
Abstract
Introduction
Telemedicine can alleviate the problems faced in rural settings in providing access to specialist stroke care. The evidence of the cost-effectiveness of this model of care outside high-income countries is limited. This study aimed to conduct: (a) a systematic review of economic evaluations of telestroke and (b) a cost–utility analysis of telestroke, using China as a case study.
Methods
We systematically searched Embase, Medline Complete and Cochrane databases. Inclusion criteria: full economic evaluations of telemedicine/telestroke networks examining the use of thrombolysis in patients with acute ischaemic stroke, published in English. A cost–utility analysis was undertaken using a Markov model incorporating a decision tree to simulate the delivery of telestroke for acute ischaemic stroke in rural China, compared to no telestroke from a societal and healthcare perspective. One-way deterministic sensitivity analyses and probabilistic sensitivity analyses were performed to test the robustness of results.
Results
Of 559 publications found, eight met the eligibility criteria and were included in the systematic review (two cost-effectiveness analyses and six cost–utility analyses, all performed in high-income countries). Telestroke was a cost-saving/cost-effective intervention in five out of the eight studies. In our modelled analysis for rural China, telestroke was the dominant strategy, with estimated cost savings of Chinese yuan 4,328 (US$627) and additional 0.0925 quality-adjusted life years per patient. Sensitivity analyses confirmed the base case results.
Discussion
Consistent with published economic evaluations of telestroke in other jurisdictions, telestroke represents a cost-effective solution to enhance stroke care in rural China.
Introduction
Clinical advances over the past few decades have transformed the management of stroke care. The use of intravenous thrombolysis is now a standard treatment for acute ischaemic stroke (AIS) that has enabled survivors to achieve improved health outcomes, but is generally limited for administration within 4.5 h of symptom onset. 1 Meeting such strict onset to needle times remains a challenge, particularly in rural areas where patients are often disadvantaged with regard to stroke care, due to limited access to specialists, poorer infrastructure and delays in hospitalisation given the greater distances travelled.2–4
Telemedicine for stroke (telestroke) allows staff at local hospitals to share information (e.g. patient data and brain imaging) in real time and communicate with stroke specialists based elsewhere, via two-way audio-visual technology. Telestroke networks can enhance and expedite diagnosis and treatment planning, increase the likelihood of thrombolysis and endovascular clot retrieval, and promote better prognoses in patients.5,6 Each minute potentially saved in time to treatment translates to approximately an average of 1.8 days of healthy life gained. 7
To determine whether telestroke is a sustainable solution and represents ‘value for money’, it is imperative to assess its cost-effectiveness. The objective of this study was: (a) to conduct a systematic review of economic evaluations of telestroke to assess the availability of current economic evidence for telestroke; and following on from the conclusion that cost-effectiveness has only been investigated in high-income countries, (b) to conduct a cost–utility analysis of telestroke compared to no telestroke in rural China, as a case study for a middle-income country, using relevant input estimates from the published literature.
Methods
Systematic review
Literature search
On 4 November 2020, an electronic literature search was conducted of Embase, Medline Complete and Cochrane databases using the following key terms (and associated variations): stroke, telemedicine and economic evaluation. Full search terms are included in Supplementary Table 1 of the online supplementary material. Results were screened by two reviewers (ET and HT). All identified economic evaluations (cost-effectiveness and cost–utility analyses) of telemedicine/telestroke networks that examined the use of thrombolysis in patients with AIS were included, provided they were reported in English. Cost-effectiveness and cost–utility analyses are types of full economic evaluations comparing the associated costs and consequences of alternative courses of action, but differ by the measure of effects – the former measure outcomes by natural units whereas the latter measure outcomes in terms of quantity and quality of life (utilities). 8 Key exclusion criteria included studies of mobile stroke units, rehabilitation, secondary prevention and return on investment.
Probabilities and cost inputs for the model.

The range used for sensitivity analyses.
Source: Whetten et al., 19 Demaerschalk et al., 20 Ickenstein et al., 24 Nelson et al., 25 Liao et al., 26 Pan et al., 27 Lees et al., 28 Yu et al., 29 Pan et al., 30 Global Times 31 Independent Hospital Pricing Authority 32 Hu et al., 33 The AVERT Trial Collaboration Group 34 Kohli et al., 35 Wang et al. 36
tPA: tissue plasminogen activator; w/: with; w/o: without; UC: usual care (without tPA); OTT: onset to treatment; mRS: modified Rankin Scale;
CNY: Chinese yuan renminbi.
Assessment of included studies
Key characteristics (country, target population, type of evaluation, perspective, costings and results) were extracted from the individual studies and documented in a table. The quality of included studies was assessed using two health economic tools – (i) the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) 9 which guides the reporting of economic evaluations (where quality was assessed based on % of the relevant criteria met), and (ii) the Quality of Health Economic Studies (QHES) checklist, 10 which evaluates the methodological quality of studies to produce a numerical score rating between 0 and 100 (where a higher score indicates higher quality).
Modelled cost–utility analysis
The systematic review provided an overview of existing research, and showed that whilst ∼70% of strokes occur in low-income and middle-income countries (LMICs), 11 economic evaluations of telestroke have only been performed for high-income countries. Given the disparities faced by LMICs (in which patients more frequently suffer severe stroke, have poorer access to services and receive less investigations and treatment compared to high-income countries), 12 and the differences in resource settings between high income and LMICs, investigating the cost-effectiveness of telestroke in the context of a LMIC may be of value. Thus, a modelled cost–utility analysis for telestroke was performed, using China as a case study for a middle-income country. China, an upper-middle income country, 13 bears the largest stroke burden in the world, accounting for nearly one-third of stroke deaths worldwide, 14 and ∼2.4 million new strokes each year. 15 Observed thrombolysis rates in China are also low – with an estimated 1.6% of AIS patients treated with thrombolysis, 16 making China an ideal case study for the assessment of the economic credentials of telestroke.
Model structure
A Markov microsimulation model preceded by a decision tree was developed to estimate the cost–utility of treating AIS patients with a telestroke network compared to no telestroke network for the rural population of a given province in mainland China (Figure 1). Microsimulation allowed for the simulation of a heterogeneous population and stored the event history (i.e. number of recurrent strokes) of each simulated patient. The telestroke network modelled was based on a hub and spoke design, in which local hospitals (spoke sites) were connected to an anchor establishment such as a stroke centre (hub).17,18 Patients receive stroke care at the spoke hospital but may be transferred to the hub for treatment in circumstances where a higher level of care is required.17,18 The model began with AIS patients presenting to a spoke hospital (with telestroke vs. without telestroke) within 4.5 h of symptom onset. Patients may receive either thrombolysis or usual care without thrombolysis (the likelihood of transfers was also considered at this point). Depending on the treatment received and onset to treatment (OTT) time, patients may transit to one of the different health states based on the transition probabilities. The model allowed for all possible health states associated with stroke to be captured. The seven health states were defined by the modified Rankin Scale (mRS), scored between 0 (no symptoms) and 6 (death). Patients may then experience recurrent stroke(s), die from background mortality or have no event. The model was built in TreeAge Pro 2019, R2 (Treeage Software Inc., Williamston, MA, USA).
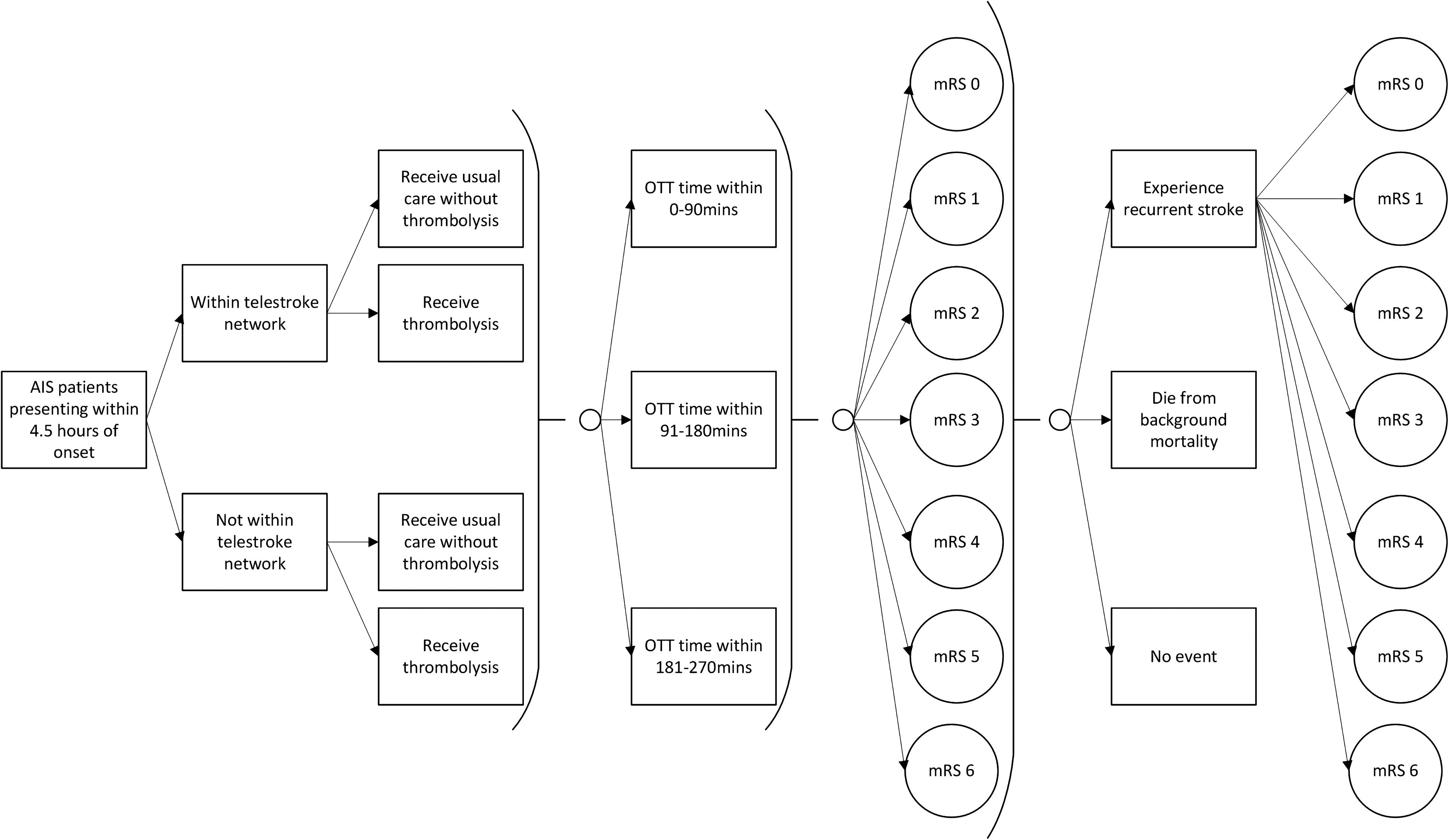
Model structure. Note that the patient's mRS cannot improve.
Several assumptions were applied in the modelling. It was assumed that the accuracy of diagnoses was the same between telestroke and face-to-face consultations, 19 and that patients received similar care post-hospitalisation. 20 Following their stroke, patients may remain in the current health state or transition to a more severe state as defined by their mRS score. Lastly, the probability of recurrent stroke was independent of initial treatment and severity of stroke.
This study took both a societal and healthcare system perspective and adopted a time horizon of 30 years to account for lifetime costs and health outcomes. Costs and effectiveness beyond the first year were discounted at a 3% standard rate to reflect the preference for the present. 21
Population
Rural patients with AIS presenting at emergency within 4.5 h of symptom onset in a province in China were simulated. Characteristics of the hypothetical cohort were derived from a nationwide population-based survey of more than 480,000 adults in China. 15 Patient mean age was 66 years, 55% were male and 70% of all strokes were AIS. 15 The population size was calculated considering a rural population of 15.46 million in the province (the median rural population across the 31 provinces in mainland China), 22 a rural incidence rate of 298 cases per 100,000 persons, 15 the proportion of AIS cases, and the fact that only 31% of patients were estimated to arrive at hospital within 4.5 h of symptom onset. 23 The number of patients with AIS presenting at emergency within 4.5 h of stroke onset for a province was calculated to be 9940 patients per year.
Model inputs
Drawing on the included economic evaluations in the systematic review, key transition probability variables were analysed to determine their suitability for use in the newly developed model. Additionally, a rapid literature search was conducted in Embase and Google Scholar to identify studies to complement the data extracted from the included evaluations. Primary model inputs are presented in Table 1.
Transition probabilities: The probabilities of receiving thrombolysis with and without a telestroke network were calculated using the weighted mean effect size (random effects) of previous studies/models.19,20,24,25 The distributions of OTT time were based on data from the Thrombolysis Implementation and Monitor of Acute Ischaemic Stroke in China (TIMS-China), a nationwide registry with 1440 records of consecutive patients treated with thrombolysis.26,27 The probability of mRS outcomes via treatment and OTT time, and inter-hospital transfers with or without telestroke, were sourced from published literature.19,28 Background mortality rate was assumed as equivalent to the World Health Organization's age-dependent death rate for China. 37 The rate of recurrent stroke (6.49% during the first year and an annual rate of 2.01% thereafter) was based on a meta-analysis by Mohan et al.38,39 Additionally, the model adjusted for the increased likelihood of recurrent strokes due to existing history of stroke by applying a risk ratio of 1.39 and accounting for the multiplicative nature with each previous event. 40
Costs: A societal perspective that captures all associated costs including productivity losses was adopted to provide a comprehensive cost analysis. All costs are reported in 2019 Chinese yuan renminbi (CNY). US dollar (US$) equivalents were calculated using a rate of 1 US$ = 6.9 CNY (2019). 41 Dated prices were inflated using the World Bank consumer price index for China.42,43
Patient transfer costs were based on typical ambulance costs in Beijing. 31 Hospitalisation and post-hospitalisation management costs stratified using the mRS score were derived from the China National Stroke Registry (CNSR) database.30,44 The hospitalisation cost for transferred patients was calculated by applying weights observed 32 to the median hospitalisation costs. Thrombolysis treatment costs were based on the estimates by Pan et al. 30 , using the CNSR and TIMS-China data. For those under retirement age (60 years), the mean indirect cost was sourced from Hu et al.'s 1-year follow-up study. 33 Using average cost analysis weights observed from the A Very Early Rehabilitation Trial (AVERT), 34 the indirect cost for each mRS score for the first year post-stroke was determined. These indirect costs were further adjusted using the expected return to work rate by mRS score to gain the indirect costs over the long term. 35
The cost of the telestroke network was applied as a cost per telestroke consultation per patient. 29 The pre-adjusted cost (i.e. without government subsidisation) was used and is assumed to include all telestroke-related costs such as the costs of neurologist on call, extra personnel to coordinate the network, telemedicine equipment, maintenance and training.
Utility: Utility scores were valued between 0 representing death and 1 representing perfect health. Utility scores, assigned according to mRS score, were obtained from Wang et al.’s 36 study. These were assessed via the EuroQol EQ-5D-3L questionnaire using Chinese preference weights.
Model outputs
Model outputs were total costs, quality-adjusted life years (QALYs), and the incremental cost-effectiveness ratio (ICER). Total costs were summed across all model cycles and averaged across all simulated patients. Effectiveness was measured by QALYs, calculated by multiplying the life years lived by the utility score associated with being in a particular health state. The ICER (incremental cost per QALY gained) was calculated by dividing the mean difference between total costs by the mean difference in QALYs between the two groups. A willingness-to-pay of ≤CNY191,378/QALY (three times the 2019 GDP per capita of China, US$27,736) was determined to be the threshold for cost-effectiveness.45,46
Sensitivity analyses
One-way sensitivity analyses were performed to identify the key drivers that influenced the ICER by varying the input parameters within a range informed by literature or assumptions. Additionally, probabilistic sensitivity analysis (PSA) was conducted where the distribution of each identified key driver was incorporated to sample 2000 iterations to parameterise the model. Lastly, a short term time horizon of 5 years was also considered relevant and was tested in our sensitivity analyses.
Results
Systematic review
Literature search
The literature search resulted in the retrieval of 543 citations. An additional 16 articles were identified from the citation lists of retrieved articles. After removal of duplicates, 448 records were screened. Of these, 58 full-text articles were assessed for eligibility. Eight articles were included in the systematic review. The search strategy performed for each database (Supplementary Tables 2 to 4), PRISMA flowchart (Supplementary Figure 1) and a master list of included studies are provided in the online supplementary material.
Characteristics of included studies
The included studies comprised two cost-effectiveness and six cost–utility analyses investigating the use of telemedicine network(s) in the USA (five), France (two) and Denmark (one). All studies entailed the development of a model to estimate the costs and effectiveness of telestroke, with five20,47,48,49,50 mainly relying on inputs sourced from the literature, whilst the other three19,25,51 used within-trial data and model-based extrapolation analyses. The perspective ranged from individual hospitals25,47,48 to a broader societal context.20,49 The time horizon ranged from the length of inpatient stay 25 to a lifetime approach.20,49
Of the eight studies, five reported telestroke as cost-effective (included four as cost-saving),19,20,47,49,50 two were potentially cost-effective25,51 and one did not report results clearly. 48 For studies that compared cost-effectiveness across various time horizons, the cost-effectiveness of telestroke consistently improved over a longer period of time.20,49,50 Table 2 summarises characteristics of each study and their key results.
Comparison summary of included studies.
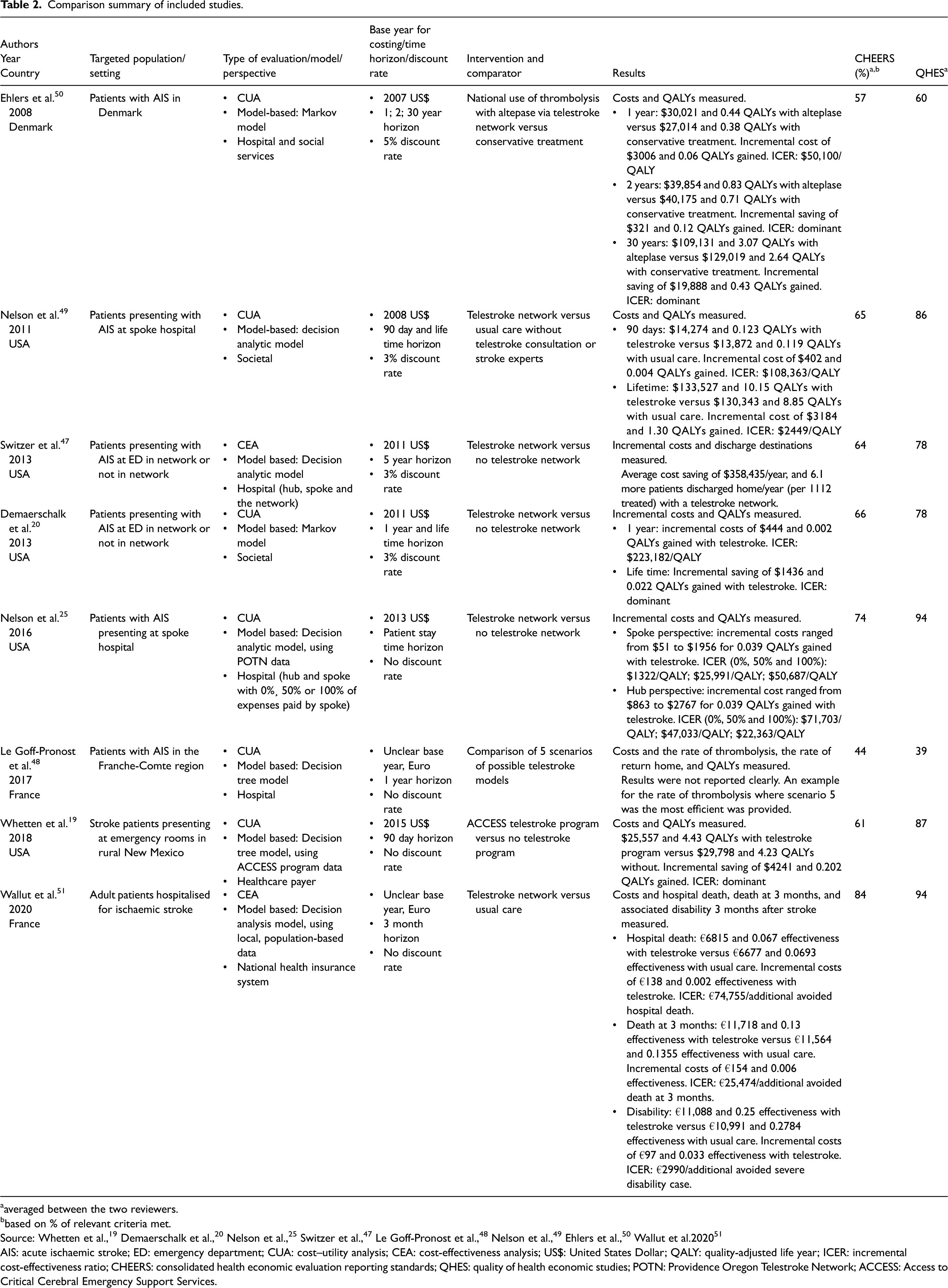
averaged between the two reviewers.
based on % of relevant criteria met.
Source: Whetten et al., 19 Demaerschalk et al., 20 Nelson et al., 25 Switzer et al., 47 Le Goff-Pronost et al., 48 Nelson et al., 49 Ehlers et al., 50 Wallut et al.2020 51
AIS: acute ischaemic stroke; ED: emergency department; CUA: cost–utility analysis; CEA: cost-effectiveness analysis; US$: United States Dollar; QALY: quality-adjusted life year; ICER: incremental cost-effectiveness ratio; CHEERS: consolidated health economic evaluation reporting standards; QHES: quality of health economic studies; POTN: Providence Oregon Telestroke Network; ACCESS: Access to Critical Cerebral Emergency Support Services.
With regard to the quality assessment of the eight studies, the majority were of good quality, but tended to perform less well with regard to reporting (Table 2).
Modelled cost–utility analysis
Base case
The results indicate that a telestroke network in rural China was a dominant strategy (both cost saving and more effective) compared to no telestroke network. The telestroke network resulted in a cost saving of CNY4328 (USD627) and 0.0925 QALYs gained per patient, compared to no telestroke network. Table 3 reports average total costs per patient and costs by cost category, and shows that the cost savings were primarily attributable to transfers avoided given a telestroke network.
Results for base case and probabilistic sensitivity analysis.
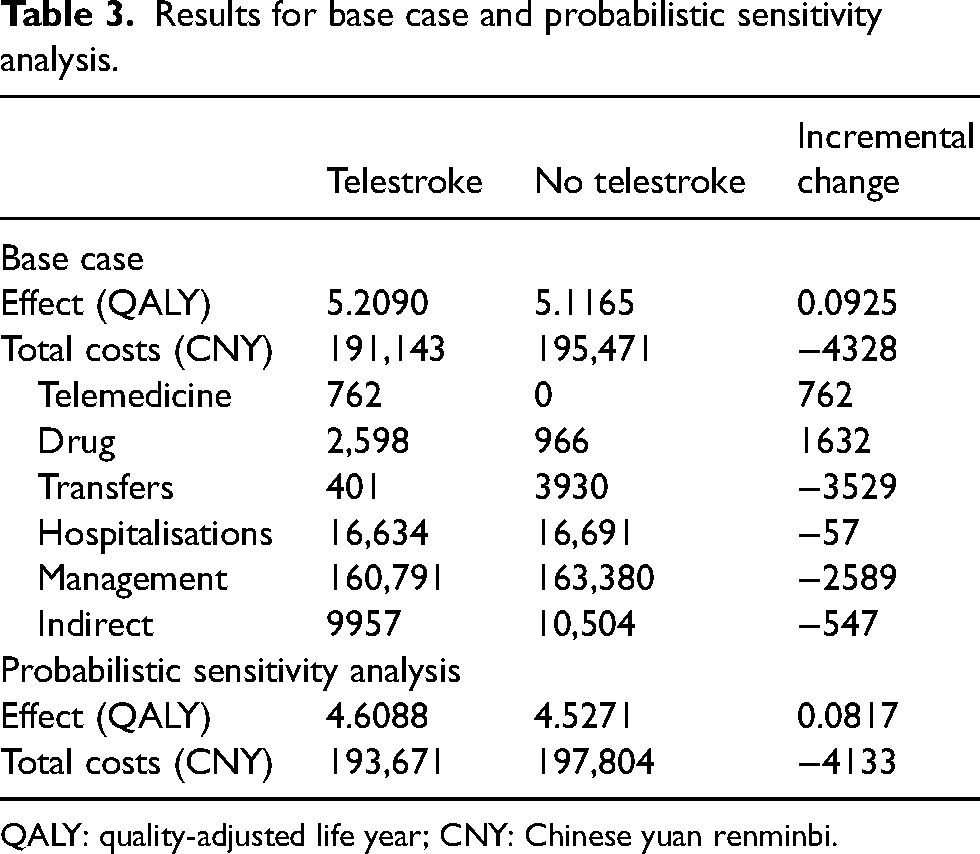
QALY: quality-adjusted life year; CNY: Chinese yuan renminbi.
Sensitivity analyses
Results were most sensitive to the probability of receiving thrombolysis and the cost of hospitalisation for transferred patients. The results of the one-way sensitivity analysis are presented in a Tornado diagram (Figure 2). In terms of deterministic probability analysis, the probabilities of mRS outcome via OTT time for thrombolysis were tested by increasing and decreasing the effect size of thrombolysis by 10%. When the efficacy was reduced, thrombolysis did not produce a benefit in terms of incremental QALYs, but remained less costly.
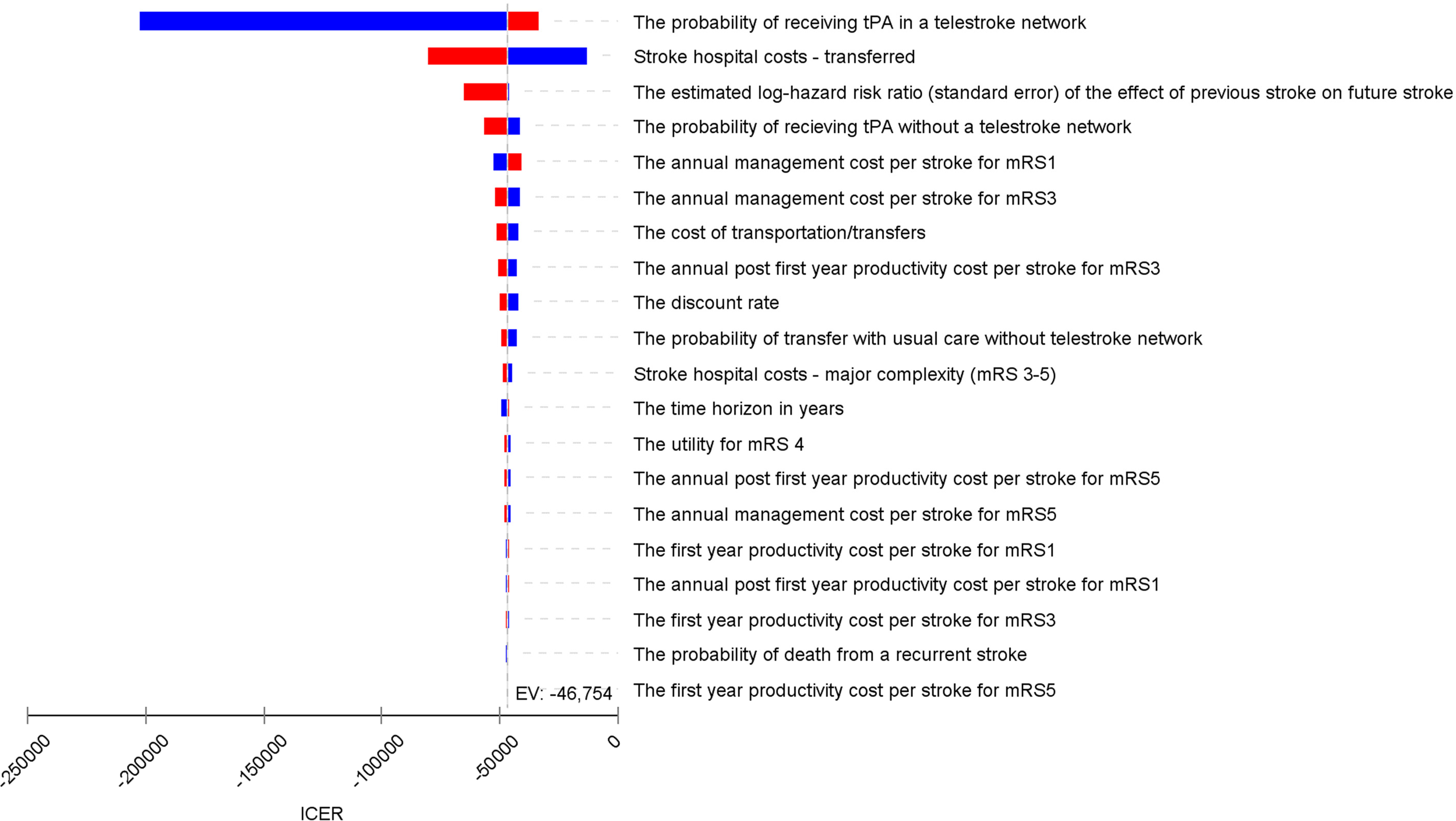
Tornado diagram. This illustrates the change in the incremental cost-effectiveness ratio (ICER) when relevant variables are tested with the high and low values of the input parameters.
PSA confirmed the robustness of base case result. Of the 2000 iterations modelled, the telestroke network resulted in a mean cost saving of CNY4133 (95% confidence interval (CI) 3863, 4353) (US$599) and 0.0817 (95% CI 0.0764, 0.0938) QALYs gained per patient, compared to no telestroke network. A hundred percent of these iterations fell within the south-east quadrant of the cost-effectiveness plane, indicating that having a telestroke network was both cost saving and more effective compared to no telestroke service (Figure 3).
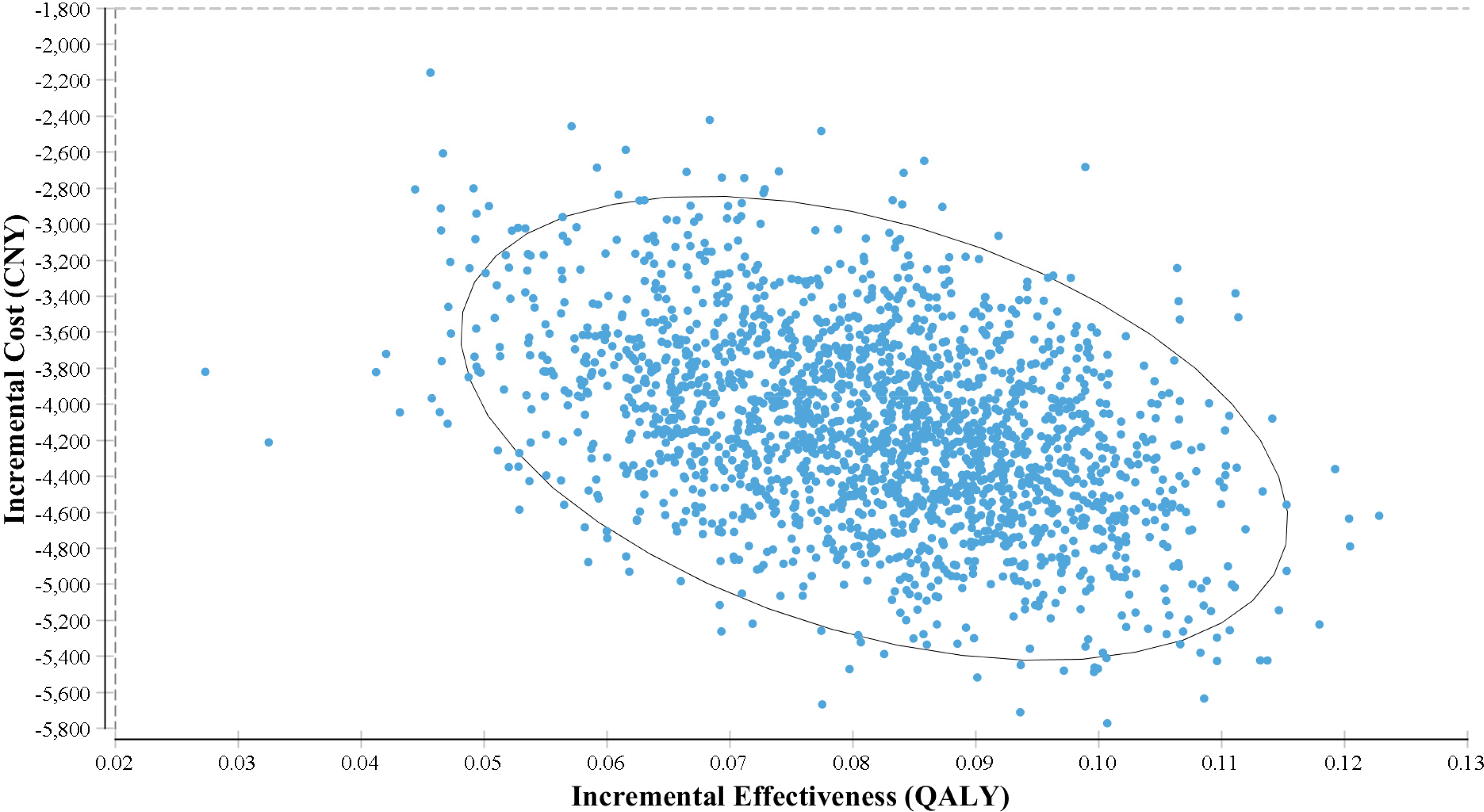
Cost-effectiveness scatterplot. This shows the probability that a telestroke network is cost effective under a willingness-to-pay (WTP) threshold of CNY 191,378. Out of 2000 iterations, 100% fell within the south-east quadrant, suggesting telestroke was less costly and more effective.
Sensitivity analysis conducted for a short term time horizon of 5 years indicates that telestroke remained the dominant strategy compared to no telestroke network. The telestroke network resulted in a cost saving of CNY2550 (US$370) and 0.0299 QALYs gained per patient, compared to no telestroke network (Table 4).
Results for short term (5-year) time horizon.

QALY: quality-adjusted life year; CNY: Chinese yuan renminbi.
Discussion
Systematic review
This is the first systematic review performed for the economic evaluation (cost-effectiveness and cost–utility analyses) of telemedicine/telestroke on the use of thrombolysis in patients with AIS. Overall we identified eight economic evaluations that met our inclusion criteria whereby each adopted different analysis time horizons, ranging from length of inpatient stay 25 to a lifetime horizon.20,49 Cost-effectiveness of telestroke was observed to consistently improve over time, largely due to the high upfront costs of implementation, coupled with greater cost savings in care and quality-of-life gains in the longer term. Cost savings arose primarily from decreased nursing home care required or avoided between hospital transfers. Whetten et al. 19 concluded a cost-saving associated with telestroke within 90 days from a healthcare payer perspective, mainly attributable to transfers avoided.
Incremental costs measured over short timespans ranged from cost savings of US$4241 19 to costs of US$3006 50 per patient, whilst for long-term horizons, they ranged from cost savings of US$19,888 50 to costs of US$3184. 49 All studies reported improved effectiveness or quality-of-life outcomes with telestroke. Cost-effectiveness studies reported an estimated 6.1 more patients discharged home per year (per 1112 patients treated) 47 or a reduction of three disability cases per 100 patients 51 associated with a telestroke network. For cost–utility analyses, the incremental benefits ranged from 0.002 20 to 0.2 QALYs 19 during the shorter time horizons, and 0.02 20 to 1.3 QALYs gained 49 over the long term. During the short term, the ICERs varied from dominant19,50 to US$223,182/QALY, 20 whereas a smaller ICER range was observed over the long term, which varied from dominant20,50 to US$2449/QALY. 49
Modelled cost–utility analysis
The results of our modelled analysis for a given province in mainland China provide evidence that telestroke for AIS in rural China offers potentially greater benefits and lower costs, compared to no telestroke network. Similar to Whetten et al., 19 the cost savings were mainly attributable to the decreased need for transfers. Even when the costs of transfers were excluded from the analysis, telestroke was still considered to be cost-effective, with a cost saving of CNY799 (US$116) from a societal perspective. This is consistent with the majority of previous economic evaluations, which determined telestroke as cost-effective (or cost saving). The values from our model fell well within the incremental cost savings/costs and QALYs of these previously reported evaluations.
Despite the advent of a telestroke network increasing the proportion of patients who arrive within 4.5 h receiving thrombolysis from 7.8% to 20.4%,19,20,24,25 the resultant difference in QALYs and post-stroke management costs were modest. The incremental benefit of thrombolysis due to telestroke may be underestimated in our study. Zhao et al. 52 have reported the ability of telestroke to successfully increase the rate of thrombolysis comparable to that of leading stroke centres. Data from the Big Data Observatory Platform for Stroke of China (of 227 hospitals surveyed) have indicated a thrombolysis rate of 25% 53 (assuming 31% of patients arrive at hospital within 4.5 h of symptom onset 23 ), higher than the rate used in our analysis. If the probability of thrombolysis in telestroke was increased to 25%, the incremental cost savings would increase to CNY4629 (US$671) and 0.12 QALYs gained.
A major strength of our modelled analysis was that it was underpinned by evidence from a comprehensive systematic review, although this search was restricted to studies published in English. There have been no published economic evaluations of telestroke for low- to middle-income countries published in English. To the best of our knowledge, our simulation is the first attempt to show the costs and benefits that might be found from providing telestroke in China.
Our study has a number of limitations. Input variables including probability of receiving thrombolysis, telemedicine and stroke-related costs, and utilities were all indirectly applied – but were extensively tested in our sensitivity analyses. The probability of thrombolysis without a telestroke network was calculated based a small sample size of 253 (compared to the sample of 4425 used to calculate the same within a telestroke network).19,20,24,25 Transfer rates were obtained from the Access to Critical Cerebral Emergency Support Services (ACCESS) program 19 where patients within the telestroke network had significantly fewer transfers compared to those without a network. In reality, however, transfers from local hospitals (spokes) to the stroke centre (hub) may be dependent on the capacity of the spoke for treating AIS patients; this was not considered in our model. The results of this study, and in particular the costs, are pertinent to China and may not be generalisable to other settings. It, however, may provide lessons for other middle-income countries with large rural populations. Future studies investigating the cost-effectiveness of telestroke in China would benefit from using local within-trial data to validate the findings.
Conclusion
Telestroke networks are generally cost saving or cost-effective whereby they can provide health benefits that we are prepared to pay for as a society. We presented a de novo cost–utility analysis for China as an example of a middle-income country. Our results indicated telestroke was a highly cost-effective strategy, which may enhance stroke care and improve favourable outcomes in patients in rural China with AIS. With the expected future increased incidence of stroke, a nationwide telestroke network may be an ideal strategy, particularly for remote areas of China.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X211032407 - Supplemental material for Telestroke for acute ischaemic stroke: A systematic review of economic evaluations and a de novo cost–utility analysis for a middle income country
Supplemental material, sj-docx-1-jtt-10.1177_1357633X211032407 for Telestroke for acute ischaemic stroke: A systematic review of economic evaluations and a de novo cost–utility analysis for a middle income country by Elise Tan, LanGao, Huong NQ Tran, Dominique Cadilhac, Chris Bladin, and Marj Moodie in Journal of Telemedicine and Telecare
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.