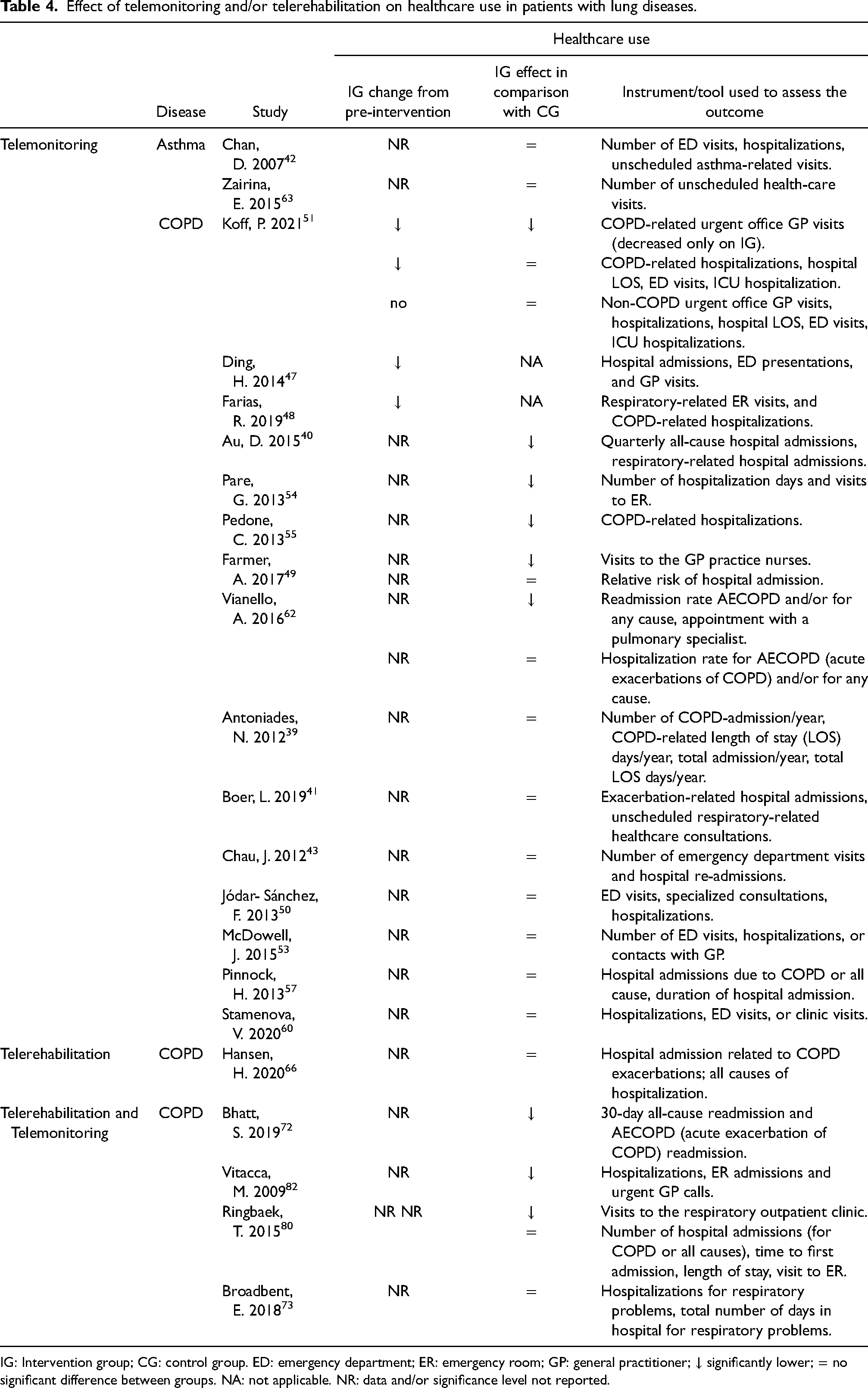
IG: Intervention group; CG: control group. ED: emergency department; ER: emergency room; GP: general practitioner; ↓ significantly lower; = no significant difference between groups. NA: not applicable. NR: data and/or significance level not reported.
Results
All 44 manuscripts were original research published between 2005 and 2021. The studies were conducted in Australia (5), Canada (5), USA (5), Denmark (4), Italy (4), Spain (4), UK (4), China (3), the Netherlands (3), Ireland (2), New Zeeland (1), Norway (1), Russia (1), Sweden (1), and 1 study in Austria, Germany, and Switzerland. The main characteristics of the included studies are presented in Table 1. Twenty-eight manuscripts reported on randomized controlled studies, 11 pre-post intervention studies, 2 matched population studies, 1 controlled non-randomized study, 1 quasi-randomized clinical trial, and 1 cohort study. Follow-up periods reported range between 10 days and 36 months. The number of participants involved in intervention groups of the studies ranged between 8 and 619 (median: 45). Thirty-five of the studies were conducted in patients with COPD, 5 in patients with asthma, 1 included patients with COPD and/or asthma, and 2 in patients with COVID-19. Two studies were conducted on children and the rest on adult patients (Table 1).
Interventions and technology
Table 1 describes the details of the interventions and the technology used. The effect of telemonitoring (25 studies), telerehabilitation (8 studies) or both interventions combined (11 studies) were reported on the physical activity, exercise capacity, HRQoL and healthcare use of patients with respiratory diseases or COVID-19. These technology-enabled remote interventions were implemented as a stand-alone approach or in combination with other elements (e.g. standard care). Twenty-seven of the studies involved mobile apps, web pages, or virtual platforms accessed using a laptop, tablet or smartphone.39,41–44,46,47,49,55,59–61,63–69,71,72,74–76,79–81 In two studies the intervention was delivered using a teleconference platform,66,76 and one social platform. 67 Other transmitting devices/systems used in the studies included the health buddy device,40,51 the iRobi robot, 73 a PalmOne, 45 touch screen telemonitoring equipment, 57 a home health system connected to a phone line, 53 a computer-linked interactive phone tele-system, 48 a tele-modem,50,54,62,82 a satellite platform, 83 computer or push-bottom telephone, 58 handheld monitor connected to a phone line, 52 a digital pen and health dairy paper together with SMS. 56 Portable devices used to monitor patients’ remotely included pulse oximeters (oxygen saturation and heart rate), spirometers (lung function), and accelerometers (physical activity) among others. Sixteen studies used more than one device to collect patient data. Information from the monitoring devices was collected using Bluetooth technology, manually entered, or verbally reported by participants to the research team or healthcare providers.
Exercise capacity and physical activity
A significant improvement in exercise capacity was reported in COVID-19 patients who received home-based telerehabilitation 64 (Table 2). Increased baseline exercise capacity was also found in COPD patients who received telemonitoring, 51 telerehabilitation (3 of 4 studies),66,69,70 or a combination of both.76–78,81 However, only one study that explored the effect of telemonitoring 51 and another that combined telemonitoring and telerehabilitation 81 found greater improvement in exercise capacity in intervention groups compared to controls. Telerehabilitation76–78,81 alone or in combination with telemonitoring was not associated with changes in physical activity compared to control groups among COPD patients.66,71,81
HRQoL and/or health status
Overall well-being improved in 83% of COVID-19 patients who participated in an intervention involving telerehabilitation and telemonitoring 75 (Table 3). Telemonitoring interventions were associated with an improvement in HRQoL in patients with asthma42,45,58,61,63 and COPD (4 of 6 studies),46,49,51,60 and no changes in HRQoL were identified in one study that included both asthma and COPD patients combined. 44 Nevertheless, when compared to control groups, telemonitoring was associated with a greater improvement in HRQoL only in 75% (3 of 4) of studies in asthma patients46,49,51,58,60,61,63 and in 23% (3 of 13) of studies in COPD patients.49,51,53 Telerehabilitation65–70,79 alone and the combination of telerehabilitation with telemonitoring76–78,81 were associated with improvement in HRQoL in COPD patients. However, no significant difference in HRQoL change was found between the intervention groups and controls.66–68,70,71,73,74,78,81
Healthcare use
A decrease in pre-intervention hospital admissions, length of hospitalization, and visits to the emergency department and GP's office were reported in COPD patients who participated in telemonitoring interventions.47,48,51 Furthermore, 6 out of 13 studies reported fewer urgent visits to GP's office, 51 fewer visits to the pulmonary specialist 62 and nurse practitioner, 49 fewer hospital admissions,40,55 and readmissions, 62 fewer days of hospitalization, and fewer ER visits 54 in patients with COPD who received telemonitoring compared to control groups. However, 7 of 13 studies found no significant difference in health care use between controls and patients with COPD,39,41,43,50,53,57,60 who participate in telemonitoring interventions, and the same was reported in two studies among patients with asthma.42,63 No significant differences were found in COPD exacerbation-related hospital admission or in all causes of hospitalization between COPD participants of a telerehabilitation program compared with a conventional pulmonary rehabilitation (PR) program. 66 Three of 4 studies reported lower use of healthcare in COPD patients who participated in interventions combining telerehabilitation and telemonitoring compared with control groups.72,80,82
Discussion
This paper aimed at portraying the use of telemonitoring and telerehabilitation in patients with chronic lung diseases such as asthma, COPD or COVID-19 patients and the effects of these modalities of intervention on physical activity, exercise capacity, health-related quality of life and healthcare use. A scoping review methodology was followed to explore the literature in the field. 27.3% of the studies retrieved were published after 2020 demonstrating the expanding need for technology in PR, especially after the rise of COVID-19. The first objective was to identify the telemonitoring and telerehabilitation interventions that are used to provide telehealth care for people with chronic respiratory conditions or COVID-19. The literature review identified various technologies and technology-based approaches used to provide telemonitoring and/or telerehabilitation interventions for patients with asthma, COPD, or COVID-19. The technologies used were classified into two types. The first type included portable and mobile technologies to capture physiological and other-non-invasive variables measured by patients themselves at home (e.g. heart rate, oxygen saturation) and the second type included information and communication technologies that allow seamless transfer of health data from the remote location to the healthcare provider. Overall, technologies were diverse, involved various levels of complexity, and were deployed in specific ways depending on the cases used. As such, we have classified the interventions into telemonitoring where only the surveillance of physiological and other non-invasive variables was needed, telerehabilitation where a PR or exercise intervention was administered remotely, or a combination of both.
The second objective of this paper was to provide an overview of the effects of telemonitoring and telerehabilitation on exercise capacity, physical activity, HRQoL, and healthcare use in patients with lung diseases or COVID-19. Results indicated that telemonitoring and telerehabilitation were associated with an improvement in exercise capacity, higher HRQoL, and lower healthcare use in these patients. Furthermore, these interventions produced outcomes comparable to standard care, which aligns with previous evidence that reported similar benefits of telerehabilitation to traditional in-person outpatient PR programs.84,85 Previous evidence has also suggested that telemonitoring interventions can contribute to better disease management, higher patient empowerment, higher patient engagement and satisfaction, facilitate communication between the patient and healthcare team, and facilitate data collection and data access in patients with COPD. 86 Some potential barriers associated with these interventions included heterogeneity of care, lack of patient comfort with technology, patient resistance, time-consuming, increased workload for healthcare providers and staff shortages. 86 From the cost-effective perspective, evidence suggested that although technology-based interventions require an initial financial investment, they will substantially reduce costs in the long-term, potentially due to a reduction in healthcare use and travel costs. 87
Overall, evidence suggested that telemonitoring and telerehabilitation are potentially valuable mechanisms to improve patient care and access, especially in rural areas, 88 and do not increase mortality rates. 89 Therefore, policy and decision-makers should consider supporting the implementation of telemonitoring and telerehabilitation interventions by providing an initial investment associated with the cost of the equipment, regulating the practice of telerehabilitation including protected time for healthcare providers, and involving in-institution information and technology services to support data transmission and enable secure remote sessions.90,91 Future studies should explore mechanisms to reduce potential barriers associated with the use of technology-based interventions, such as lack of standardization and cost-effectiveness analyses.
Strengths and limitations
The results of this study contribute to filling a significant knowledge gap about the value of telemonitoring and telerehabilitation in the management of patients with chronic lung diseases or COVID-19. This knowledge is needed among the first priorities identified by the patients and clinicians after COVID-19 widely affected the delivery of rehabilitation services.92,93 63.6% of the retrieved manuscript reported on randomized controlled trials demonstrating the current need for evidence about the effectiveness of telemonitoring and telerehabilitation in patients with chronic lung diseases or COVID-19. This paper presented the evidence available as of June 2021. The generalizability of the results of this study may be influenced by the higher variability between the characteristics of the studies included such as the number and age of the patients, outcome measurements, length of the intervention, technological components involved, and additional elements included (e.g. education components, type and numbers of healthcare providers involved, etc.). Due to this heterogeneity, authors suggested a cautious interpretation of the results and compiled the studies characteristics in Table 1 to facilitate the readers’ interpretation.
Conclusion
Telemonitoring and telerehabilitation interventions had a positive effect on patient exercise capacity and HRQoL and are associated with fewer healthcare use in patients with chronic lung diseases such as asthma, COPD, or post COVID-19. Furthermore, the results indicated that the outcomes of these interventions are comparable to standard care. Therefore, they are promising alternatives to support remote home-based rehabilitation in this group of patients that should be supported by policy and decision-making.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X221122124 - Supplemental material for Effect of telemonitoring and telerehabilitation on physical activity, exercise capacity, health-related quality of life and healthcare use in patients with chronic lung diseases or COVID-19: A scoping review
Supplemental material, sj-docx-1-jtt-10.1177_1357633X221122124 for Effect of telemonitoring and telerehabilitation on physical activity, exercise capacity, health-related quality of life and healthcare use in patients with chronic lung diseases or COVID-19: A scoping review by Diana C Sanchez-Ramirez, Margriet Pol, Hal Loewen, and Mohamed-Amine Choukou in Journal of Telemedicine and Telecare
Footnotes
Acknowledgements
The authors would like to thank Yang Zhaoyun, Rachel Adodo, and Amarzish Qadeer for their contribution to article screening and data extraction.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the start-up funds provided to Dr Sanchez-Ramirez by the University of Manitoba.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.