
Abstract
Summary
We conducted a systematic review of research into callers making multiple calls to crisis helplines. Two databases were searched, identifying 561 articles from 1960 until 2012, of which 63 were relevant. Twenty-one articles from 19 separate studies presented empirical data about callers making multiple calls to crisis helplines. Of the 19 studies, three were intervention studies, five were surveys of callers and 11 were call record audits. Most studies were conducted in the USA and defined frequent callers as people making two or more calls. Frequent callers were more likely to be male and unmarried compared to other callers. There were no reported differences between frequent callers and other callers with regard to age, mental health conditions or suicidality. Three studies tested interventions designed to better manage frequent callers. These studies, even though small, reported reductions in the number of calls made by frequent callers. Suggested techniques for responding to frequent callers included: limiting the number and duration of calls allowed, assigning a specific counsellor, implementing face to face contact, the service initiating contact with the caller instead of waiting for callers to contact the service, providing short term anxiety and depression treatment programmes by telephone, and creating a specific management plan for each frequent caller. Future work requires robust study design methods using larger sample sizes and validated measurements.
Introduction
Crisis helplines for emotional wellbeing have existed since the 1950s, 1 each with their own purpose and target group.2–4 Most were established to provide timely assistance to people who were experiencing a crisis of suicidality or depression. 5 The crisis helplines have used different service models, from a non-directive, listening approach to a more directive approach.2,4,6,7 Callers to crisis helplines typically remain anonymous, call at any time of the day, and speak to trained personnel who assist them to manage their crisis.2,5,8 The support provided is usually not of an ongoing nature. 2 A mixture of lay and professional personnel operate crisis helplines, some on a paid basis and some as volunteers.
Research suggests that people who make multiple calls to crisis helplines may be using the services inappropriately.9,10 These callers are commonly known as frequent, 11 chronic, 10 multiple or repeat callers. 12 In this paper we refer to them as frequent callers. The first study of frequent callers to crisis helplines for emotional wellbeing was published in 1965 and described them as callers who took up a lot of time with complex physical and mental health problems. 13
Crisis helplines struggle to know how to best respond to frequent callers as they challenge the conventional crisis model of care with their contacts.6,8,9,12,14 Frequent callers seek help regularly from crisis helplines and do not always appear to have an immediate crisis.10,12 They also take up time, which prevents other crisis calls from being taken.8,11 Crisis helplines have begun to consider different ways to respond to frequent callers, including limiting their access.10,11 However, concern exists over whether limiting their access may trigger a further crisis. 9 Currently, crisis helplines manage this subgroup of callers in an ad hoc manner. There is a need for an evidence-informed approach.
We have therefore carried out a systematic review of the literature about frequent callers to crisis helplines. The aims of the systematic review were to:
describe frequent callers, in terms of their socio-demographic and clinical characteristics, the nature and frequency of their calls, their use of other services and treatments, and the outcomes of their contact; discuss the impact that frequent callers have on crisis helplines; identify potential interventions to respond to the needs of frequent callers.
Methods
Articles were included in the review if they presented empirical data on callers who made multiple calls to crisis helplines, and were published in English between 1960 and 2012. The exception was brief case studies, which were excluded.
Two databases, Medline and ProQuest, were searched in March 2013. The search terms included: (Suicide OR Depression OR Mental Health) AND (Emergency Telephone Advisory OR Helpline OR Hotline OR Crisisline OR Suicide Prevention Cent* OR Crisis Intervention Service OR Crisis Support Service) AND (Chronic OR Frequent OR Repeat) AND (Call* OR User). The reference lists of potentially relevant articles were searched to identify additional articles, which were obtained. Titles and abstracts were reviewed to identify relevant articles, and all duplicate records were removed. The full text article and citation of potentially relevant articles were downloaded into Endnote and read by one author. Articles about which there was uncertainty were discussed with the other authors and a decision was made about whether to include them. All articles which presented empirical data on callers who made multiple calls to crisis helplines were included.
After identifying eligible papers, information from each article was stored in a spreadsheet. The information included: authors, publication year, study aim, crisis helpline name and location, frequent callers definition, sample selection and size, time period and follow-up, data collection methods, variables measured, interventions, results, limitations and conclusion. Data for each of these variables were categorised and then summarised. The ratio between calls and callers and the 95% confidence interval was calculated using a standard package (STATA version 12 15 ) for the studies that provided sufficient information about the caller population.
Results
A total of 561 articles were identified through the database search and from within text references, after duplicate records were removed. Four hundred and ninety-eight articles were excluded after reading the title and abstracts as they did not have crisis helplines as their primary focus. Of the 63 full text articles reviewed, an additional 29 articles were excluded as they did not relate to callers making multiple calls. Thirty-four articles discussed callers who made multiple calls; however on further review only 21 presented empirical data, and the remaining articles comprised opinion pieces and brief case studies (Figure 1). Thus 21 articles met the inclusion criteria, see Tables 1–3. The 21 articles represented 19 separate studies as Gould et al.
16
and Kalafat et al.
17
reported on an evaluation of crisis helpline outcomes at eight sites in the US; and Farberow et al.
18
and Litman et al.
13
presented findings on a study of frequent callers to a Los Angeles crisis helpline. In the 21 articles included in this review, callers who made multiple calls to crisis helplines were referred to as frequent, chronic or repeat callers.
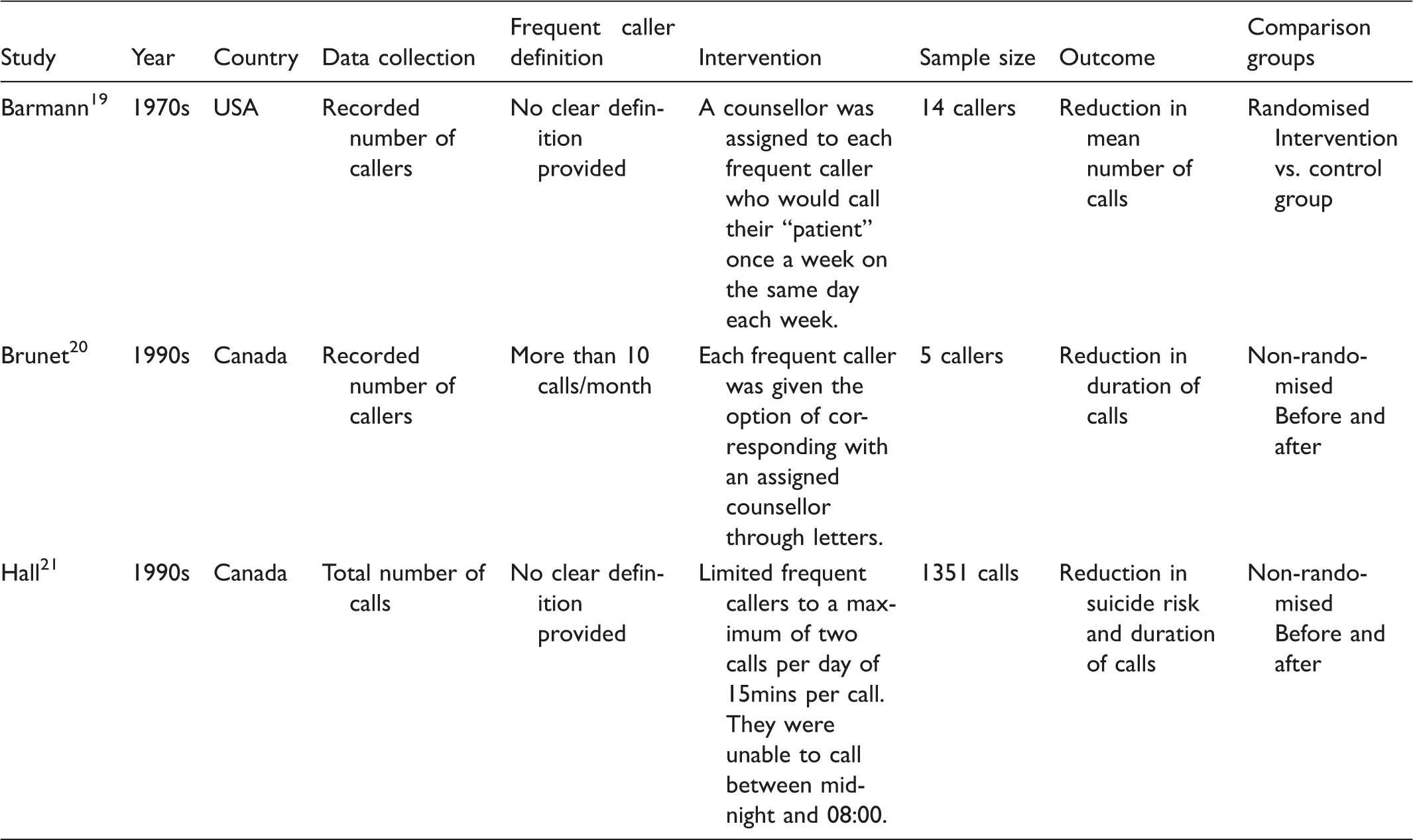
Flow diagram of studies included in the systematic review. Intervention studies included in the review.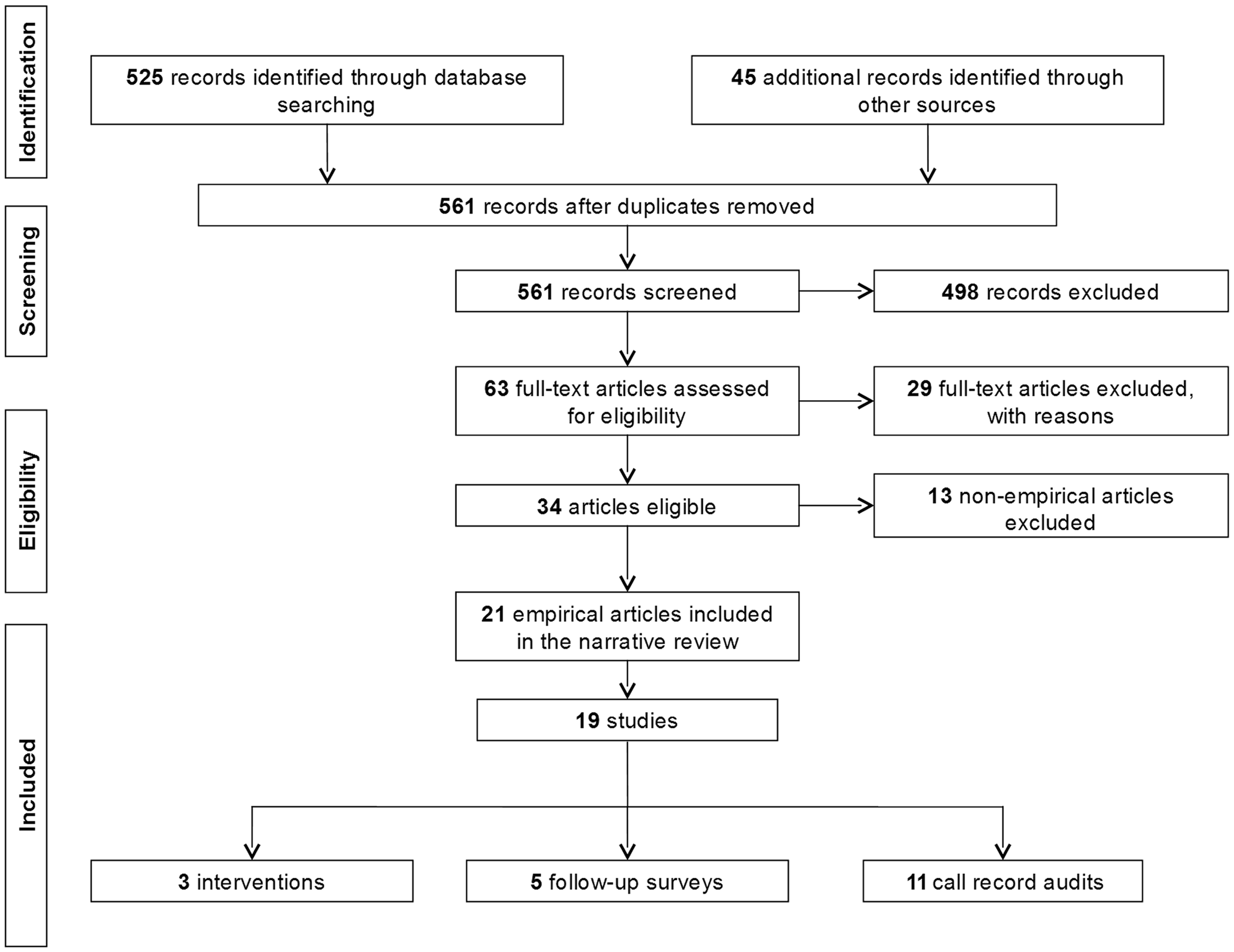
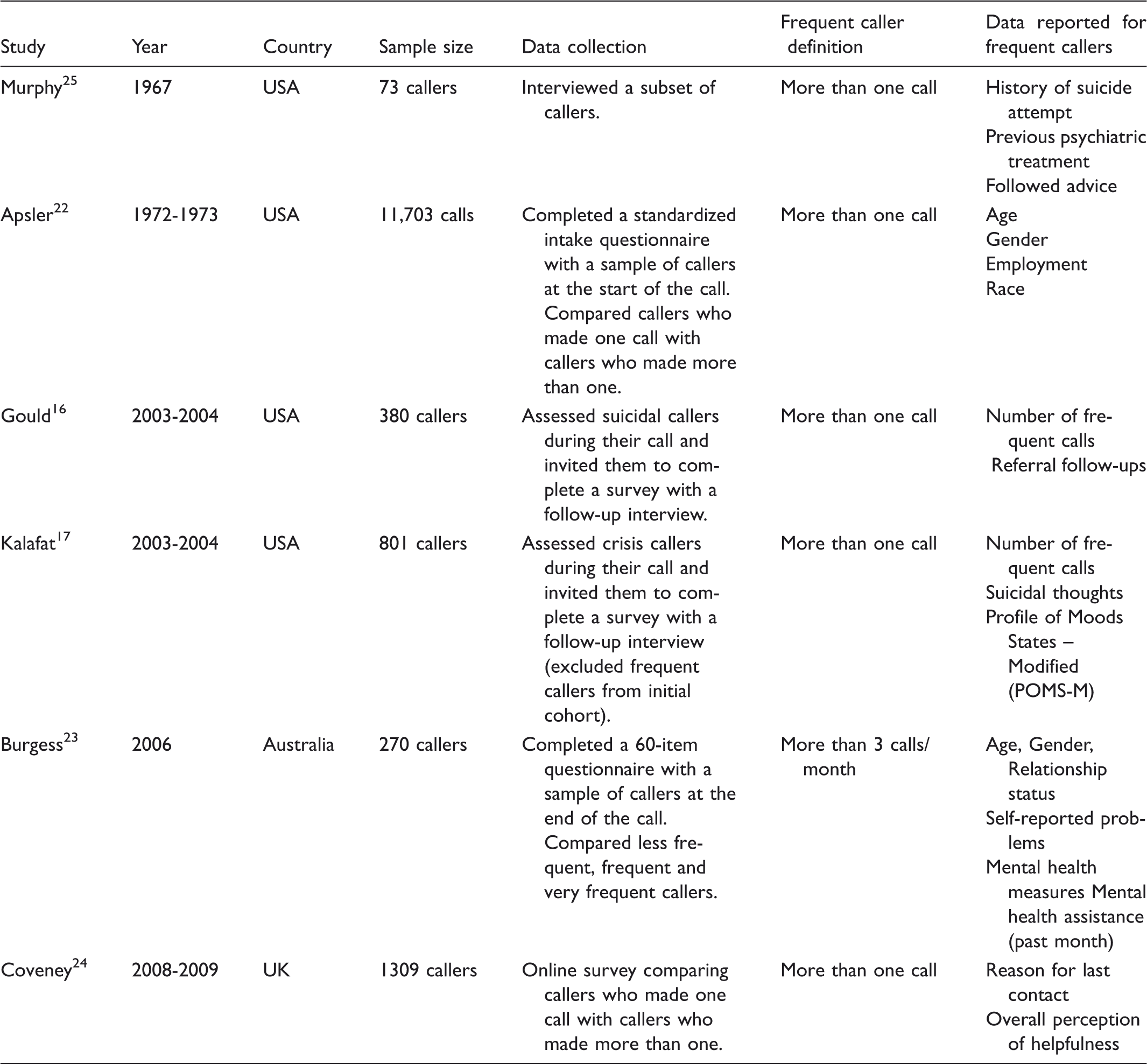
Survey studies included in the review.
Call record audit studies included in the review.

The intervention studies all took place in North America; two in Canada20,21 and one in the USA. 19 All were restricted by a small sample size and only one study used a randomised controlled design. Brunet et al. 20 was the only intervention study to provide a specific definition of frequent callers.
A range of interview techniques were used in the studies that surveyed callers, with most completing one-off surveys.22–25 Nearly all of the survey studies defined frequent callers as making more than one call.16,17,22,24,25 Only the studies by Apsler 22 and Coveney et al. 24 surveyed more than 1000 callers. All studies analysed a sub-sample of callers to crisis helplines. The studies by Apsler, 22 Burgess et al. 23 and Coveney et al. 24 compared frequent callers with other callers.
The majority of the call record audit studies were completed before 1980 in North America.13,18,27,29,30,32,33,35 Only the studies by Ingram et al. 28 and Watson et al. 34 were completed after 2000. These had the largest sample sizes of the audit studies. There was greater variation in the definition of frequent callers for the audit studies compared to the survey and intervention studies. More than half of the audit studies presented some comparison of frequent callers with other callers.27–32
Of all the studies, nine defined frequent callers as callers who made more than one call to a crisis helpline.13,16–18,22,24,25,28,31,33,34 Other studies defined frequent callers as callers who made a specific number of calls over a period of time. These definitions ranged from three calls over one month, 23 10 calls over one, 20 six 26 or eight 30 months or 19 calls over two years. 27 The study by Johnson and Barry 29 discussed the need for a definition of frequent callers to include not only the number of calls but also the pattern of calls and follow-up policy of the crisis helpline. Their definition separated callers into six types of calling patterns based on the number of calls made, the time period over which the calls occurred and whether each call was related to the same problem or multiple problems. 29 There were four studies that did not provide a specific definition of frequent callers but referred to them as a subgroup of callers who made multiple calls.19,21,32,35
Calls and call frequency in studies reporting on a representative sample.
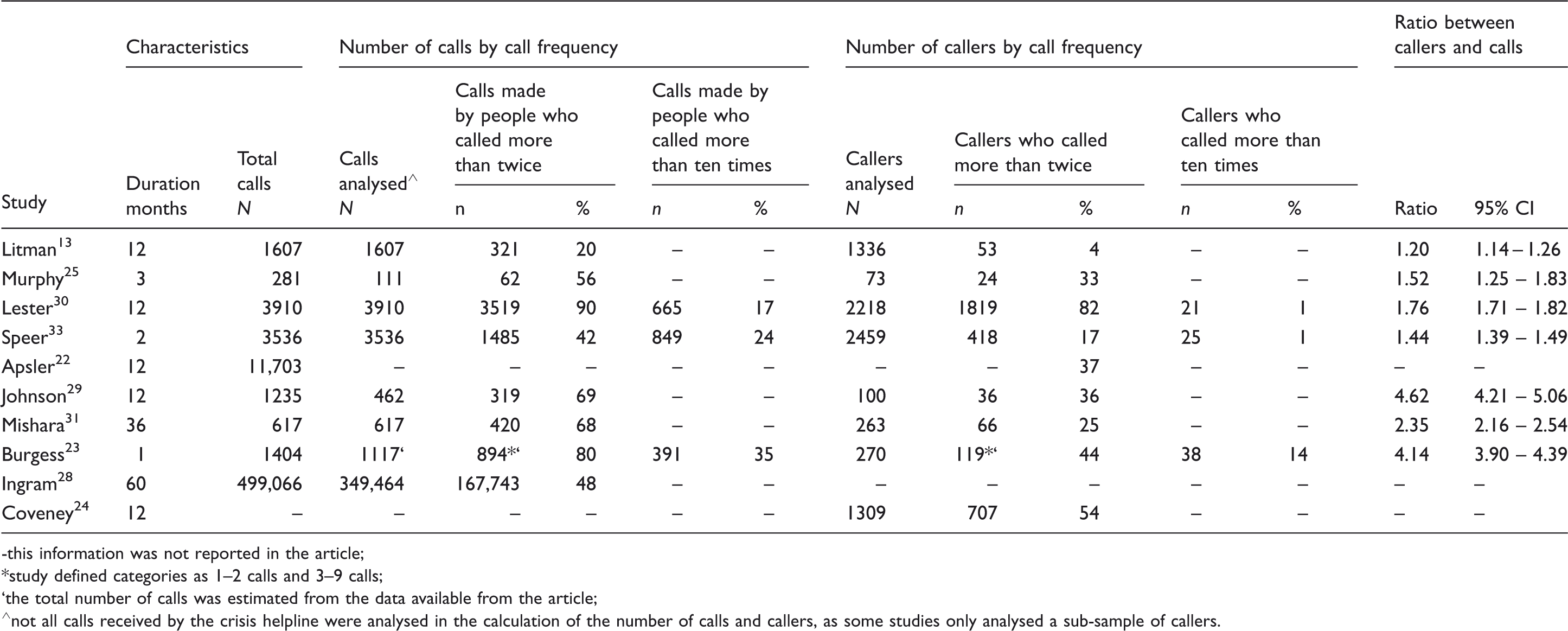
-this information was not reported in the article;
study defined categories as 1–2 calls and 3–9 calls;
the total number of calls was estimated from the data available from the article;
not all calls received by the crisis helpline were analysed in the calculation of the number of calls and callers, as some studies only analysed a sub-sample of callers.
The ratio between callers and calls in all of the studies was more than one call per caller. In the 2006 study by Burgess et al. 23 completed in Australia, the ratio between callers and calls was one caller to 4.14 calls (95% CI 3.90 - 4.39) for one month of follow-up. Due to the wide variation in the methods, sample size and follow-up time period the ratio calculated for these studies cannot be compared. The call ratio could not be calculated for three of the studies as insufficient information of the caller population was provided.22,24,28
The different study designs, sampling strategies, definitions of frequent callers and methods made it difficult to combine the data or to undertake a formal meta-analysis of the intervention studies. However, the studies addressed similar problems relating to frequent callers allowing the findings to be presented around common themes.
Characteristics of frequent callers
Seven studies reported on the demographic characteristics of frequent callers.22,23,26–28,30,32 Of these studies, five compared frequent callers with other callers23,27,28,30,32 of which three reported on a representative sample.23,28,30 Based on the findings of these studies, frequent callers were more likely to be male23,27,28,32 and unmarried.23,26,27,32 It is unclear whether frequent callers differed from other callers in terms of age,22,23,26–28,30,32 ethnicity22,30,32 or employment status22,32 as few studies reported on these characteristics and there were inconsistent findings.
Frequent callers contacted crisis helplines because they were seeking social support,23,24,26,34 had mental health concerns,24,28 and/or experienced a physical illness. 23 Mental health concerns were identified in three studies as the main reason for contact from frequent callers.24,26,28 However, whether these problems were more commonly experienced by frequent callers compared to other callers is unknown.22,24,30
In the five studies reporting on suicidal behaviour, at least half of frequent callers were identified as having a history of suicidal behaviour.25–27,30,32 Frequent callers were more likely to have a history of suicidal behaviour than other callers in only three studies.17,26,27 The severity of suicidal behaviour was higher for frequent callers compared to other callers in the studies by Greer 27 and Sawyer and Jameton. 32
Frequent callers experienced mental health problems that included depression,17,26 panic attacks, 23 confusion and overall distress, 17 and personality disorder problems. 18 Frequent callers were also identified in some studies as having a diagnosis of schizophrenia, 32 possible psychosis, 18 or social and simple phobias. 23 These studies did not use validated measurements. The use of alcohol and drugs by frequent callers was unknown as only the studies by Greer 27 and Sawyer and Jameton 32 found an association, but were completed in small samples in the 1970s. The study by Burgess et al. 23 found frequent callers in Australia in 2006 were less likely to drink alcohol than other callers.
Using validated measurements, frequent callers in the study by Burgess et al. 23 had significantly higher anxiety scores on the Goldberg Anxiety Scale (GAS). However, there was no difference between frequent and other callers on the Goldberg Depression Scale (GDS). 23 Using the Profile of Mood States (POMS) scale, the study by Kalafat et al. 17 found that frequent callers experienced hopelessness and were more anxious compared to other callers. The study by Mishara and Daigle 31 found frequent callers were less likely to have decreases in depression scores over time.
Four studies found that frequent callers were seeking help from several mental health professionals, with many already undergoing formal treatment.18,23,25,32 Up to 85% of frequent callers in the study by Murphy et al. 25 had a history of previous psychiatric treatment. However, in the study by Sawyer and Jameton 32 there were some frequent callers (11%) who only used crisis helplines for support and reported no contact with other mental health services.
The duration of calls made by frequent callers were found in the studies by Greer 27 and Ingram et al. 28 to be shorter than the calls made by other callers. Contracts for follow-up and referrals were often arranged by crisis helplines to ensure further support for frequent callers.28,31 It is unknown whether these contracts were more likely to be prepared with frequent callers compared to other callers. However, it has been estimated that 16–50% of frequent callers follow through with the advice provided by the crisis helpline.16,25 Reductions in the level of urgency during crisis calls were less likely to be seen with frequent callers compared to other callers in the study by Mishara et al. 31
The study by Apsler 22 explicitly made the assumption that frequent callers found crisis helplines helpful because they continued to call. This assumption was supported by the findings of the study by Coveney et al. 24 that measured frequent caller’s overall perception of helpfulness. This study found that frequent callers gave an average score of eight out of ten for helpfulness. 24
Impact of frequent callers on helplines
The studies in the present review did not formally measure the impact of frequent callers on crisis helplines. However, some studies commented on the frequency, nature and appropriateness of calls made by frequent callers as being problematic for crisis helplines.13,18,19,27,28,30,32,34,35 Frequent callers were described as time-wasters who took up a significant amount of time for crisis helplines, limiting the amount of time available for other callers.13,17,18,29,33,34 They were seen to contact crisis helplines continuously with recurring problems, without appearing to make discernable positive changes over time.18,27,28,35 In responding to frequent callers, crisis helpline workers were described as developing feelings of frustration and resentment 27 and experiencing an overall emotional drain. 32 These feelings have been associated with crisis helpline workers thinking of themselves as ineffective counsellors.27,28 One study also described frequent callers being treated differently to other callers as a result of these feelings. 27
Managing frequent callers
Three intervention studies were identified in the review (Table 1). The study by Barmann 19 tested different responses to frequent callers. Fourteen frequent callers were identified from call records and seven were randomly assigned to the intervention. A counsellor was assigned to each caller with a limit on the amount of calling time they were permitted each week. If a crisis was experienced, callers were allowed to call at any time; however they were reminded of these restrictions. The mean number of calls for the intervention group reduced from 24 to 11 calls over a nine week period compared to 24 to 21 calls in the control group. 19
The study by Hall and Schlosar 21 limited frequent callers to a maximum of two calls per day for 15 minutes per call with no contact allowed between midnight and 08:00. Changes in suicide risk before and after the intervention were used to measure improvement, and a minor reduction in the suicidal behaviour of frequent callers was observed. The number of hours spent on the telephone by frequent callers reduced from 172 hours before the intervention to 82 hours five months after the intervention. 21
The study by Brunet et al. 20 implemented a 6-month written correspondence intervention with 22 frequent callers. Callers were assigned a counsellor with whom they started written correspondence. No limitations were made on the number of calls they could make to the crisis helpline. Only 23% (n = 5) of the frequent callers, all female, completed the trial. 20 Before the intervention the five frequent callers took up a mean total of 541 min over a three-month period compared to three months after the intervention where the mean total was 261 min. 20
Based on the findings in the survey and audit studies, suggested techniques for responding to frequent callers included: using a directive and rigid management technique,32,33 discouraging the caller from contacting the service, 30 limiting the call duration allowed,30,32 implementing face to face contact, 32 the service initiating contact with the caller instead of waiting for callers to contact the service, 32 providing short term anxiety and depression treatment programmes by telephone, 23 and creating a specific management plan for each frequent caller. 30
Discussion
The present systematic review found that the research into frequent callers to crisis helplines is limited and of highly variable quality. Frequent callers were more likely to be male and unmarried. There were no reported differences between frequent callers and other callers with regard to age, employment, ethnicity, mental health conditions and suicidality. No study reported data on the impact of frequent callers on crisis helpline staff. Responses to frequent callers could include limiting the number and duration of calls allowed, and/or assigning a specific counsellor. These responses were shown in three intervention studies to reduce the number of calls made by frequent callers.
The strength of this review is that we have conducted an extensive search of the literature and have synthesised the findings according to themes. We have documented the research techniques utilised by studies investigating frequent callers to crisis helplines and provided an analysis of frequent caller characteristics. Our review also provides a summary of the interventions for frequent callers and identifies areas for further research. The limitations of the review are that there are various definitional and methodological limitations with the studies included in it. The review includes studies from over 40 years ago when telephone access was limited, and therefore the characteristics of frequent callers may have subsequently changed.
A range of terms were used in the studies to refer to callers who made multiple calls to crisis helplines. Most of these terms referred to callers who made more than one call. However, it emerged that crisis helplines are more concerned about the callers who may be using the service inappropriately, rather than just callers who made multiple calls. The definition of calling more than once appeared to be used as a convenience definition to try and identify callers who may be using the service inappropriately. Crisis helplines are interested in understanding those who may call inappropriately so that they can respond to them more effectively.
In order to understand the callers who may be calling inappropriately, an improved definition of frequent callers is needed. Such a definition cannot simply be more than one call to crisis helplines, as one would expect people to commonly make a follow-up call after their initial crisis call. As suggested by Johnson and Barry 29 the definition needs to extend beyond the number of calls made to consider the length, nature, appropriateness and the period of time over which the calls are made. Having a definition that considers more than the number of calls made will assist crisis helplines in identifying the frequent callers in their caller population who may require a different response.
For crisis helplines to respond effectively to frequent callers they also need to understand the impact that frequent callers have on crisis helpline staff and how frequent callers differ from other callers in personal characteristics and mental health. In order to achieve this future research needs to include representative samples and validated measures. Crisis helplines could also explore a response that includes collaboration with external mental health professionals. This could be through referrals to mental health professionals or running telephone-based cognitive behavioural therapy programmes.
In conclusion, most callers to crisis helplines make more than one call. Future studies need a definition of frequent callers that considers more than the number of calls made. To understand how frequent callers affect crisis helplines and differ from other callers, robust study design methods using larger sample sizes and validated measurements are required. Once these differences are understood, crisis helplines will be able to respond appropriately to frequent callers.
Footnotes
Acknowledgements
We are grateful for feedback and support from by the staff at the Lifeline Foundation, particularly Mr Alan Woodward. The research was supported by the Lifeline Foundation with funding from Servier Australia. Miss Middleton is the holder of a National Health and Medical Research Council PhD scholarship, and an Ian Scott PhD scholarship awarded by Australian Rotary Health.