
Abstract
Keywords
Introduction
Indigenous populations, and racial and ethnic minorities worldwide often suffer from a lack of access to culturally safe mental health care. 1 These populations often have less access to mental health services and less availability of these services. 2 Also, previous negative experiences with mental health services can lead to mistrust about these services, contributing to a low engagement. 3 When accessing mental health care, minority groups are commonly met with significant cultural or linguistic barriers. 4 Other barriers include an inadequate recognition or response to their mental needs or insensitivity and discrimination toward them. 5 Moreover, there is a recognized gap in the adoption of a cultural lens from clinical services and mental health care practice.6–8
Still, there are examples of attempts to improve the cultural competence, i.e. efforts that aim to communicate to those being served that their culture is acknowledged and respected. 9 But, beyond cultural competence, 9 services should aim toward cultural safety, as in reflecting on their own biases and structures, and how these could affect service delivery and health outcomes, while focusing on service users’ experiences to define and improve the quality of care. 10 It is cultural safety that enhances provider-user effective communication, hence the therapeutic relationship and potentially, healthcare outcomes, 11 along with the cultural responsiveness of evidence-based mental health treatments. 12 These efforts can reduce health inequities by increasing the appropriateness and effectiveness of clinical interventions.13,14
Telepsychiatry can improve access to quality health care. 15 Enhancing engagement could be improved by pooling resources across multiple locations and enabling access to trained interpreters and healthcare providers who share users’ cultural backgrounds or primary language. 16 Telepsychiatry could provide quality and culturally safe care for Indigenous populations 17 and remote or rural communities. 18 However, it is first essential to understand the elements involved in designing and developing culturally safe telepsychiatry services. There has been no study synthesizing the evidence of initiatives for cultural adaptations, barriers, or opportunities for telepsychiatry services for Indigenous peoples and ethnic minorities. The findings of such a study could assist the development of culturally informed models of care to best achieve equitable access and health outcomes.
Methods
The present scoping review followed the PRISMA extension for scoping reviews (PRISMA-ScR) guidelines 19 to answer the following study questions: (1) What adaptations have been incorporated into telepsychiatry services to improve its cultural safety? And (2) What are the barriers, opportunities, and facilitators for using telepsychiatry to deliver mental health services to Indigenous peoples and ethnic minorities? For this review, we defined telepsychiatry as synchronous video and telephone-based services used for mental health and addiction assessment and care. 20
Search strategy
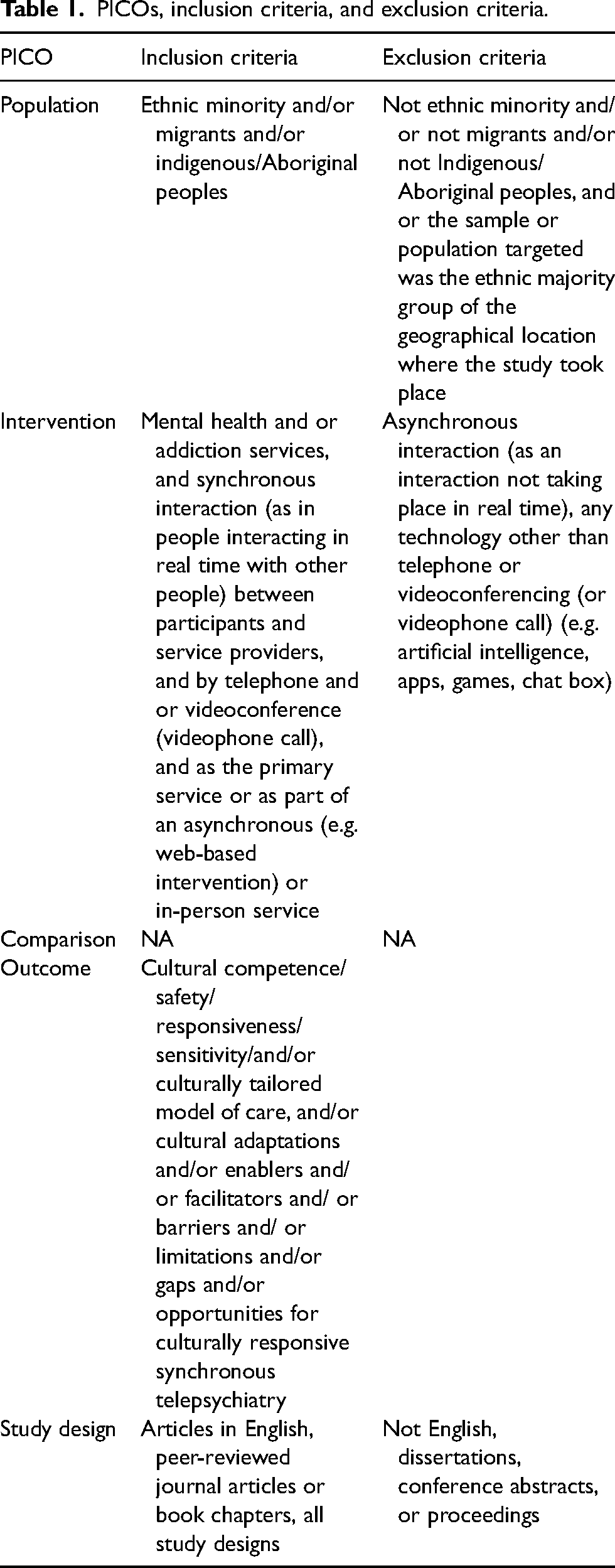
We searched six databases: PubMed, MEDLINE (Ovid), CINAHL(Embase), PsycINFO (Ovid), Web of Science, and Scopus. We divided our search terms according to the PICO framework, i.e. Population, Intervention, Comparison, and Outcomes. The PICO and the eligibility criteria are detailed in Table 1 (see Appendix 1 for detailed search strategy). We performed the search in January 2021 and conducted a reference lists screening to identify additional relevant literature.
PICOs, inclusion criteria, and exclusion criteria.
Study selection
All identified articles were downloaded to the Endnote® X9 database and uploaded to the online systematic literature review manager Covidence®. Two authors (DR, RR) independently conducted an initial title and abstract screening. Full-text records were retrieved for all studies that met the inclusion criteria or when the title and abstract did not provide sufficient information for them to be excluded. Conflicts were solved by consensus with a third author (YC). Two reviewers (DR, RR) independently screened the full texts against the inclusion and exclusion criteria. Disagreements were resolved through discussion with YC.
Data extraction and study quality assessment
DR extracted relevant data from the 58 studies to a Microsoft Excel® table designed by the research team for this review. The following data were extracted: study design, objective, recruitment methods, sample characteristics (e.g. age, gender, and ethnicity), sample size, eligibility criteria, participants’ diagnoses, intervention, and a summary of outcomes related to one or more of the aims of our study. We used the 2018 version of the Mixed Methods Appraisal Tool (MMAT) 21 to assess study quality. Two reviewers (DR, RR) independently performed the quality assessment of the studies. Disagreements were solved by consensus with a third author (GC) (see Appendix 2). No articles were excluded based upon this quality appraisal.
Data synthesis and analysis
We followed Braun and Clarke's (2013) six-step approach for conducting thematic analysis. 22 DR first read and reread the dataset to become familiar with it and then coded the entire dataset. Three reviewers (DR, RR, YC) then revisited the dataset and initial codes to identify potentially missed information. DR searched, identify, defined, and named the themes presented below.
Results
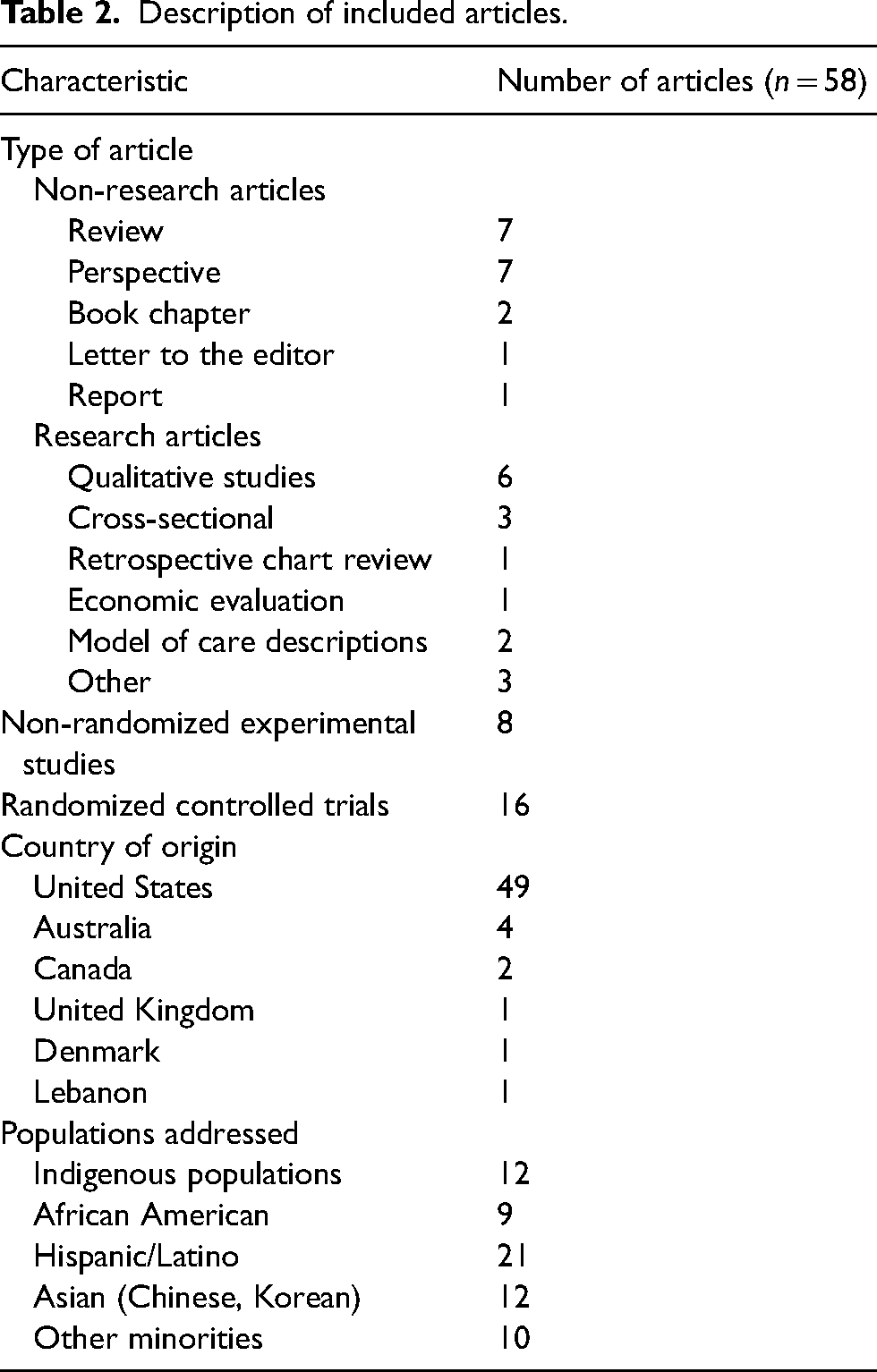
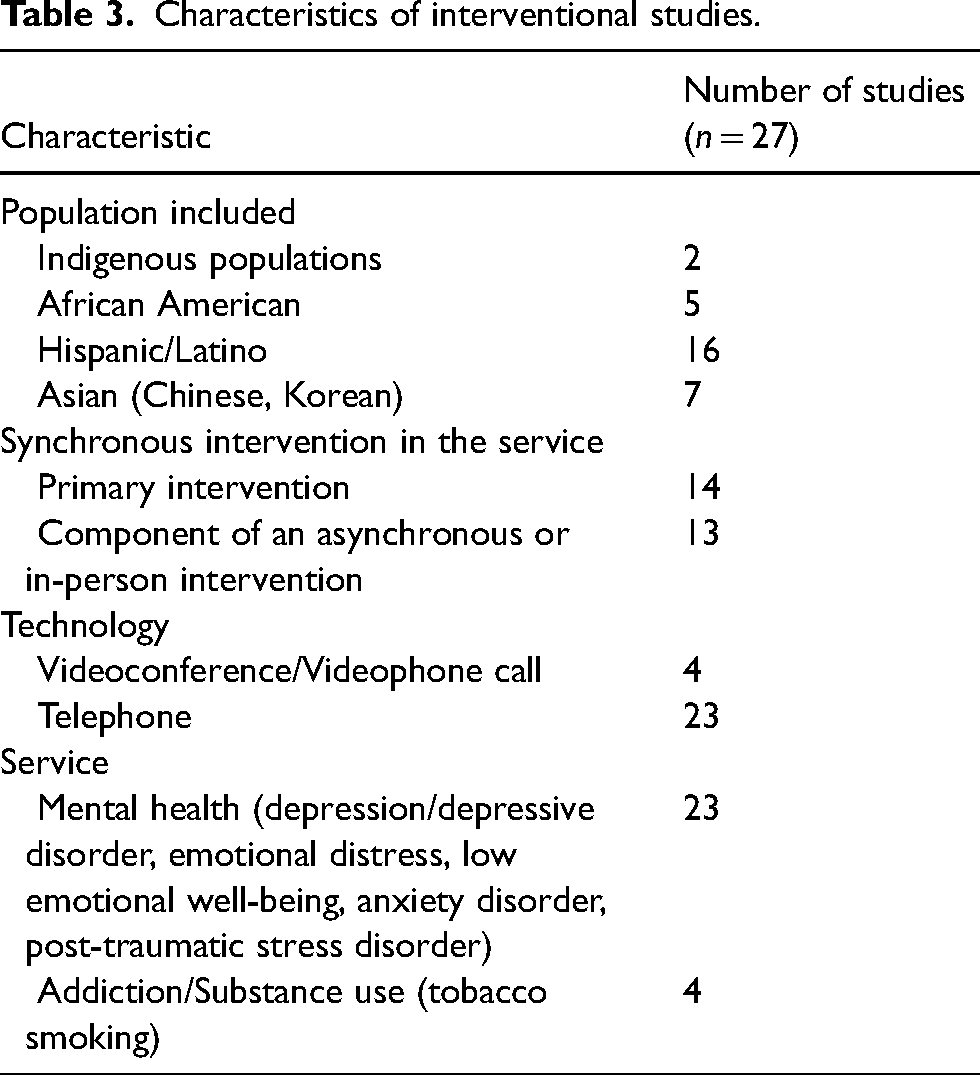
The PRISMA flow diagram in Figure 1 illustrates the study selection process. A total of 1514 citations were first identified. After duplicates were removed, the titles and abstracts of 1016 records were screened, and 886 articles were excluded. After screening the full text of the resulting 130 articles, a total of 52 articles were included for data analysis and synthesis. Six additional articles were identified through reference lists screening. The final total of 58 articles included research and non-research articles. Most articles were conducted in the United States (n = 49; 84%). The ethnic group on which the articles focused were Hispanic/Latino (n = 21), Indigenous populations (n = 12), Asian (Chinese, Korean) (n = 12), African American (n = 9), and other minorities (n = 10). Most articles presented telephone-based interventions (>85%) (see Tables 2 and 3).
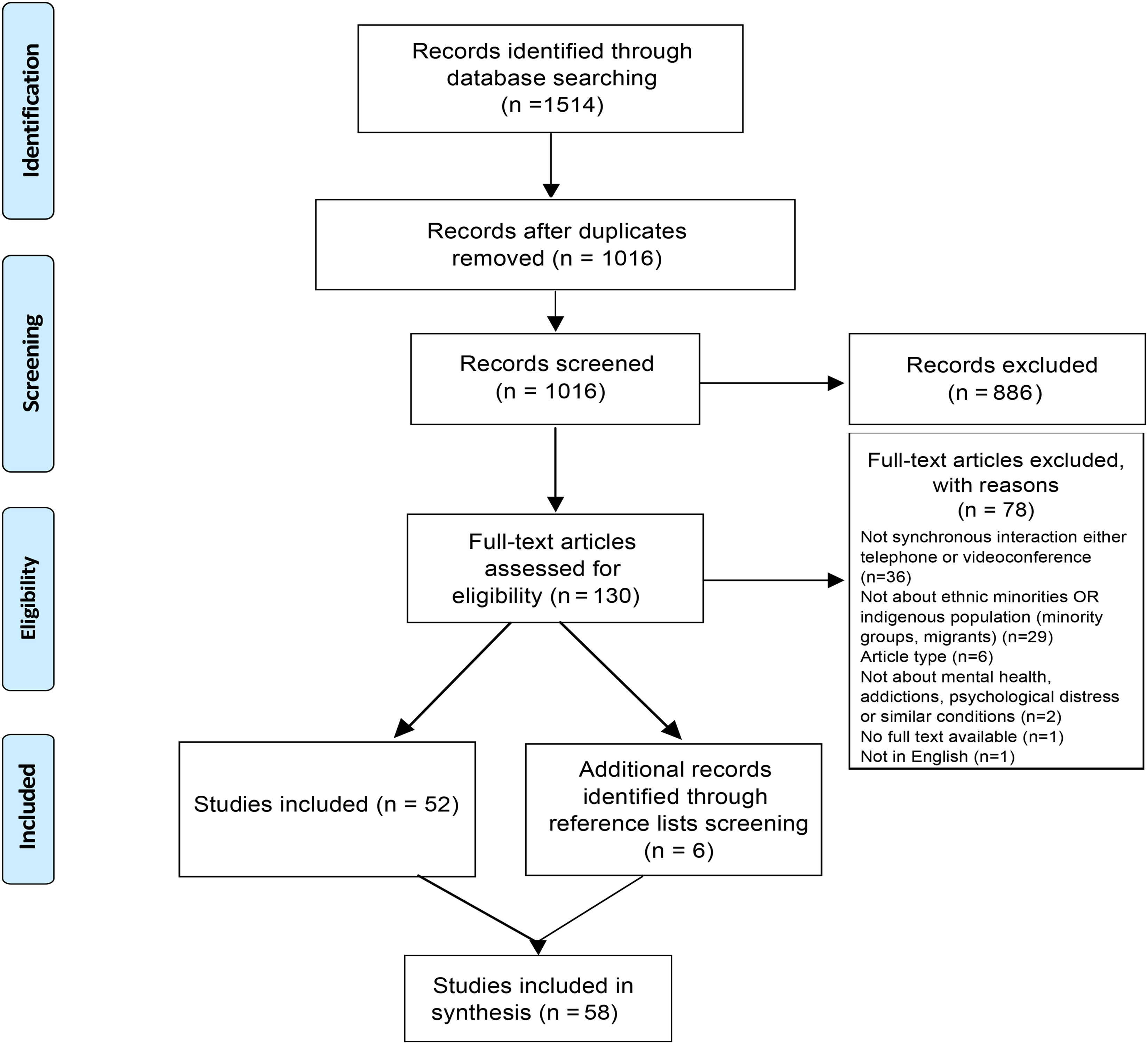
PRISMA diagram.
Description of included articles.
Characteristics of interventional studies.
Themes
Regarding cultural adaptations incorporated into telepsychiatry services to improve its cultural safety for minority populations, we identified two themes in the literature: (i) community involvement and (ii) quality service delivery. Regarding barriers for using telepsychiatry to deliver mental health services to Indigenous peoples and ethnic minorities, we identified two themes: (i) service and infrastructure and (ii) socioeconomic and cultural context. Finally, regarding opportunities and facilitators, we identified two themes: (i) enhanced access and rapport and (ii) multi-organizational collaborations and partnerships (Appendix 3 offers a detailed description of the data informing these themes).
Cultural adaptations
Community involvement
Community involvement was a pivotal step in the cultural adaption of telepsychiatry services. Strategies used included (i) obtaining internal or external input from the targeted community, (ii) becoming familiar with the cultural context, (iii) assessing the community's needs and the resources available, (iv) building local collaboration relationships, and (v) establishing the foundations for future partnerships. Through different strategies,23–27 service providers would consult and involve highly respected and trusted individuals, with valuable cultural knowledge25,28–30 or critical roles within their communities,31–36 and/or organizations within or concerned with the community.31–33,36–39 These individuals or organizations may participate as volunteers or employees working for the service provider or an external entity. Their primary role is to facilitate the process of service delivery, serving as a ‘cultural bridge’ 32 between the provider and the service users and their communities, or to contribute through the delivery of specific components of the intervention.31,32,34,36
Quality service delivery
This theme describes strategies that, tailored to a particular population, facilitate the process of delivery, increase access to the services, and enhance engagement and participation. These strategies included (i) matching provider-user language25,28,34,37,39–50 or ethnicity (race or culture),25,34,39,40,42,43,45,47,50–55 (ii) translating any supporting written and audiovisual material,23,25,28,30,51,53,56 (iii) training providers in cultural safety, as well as selecting culturally knowledgeable and experienced personnel,27,29,31,33,36–38,40,41,43,47,51–54,57–59 and (iv) supervising service delivery, assuring the fidelity of the intervention and assessing that cultural and ethical aspects are respected.27,40,43,54,60 Considering sociocultural factors and cultural and religious values, beliefs, and practices for the design of the services25,28–33,35,39,42,43,45,46,48,51,59,61,62 also plays a fundamental role in a quality service delivery.28,35,44,51,53,60
Barriers
Service and infrastructure
There are some characteristics of the service and aspects related to the infrastructure required for its functioning that can be potential gatekeepers for the successful implementation of telepsychiatry programs delivered to Indigenous peoples and ethnic minorities. For example, service providers and service users not sharing a primary language can be a barrier affecting help-seeking attitudes.23,26,56,57,63 Also, inadequate interpretation services, usually by untrained translators, can cause miscommunications, as well as misinterpretations of culturally informed narratives. 26 Inappropriate physical settings may also adversely affect the service, especially among previously trauma-exposed minority groups. 64 Similarly, the technical unsuitability of used devices 37 and unreliable networks24,31,32,34,43,65,66 can be detrimental to the service. Finally, the high complexity organization and planning required24,31,67 can pose an additional challenge, especially when the cooperation of entities that are external to the provider is crucial, for example, in remote areas.
Socioeconomic and cultural contexts
The reviewed literature also identified barriers related to service users’ socioeconomic and cultural contexts. These included low health literacy,23,41 limited awareness of the availability of services, 63 work and family responsibilities, and financial constraints.25,26,34,43,45,64,68 Also, provider service user cultural gaps and values differences, 69 and cultural and religious practices and beliefs,36,41,57,63 such as gender issues, or the view that specific topics should not be discussed unless discussed with a religious leader, were also reported as potential barriers. Personal reservations or concerns—mainly distrust toward the government's or unknown organizations—31,32,34,36,37,41,44,57,61,63,64,66–71 in some cases influenced by previous experiences or historical backgrounds of abuse and discrimination, 31 were also reported as barriers. Finally, the reviewed literature also identified users’ degree of exposure to and comfort with technology as a potential barrier.17,23,26,32,34,43,45,49,66,70
Opportunities and facilitators
Enhanced access and rapport
Telepsychiatry was identified as a tool that can enhance access and delivery of mental health services to Indigenous populations and ethnic minorities. It can help reduce consultation costs, waiting times, and the need to travel long distances while allowing flexible scheduling of sessions.23,25,29–31,37,40,45,56,60,64,68,72,73 It was also described as cost-effective, safe, confidential, and showing comparable satisfaction levels to in-person services of both providers and service users.17,23,28,30,37,39–44,49,57,60,64,67,68,73–75 The reviewed literature also described several strategies to promote engagement and rapport building.26,28,31,32,37,42,54,57,69,74
Ongoing technological advances, including the simplicity, availability, and reliability of software, hardware, and networks, also represent opportunities and facilitators for telepsychiatry.25,26,31,36,37,56,61,73,76 Other enablers include accessibility to service navigators, and users’ more extensive exposure to and training in technology.31,37,44,50,76–78
A culturally competent workforce is essential for providing culturally safe telepsychiatry, and telepsychiatry also offers the possibility to enhance capacity building of health professionals, particularly in remote areas. 67 There are several initiatives for capacity building mentioned in the literature. These include recruiting a more diverse population into healthcare professions to better reflect our communities, 26 involving cultural safety and telepsychiatry-experienced faculty members in training programs,62,65 liaising healthcare providers with the community,31,32,65 employing and training nonmedical workforce, 73 and promoting peer consultation from those knowledgeable and experienced in providing care to specific underserved populations.32,36,69
Multi-organizational collaborations and partnerships
Multi-organizational collaborations were reported as crucial for the success of telepsychiatry services delivering mental health services to Indigenous peoples and ethnic minorities. 33 Partnerships between different organizations, including local organizations in remote communities, 38 and between organizations and the community allow to co-design and assess the service's potential impact, suitably, and appropriateness. 24 The structuring and organization of these partnerships must be configured through an ‘agreement of understanding’ 38 that details clear communication channels, protocols, and roles and responsibilities of each party.31,32,38 A local facilitator—who acts as a mediator between the local organization and the external organization that provides telepsychiatry service—and efficient care coordination between medical systems (e.g. through electronic medical records) 33 can assist with the process.
Discussion
This systematic scoping review and thematic analysis of the literature is the first attempt to collate the evidence regarding cultural adaptations, barriers, and opportunities and facilitators for synchronous telepsychiatry services for Indigenous populations and ethnic minorities. The findings emphasize how ensuring community involvement and a quality service delivery are crucial in all cultural adaptations. The study also identified potential barriers, opportunities, and facilitators. Potential barriers identified in the reviewed literature were related, on the one hand, to the service and its required infrastructure, and on the other hand, to service users’ socioeconomic and cultural contexts. Finally, themes describing both opportunities provided by and facilitators of a telepsychiatry service were enhanced access and rapport and multi-organizational collaborations and partnerships.
The components and strategies used for cultural adaptations identified in the reviewed literature are consistent with existing models for cultural adaptations of behavioral health interventions79–82 and with the model proposed by Shore & Manson (2005). 24 All these models share three stages in the adaptation or design process of a telepsychiatry service for ethnic minorities. The first stage is pre-intervention, which involves identifying needs and preliminary adaptations through direct consultation and involvement of community members and organizations. The second stage, pilot testing, involves multisource feedback gathering after pilot implementations to guide further adaptations. The final stage is the clinical trial, where it is essential to consider the adaptation as an iterative process. However, there is still a need for an up-to-date evidence-based guideline for adapting or telepsychiatry services for Indigenous populations and ethnic minorities.
It is relevant to mention that the identified barriers or challenges were closely related to the identified opportunities and facilitators. For instance, services users’ work responsibilities or the high complexity organization and planning required for the service may represent barriers; yet, flexible scheduling, and careful planning in collaboration with local organizations are both opportunities provided by the service and facilitators for the development of a quality service and its success. This also highlights the importance of certain steps during the cultural adaptation or development of the telepsychiatry service, for example, the key role of developing a partnership with local primary healthcare or community-based services. 37 In addition, the reviewed literature indicates that these partnerships facilitate adopting holistic models of care, connecting service users to a diverse network of local healthcare, psychological, social, and spiritual support.
This review offers an overview of the available evidence related to cultural adaptations, barriers, opportunities, and facilitators for telepsychiatry for Indigenous peoples, and ethnic and racial minorities. Although quality assessment is not a requirement for scoping reviews, one was performed individually for each included study (Appendix 2). Regarding the level of evidence of the reviewed literature, about 80% of the included articles were randomized controlled trials, single descriptive or qualitative studies, and expert opinions (about one-quarter of the total each). In addition, close to two-thirds of the included articles met from 80% to 100% of the quality criteria of the MMAT. Still, there are limitations to this review. Even though only one report was excluded based on language, the inclusion criteria were set for peer-reviewed articles and book chapters published in English. The included literature represented a diverse population with an equally diverse experience of healthcare services, albeit one sharing the experience of being minoritized. Nevertheless, future research should pay further attention to this diversity. Finally, over 85% of the included publications reported telephone-based interventions, pointing to the need for further research on videoconferencing or the reduced number of these services developed with a cultural safety lens.
In conclusion, the reviewed literature highlights the pivotal role of community involvement and multi-organizational collaborations and partnerships when adapting or developing a telepsychiatry service for Indigenous populations and racial and ethnic minorities. Partnerships, collaboration, and cultural connectedness are key domains to culturally safe practice in telepsychiatry. Plus, when developing these services, addressing potential barriers through these partnerships can increase the opportunities provided by the service and simultaneously facilitate the success of the service. Culturally safe telepsychiatry programs must be specifically designed for the populations they seek to serve, and this review could strategically inform further developments and research in successful telepsychiatry implementation to maximize health outcomes.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X211069664 - Supplemental material for Adaptation models, barriers, and facilitators for cultural safety in telepsychiatry: A systematic scoping review
Supplemental material, sj-docx-1-jtt-10.1177_1357633X211069664 for Adaptation models, barriers, and facilitators for cultural safety in telepsychiatry: A systematic scoping review by Daniela Ruiz-Cosignani, Yan Chen, Gary Cheung, Mark Lawrence, Mataroria P Lyndon, Etuini Ma’u and Rodrigo Ramalho in Journal of Telemedicine and Telecare
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The present study was funded by the 2020 Health Delivery Research Activation Grant of the Health Research Council of New Zealand, as part of the project: e-Mental Health in Aotearoa: sector engagement and research agenda priorities.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Research Council of New Zealand
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.