
Abstract
Ageing populations have resulted in more patients living in long-term care or nursing homes, where they face challenges to accessing prompt specialist care exacerbated in many cases by physical or cognitive decline. Electronic consultation has demonstrated an ability to improve access to specialist care for vulnerable groups and offers a potential solution to this gap in care. To support electronic consultation's uptake among long-term care homes, we created the electronic consultation long-term care utilization and savings estimator, an Excel-based tool that estimates the number of off-site appointments that patients in a long-term care home could avoid through electronic consultation, along with the consequent time and cost savings. In this brief report, we discuss the electronic consultation long-term care utilization and savings estimator's creation and function, and provide a case study using long-term care data to demonstrate its potential impact. We anticipate the electronic consultation long-term care utilization and savings estimator will be a highly impactful tool and intend to test it in real-world conditions following the relaxation of COVID-19 restrictions.
Keywords
Introduction
Ageing populations in many countries have resulted in more patients residing in long-term care (LTC) homes (i.e. nursing homes). 1 These individuals are at an elevated risk of medical error 2 and hospitalization, 3 and often receive poor transitional care. 4 One of the reasons for this is because individuals in LTC have more medical comorbidities, in addition to greater degrees of functional and/or cognitive decline than the general population. 5 Thus, their greater medical complexity may benefit from additional specialist physician care; however, it can also greatly limit the ability for LTC residents to travel to and participate in such specialist visits. Compounding this problem, research has shown that among LTC residents, the rate of specialist appointments occurring outside of LTC home (i.e. off-site) was nearly double that of on-site appointments. 6
Electronic consultation (eConsult) services present a potential solution. These web-based platforms allow primary care providers (PCPs), such as family doctors or nurse practitioners, to obtain timely specialist advice to inform patient care, minimizing the need for costly and burdensome off-site specialist visits. In Ontario, the Champlain region's BASE™ eConsult Service has been active since 2009 and has been replicated provincially as part of the Ontario eConsult Program. eConsult has been instrumental in providing accessible, cost-effective care to traditionally underserved communities and populations,7,8 and has been shown to be well-suited for the LTC environment, with a median specialist response time of 0.6 days and a mean cost of $50.00 per eConsult case compared to a mean of 79 days and $133.60 for non-urgent face-to-face referrals. 9
Though eConsult is free to use and easily accessed through a secure web portal, adoption can be limited by the lack of time busy clinicians can invest in the initial sign-up process and integration into their workflows. 9 One method of encouraging continued implementation and adoption may be the development of communication and advocacy aides that can demonstrate the value of eConsult to all relevant stakeholders including family caregivers, physicians, LTC administration, and government officials.
To accomplish this, we created a tool that can estimate the number of off-site appointments that could be avoided using eConsult, and the resultant cost and time savings of these avoided appointments. This brief report outlines the methodology used to create this tool, known as the eConsult Long-Term Care Utilization and Savings Estimator (eCLUE).
Methods
Mechanics of eConsult
eConsult is a secure online application hosted on a Microsoft SharePoint platform. To use the service, PCPs log in using any device with a web browser, enter their question into a free-text field, attach any files they deem relevant (e.g. photos, medical histories, test results), and select a specialty from a drop-down menu. A case assigner allocates the question to a specialist from the chosen specialty, based on availability. The specialist receives a notification of the case and is asked to respond within 1 week (the average response time is 2 days) with advice for the PCP, a recommendation for referral, or a request for more information. The PCP reviews the response and chooses to either ask an additional question or close the case. PCPs complete a short mandatory survey upon closing. All PCPs in Ontario are eligible to use eConsult, including those practicing in rural clinics or LTC homes. Satisfaction with eConsult has been consistently high, with users ranking the service as high or very high value in 94% of cases. 10 As of November 2021, over 3800 PCPs across Ontario are using eConsult regularly, and nearly 100,000 eConsult cases have been sent. 11
eCLUE tool concept
eCLUE consists of two sections. Section 1 estimates the expected annual number of eConsults in a given LTC home, and the number of off-site specialist appointments that could be avoided due to eConsult. Section 2 estimates the associate cost and time savings for these avoided appointments, broken down into stakeholder-specific categories including resident/family, LTC home, and ministry (i.e. the provincial government). eCLUE was developed over a period from June 2019 to December 2019 in five phases (Supplemental File 1), with its plans for validation and use on hold due to the COVID-19 pandemic.
Data sources
eCLUE uses health care utilization data on Ontario residents obtained from the health administrative datasets of ICES and the Champlain BASE™ eConsult Service.
ICES
ICES (formerly known as the Institute for Clinical Evaluative Sciences), is a research institute that houses health administrative data of individuals living in Ontario, Canada. An ICES study conducted by Shaver et al. 6 explored specialist physician visitation patterns across Ontario LTC homes from 2007 to 2016, determining the number of off-site face-to-face specialist physician appointments that occur per resident-year, stratified by LTC home size (Supplemental File 2). This information is integrated within eCLUE as a series of coefficients, which allows us to estimate the total number of specialist visits that typically occur outside of the LTC-home, and through that estimate the number of visits that eConsult could address.
BASE™ utilization data
Service utilization data for all cases submitted through the Champlain BASE™ eConsult Service includes the specialty consulted and specialists’ self-reported billing time for responding to the case. Additionally, providers complete a mandatory five-question close-out survey (Supplemental File 3) with each case. These data provide us with the mean and median cost of an eConsult, and allow us to estimate the number of future eConsult cases that may result in an avoided in-person appointment or that may require follow-up care (i.e. an in-person off-site appointment) (Table 1).
List of the costing constants utilized in sections 1 and 2 of eCLUE.
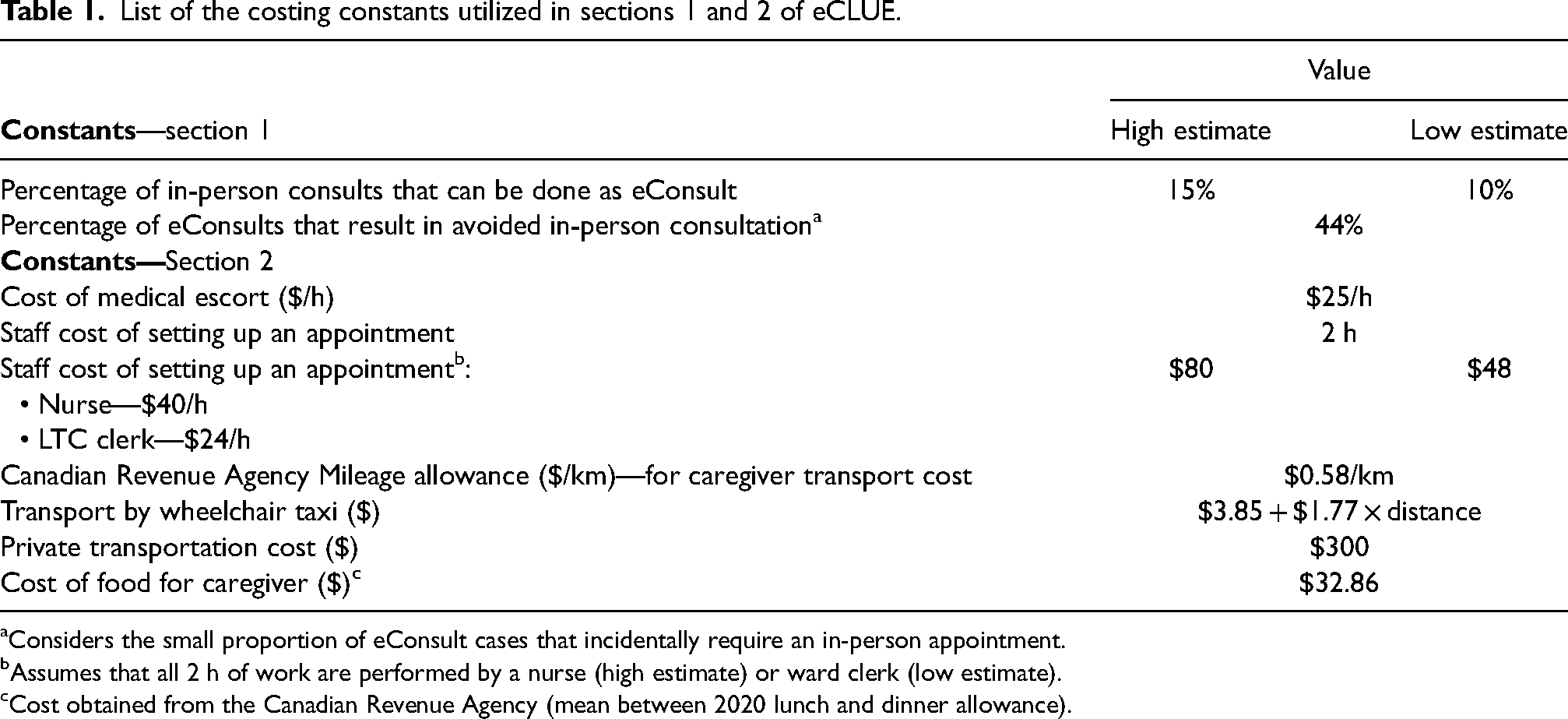
Considers the small proportion of eConsult cases that incidentally require an in-person appointment.
Assumes that all 2 h of work are performed by a nurse (high estimate) or ward clerk (low estimate).
Cost obtained from the Canadian Revenue Agency (mean between 2020 lunch and dinner allowance).
Costing and time savings
The following elements of an off-site specialist appointment were costed in Section 2 of eCLUE: (1) resident transportation by various means (caregiver, taxi, or specialized transportation service), (2) caregiver food, (3) caregiver mileage, (4) medical escort, (5) LTC staff hourly wage (nurse and clerk), and (6) the specialist appointment itself. These elements were divided into three categories: resident/family, LTC home, and Ministry-level, representing the different payers involved in LTC residents’ specialist appointments.
Resident/caregiver time savings are collected directly through eCLUE, as the tool asks users to provide “high” and “low” estimates for typical appointment length including transportation time. LTC staff time savings represent the time necessary for LTC staff to submit a specialist referral and prepare the resident for their appointment.
Taxi fares were obtained online, using the standard fare in Ottawa, Canada. 12 Caregiver mileage and food costs were estimated using standard rates provided by the Canadian Revenue Agency (Table 1). 13 The cost of a medical escort, specialized transportation service, and LTC staff wage/hours were obtained from the technical expertise of an Ottawa-area LTC home medical director. Specialist appointment costs were determined using the Ontario Health Insurance Plan's Schedule of Benefits, which lists the cost of healthcare procedures/appointments in Ontario's public healthcare system as a billable fee code. 14 We used the cost of a “general consultation” by the top 15 specialties accessed by LTC providers through eConsult between January 1, 2017, and September 30, 2019 (Table 2) as the benchmark comparator. These top 15 specialists made up 86% of eConsult cases and represent an expected utilization of eConsult in a pre-pandemic LTC environment. Furthermore, built into the eCLUE tool's design is the ability to modify each of these constants for different circumstances, such as using the tool in a different province or during the COVID-19 pandemic.
Specialties most frequently contacted via eConsult and their fee for typical off-site general consultation.
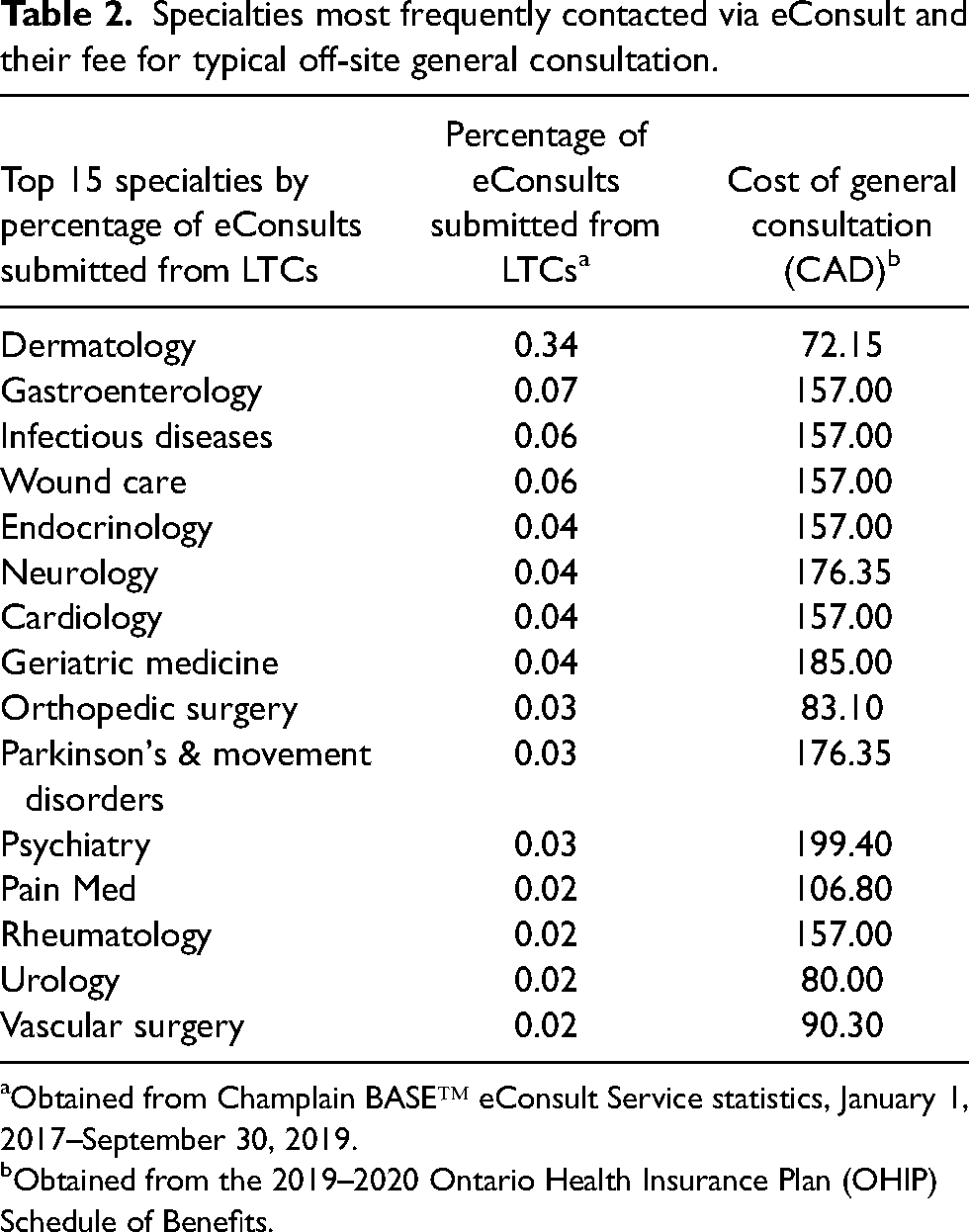
Obtained from Champlain BASE™ eConsult Service statistics, January 1, 2017–September 30, 2019.
Obtained from the 2019–2020 Ontario Health Insurance Plan (OHIP) Schedule of Benefits.
Results
The eCLUE tool
eCLUE is presented as a Microsoft Excel spreadsheet. The first page consists of introductory information followed by the two sections. Each section consists of a table for users to input information specific to their LTC home and its residents, which is then used to generate the relevant outcomes. To the right of each table, users will find instructions for how to populate the tables and explanations for each outcome to facilitate interpretation.
Section 1: eConsult utilization and avoided off-site specialist appointments
Section 1 estimates the number of eConsults that may be sent on behalf of LTC residents over a one-year period (Table 3, Output 1.1) and the number of those eConsults that can result in an avoided off-site appointment (Table 3, Output 1.2). This process begins with two LTC-specific user inputs: (1) the LTC home's bed capacity and (2) its annual occupancy. Once these are provided, eCLUE calculates the LTC's resident population and applies a coefficient derived from Shaver et al. 6 to convert the population to a total number of off-site specialist appointments.
eCLUE formula breakdown by section and output.
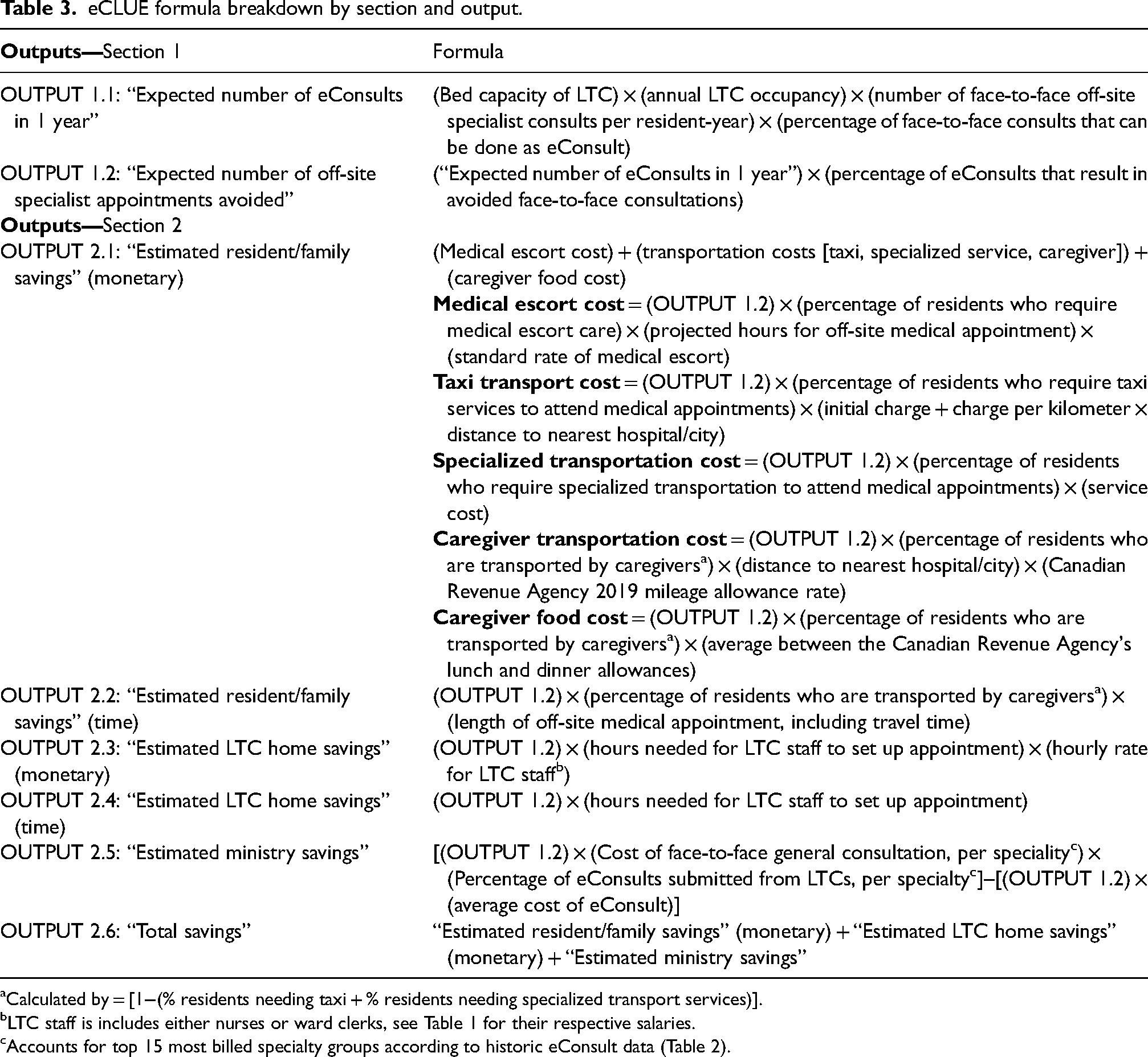
Calculated by = [1−(% residents needing taxi + % residents needing specialized transport services)].
LTC staff is includes either nurses or ward clerks, see Table 1 for their respective salaries.
Accounts for top 15 most billed specialty groups according to historic eConsult data (Table 2).
From there, a second coefficient representing the proportion of appointments that could be completed as eConsults is applied to obtain Outcome 1.1. Based on the experience of eConsult in the primary care setting and existing literature, 15 this was determined to be between 10% and 15% (Table 1). To calculate the estimated number of off-site specialist appointments avoided due to the use of eConsult (Output 1.2), the expected annual eConsult utilization (Output 1.1) is multiplied by a third coefficient representing the percentage of in-person appointments avoided due to the use of eConsult (Table 1). This coefficient was derived from the five-question close-out survey from the Champlain BASE™ eConsult Service (Supplemental File 3).
Section 2: Cost and time savings
Section 2 estimates cost and time savings by taking the estimated number of off-site specialist appointments avoided due to eConsult (Output 1.2) and costing them as though they were actual face-to-face appointments. To do this, it requires user-inputted information about the specific LTC home including the proportions of LTC residents requiring medical escort services and specific transportation services (taxi or specialized services), as well as LTC-to-hospital distance and typical appointment length, with allowance for ‘high’ and ‘low’ estimates. Each input is costed using the same fundamental formula: Output 1.2 multiplied by the user input proportion multiplied by the respective cost or time constant (Table 3, Outputs – Section 2).
Case example
Figure 1 presents a case example of a medical director of a rural LTC home using eCLUE. Their 90-bed LTC home is located 50 km away from the nearest city hospital and operates at max capacity year-round (inputs for Section 1). In terms of its residents, ∼30–40% of them require a medical escort to and from appointments, 10–20% require specialized transportation services (eg. specialized buses or ambulances), 25–35% requiring taxi services, and the remainder are transported and accompanied by their family caregivers for appointments that last between 3 and 5 h (inputs for Section 2). This case is representative, as data from the Ontario Long-Term Care Association's 2019 Long-Term Care Utilization Report identified that 40% of facilities contain fewer than 96 beds, and that 45% of these facilities are located in rural areas. 16 Regarding the transportation and medical escort needs of the residents, this information is highly LTC home-specific, and something LTC medical directors or administrators can reliably estimate for their home based on their knowledge of their residents’ needs and limitations. A user of eCLUE would carefully populate Sections 1 and 2 with these parameters as they pertain to their LTC home and receive an automatic tailored estimation with the “high” and “low” ranges.
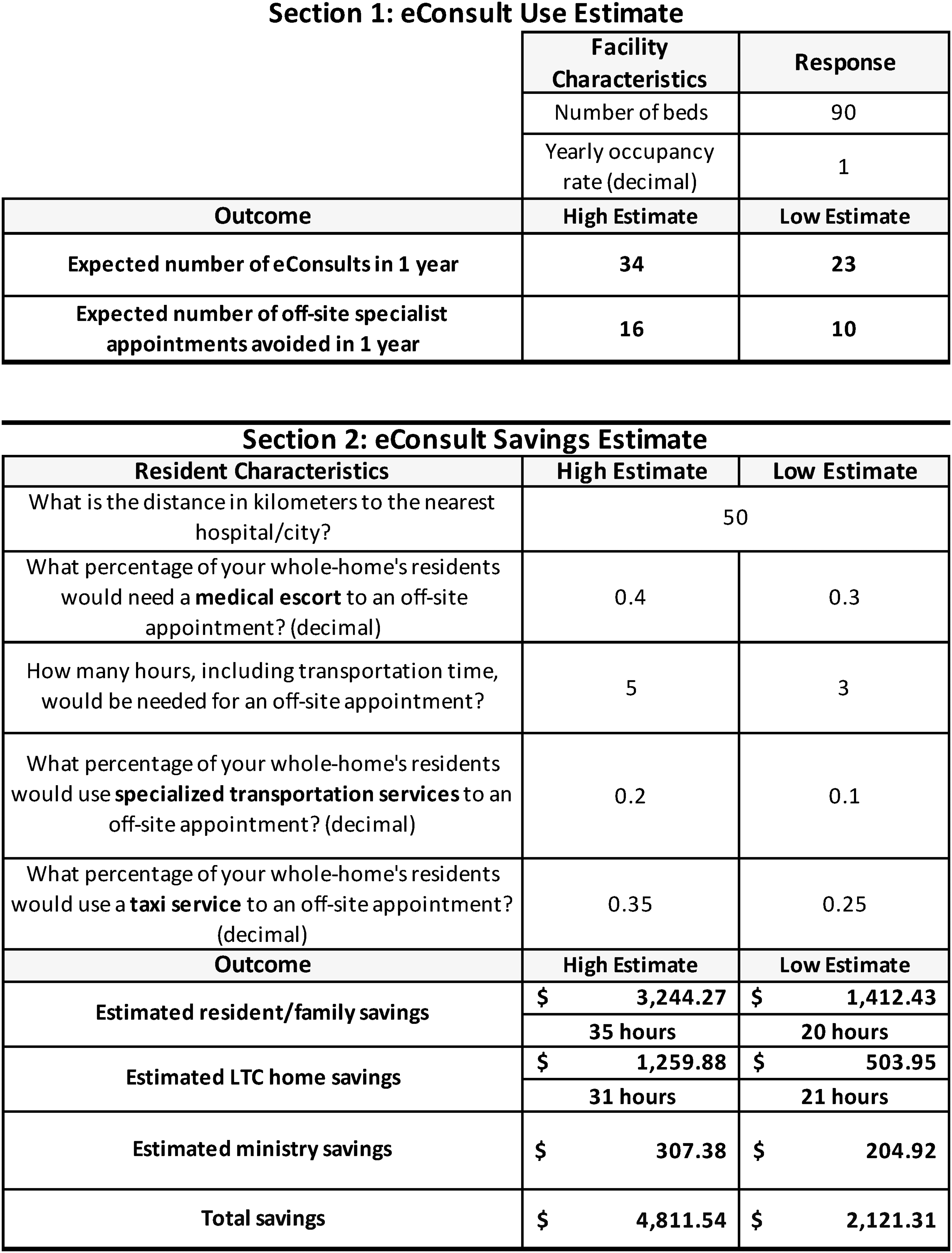
Sample case eCLUE assessment for rural 90-bed LTC home in Ontario with moderate resident transportation requirements, monetary, and time savings displayed for each cost category.
In this particular case, according to eCLUE, this home could expect their PCPs to submit between 23 and 34 eConsults in 1 year, of which 16–25 would result in an avoided face-to-face consultation (Figure 1, Section 1—outcome). This translates to an estimated total cost savings of between $2121.31 and $4811.54, of which 66% to 67% are ascribed to the LTC resident and their family caregivers, 24% to 26% to the LTC home, and 6% to 9% to the ministry. These eConsults would also save between 20 and 35 h of family caregiver time and 21 to 31 h of LTC personnel time over the year (Figure 1, Section 2—outcome).
Discussion
We successfully created a tool that estimates the number of off-site specialist appointments that can be avoided by implementing eConsult in LTC homes and the resultant savings for all stakeholders. eCLUE successfully captures the essential elements needed to convey the benefits of eConsult in an LTC setting. eCLUE's strengths are its ability to provide highly individualized estimates using only six user inputs that capture LTC size, geography, and resident population characteristics. eCLUE is also highly adaptable, with its high-low estimates and fully editable constants, making it well suited for use in different jurisdictions and/or circumstances both provincially and nationally.
Through the hypothetical case example, eCLUE highlights out-of-pocket costs borne by caregivers as one barrier to providing accessible care to LTC residents. This is corroborated by Taylor and Quesnel-Vallee, who identify care coordination, transportation, and out-of-pocket costs as major burdens for many caregivers in the United States and Canada. 17 Our case example also illustrates how eCLUE may also reduce costs borne by LTC homes and the ministry. Although these cost savings are smaller relative to residents/caregivers, it is important to consider the conservative nature of the estimates. Where eCLUE captured a multitude of elements for the resident/caregiver category, the LTC home cost category only quantifies the time and wage savings associated with an avoided appointment (i.e. not having to prepare paperwork or the resident for their appointment). Likewise, the government cost category only compares the physician billings between an eConsult and a general consultation.
The addition of more nuanced parameters to both Sections may serve to provide more robust estimates and are important future directions for eCLUE. For instance, adding a “clinician time savings” component may be very impactful for policy makers and potential clinician users. We know from the literature that LTC eConsult cases take specialist physicians a median of 15 min to complete, 9 compared to the roughly 20 min they spend with their patients during in-person appointments. 18 However, this only represents the clinical aspect of a patient encounter, which accounts for 27% of their total time, whereas administrative tasks (including charting, orders, and reviewing diagnostic tests) make up over 49%. 19 Therefore, since the completion of an eConsult requires little to no administrative work on the part of the specialist, the replacement of some traditional appointments with eConsults could provide specialist physicians with quantifiably more time to take on new patients or care for current ones. Lastly, one limitation at present is that eCLUE uses coefficients derived solely from LTC facility size as its primary means to estimate the number of off-site specialist appointments avoided in Section 1 of the tool. While these coefficients are validated in the literature, 6 future versions of eCLUE can look to integrate additional validated coefficients representing other LTC characteristics, such as LTC ownership status, into its formula for more precise estimates.
Conclusion
We anticipate eCLUE will be a highly impactful tool for caregiver advocates, LTC home administrators, PCPs, and policy makers. It can also be used to support the introduction of policies and strategic approaches to promoting eConsult use in LTC, which will ultimately improve a person-centered approach to accessing timely specialist advice for all residents within their own homes. The next steps for eCLUE are to conduct a validation study in Ontario LTC homes when it is safe to do so. eCLUE's conception and development present a road map for the creation of future tools that aim to evaluate eHealth services, like eConsult, both economically and holistically.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X211074500 - Supplemental material for Development of the electronic consultation long-term care utilization and savings estimator tool to model the potential impact of electronic consultation for residents living in long-term care
Supplemental material, sj-docx-1-jtt-10.1177_1357633X211074500 for Development of the electronic consultation long-term care utilization and savings estimator tool to model the potential impact of electronic consultation for residents living in long-term care by Emiliyan Staykov, Mary Helmer-Smith, Celeste Fung, Peter Tanuseputro, and Clare Liddy in Journal of Telemedicine and Telecare
Footnotes
Acknowledgements
The authors wish to thank Justin Joschko for his assistance in editing the manuscript and preparing it for publication.
Ethics
Our study included data collected automatically from the Champlain BASE™ eConsult Service. Patients and providers did not participate directly in the study, and no identifying information was included in the analysis or publication. Studies involving eConsult data are fall under the approval of the Ottawa Health Science Network REB Protocol 20190385-01H.
Declaration of conflicting interests
Dr Liddy is Co-Executive Director of the Ontario eConsult Centre of Excellence, funded by the Ontario Ministry of Health. She co-founded the Champlain BASE™ (Building Access to Specialists through eConsultation) eConsult service, but she does not retain any proprietary rights. As Long-Term Care Lead of the Ontario eConsult Centre of Excellence, Dr Fung receives salary support from the Ontario Ministry of Health. Dr Fung is the Medical Director of St Patrick's Home of Ottawa, which received financial support to pilot the eConsult service. She did not receive any financial support as an individual for the pilot. The authors have no other conflicts of interest to declare.
Funding
This work is supported in part with funding from the Government of Ontario through the Ontario Centres for Learning, Research and Innovation in Long-Term Care hosted at Bruyère. The views expressed herein do not necessarily reflect the views of the Province. This work was also supported by the Ontario QUILT (QUality for Individuals who require Long-Term support) Network (grant ID no. 255) and Canadian Institutes of Health Research (grant no. 137008).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.