
Abstract
Introduction
As coronavirus disease 2019 (COVID-19) hit the US, there was widespread and urgent implementation of telemedicine programs nationwide without much focus on the impact on patient populations with known existing healthcare disparities. To better understand which populations cannot access telemedicine during the coronavirus disease 2019 pandemic, this study aims to demographically describe and identify the most important demographic predictors of telemedicine visit completion in an urban health system.
Methods
Patient de-identified demographics and telemedicine visit data (N = 362,764) between March 1, 2020 and October 31, 2020 were combined with Internal Revenue Service 2018 individual income tax data by postal code. Descriptive statistics and mixed effects logistic regression were used to determine impactful patient predictors of telemedicine completion, while adjusting for clustering at the clinical site level.
Results
Many patient-specific demographics were found to be significant. Descriptive statistics showed older patients had lower rates of completion (p < 0.001). Also, Hispanic patients had statistically significant lower rates (p < 0.001). Overall, minorities (racial, ethnic, and language) had decreased odds ratios of successful telemedicine completion compared to the reference.
Discussion
While telemedicine use continues to be critical during the coronavirus disease 2019 pandemic, entire populations struggle with access—possibly widening existing disparities. These results contribute large datasets with significant findings to the limited research on telemedicine access and can help guide us in improving telemedicine disparities across our health systems and on a wider scale.
Introduction
One aspect of the US healthcare system is rarely disputed—that disparities exist within it, creating a system that does not equally serve those who participate in it. This issue has been researched, analyzed, and discussed to better understand who is impacted and what changes can be made to improve the system.1,2 Much of the research has been limited to evaluating baseline health without having to contend with a major public health crisis. An extraordinary event occurred in 2020 that transformed the US healthcare system and impacted millions of US residents who seek assistance from healthcare providers. The coronavirus disease 2019 (COVID-19) virus arrived in the United States in late 2019 or early 2020, with the first case officially reported in Florida on March 1, 2020. 3 This pandemic changed the way in which healthcare would be provided to patients by diverting many patient encounters to occur via telemedicine. While telemedicine has existed since 1959, its main use was in rural areas (1990s–2000s) and generally focused on certain specialties including: cardiology, dermatology, and pulmonology. 4 Due to many patient-centered factors including resistance to new technology and uncertainties regarding insurance coverage, telemedicine has not been widely embraced. Many patients felt they would not receive the same level of medical care via telemedicine that they would with an office visit. “According to some patients and providers, contact via telecommunications lacks personal connection, limits interaction, and inhibits a sincere patient-provider relationship.” 5 While patients were concerned about their relationships with their providers, the resistance to telemedicine was quickly overcome by fear for COVID-19 exposure during an in-office experience.
This desire to receive medical attention, without requiring social interaction and physical contact, helped to make telemedicine more desirable to patients. Simultaneously, on March 30, 2020, the Centers for Medicare and Medicaid Services (CMS) took unprecedented and rapid action expanding telemedicine reimbursement to include the majority of outpatient and inpatient healthcare with commercial health insurers following suit. 6 Prior to COVID-19, “uncertainty about insurance coverage and reimbursement policies for telemedicine has historically been a major barrier to adoption.” 6 While these new policies removed the barrier of insurance reimbursement, some patients were likely unaware of this change. The interest to be treated virtually in combination with the reimbursement changes amounted to a dramatic shift in the way in which healthcare providers serviced patients, a transformation that occurred in an incredibly rapid timeframe.
While there was great interest in telemedicine, the challenge with virtual visits is that people must not only have access to capable devices and high-speed internet, but also must be able to navigate the institution-specific telemedicine workflow. Research has shown that for marginalized populations, the percentage of people with both access to and comfort with technology is reduced relative to other populations. 7 While it seemed likely that telemedicine might further exacerbate disparities in the US healthcare system, the impact on the marginalized populations had not been studied extensively. One study with only 331 patients identified patient disparities in telemedicine implementation among adolescents, finding “no significant differences in telehealth visit completion rates by age, sex, gender, or insurance.” 8 However, non-White patients had lower visit completion rates than White patients (p = 0.003). 8 Another study with 52,585 patients over a 2-month period focused on patient characteristics predicting use of telehealth, emergency room (ER), or office visits. This study found that Blacks, Hispanics, and over age 65 years groups had higher odds of using either ER or office visits versus telehealth, and they concluded “additional research into sociodemographic heterogeneity in telehealth use is needed.” 9 Population-level studies have been performed using county-level data as a proxy for patient race/ethnicity and found lower telemedicine use in majority non-White communities. 10 However, to positively shape the use of telemedicine and equalize healthcare access, there is a need for more robust studies with person-level ethnic/racial data, larger sample sizes, more diverse patient sampling, and over a longer period of time. Our study tries to shed additional light into the impact of telemedicine on these disparities using several months of data in a large, diverse, urban healthcare system.
Methods
De-identified patient data (including: age, race, ethnicity, sex, insurance, preferred language, zip code, and religion) from all UHealth (University of Miami Health System) telemedicine visits (N = 382,076) between January 1, 2020 to October 31, 2020 was compiled. Patients self-selected the categories they identified with for race, preferred language, and religion; however, to standardize these categories, the data were systematized into accepted categories used by the Pew Research Center. 11 Additionally, health system-wide data (provider specialty, clinic location, name of provider, etc.) was collected. Patient zip code data were combined with Internal Revenue Service (IRS) 2018 individual income tax data stratified by income level 12 in order to calculate a weighted average income for each zip code. Additionally, for 1.6% of visits (N = 5762), patients were missing average income; so, these values were imputed with the average of the overall sample (simple mean imputation) to include them in the model. Unscheduled (on-the-fly) visits (N = 6743), erroneous visits (N = 8084) that did not meet telemedicine criteria, and visits that were missing substantial (>50% of) demographic data (N = 4326) were excluded. Visits prior to March 1, 2020 (date of first COVID-19 case in Florida) were excluded from the dataset (N = 159), as pre-COVID telemedicine was infrequently used and designated for a narrow patient population and purpose. Data were checked to confirm that deleted observations were not significantly associated with a particular completion status group. A total of 362,764 visits were included in the analysis. The dataset was analyzed with RStudio 1.2.1335 13 with the additional packages of furniture 14 and lme4 15 and visualized with Tableau 2020.3.2. Descriptive statistics were run as t-tests for continuous variables, and χ2 tests were used for categorical variables. A Bonferroni correction was applied to descriptive statistics to adjust for multiple comparisons. The corrected alpha value used to assess for significance for the descriptive statistics was 0.0036. Mixed effects logistic regression was used to determine impactful patient predictors of telemedicine completion, to control for the effects of the other variables (alpha = 0.05), and to adjust for clustering at the hospital (clinical site) level. Prior to modeling, continuous variables were scaled. The clinical site of the visits (with 51 unique levels) was used as a random effect in the model. Originally, all predictors (both patient and health-system-wide) were put into the model. The model was then optimized using comparison of model fit statistics (Akaike's Information Criteria (AIC) and Bayesian Information Criteria (BIC)).
Results
Overall, 230,030 telemedicine visits were completed out of 362,764 scheduled visits over the months of March to October 2020 at UHealth. Visits hit a peak of 14,852 during the week of May 10, 2020, and overall visit counts slowly decreased over the subsequent months (Figure 1). These results are similar to other population-level studies examining telemedicine use during COVID-19, which saw a similar rapid rise in telemedicine in March (week 11 and 12 of 2020) and hit a peak of visits in week 16 of 2020 (week of April 13). 16 In the final weeks analyzed, the number of visits per week was relatively stable with 9951 visits in the last week. Completion rates were relatively constant (> 60%) with a slight upward trend during the months following April.
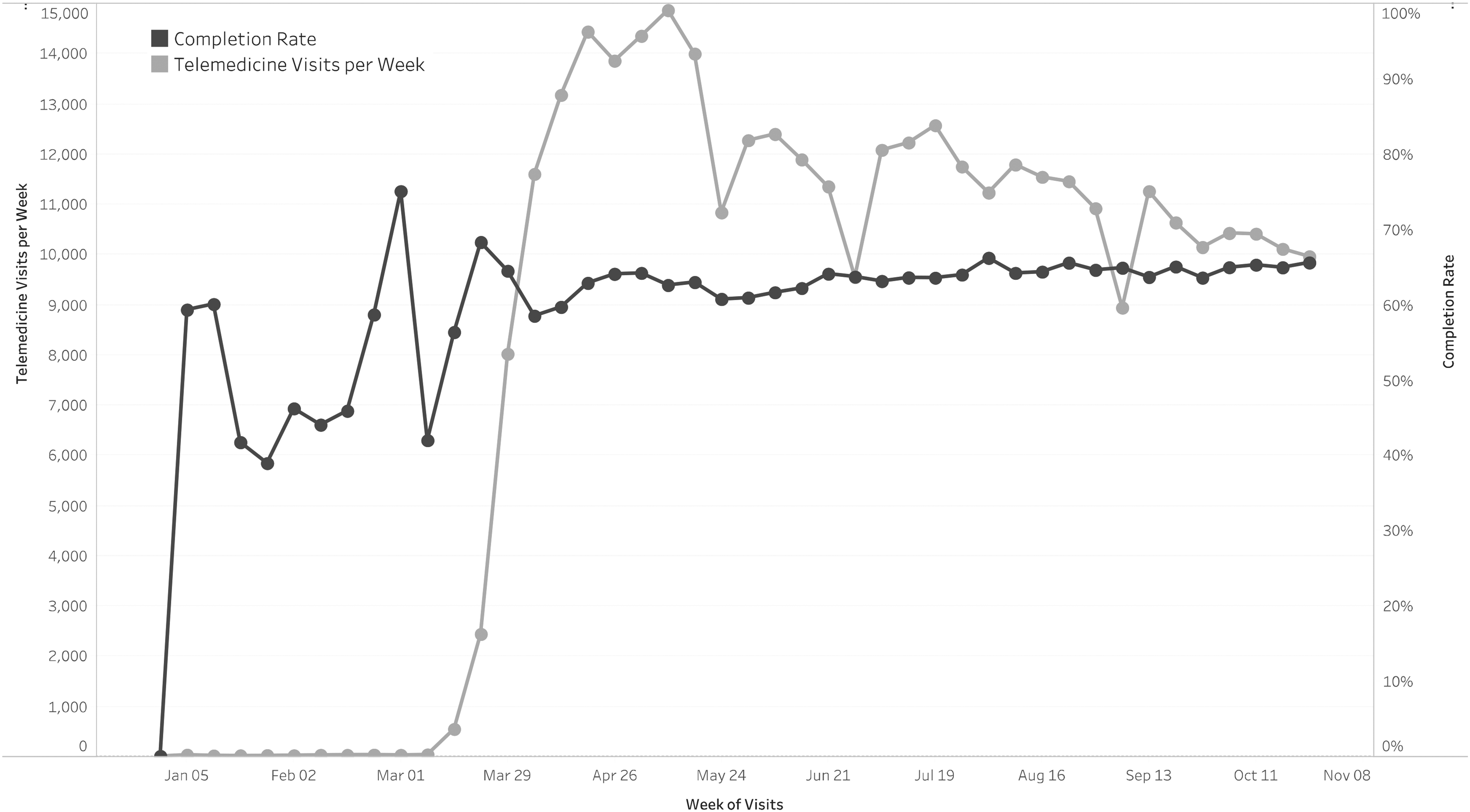
UHealth telemedicine visits and completion rates (per week) between January 1, 2020 and October 31, 2020.
The complete sample included more female patients (59.9% vs. 40.1%) with an average age of 50.8 years (Table 1). The majority of patients were White (73.2%) with only 12.6% of patients being Black and smaller percentages of unknown race (11.7%), Asian (1.7%), or other racial groups (0.9%). Representative of the South Florida population at large, most patients (51.3%) were Hispanic (regardless of race) and 42.2% were non-Hispanic with the remaining 6.4% of unknown ethnicity. Although most of our study population was English-speaking (71.6%), there was a notable proportion of patients self-identifying as Spanish-speaking (27.1%). The breakdown of patient religions was stratified with 32.9% Catholic, 20.6% non-Catholic Christian, 20.4% unaffiliated, 14.4% unknown religion, 7.1% non-Christian Faiths (Jewish, Muslim, etc.), and 4.7% other religions. Much of the study population had commercial insurance (57.8%), followed by Medicare (27.2%), Medicaid (11.9%), uninsured (1.6%), and others (1.5%). The overall weighted average income was $97,700 with the largest percent (38.5%) of patients falling into the income category of under $50,000.
Demographic characteristics overall and by telemedicine completion status from all scheduled telemedicine visits at University of Miami Health System (March 1, 2020–October 31, 2020).
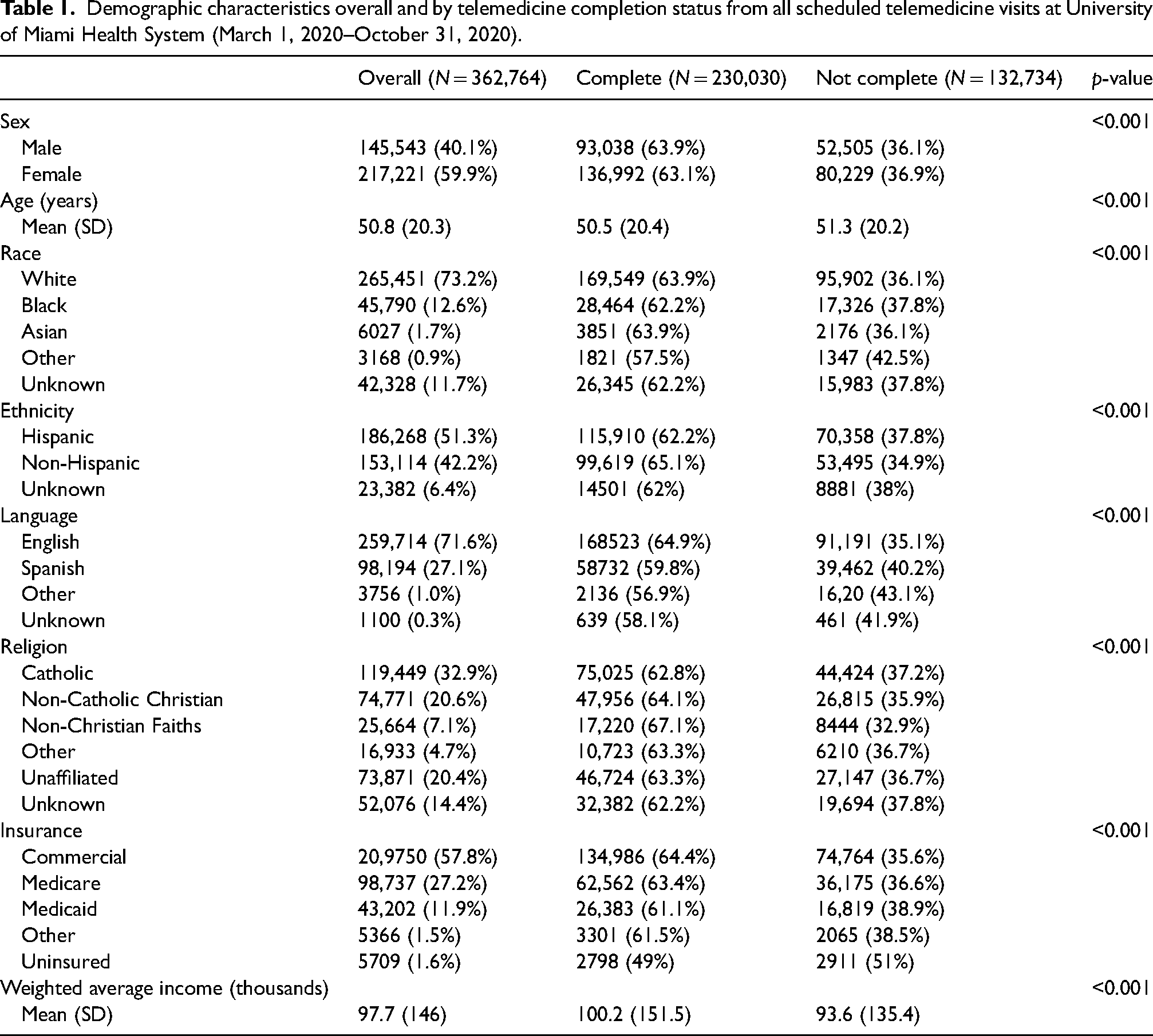
Comparisons between the “completed telemedicine” and “not completed telemedicine” groups showed males having a higher percentage of completion compared to females (63.9% vs. 63.1%) (p < 0.001) (Table 1). Patients were found to be younger in the completed group compared to the not completed group (mean age of completed was 50.5 vs. 51.3; p < 0.001). Statistically significant differences in completion were also found between racial groups (p < 0.001). Also, Hispanic patients (including all races) had statistically significant lower completion rates (62.2% vs. 65.1% of non-Hispanic patients). There were differences between religions with non-Christian Faiths having the highest percentage of completion (67.1%; p < 0.001). Between different insurances, there were substantial differences in completion rates where commercial insurance attained 64.4% of patients completing visits compared to 63.4% of Medicare, 61.5% of other insurances (i.e. Tricare), and 61.1% of Medicaid. The largest disparity was seen in uninsured patients with only 49% completing their visit. The weighted average income of incomplete patients was $93,600 compared to $100,200 for completed patients (p < 0.001).
The best fitting (lowest AIC and BIC) mixed effects logistic regression model included all variables collected, even system-wide predictors such as pre-visit phone/text confirmation status, MyUHealthChart status (UHealth's patient portal in Epic), provider specialty, new to provider, and new to UHealth. With the inclusion of all variables, not only were the fit statistics for the model optimized, but also system-wide factors could be controlled for, allowing close examination of health disparities without concern for confounding effects of other variables. Additionally, possible effects of clustering at the clinical site level were also adjusted for by including clinical site as a random effect. Logistic regression showed similar results to descriptive statistics. Females (odds ratio (OR): 0.957) had a reduced odds ratio of completion (95% confidence interval (CI): 0.943, 0.972) compared to males (Figure 2). For every one unit increase in age, the odds of completion is 0.919 times (95% CI: 0.909, 0.929). Compared to the reference group (White) and controlling for all other factors, minorities had reduced OR of completion (p < 0.001), specifically Black patients (OR: 0.906), Asian patients (OR: 0.892), and other racial group patients (OR: 0.836). Compared to Catholic religion, non-Catholic Christian (OR: 1.034) and non-Christian Faiths (OR: 1.046) had higher completion (p < 0.01); unaffiliated religion (OR: 0.975) had lower completions (p = 0.02), and other or unknown religions were not significantly different from the reference (p = 0.81 and p = 0.36). Regarding insurance, compared to the reference Medicare, uninsured patients (OR: 0.631) had a much lower odds of completion (p < 0.001) (95% CI: 0.592, 0.671). Medicaid patients (OR: 0.852) and other insurance (OR: 0.862) patients also had a lower odds of completing their visits compared to Medicare patients (p < 0.001). Patients covered by commercial insurance (OR: 0.919) had a slightly lower odds of completion compared to Medicare patients (p < 0.001). For every one unit increase in weighted average income, the odds of completion was 1.024 times as likely (95% CI: 1.016, 1.033).
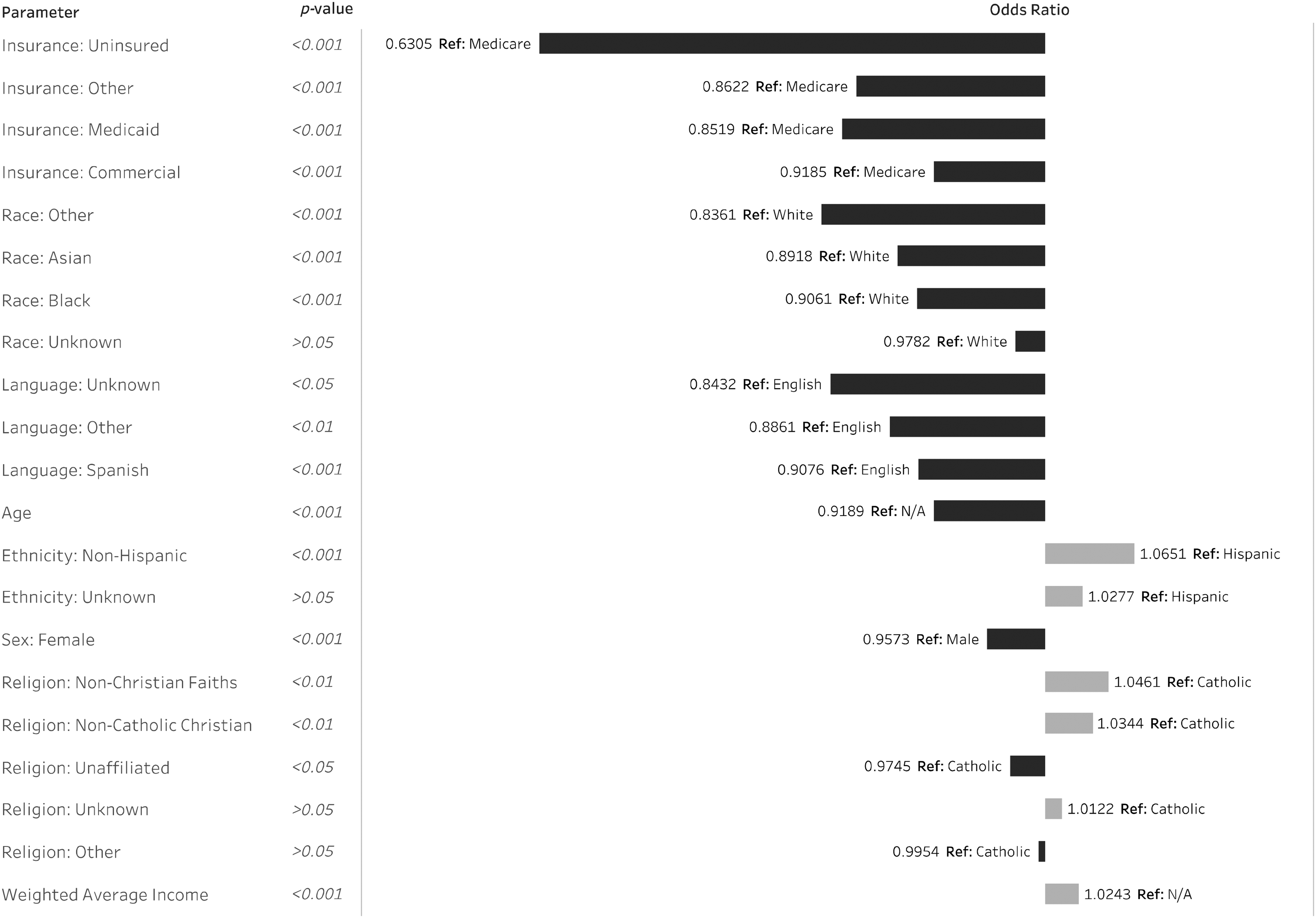
Mixed effects logistic regression of telemedicine visit completion status at UHealth (March 1, 2020–October 31, 2020).
Discussion
In order for patients in our health system to successfully complete a telemedicine visit, they must have access to a capable device (computer, tablet, or smartphone), high-speed internet for video visits, existing MyUHealthChart access (UHealth's Epic patient portal), and the Zoom application downloaded. One possible explanation for our findings is limited broadband access or access to digital technology among our patient population. While this study is unable to examine these factors directly and thus cannot adjust for them in the model, we believe these may be drivers of the disparities we see regarding successful telemedicine use. Results from this study’s descriptive statistics were aligned with the national statistics for access to smartphone ownership, 17 computer, 18 and Internet use. 19 Recent surveys reveal 92% of 30–49 years old own a smartphone, compared to only 53% of those >65 years old. Household income also plays a role in smartphone ownership. Of those earning >$75,000, 95% owned a smartphone in comparison to 71% for those earning <$30,000. For computer ownership and internet usage, there were similar inequities along age, race, and income. Comparing races, 89.9% of Whites had a computer at home, and 83.9% had Internet. Minorities reported lower rates, specifically 84.1% of Blacks had a computer at home, and 72.6% had internet; 88.7% of Hispanics had a computer at home, and 77.3% had internet. Of those with household income <$25,000, only 71.7% had a computer at home and 58.8% had internet. In contrast, 98.8% of those with household income >$150,000 had a computer at home and 96.5% had internet.
Additionally, these internet and device disparities results mirrored those from the 2018 National Healthcare Quality and Disparities Report (QDR), 20 which reported significant differences in the quality of and accessibility to healthcare based on race/ethnicity and income. The QDR showed that 40% of health quality measures were worse for Blacks than Whites and 35% of measures were worse for Hispanics. In terms of income inequities, the QDR reported that those in the “Poor” category, with an income less than 100% of the Federal Poverty Level (FPL) had 60% of health quality measures worse than those in the “High income” group (400% or more of FPL).
While telemedicine use continues to increase, entire populations may struggle with accessing it—mirroring existing disparities in technology and medicine. Perhaps, the known healthcare disparities are exacerbated in telemedicine due to the lack of access to technology such as smartphones, computers, and the Internet. This digital divide could put those individuals at a disadvantage to effectively use telemedicine and may further increase healthcare disparities due to limited access to healthcare at peak COVID times. Within UHealth, the percentage of telemedicine visits out of overall visits went from less than 1% (pre-COVID) up to 68% during the month of April. This reflects an overall decreased opportunity for in-person visits and predilection for virtual visits at the health system level during this time. This temporary switch in how healthcare was traditionally delivered likely could have exacerbated existing health disparities as those of less means would lack access to technology and be unable to complete virtual visits and receive care. While some of this population may have been able to access in-person care (even though it was limited) at this time, there would still ultimately be disparities. These people would have less opportunity for social distancing and have increased COVID exposure risk than those that could have completed a telemedicine visit. Ultimately, additional research into telemedicine disparities is needed to better understand this connection between existing disparities and those found in this study in order to address disparities on a wider scale.
While this study elucidates many disparities in telemedicine, there are limitations to its usefulness and applicability. For example, there are a subset of patients who are unaccounted for in this study—those who cancelled or never scheduled a telemedicine appointment. We only capture those interested and willing to participate in a telemedicine visit, which is not reflective of our entire patient population. In addition, we lacked the ability to identify repeat patients, as we were missing unique identifiers (i.e. medical record numbers (MRNs)) since we were provided with a de-identified dataset, hampering our ability to evaluate completion rate changes with repeat patients. However, it was anecdotally noted, that patients with difficulty accessing telemedicine on one visit tend to have difficulty on subsequent visits. Due to limitations in the IRS 2018 dataset, we only had access to weighted average income instead of median income (more typically used), potentially overestimating the income of a specific zip code and increasing differences between zip codes. Additionally, since we only had data from a single healthcare system, this research's application is limited to those that are similar in the patient populations they serve and in their overall structure.
Having seen these disparities, we must take tangible steps to improving access and equity across all populations. Especially in light of studies showing minorities being greatly afflicted by COVID-19 in comparison to others, 21 this is a critical time for minorities' health. In the early ages of telemedicine, this new technology was used in order to reach rural and Native American populations that could not otherwise access healthcare. 22 Today, telemedicine could be a stepping stone to improving the health of marginalized populations by removing major barriers to in-person care. Not only does it remove the physical commuting to a visit, but also reduces the required time away from work/family duties to seek care, which should lead to a favorable cost/benefit outcome. It may also reduce some hesitations or personal biases certain populations may have to seeking care. With the ability to speak with a provider while remaining “distanced” through a computer or phone screen, populations may feel less intimidated and more comfortable speaking with a physician. Additionally, telemedicine can reduce the need for coordination of assistance with transportation and mobility for appointments. Overall, telemedicine has many benefits to increasing the health of the population; therefore, we must strive to improve equity in access.
As a first step to addressing disparities across telemedicine, improving computer and internet access is paramount. Establishing designated areas in public libraries or community centers that individuals can reserve for telemedicine visits is a possible way to address access inequities. This would require buy-in from government or community stakeholders but could assist populations struggling to access telemedicine. Previous studies have recommended partnerships with community organizations as they “are best equipped to serve patients in their communities.” 23 Utilizing these people who have local expertise can ensure that these interventions are best directed at the target population. 23 It is important to note that Florida currently has laws that restrict community broadband access by imposing taxes and subjecting “municipalities to restrictions on capital-intensive initiatives that make broadband projects difficult to begin.” 24 Given these challenges to establishing municipal broadband networks, to enact change on a community level, we may first need to address this problem on a larger state-wide or national level. Additionally, state and national policies that promote inclusion of marginalized populations in telemedicine and all forms of electronic health delivery could help incentivize and improve access.
In addition to the issues with building telemedicine infrastructure, there are also issues regarding the economics of wide-scale telemedicine usage. With insurance changes in March 2020, most insured patients nationwide became covered for telemedicine visits. However, the awareness of this change may be limited especially in marginalized populations who may not know the changing details of their health insurance or be able to easily get updated information. It is essential to have wide-scale patient education on the coverage of telemedicine so that more people can confidently utilize this method of care delivery. Ideally, this patient education can be integrated into existing outreach programs that already serve these populations. It is important to note that there is uncertainty regarding the post-COVID-19 telemedicine reimbursements and coverage, because during this current public health crisis, telemedicine coverage was urgently expanded and may change in the future. For uninsured individuals, additional governmental funding to community clinics that aim to expand their telemedicine utilization would be key to reaching this population. 23 Overall, governmental policy that promotes continued usage of telemedicine is necessary to develop this technology and reach those that would otherwise be unable to access care.
Critical to all of these possible interventions is awareness of disparities and promotion of inclusive policies at all levels, extending from the health system to the federal level. Establishment of “health equity task forces” at hospitals could help in addressing these disparities. 23 This could be achieved by closely monitoring equitable access to telemedicine by collecting individual data on “technology literacy, access, and privacy.” 23 In addition to monitoring access to telemedicine, these task forces could also monitor patient experience and self-reported outcomes 25 to ensure not only equitable access, but also equitable benefits from telemedicine. Findings from these task forces could help guide hospital-level policies of equity and inclusion. Our patient population is uniquely diverse, which enables us to look at certain disparities that other parts of the US might be unable to assess. While this allows us to better understand disparities across the Latino and Caribbean populations, the regional population is not necessarily representative of generalized US demographics. 26 Additional research into other minority groups is necessary to guide policy decisions overall. As we continue to move forward, it is imperative that actions are taken to allow telemedicine to be accessed by all who are interested, so that this technology can fulfill its potential.
Footnotes
Acknowledgements
The authors would like to thank Anantha Gangadhara who performed the clinical data request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.