
Abstract
Introduction
The COVID-19 pandemic-related visitation restrictions started in March 2020 in Alberta, Canada. In the Neonatal Intensive Care Unit, we implemented a Virtual Communications initiative to allow parents to continue to be present with their infants, attend daily rounds, and communicate with the medical team. The purpose of this survey study was to describe our approach and evaluate the experience for families and staff.
Methods
The study surveys consisted of 13–18 questions directed toward understanding staff and family experience with the process and emotional impact using Likert scale and open-ended questions. The study team reviewed results and implemented changes in real time. Analysis was mixed quantitative and qualitative design, with descriptive data organized into themes.
Results
Twenty-six surveys were completed by 16 staff (62%) and 10 parents (38%). About 50% to 100% of respondents agreed or strongly agreed with statements addressing the quality and value of the virtual sessions. Staff identified challenges with slow devices and need for awareness and education. Both staff and parents expressed gratitude for the initiative and an overall positive experience.
Discussion
Offering Virtual Rounds and Bedside Presence in the Neonatal Intensive Care Unit is a well-received and feasible alternative to in-person presence that allows parents to stay involved and connected to their infants. Families have a better understanding of their babies’ clinical status and plans with an overall positive experience.
Introduction
Family centred care (FCC) is a framework approach that focuses on enabling parents to participate in the planning and delivery of healthcare to their child. 1 Parental presence and involvement in their child's care greatly contributes to improved patient and family outcomes.2–5 Family Integrated Care (FICare) is an extension of the principles of FCC that has been implemented by Neonatal Intensive Care Units (NICUs) across the province of Alberta in Canada.2,6–8 In addition to improving infant outcomes such as reduced length of stay, the aim of the Alberta FICare model is to promote parent–infant connections, build parent confidence, and improve parent mental health through relational communication, education and support. 8 Barriers such as parental illness, transportation issues, or work commitments can impede the delivery of Alberta FICare and alternative arrangements are not often readily available.
The public health and institutional restrictions associated with the onset of the SARS-CoV-2 (COVID-19) pandemic have resulted in an increasing number of parents and caregivers who are unable to enter the NICU. They cannot see or interact with their infants or participate in discussions and care plans with the healthcare team. Families and healthcare providers are already describing the significant impact of the COVID-19 pandemic restrictions on parental mental health and well-being, and disruption to parent integration in care, education, and transition to home. 9
To ensure that families remain active members of the care team, the NICU at the Foothills Medical Centre (FMC) in Calgary, Alberta launched a Virtual Communications initiative. Parents can see and speak with their infants and healthcare providers or attend and participate in the daily multidisciplinary rounds using video- and audio-enabled devices. Similar work in virtual health prior to the pandemic had demonstrated parental satisfaction and interest.10,11 These efforts highlighted some crucial considerations when implementing this type of service, most notably technical challenges, staff buy-in, and the importance of support at organizational, operational, and human resources levels.10,11
An increasing number of healthcare institutions worldwide have embarked upon and described their experiences with adaptation of virtual technologies during the COVID-19 pandemic.12,13 Comprehensive description and evaluation of such Virtual Communications initiatives in the NICU may be helpful for other institutions wishing to launch or improve upon similar initiatives.
The purpose of the present study was to describe our institutional approach and evaluate the overall experience for staff and families with Virtual Communications in a Level III NICU in Calgary. Our goal was to understand the user perspective and inform quality improvement efforts to attain an effective and sustainable alternative to face-to-face communication when in-person presence is limited.
Methods
Setting and virtual communications process development
The FMC is a tertiary perinatal centre that provides services to all premature deliveries less than 32 weeks, high-risk obstetrical deliveries, and critically ill neonates in the southern part of the province of Alberta. The NICU is comprised of 39 Level III beds with average of 1100 admissions annually, including a mix of inborn and outborn infants. Out of these, approximately 120 infants are born less than 29 weeks gestation.
Alberta Health Services (AHS) first announced visitation restrictions to hospitals in relation to COVID-19 on 18 March 2020 – permitting one ‘well’ visitor at a time and no children. At this time, there was no alternative for parents and caregivers of infants admitted to the NICU. While the FMC NICU team leadership, collaborating with the Parent Advisory Council Team (PACT), hurried to find a virtual solution, AHS announced acquisition of an enterprise license for Zoom for all organizational members on 25 March 2020. Development for the Virtual Communications process began and representatives from the Legal and Privacy Department were engaged to ensure adherence to organizational standards such as the privacy and confidentiality principles from the Health Information Act and the Freedom of Information and Protection of Privacy Act as well as AHS virtual health policies (document available internally only).14,15 The first approved and configured tablet (an iPad) was provided by AHS for staff to use in the NICU on 30 April 2020 and the process was soft launched. Families wishing to participate required their own personal device. After further modifications to the process and troubleshooting which included obtaining software updates and new protective cases that enabled better audio and video quality, the NICU received one additional requested device from AHS and was able to implement the process to include the entire clinical care team with an official launch date of 28 May 2020 – over 2 months after the first visiting restrictions were announced (see Figure 1). Educational materials for staff and families such as informational handouts and a short video with frequently asked questions and how to troubleshoot technical difficulties were developed and distributed by the project team which included the study authors.
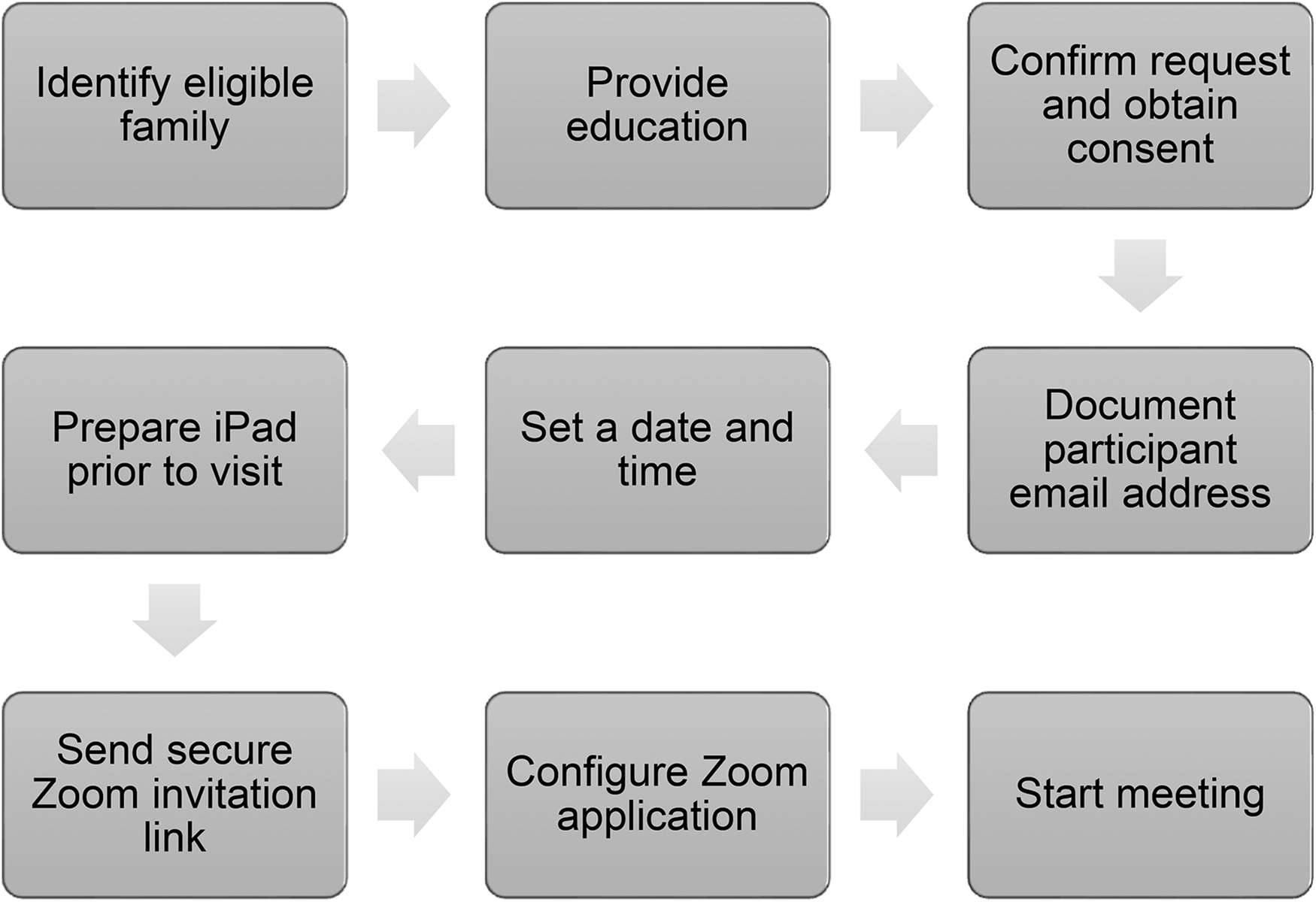
Virtual communications process flow diagram.
Study design
Mixed methods quantitative and qualitative questionnaires were developed for this study using QualtricsXM Software through the University of Calgary. Two separate versions were created, one for staff and one for families, about their recent experience with Virtual Communications in the NICU in the format of multiple choice, 5-point Likert scales, and free-text responses (see Appendices 1 and 2). General topics of interest included: participant demographics, ease of use and challenges with devices and technology, usefulness of educational handouts, burden to workflow and daily life, overall satisfaction and feedback, likelihood of using again or recommending to other parents. Staff and parents were asked about their level of confidence using Virtual Communications, if they received education, information, or support, and to rate their level of agreement with statements about process and impact on a 5-point Likert scale. They were also asked to provide comments to elaborate on their responses. Additional topics of interest for parents included: understanding medical issues and care plans, ability to participate in planning and decision making, and ability to interact and bond with infant. Finally, parents were asked to rate the degree to which they experienced a list of positive and negative emotions on a 4-point scale including ‘not at all’, ‘very little, ‘somewhat’, and ‘very much’, as directly related to their Virtual Communications session.
Ethics
The study protocol including process for informed consent and questionnaire was screened using the A pRoject Ethics Community Consensus Initiative Tool and it was determined to be ‘Low Risk’. 16 A formal letter of exemption from the University of Calgary Conjoint Health Research Ethics Board review was obtained. It was also presented to and approved by the FMC NICU Parent Advisory Council Team (PACT) as well as the Calgary Zone Neonatal Quality Improvement Committee and the questionnaire was validated by pilot testing with members of PACT. Participants provided informed consent by reviewing the purpose, expectations, and potential risks and benefits of the study and proceeding to submit in completion. No personal identifying data was collected for research purposes and participants could withdraw from the study at any time. Personal information including email addresses was collected and managed in accordance with AHS guidelines and standards. Study investigator's contact information was provided. There was no incentive to participate.
Participants
The target populations for this survey study included: (1) parents and caregivers of infants admitted to the NICU, and (2) NICU staff, including physicians, nurses, nurse practitioners, and allied health professionals. Inclusion criteria included usage of any form of Virtual Communications in the NICU (i.e. Virtual Multidisciplinary Team Rounds, Bedside Presence, or other Meeting) and ability to read and understand English.
Data collection
All families and staff who used Virtual Communications in the NICU and met the inclusion criteria were invited to complete the survey. Dissemination occurred via email of a secure link along with a brief description of the project or Quick Response (QR) code. Individuals were invited to complete the survey after any participation respective to that session and there was no restriction on the number of times an individual could respond. There was no expiration for the link or QR code but once the survey was started participants had 1 week to submit.
Data analysis
Responses were collected for 6 months from December 2020 to June 2021, with interim analysis at 2 and 4 months. Quantitative results for Likert scale questions determined agreement as either ‘strongly agree’ or ‘agree’ responses. Qualitative free-text answers were transferred verbatim to Microsoft Excel and inductively analysed by the primary investigators as described in the Association for Medical Education in Europe Guide No. 131. 18 Descriptive data was organized by topic into major and minor themes with key direct quotations extracted. Emerging themes were discussed and reviewed by the study team during interim analysis to identify areas in need of immediate improvement.
Results
Participant information
A total of 26 complete responses were received from 16 staff (62%) and 10 parents (38%). Key demographics are shown in Table 1. Most staff and parents evaluated Virtual Bedside Presence with their infant (n = 20; 77%), as opposed to Virtual Multidisciplinary Team Rounds (n = 5; 19%), and one parent did both. Parents were asked to select any reason for their participation in Virtual Communications. Of note, four parents chose ‘illness in self or family other than infant’, three selected ‘other children to care for’, and zero selected ‘preferred to in-person visit’.
Survey participant demographics.
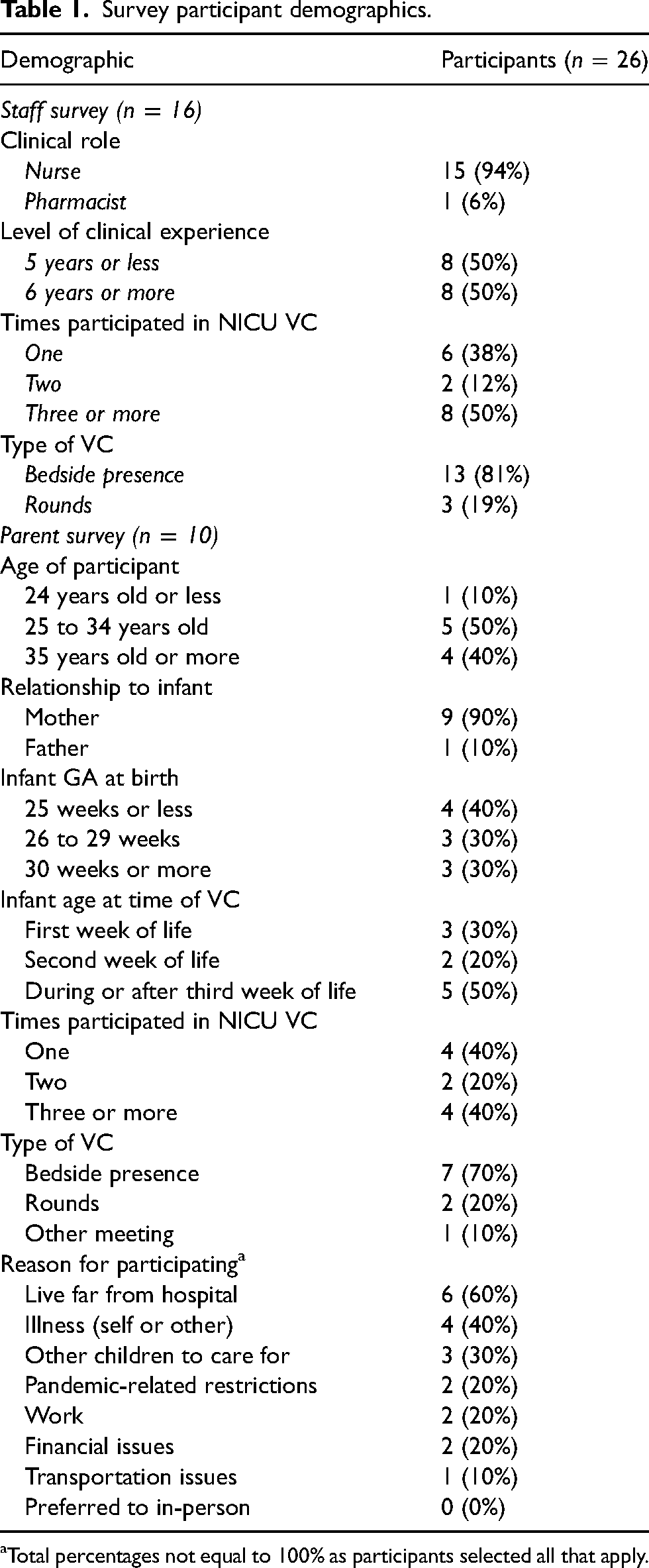
Total percentages not equal to 100% as participants selected all that apply.
Survey responses
Staff responded to 11 statements on the quality and value of the virtual sessions. Agreement level indicated by responding with ‘agree’ or ‘strongly agree’ for each statement ranged between 50% and 94% of respondents, with an average agreement rate of 73% (Figure 2, Appendix 3). Parents responded to 12 similar statements with an agreement rate of 83%, ranging from 50% to 100% of respondents agreeing per statement (Figure 3, Appendix 3). The statement with which staff had the highest rate of agreement was, ‘I perceived a positive impact on the caregiver’, and the lowest rate of agreement was with, ‘I perceived a positive impact on the infant’. There were three statements with which parents agreed the most, including, ‘Zoom was easy to set up and use’, ‘Length of session was appropriate’, and ‘This was convenient in my daily life’. The statement parents agreed with the least was, ‘During [Virtual Communications] I was able to participate in making decisions about my infant's care plans’. When parents did not agree, they most often responded ‘neutral’ and ‘disagree’ was only selected four times. Most of the staff were ‘extremely’ (38%) or ‘fairly’ (44%) confident with using Virtual Communications and 69% of all respondents had received education or information prior to use (see Appendix 4). Eighty-eight per cent of staff and 90% of parents replied that they had an ‘excellent’ or ‘good’ experience and 100% of parents said it met their expectations. Hundred per cent of all survey respondents selected ‘yes’, they would recommend Virtual Communications to other families.
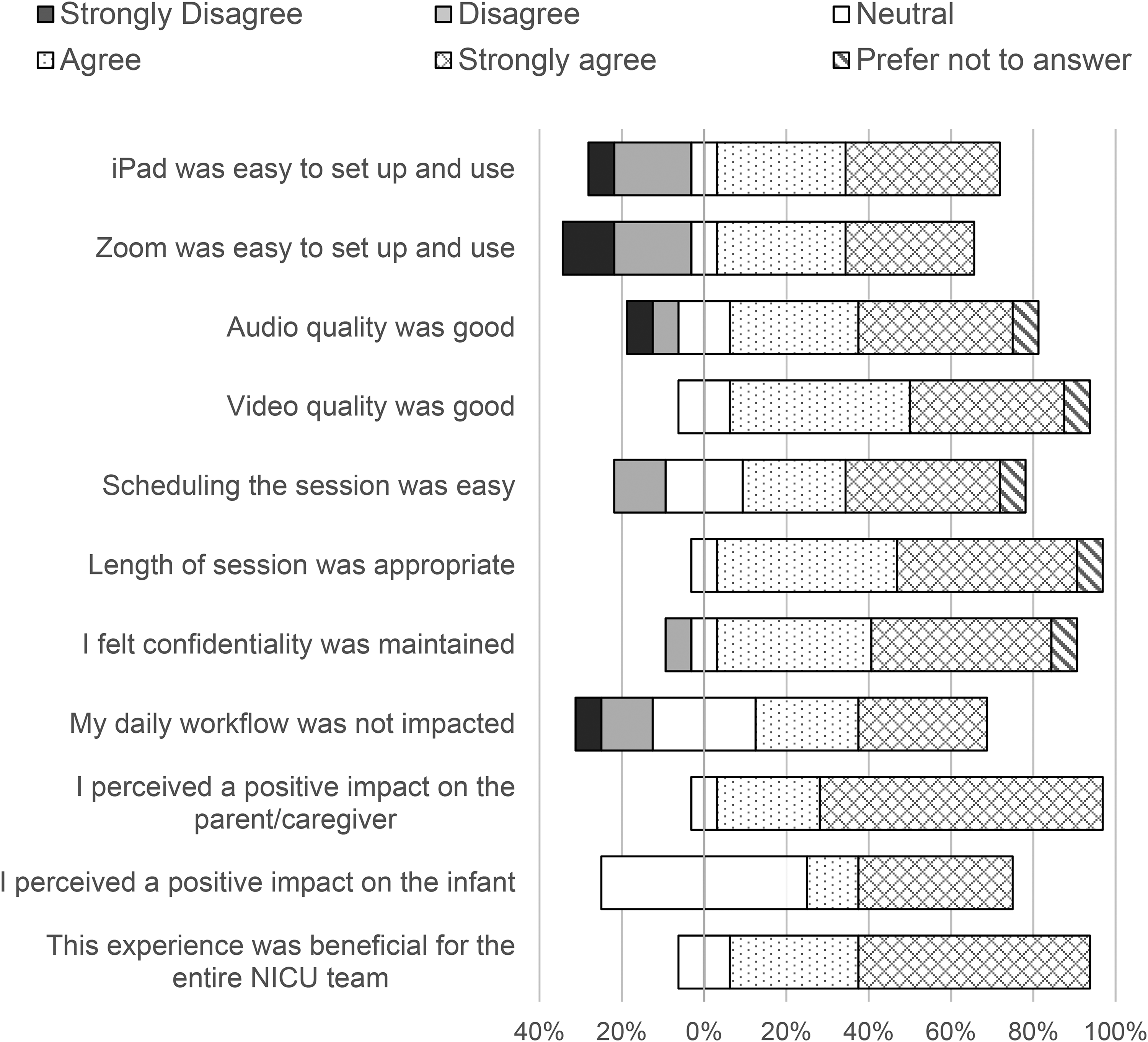
Staff responses to Likert scale questions (n = 16). The percentages of respondents who agree with the statement are shown to the right of the zero percentage line; the percentages who disagree are shown to the left; the percentages who neither agree nor disagree are split down the middle.17
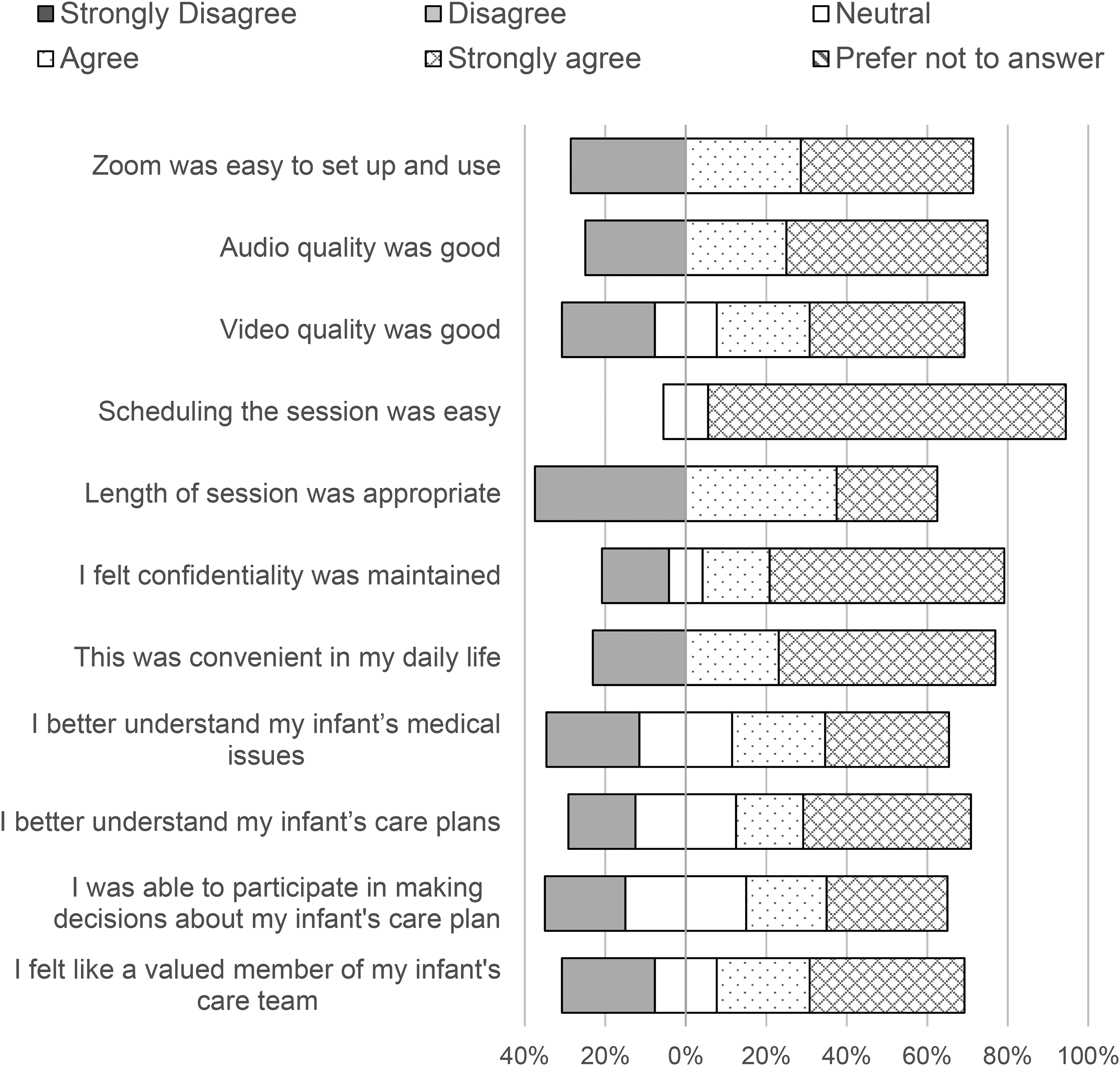
Parent responses to Likert scale questions (n = 10). The percentages of respondents who agree with the statement are shown to the right of the zero percentage line; the percentages who disagree are shown to the left; the percentages who neither agree nor disagree are split down the middle.17
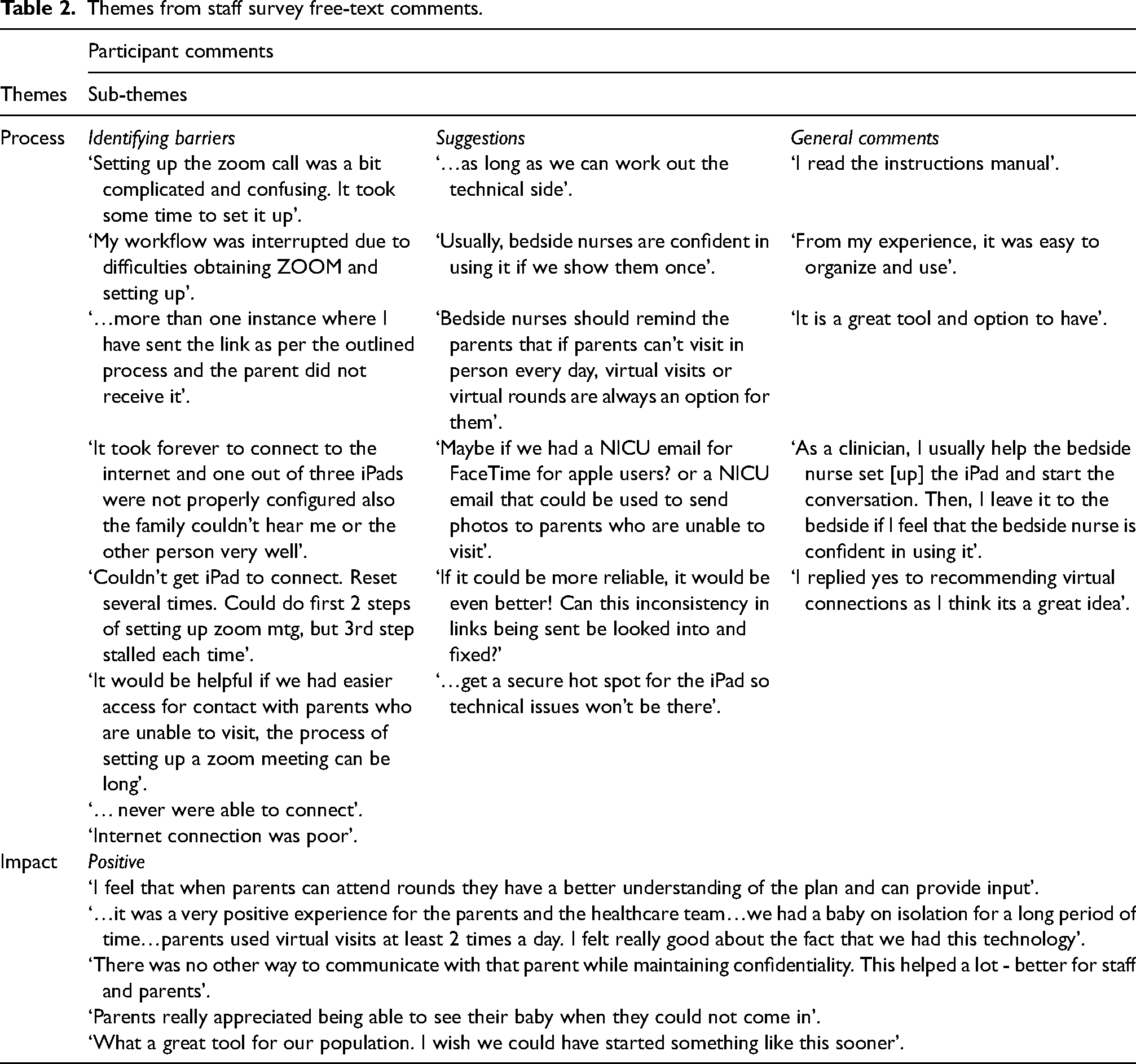
Thematic analysis of free-text comments lead to the identification of Process and Impact as the two major themes in both survey groups as presented in Tables 2 and 3. Sub-themes included Identifying barriers, Suggestions for improvement, General comments about use, and Positive and Negative impacts (staff did not make any comments about negative impact). The main barriers staff identified were issues with set up and connection, and suggestions included increasing awareness and education for all users, and technical improvement strategies like configuring wireless internet hotspots within the NICU. Parents commented less on process barriers, possibly because while staff were faced with connection issues with the hospital internet server, parents likely used home internet or cellular network technology. Parents similarly recognized the need for further staff awareness and education. The other suggestion was to consider a 24 h live feed in the NICU of each baby.
Themes from staff survey free-text comments.
Themes from parent survey free-text comments.
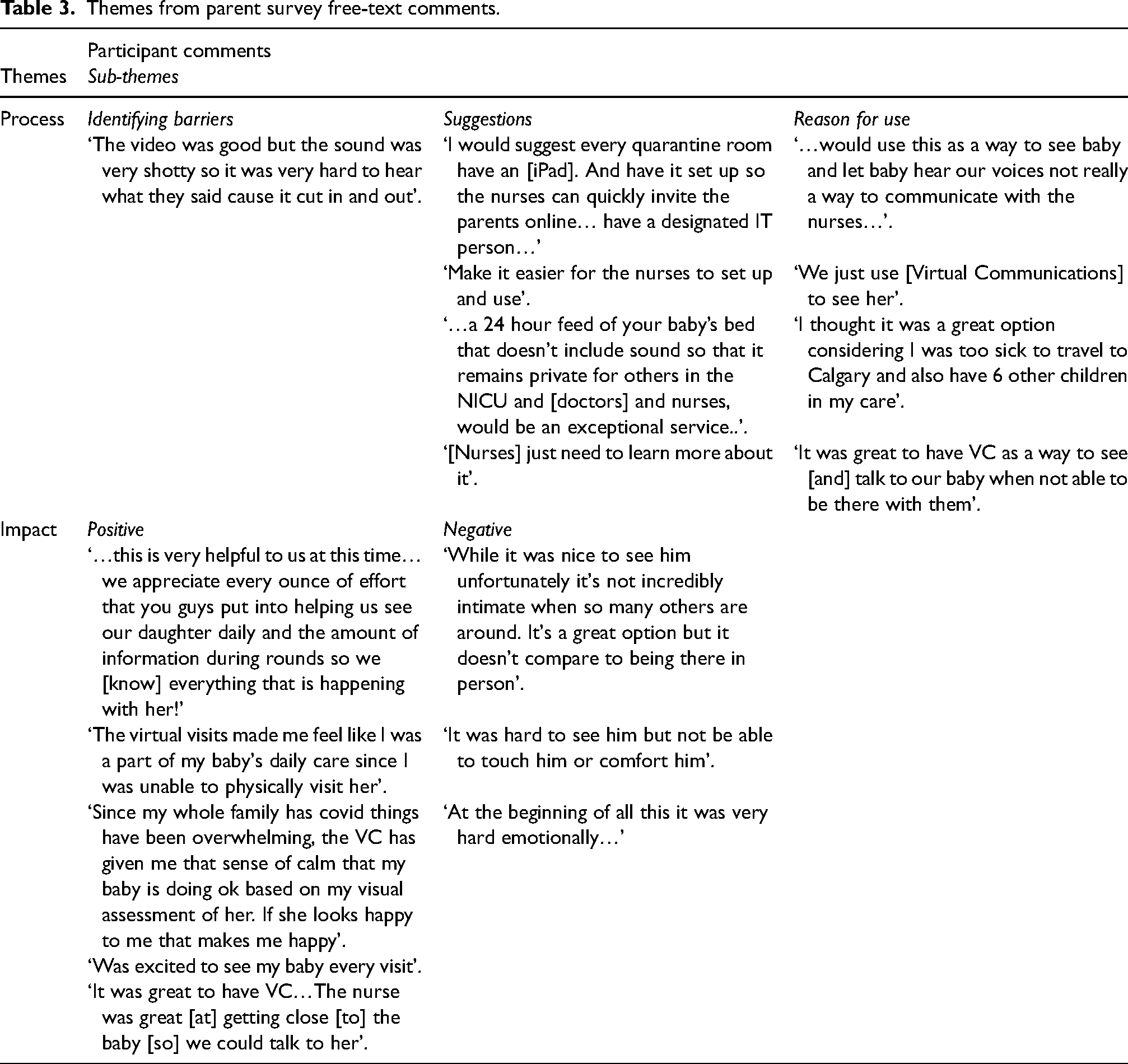
Most comments from both groups of respondents about perceived impact of using Virtual Communications were descriptions of extremely positive experiences for the healthcare team and parents. While few parents provided insight into the emotional difficulty of not being physically present, feedback was mostly encouraging about the benefits of and gratitude for the opportunity to see and speak with their babies’ and being able to remain a part of the daily care plans.
Lastly, when parents were asked to rate different emotions as directly related to their Virtual Communications session, they selected grateful, relieved, and happy as the most frequently experienced and angry, overwhelmed, and frustrated as the least frequently experienced (Figure 4).
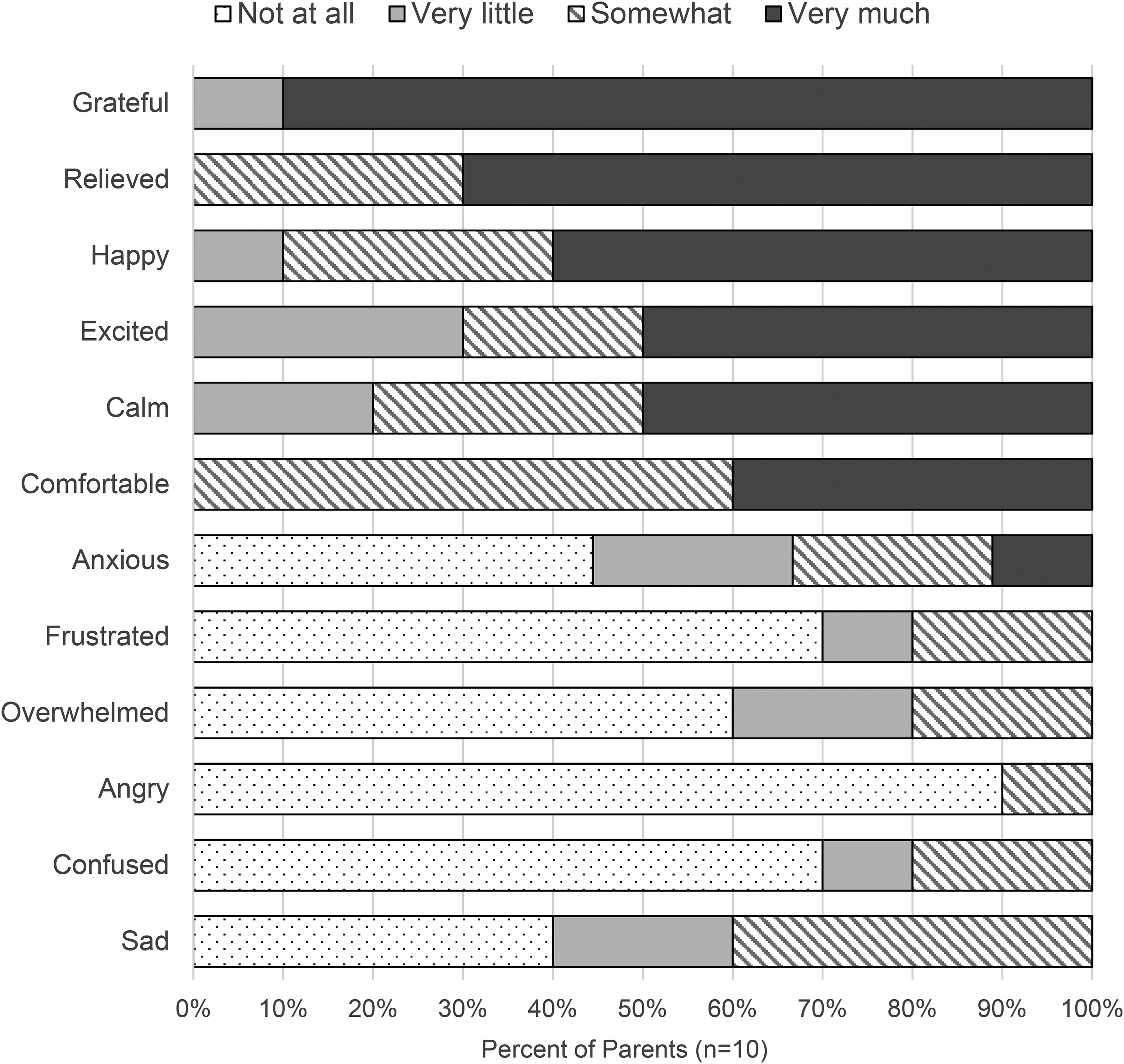
Parent emotional experiences during virtual communications in the NICU (n = 10).
Discussion
The negative impacts of the COVID-19 pandemic are recognized globally and have affected even the most vulnerable infants in the NICU and their families. 9 Our study findings were consistent with work done by others in this area – that Virtual Communications is a well-received and feasible alternative for parents and caregivers who are unable to physically be present such as during times of visiting restrictions.9–13 Additionally, our study comprehensively explored and helped leadership understand parent and staff experiences with Virtual Communications and assisted with improving the process in real time.
Detection of issues with the tablets very early in the process based on staff responses allowed leadership to quickly obtain higher quality devices to overcome this barrier to implementation. We were also informed about challenges with slow connection and time required to set up that was affirmed by the low number of respondents who took part in Virtual Rounds compared to Bedside Presence. This was partially addressed by upgrading devices and increasing support to frontline staff as indicated by improved feedback in subsequent surveys, but it has not been overcome completely and there is further work to be done. We also identified that although staff expressed feeling generally confident with process, many had not received education, information, or support. Thus, our team developed a brief video for staff to refer to as needed. We established that there was a positive overall experience for staff despite technical issues as almost all respondents ‘strongly agreed’ that there was a positive impact on the caregiver and that it was beneficial for the entire team. This evidence will be extremely useful to the sustainability of Virtual Communications in the NICU. We hope that it will encourage local staff and leadership that the time and resources required to support this service are valuable.
Parents were generally satisfied with the Virtual Communications process and there were no significant issues identified. As in staff surveys, we were alerted to the internal challenges with devices and connection. Most parents received education, information, or support, which confirmed that frontline staff were doing an excellent job. We were very encouraged that the overwhelming majority of parents reported either an ‘excellent’ or ‘good’ overall experience with Virtual Communications, and every respondent indicated that they would recommend the service to other families. We determined an overall successful endeavour in that most parents were better able to understand their infant's medical issues and care plans and felt like a valued member of the care team with participating in decisions and feeling a bond with their infants’. However, many parents indicated they were ‘neutral’ about these efforts, and a few expressed that they were not able to participate in decision making for their infant's care plans. As we did not identify a similar finding in the literature, this may require further exploration in future studies. In our context, we believe this result may have been influenced by individual motivation for use as some parents indicated they only wanted to see and interact with their baby, to know that they are doing well. Determining that each parent has unique expectations and needs during Virtual Communications has allowed us to emphasize the importance of individualizing the experience and establishing goals prior to each session. We found it very reassuring that no parent responded that they preferred Virtual Communications as we did not wish to discourage in-person presence. Similar to staff, more parents had participated in Virtual Bedside Presence, and further work is required to understand and address associated barriers to Virtual Rounds.
Finally, most parents expressed experiencing positive emotions related to using Virtual Communications. We were encouraged that a large proportion felt grateful, relieved, happy, excited, calm, and comfortable. Very few parents expressed feeling negative emotions such as sad, confused, angry, overwhelmed, or frustrated. Based on free-text comments, we determined that the parents who did feel these emotions ‘somewhat’ may have felt so in relation to being separated from their baby or seeing them in a NICU environment. Overall, this is a reassuring outcome of the survey indicating that our primary aims are being achieved.
In our experience, we identified three principal lessons that might be helpful to other organizations. First, organization-wide timely and effective communication strategies and information-sharing are crucial. In addition to minimizing time and resources wasted by duplicate efforts, this may have avoided extraneous worry and frustration by reassuring all departments within the hospital that tools and resources would soon be available. Second, organizational preparedness and adaptability in time of crisis is paramount. The recognition of a shared vision and acceptance of new technologies to support family presence during times of visitation restriction were appreciated as a priority. Organizational leadership support was a critical rate-limiting step in propelling this innovation forward. Previous requests to use Zoom had been denied due to organizational risks that were subsequently mitigated through proper process development ensuring privacy and safety of all participants. Third, access to resources and funding is time sensitive. Lack of readily available resources and funds to support process development and device acquisition was another barrier to implementation. Requests were submitted then triaged resulting in slow procurement of devices for the NICU; delaying process launch by nearly 2 months. Large organizational investments in technology including telehealth platforms and devices as well as teams dedicated to support the process would significantly improve time to implementation.
Limitations
One of limitations of this study is the small sample size. Secondly, while the survey tool was validated, responses could have been influenced by external factors such as individual user interpretation and technical issues with completing the survey online. Furthermore, although our results indicate overall positive user experiences, there may be bias in participant selection as online survey respondents may be more technologically-savvy, English-speaking, and potentially of higher socio-economic and educational status. Finally, other institutions may find little use in the description of our approach if it does not fit within the policies and practices of their organization.
Conclusion
The development and implementation of Virtual Communications in a Level III NICU was an onerous but invaluable process. Through the dissemination and analysis of surveys to staff and parent participants, we have demonstrated that offering this service is deeply appreciated to fulfil a variety of needs including allowing parents to see and interact with their infants when in-person presence is not possible, and to remain an active member of the medical care team. This information has been used to expand implementation of Virtual Communications across Level II NICUs in Calgary. We hope that this comprehensive description and evaluation will inspire other institutions wishing to embark or improve upon similar initiatives, and that it will be useful at a local organizational level to keep Virtual Communications a sustainable process that we can continue to offer families long into the future.
Footnotes
Acknowledgements
The authors would like to thank the families and staff, including the NICU Parent Advisory Care Team, at the Foothills Medical Centre NICU for their participation and support with this initiative and study.
Authors contributions
Ashley Blagdon and Ayman Abou Mehrem conceptualised the study, developed the survey, analysed the data, drafted the initial manuscript and reviewed and revised the final manuscript. Dani Smith and Tara Bramfield conceptualized the study, developed the survey and reviewed and revised the initial and final manuscript. Amuchou Soraisham contributed to the study concept, critically reviewed and edited the initial manuscript and revised the final manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Appendix 1. Staff Survey Questions
How many times have you participated in Virtual Communications in the NICU (including the most recent time)?
1 2 3 4 or more In which type of Virtual Communication in the NICU did you most recently participate?
Bedside Virtual Visit Virtual Rounds Other Virtual Meeting (specify if possible) What is your clinical role in the NICU?
Registered Nurse Nurse Clinician Respiratory Therapist Fellow/Resident/Nurse Practitioner Neonatologist Other/Allied Health (please specify) Please indicate your level of experience within your clinical area:
0 to 2 years 3 to 5 years 6 to 9 years 10 to 19 years 20 years or more How confident were you using Virtual Communications in the NICU?
Not at all confident A little confident Fairly confident Extremely confident Did you receive any education, information, or support for using Virtual Communications in the NICU? (please comment on how we can improve)
Yes No Rate your level of agreement with the following statements about your most recent Virtual Communications in the NICU experience:
Please explain your responses to the previous Q7. (particularly if you replied with ‘Strongly agree’ or ‘Strongly disagree’): Rate your level of agreement with the following statements about your experience with Virtual Communications in the NICU:
Please explain your responses to the previous Q9. (particularly if you replied with ‘Strongly agree’ or ‘Strongly disagree’): Rate your overall experience with Virtual Communications in the NICU:
Excellent Good Neutral Poor Terrible Would you recommend Virtual Communications in the NICU to families who cannot visit?
Yes No Please provide any additional comments, feedback or suggestions for improvement:
Strongly
agree
Agree
Neutral
Disagree
Strongly
disagree
Prefer not
to answer
iPad was easy to set up and use.
Zoom was easy to set up and use.
Audio quality was good.
Video quality was good.
Scheduling the session was easy.
Length of session was appropriate.
I felt confidentiality was maintained.
My daily workflow was not impacted.
Strongly agree
Agree
Neutral
Disagree
Strongly disagree
Prefer not
to answer
I perceived a positive impact on the Parent.
I perceived a positive impact on the Infant.
I believe this experience was beneficial for
the entire NICU Care Team.
Appendix 2. Parent Survey Questions
What gestational age was your infant at birth?
25 weeks or less 26 to 29 weeks 30 to 34 weeks 35 weeks or more How old was your infant when you most recently participated in Virtual Communications in the NICU?
First week of life Second week of life During or after the third week of life How many times have you participated in Virtual Communications in the NICU (including the most recent use)?
1 2 3 4 or more What is your age?
Less than 18 years 18 to 24 years 25 to 34 years 35 to 44 years 45 years or older What is your relationship to the infant?
Mother Father Other caregiver, ie. Grandparent (please specify) In which type of Virtual Communications in the NICU did you most recently participate?
Bedside Virtual Visit (w/ infant) Virtual Rounds (w/ medical team) Other Virtual Meeting (specify if possible) I'm not sure For what reason(s) did you use Virtual Communications in the NICU? (select all that apply)
Illness (in self or family other than infant) Work Other children to care for Live far from hospital (in Calgary) Live far from hospital (outside Calgary) Transportation issues Financial issues Hospital / unit restrictions Preferred virtual visit instead of in-person visit Other (please specify): If possible, please explain why you preferred to do virtual visit instead of in-person visit: Did you receive any education or information about using Virtual Communications in the NICU? (please comment on how we can improve)
• Yes • No Rate your level of agreement with the following statements about your most recent Virtual Communications in the NICU experience:
Please comment on your responses to the previous Rate your level of agreement with the following statements about your most recent experience with Virtual Communications (VC) in the NICU:
Please comment on your responses to the previous: Please tell us about any emotions that you experienced directly associated with Virtual Communications in the NICU - not related to your infant's medical condition (select any that apply):
Please provide additional comments about your emotional experience with Virtual Communications in the NICU: Did Virtual Communications in the NICU meet your expectations?
• Yes • No If not, please tell us how we can improve: Would you recommend Virtual Communications in the NICU to other families who cannot visit?
• Yes • No Please rate your overall experience with Virtual Communications in the NICU:
• Excellent • Good • Neutral • Poor • Terrible Please provide any additional comments, feedback or suggestions for improvement:
Strongly
agree
Agree
Neutral
Disagree
Strongly
disagree
Prefer not
to answer
Zoom was easy to set up and use.
Audio quality was good.
Video quality was good.
Scheduling the session was easy.
Length of session was appropriate.
I felt confidentiality was maintained during the call.
This was convenient in my daily life.
Strongly agree
Agree
Neutral
Disagree
Strongly disagree
Prefer not
to answer
VC helped me better understand my infant's medical issues.
VC helped me better understand my infant's care plans.
During VC I was able to participate in making decisions about my infant's care plan.
VC helped me feel like a valued member of my infant's care team.
During VC I felt a bond with my infant.
Not at all
Very little
Somewhat
Very much
Happy
Sad
Excited
Confused
Relieved
Grateful
Anxious
Comfortable
Calm
Angry
Overwhelmed
Frustrated
Other (describe)