
Abstract
We describe a case of a term female infant born in a rural community hospital and who developed a left-sided spontaneous tension pneumothorax shortly after birth. We used telemedicine to guide the family physician and healthcare team at the referring hospital to perform a life-saving thoracentesis using an intravenous cannula. The cannula was kept in place to drain the persistent pneumothorax during transportation to the pediatric intensive care unit at the tertiary hospital.
Introduction
Historically, perinatal spontaneous pneumothorax occurred in 0.5%–2% of all live births.1,2 The current prevalence is unknown due to lack of surveillance and that the majority of cases are asymptomatic or associated with mild symptoms that resolve with supportive care. 3 In a study including 76 infants with perinatal spontaneous pneumothorax, 29% underwent thoracentesis, chest tube insertion, or both. 3 Tension pneumothorax leading to mediastinal shift and hemodynamic instability occurred in 2.5% of term neonates with symptomatic spontaneous pneumothorax in one study. 4 Tension pneumothorax requires immediate intervention with thoracentesis and/or thoracostomy. Trained providers familiar with such procedures are not always available in rural centers. Telemedicine has been described as a useful tool to improve the quality of neonatal resuscitation in resource-limited settings and reduced unnecessary neonatal transports to higher levels of care.5,6 Some reports cited using telemedicine to guide thoracentesis in resource-limited settings without providing details on how to guide such procedure through telemedicine.7,8 In this report, we describe a term neonate presenting with persistent tension pneumothorax in a rural community hospital that was managed using telemedicine.
Case report
A female infant was born at 414/7 weeks’ gestation in a community hospital in a small town 100 km away from the Foothills Medical Centre, which is the tertiary perinatal center in the southern part of Alberta. The mother was a 26-year-old primigravida, with uncomplicated pregnancy apart from urinary tract infection treated with oral antibiotics. Group B streptococcus screening was negative. An ultrasound scan at 21 weeks gestation was normal. Spontaneous vaginal delivery ensued after 3 h of rupture of membranes resulting in an appropriate-for-gestational-age female infant. She received 60 s of delayed cord clamping, did not require resuscitation, and was placed skin-to-skin with mother. Apgar scores were 8 and 9 at 1 and 5 min, respectively, and cord pH was 7.27. At 15 min of age, she was noticed to have grunting and respiratory distress. She was placed on a radiant warmer and examination revealed decreased breath sounds throughout the left lung fields. She was managed with continuous positive airway pressure (CPAP) at 5 cmH2O and fraction of inspired oxygen (FiO2) of 1.0 with oxygen saturation of 60%–70% by pulse oximetry. Initial chest X-ray (Figure 1) revealed left-sided tension pneumothorax with mediastinal shift to the right. The treating general practitioner immediately consulted Southern Alberta Neonatal Transport Team by phone and a transport team composed of a specialized transport nurse and a respiratory therapist was deployed by helicopter. Meanwhile, the transport physicians at Foothills Medical Centre initiated telemedicine and provided guidance to the general practitioner for infant management. CPAP was discontinued and the patient was placed on nasal cannula with 100% oxygen at 2 liters per minute; however, the patient developed desaturation; therefore, CPAP was resumed. The general practitioner inserted a peripheral intravenous access to provide maintenance fluids and emergency medications, if needed. The general practitioner had never performed thoracentesis in a newborn previously. The transport physicians instructed the team in the rural hospital to prepare equipment for thoracentesis including a 20G intravenous catheter, connection tube, 3-way stopcock Luer lock, 20 ml syringe, sterile huck towels, and chlorhexidine sterile swabs. The transport physicians guided the general practitioner and the assisting nurse to insert the intravenous catheter through the third–fourth left intercostal space at the anterior axillary line while directing the tip cephalad and anteriorly. One hundred milliliters of air were drained with immediate improvement of the oxygen saturation and ability to wean FiO2. The catheter was maintained in place to assess for reaccumulation of the pneumothorax. After a few minutes, the assisting nurse was able to aspirate again. At this point, the decision was to keep the catheter in place and to continue draining the air every few minutes; 735 ml of air were drained prior to the transport team arrival. The transport team arrived at the rural hospital 62 min after the initial call. They intubated the patient using a 3.5 mm endotracheal tube after administration of atropine, fentanyl, and succinylcholine, and connected her to mechanical ventilation. Blood culture was drawn, and empiric ampicillin and gentamicin were initiated. White cell count was 20 × 109/l, neutrophils 15.7 × 109/l with no band cells. Arterial blood gas 48 min after intubation showed pH 7.32, PaCO2 46, PaO2 331, HCO3 24, and base excess −2. The transport team maintained the intravenous catheter in the pleural space as it continued to drain air. Fentanyl infusion was initiated for analgesia and sedation, and the patient was transported by ground ambulance to avoid the risk of worsening pneumothorax with air transport. The transport team evacuated 2165 ml of air during the trip. The patient was admitted to the pediatric intensive care unit (PICU) at Alberta Children's Hospital, as there was no bed available in the neonatal intensive care unit (NICU). Vital signs were stable on admission; heart rate 125 beats per minute, blood pressure 65/38 mmHg, SpO2 95%, end-tidal carbon dioxide of 47 mmHg on volume-targeted ventilation settings of tidal volume 4 ml/kg, positive end-expiratory pressure 5 cmH2O, rate 30 breath per minute, and FiO2 0.25. Upon arrival to PICU, a left chest tube was inserted. She was extubated 20 h later and remained stable. The chest tube was removed on day two of life. However, the pneumothorax reaccumulated within 6 h. The patient was re-intubated and another chest tube was inserted. A chest computed tomography scan to rule out underlying structural abnormalities was normal. She was extubated on day three of life and transferred to the pediatric ward the next day. The second chest tube was removed on day six of life, and she was discharged home on day seven of life in good condition with no respiratory support.
First chest X-ray showing left tension pneumothorax.
Southern Alberta Virtual NICU program connects the neonatal transport team at Foothills Medical Centre with 15 rural centers in the southern part of the province. It uses a high-speed fiber optic internet protocol network capable of facilitating video conferencing at a bandwidth of 768–1024 kbps. Telemedicine carts at the rural sites are equipped with high definition (1080p), pan tilt zoom cameras with a range of motion of ±100°, tilt of +20°/−30°, 10× optical zoom and 12× digital zoom at 60 frames per second. Those cameras can be remotely controlled by the transport team at Foothills Medical Centre.
Discussion
In this report, we describe the use of telemedicine to guide the management of a life-threatening perinatal spontaneous persistent tension pneumothorax in a term infant in a rural community hospital. Thoracentesis is considered the optimal procedure in case of tension pneumothorax. In a randomized controlled trial comparing thoracentesis and chest tube insertion as primary management of symptomatic pneumothorax in neonate, thoracentesis resulted in reduced use of chest tube. 9 Two reports cited the use of telemedicine to guide needle thoracentesis in rural or community hospitals; however, they did not describe the procedure details or the severity of the pneumothoraces.7,8 In addition, telemedicine has been used to facilitate outreach education and simulation to teach and maintain competency of neonatal procedures among healthcare teams in resource-limited areas. 10
Our report provides a detailed description for neonatal telemedicine practitioners on “How to” guide a high risk but life-saving procedure such as thoracentesis using telemedicine technology. Providing guidance through telemedicine differs from providing direct guidance as the consultant is frequently unfamiliar with the logistics in the referring center and does not have the ability to view the patient and the procedure from all angles in telemedicine (two-dimensional view) compared with direct observation (three-dimensional view). We would like to highlight some practical points that we found useful for healthcare practitioners providing guidance to others through telemedicine to perform any procedure in general and, specifically, for thoracentesis. We identified four suggested recommendations that apply to any telemedicine-guided procedure. First, visualize and review all required equipment with the team in the referring center to ensure shared understanding of name and size of all pieces of equipment. Second, ensure the referring team is able to assemble the equipment correctly. For instance, in our case, the position and the direction of closure of the 3-way stopcock Luer lock while aspirating and evacuating the pneumothorax. Third, ensure the healthcare providers performing the procedure are able to correctly identify the anatomical landmarks and walk them through the procedure prior to performing it. Fourth, ensure you have an adequate view of the patient with proper positioning of the camera and healthcare providers performing the procedure. It is ideal if the consultant is able to remotely control the camera in the referring center.
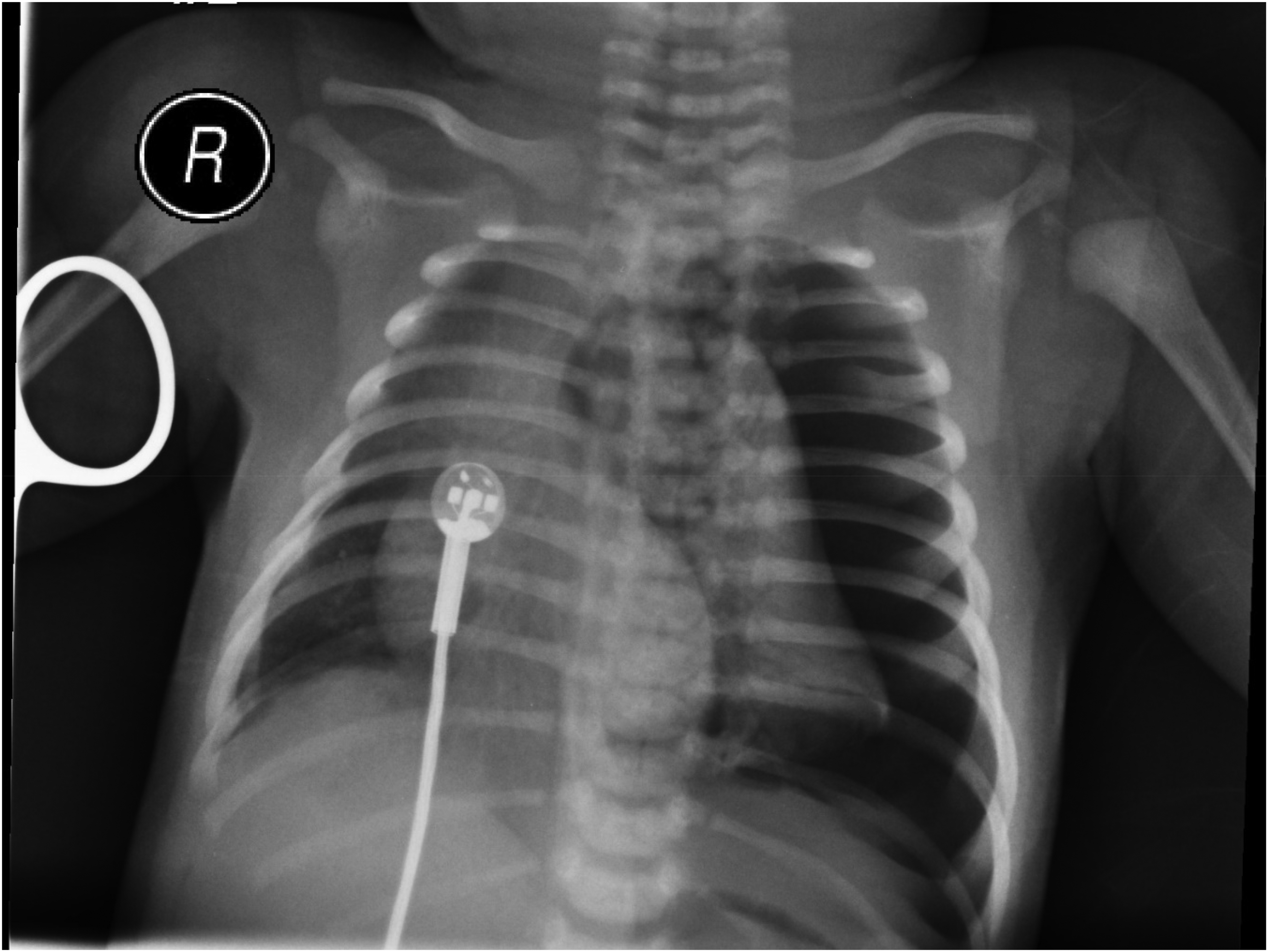
We also identified two suggested recommendations specific to telemedicine-guided thoracentesis. First, we suggest using an intravascular cannula rather than a butterfly needle. Although the use of an intravascular cannula or a butterfly needle did not result in a difference in subsequent need for chest tube insertion in a randomized clinical trial, 9 the use of an intravascular cannula carries some advantages, especially in resource-limited settings. Butterfly needle thoracentesis requires simultaneous withdrawal of the needle while aspirating the pneumothorax air. Delayed needle withdrawal may result in further injury when the lung expands and hits the butterfly needle. This risk is less with the softer material of intravascular cannula. In addition, the intravascular cannula could be kept in place after air evacuation with the stopcock closed toward the patient allowing reassessment for reaccumulation of pneumothorax over time. The other suggested recommendation is to insert the cannula in the third to fourth intercostal space at the anterior axillary line while directed cephalad and anteriorly (Figure 2). If the cannula is inserted in the second intercostal space perpendicular to the chest wall, it might bend once the lung expands preventing further use in case of reaccumulation.

Chest X-ray with the cannula in the left third intercostal space.
Conclusion
Telemedicine is useful to guide healthcare providers performing unfamiliar urgent life-saving procedures. It is important for neonatologists and healthcare providers to consider a checklist to support telemedicine-guided procedures in resource-limited settings.
Footnotes
Authors contributions
AAM, AB, EG, and TS conceptualized and drafted the initial manuscript and reviewed and revised the final manuscript. JH, SD, and CA abstracted the data and timelines of the case, critically reviewed and edited the initial manuscript, and revised the final manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.