
Abstract
In the Western context of delayed motherhood and declining fertility, an array of fertility enhancements have emerged. While bioethical debates and literature on the technological prowess of these enhancements proliferate, it is useful to explore the lived experience of women undergoing them. This article uses Tabitha Moses’ artwork Investment, a series of embroidered hospital gowns, as a vehicle to explore lived experience of women engaging with fertility enhancements, including in vitro fertilisation. This analysis challenges dominant biomedical and corporate discourses framing fertility enhancements as benign. Using constructs of patriarchy, biopower, biopolitics (Foucault), and technobiopower (Haraway), we identify how power over women’s bodies is extended through fertility enhancements. Haraway’s notion of figuration supports the analysis. Understood as a tropic melding of semiotic and material, the figuration of The Infertile Woman offers a way to explore discursive operations of power and amid them the creation of a new form of reproductive labour.
Introduction
An Overview of Fertility Enhancements
Estimates show that worldwide, 15% of couples of reproductive age experience infertility, and its prevalence is increasing (Sun et al., 2019). Introduced in the 1970s, in vitro fertilisation (IVF) offered cascading possibilities for fertility enhancements, including embryo and sperm donation, surrogacy, and sophisticated genetic testing (Leeton, 2004; Suneeta et al., 2012). Contemporary IVF practices are supported by a range of invasive procedures and technologies including injected medication to stimulate egg release, egg harvesting using transvaginal needle aspiration, cryopreservation of eggs and embryos, assisted fertilisation by injecting sperm directly into an egg, and pre-implantation genetic testing to allow identification and selective transfer of embryos with specific chromosomes (Niederberger et al., 2018).
Biomedical and corporate discourses dominate social understandings of IVF success, normalising IVF as a reliable option to achieve pregnancy later in life. For example, Fauser (2019) explains:
Today, 40 years after its heavily criticised clinical introduction, IVF is available as a successful treatment for infertility almost all over the world. Over 8 million IVF children have been born, and over 2.5 million cycles are performed every year, resulting in over 500,000 deliveries annually. There is much to be proud of in such distinct achievements. (p. 133)
While IVF has led to the birth of around five million children globally, success rates are not so promising for women over 40 years of age. Data from the United States describe that the estimated percentage of egg retrievals that result in a live birth depends on the age of the woman, and is 55% (less than 35 years), 42% (35–37 years), 27% (38–40 years), 13% (41–42 years), and 4% (43 years or older) (Centers for Disease Control and Prevention (CDC), 2021). These rates are even less promising when the definition of live birth is considered as: ‘The complete expulsion or extraction from a woman of a product of fertilization, after 22 completed weeks of gestational age ; which after such separation, breathes or shows any other evidence of life’ (Zegers-Hochschild et al., 2017: 1795). Despite contentious outcomes, the uptake of fertility enhancements is extensive, and achievements are praised. Corporate discourses expound IVF as an answer to infertility without always communicating the diminishing returns for older women. As an example, an Australian organisation floated on the Australian stock exchange claims they ‘help you achieve a family when you are ready, no matter what your life stage’ (Monash IVF Group, 2023).
Biomedical discourses are responsible for the social production of infertility as a disease: North American couples describe their confrontation with the medical definitions of abnormality that frame their engagement with IVF treatment (Becker and Nachtigall, 2008). Women engaging in IVF bear the brunt of reproductive technology’s failures:
IVF and its cognate technologies disaggregate motherhood into an array of maternal agents, whose contribution to any given child is partial and contestable, potentially at least. The oocyte economy divides and redistributes raw fertility, renders it storable, portable, transactable, a capacity that can be circulated and leveraged. (Waldby and Cooper, 2008: 192)
British women described the costs as they put their life ‘on hold’, while relationships become strained due to emotional and financial pressures (Phillips et al., 2014).
Art as a Vehicle for Discursive Analysis
In collaboration with two other women with lived experience of fertility enhancement, English artist Tabitha Moses (2014) created the artwork series Investment, offering a glimpse into the usually very private experience of infertility and its treatments. The visual arts have long provided a vehicle to uncover and critique social institutions, conventions, and relations of power (Harrington, 2004). Art also offers an opportunity to address underlying social assumptions and biases (Knight, 2006). Taking Investment as a focal point of analysis, the aim of this article is to explore Moses’ depictions of the lived experience of infertility for three British women, and to contribute to a critical dialogue about contemporary fertility enhancements.
We approach the organisation of this article as a viewer might experience an artwork. We start by appreciating the way the women’s experiences of fertility enhancement are documented by embroidery as medium, photographic portraits as performance, the hospital gown as canvas, and exhibition notes as narrative. Next, drawing on critical social theory, we seek greater depth of understanding through a symbolic reading that makes meaning of the artwork in relation to our social world. The theories of biopower (Foucault, [1976] 1990), biopolitics (Foucault, [1978–1979] 2008) and technobiopower (Haraway, 1997) provide a useful critical lens for this discussion. Haraway’s idea of figuration supports our identification and analysis of The Infertile Woman as a discursive trope in our interpretations of Investment. We analyse how The Infertile Woman is produced within the context of discriminatory gendered social relations of power, and how the figuration participates in concentrating and extending these power relations through advances in technoscience. In doing so, we flag the limitations of universalising white, middle-class women’s experiences of infertility. The use of The Infertile Woman as a discursive trope may suggest an emotional and physical uniformity that erases the diversity of women’s IVF experiences internationally, and the many facets of women’s being (Healy, 2023). Nevertheless, The Infertile Woman supports a discussion of how fertility enhancements may operate within the social, and how they have given rise to a new form of reproductive labour.
Investment: The Lived Experience of Infertility Enhancements
Investment consists of a hand embroidered hospital gown and a short explanatory narrative for each woman, exhibited alongside portraits of two of the women wearing their gowns (Figures 1 to 6, reprinted with permission of photographer Jon Barraclough). The layers of this work, including the embroidery on, and portraits in their hospital gowns, offer a glimpse into the women’s lived experiences.

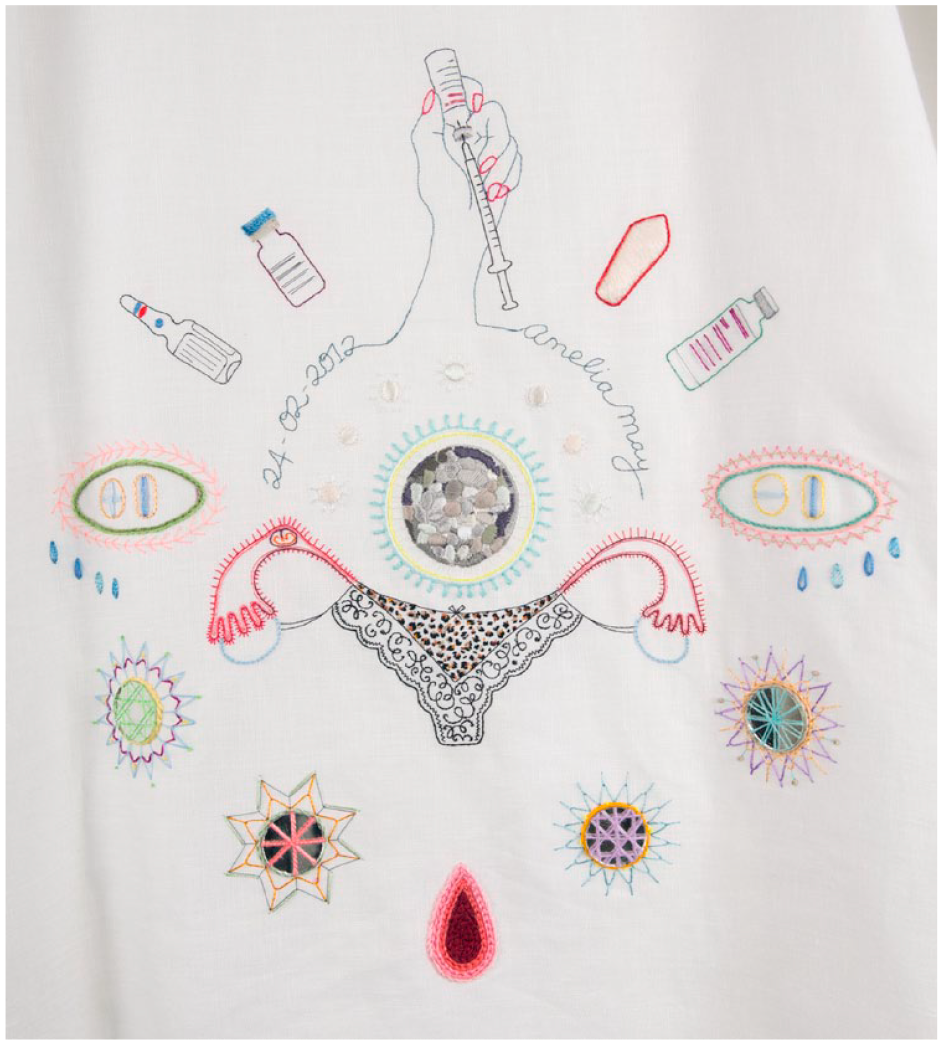
Tabitha’s gown ‘includes images of a mature egg, sperm, pregnancy test results, vials of drugs, a syringe, a thermometer, four embryos from unsuccessful IVF [in vitro fertilisation] cycles, blood, fertility figurines, a baby figure, an acupuncture body map and tears’ (Jackson, 2015).
Melanie’s gown ‘includes images of a blastocyst (a five-day-old embryo), symbols of seven frozen embryos, vials of drugs, a syringe, a progesterone pessary, an ectopic pregnancy, blood, inflamed fallopian tubes, pregnancy test results and tears’ (Jackson, 2015).
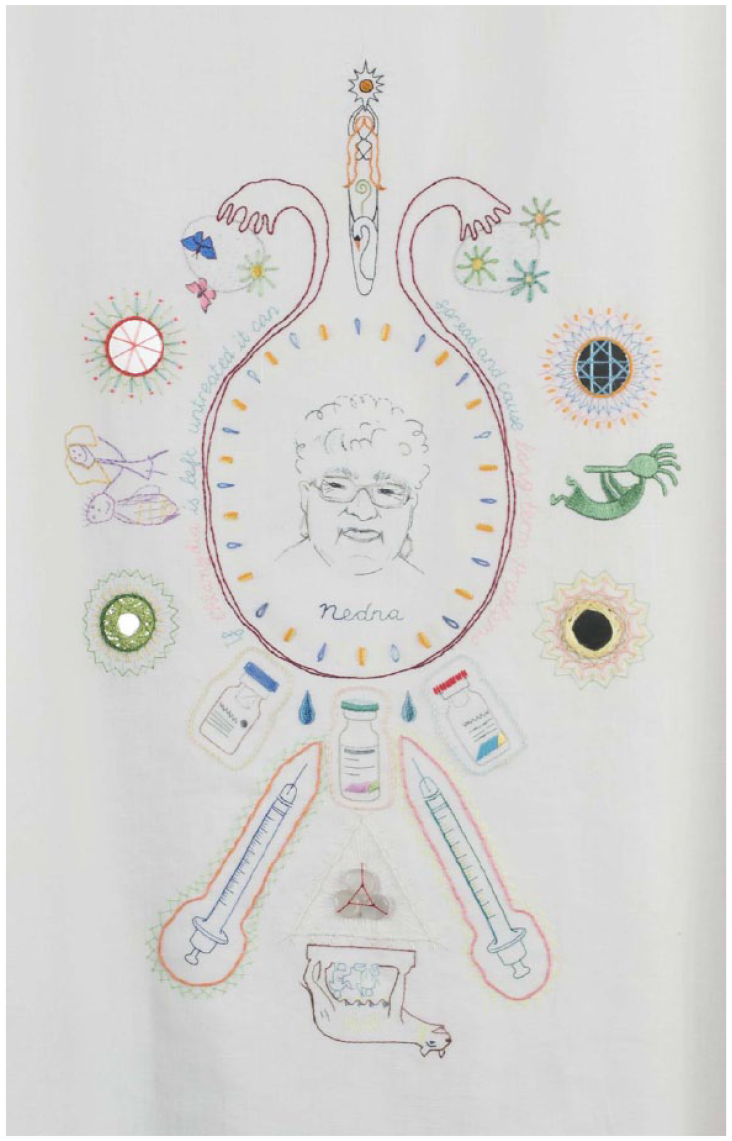
Emma’s gown ‘includes images of Emma’s grandmother, fallopian tubes, ovaries, symbols of four frozen embryos, Kokopelli (a god of fertility and music), a child’s drawing of ‘Emma and her baby’, a she-wolf suckling Romulus and Remus (symbol of Rome), a fertility pendant, vials of drugs, syringes and tears’ (Jackson, 2015).

Tabitha.

Melanie.

Emma’s empty gown.
Embroidery as Silent Testimony
Embroidery is a traditional, gendered art form. Textile art is historically marginalised, and devalued, and women artists excluded from the androcentric world of fine art (Michna, 2020). Embroidery as a communication of ontological existence is understudied, trivialised, and culturally constructed as feminine (Pérez-Bustos, 2017). With the expression of women’s experiences historically constrained to creating everyday functional and decorative objects, understanding the history of embroidery gives access to the history of women (Parker, 2010). This constructed knowledge arises from feminist methods of cognition. Described by Mary Daly as ‘spinning’, women’s knowledge is first gained through a critical grasp of permanent androcentric truths, which are disassembled, then reconstructed into a dynamic gynocentric understanding of the world, ‘intertwined with threads of reality’ (Michna, 2020: 180). As a piece of contemporary feminist art, Moses’ use of embroidery with the hospital gown as canvas is both critical and therapeutic. Needlework in this feminist context draws on an artist’s memories and emotions as biographical, subversive and to some degree, healing (Michna, 2020).
Hand-stitched embroidery requires precise and meticulous labour. The detailed stitching that comprises Investment stands as a material complement to the precision required of women to monitor their bodies and enact procedures. The title Investment has multiple possible meanings. While most obviously suggesting financial investment, the embroidered stories also reveal emotional investment. Emotion is threaded into the gowns through, for example, the embroidery of tears. Mason (2017) describes embroidery as a powerful form of expression, where ‘emotion is embedded . . . stitch speaks for the body and acts as a carrier for emotion’ in an act of ‘silent testimony’ (p. 43).
Needles, syringes, and vials stitched on each gown remind the audience of the daily hormone injections that create heightened and dysregulated emotion. The testimonies also suggest other embodied investments. The disruption of sexuality is insinuated by a syringe stitched in the shape of a phallus piercing Tabitha’s womb (Figure 1).
Melanie’s womb is represented by her ‘lucky’ leopard skin panties, connected to her fallopian tubes and ovaries (Figure 2), perhaps as a way of reclaiming sensuality in an otherwise medicalised conception.
Emma points to the importance of blood lineage with a portrait of her grandmother Nedna stitched in the centre of her gown. The she-wolf suckling Romulus and Remus also suggests the importance of blood lineage and these women’s need for salvation with extrafamilial support (Figure 3).
Requiring dutiful performance of rituals and conscientious monitoring, fertility enhancements have a religious character. The baby Jesus embroidered on Tabitha’s gown suggests an immaculate conception. Donning their gowns for the portraits (Figures 4 and 5), Tabitha and Melanie can be seen as quite literally, ‘in vestments’, where vestments are religious garments, and the right to don them a sacred privilege (Hwang, 2016). In the exhibition notes, Moorhead (2014, December 13) describes:
Two rounds of IVF ended without a pregnancy – [and Tabitha] began to realise what desperation meant. As well as using all the help medical science could offer, she found herself gravitating towards alternative therapies, folklore and superstitions: she had acupuncture, massages and hypnotherapy, and each evening she’d light a candle surrounded by a kind of shrine with a Ghanaian fertility figurine and a baby Jesus figure from a Christmas crib. ‘I’m not normally superstitious, but it just felt as though anything was worth trying’.
Tabitha, Melanie and Emma’s gowns each feature fertility figures. Their silent testimonies speak to the spiritual aspect of their experiences and an appeal to the divine that melds mysticism with technoscience (see Figures 1 to 3).
Portraits as Performance
In the photographic portraits, Tabitha and Melanie wear their gowns in deliberate poses (Figures 4 and 5). Despite being in the same clinic room, they are photographed alone. In Tabitha’s portrait, her head tilts off to one side with a solemn downward gaze. Her arms hang limply at her sides. In Melanie’s portrait, her facial expression is pained. On her embroidered gown, Melanie’s hand with pink nail polish actively draws up an injection; perhaps suggesting her agency. In contrast, in her photographed portrait, Melanie’s hands (with nails painted with the same pink polish) passively cup her flat abdomen, as if pregnant only with her story.
Emma is missing from the portrait series. She was unable to attend the photoshoot, being hospitalised to treat a complication associated with her fertility procedure. Her gown hangs empty from a hanger (Figure 6). Grief permeates the portraits.
Hospital Gowns as Canvas
The artists use the open-backed hospital gown, an icon of Western medicine, as a canvas. Hospital gowns are made of thin material that offers minimal covering and unencumbered access to the body. Research positions the gown as provoking vulnerability. Stripped of clothing and dressed in only a hospital gown, one loses identity and embodies the sick role, surrendering control of the body to clinical experts (Cogan et al., 2019). Morton et al. (2020) question the hegemony of the gown as a clinical necessity, describing patient experiences of bodily exposure, cold, discomfort, and embarrassment.
By using the hospital gown as canvas, Investment signals the experience of vulnerability, humiliation, and a loss of control. While appreciative of access to technology, Australian women undergoing fertility enhancements have felt:
reduced to being a series of body parts, subjected to technical and dehumanising procedures. They described the treatments as ‘gruelling’, ‘stressful’, ‘damaging’, ‘humiliating’ and ‘destructive’. They discussed feelings of isolation, and they felt their interactions with . . . medical personnel were often impersonal and sometimes distressing. (Rayner et al., 2009: 52)
Exhibition Narratives as Testimony of Loss
Tabitha’s narrative explains that she underwent two cycles of IVF before using an egg donor for an embryo transfer, resulting in the birth of her daughter. When trying for a second child, the next embryo transfer ended in miscarriage. Melanie’s first cycle of IVF resulted in pregnancy and birth of her daughter, but two subsequent attempts at embryo transfer were not successful. Emma became pregnant with an embryo transfer and gave birth to her daughter. However, she lost her healthy fallopian tube in the process of oocyte retrieval; it was clipped and sealed, resulting in an infection. While grief and loss dominate Investment, Tabitha, Melanie and Emma became pregnant and each gave birth to a healthy baby. This demonstrates the tension between joy and pain for many women undergoing IVF. Pain was reported as central to Israeli-Jewish women’s experiences of IVF, who chose to either silence this sensation, so it did not impede the goal of childbirth, or they directed their attention to their pain to define their own body boundaries and enable an active negotiation with medical professionals (Ha’elyon and Gross, 2011). The cultural norms that compelled Portuguese women to seek motherhood through IVF created a moral framework in which pain and complications were normalised and accepted (Silva and Machado, 2010).
While IVF experiences are nuanced, complex and context-specific, with successes that may bring a much wished-for child, Tabitha, Melanie and Emma have chosen to communicate their pain and loss in Investment. These are, perhaps, the experiences that are routinely glossed over, with no means for socially acceptable expression.
Subjugation: Biopower, Biopolitics, and Technobiopower
Fertility and Reproductive Labour
While the stories shared by Tabitha, Melanie and Emma highlight their multi-faceted investment in their quest for a child, globally, a new form of reproductive labour has emerged from fertility enhancements. While Marxist economic analysis sees productive labour creating value through production of saleable goods that increase a society’s wealth (Smith, 1974), reproductive labour refers to the unpaid work that reproduces the labour force. This includes not only the production of children, but also the domestic labour of childrearing that ensures children become productive citizens. Despite requiring more women to join the workforce, neoliberalism has shifted the weight of responsibility for reproductive labour to families, at the same time marketising domestic work by creating a need to outsource childcare and housework (Briggs, 2018). Feminist theory draws attention to women’s dual subjugation to productive and reproductive labour; for example, Adkins and Dever show how, ‘despite emancipatory promise, the commodification of domestic and caregiving labour has worked paradoxically. Instead of achieving equality in economic terms, women continue to be pressed to do more for less’ (Einboden, 2019: 437). With increasing options to address infertility, reproductive labour has been transferred to poor and/or migrant women, through cross-border egg donation, and surrogacy (Gupta, 2018; Nahman, 2016; Weis, 2021).
Fertility, Biopower and Biopolitics
Women are socialised to engage in this form of reproductive labour silently, keeping their efforts hidden privately away. Management of women’s reproduction sits within a logic of patriarchy. While women do not relinquish agency, within this new form of reproductive labour, imprints of dominant social relations of power can be traced using the ideas of Foucault. Biopower evolved following the transition from monarchical to state governance, when the mechanisms of power shifted from the threat of death to the management of life through a range of techniques that both subjugated bodies and controlled populations (Foucault, [1976] 1990: 144). Foucault further argued the integration of the disciplinary elements of biopower with a ‘biopolitics of the population’; a political rationality that administered supervision, interventions, and regulatory controls to manage conception, birth, health, and longevity. With the body conceptualised as a unit of population, new metrics of a population’s birth and death rates, diseases, pauperism, and deviancy were collected. These arbitrary classifications made visible those elements open to government intervention to increase productivity: the docile bodies produced through biopower, when optimised through biopolitics, now provide the basis for capitalist labour (Foucault, [1977–1978] 2008, [1976] 1990).
Surveillance is a key technique of biopolitical relations and a mechanism of social control, which operates covertly through subjugation, an internalised power relation. The subject ‘assumes responsibility for the constraints of power; he makes them play spontaneously upon himself’ (Foucault, [1975] 1995: 202–203). Through covert and widely accepted operations, biopower has become an insidious, efficient, and effective form of power. More intense forms of surveillance of bodies, made possible by advances in technoscience, extend, and concentrate biopower into technobiopower (Haraway, 1997: 50). Australian scholar Lupton argues that this technological surveillance is persuasive in discourses of risk management, personal goal attainment, and reproductive responsibility (Hamper, 2020).
Figuration as a Critical Theoretical Device
Haraway (1997) proposes how, in the context of technobiopower, our bodies combine with other bodies and worldly elements, including discursive aspects such as ideologies and images. This integration of the material and the semiotic form new ways of being through hybrid bodies, or figurations. Analysis of figurations offers a way to identify operations of technobiopower (Haraway, 1997). Within healthcare discourses and practices, discourses of biology and nature are used to legitimise figurations, focusing our gaze onto their materiality and away from their discursive aspects and the relations of power that render them subjects (Einboden et al., 2023). Taking a step back supports analysis of the discursive elements of figurations, resisting naturalisms and appreciating how social relations of power operate and obscure the material bodies from our view (Einboden, 2017; Einboden et al., 2023).
Our application of a critical theoretical lens using biopower, biopolitics, and technobiopower, supported the identification of the figuration of The Infertile Woman in our interpretations of Investment. This figuration supports analysis by considering how dominant gendered social relations of power and control over women’s bodies are concentrated and extended through advances in technoscience. The Infertile Woman disrupts the discourses of fertility enhancements as benign support for women and offers a critical perspective on the operations of power within this new form of reproductive labour.
The Infertile Woman: Making the Social Order Visible
A Gendered Culture of Surveillance and Body Management
The idea that engaging in fertility enhancements is an autonomous choice oversimplifies the social contexts in which women make choices, and highlights agency in a way that subverts attention away from covert relations of power. The body is not simply a passive surface upon which meanings are inscribed. Gender is learned, performed, and embodied, with the ‘self’ constituted through reiterations of gendered practices. While women are active agents in the reproduction of social norms, they are also creative and transformative, adjusting practices to specific situations (Hogan, 2020). Notwithstanding, women have been subjected to long-standing management of their reproductive behaviours and bodies across their lifespan, which are internalised from a young age. Little girls are socialised to embody normative gendered physicality in the way they sit, play, and behave. When menstruation begins, they learn to manage their leaky and out-of-control body (Shildrick, 2015) through vigilant surveillance, hygiene, and sexual abstinence. Pregnant women, with access to such resources, regularly measure and manage their diet, blood pressure, glucose, weight, fundal height, and foetus: their body is in a state of controlled chaos that they are held accountable for (Bønnelycke et al., 2022). After birth, surveillance continues for parenting practices, infant feeding, and development. Women’s post-reproductive years are increasingly managed with hormone supplements to prevent menopause and its symptoms.
Reproductive technologies, and their use of imaging and monitoring, are mediators of bodily experiences that increase the intensity of surveillance over women’s bodies (Bønnelycke et al., 2022). By extension, this increases the intensity of surveillance over women’s lives. These new relations of power, which target women, are ‘productive of, and products of, an intersection of ideologies of science, technology, reproduction and the gendered body’ (Throsby, 2004: 10).
Almost three decades ago, American scholar Carol Stabile (1992) argued that ultrasound technology altered our relations with pregnant bodies. Images dominate the social space while removing the woman from view, encouraging an understanding of the foetus with a separate identity, rights, and needs. The invisibility of the mother strengthened social discourses of maternal altruism, where a child’s needs are separated and prioritised over that of the mother (Stabile, 1992). The focus on a baby in fertility treatments operates similarly, within the ‘visually saturated technoscientific culture of the clinic’ (Haraway, 1997: 11). Investment brings the women and their experiences back into view.
In an interview for The Guardian, Moses draws attention to the constant self-regulation and interventions that she practised daily: ‘[p]eople say, “relax, just forget about it”, but they don’t realise how much trying for a baby dominates your life. You’ve stopped drinking alcohol and caffeine, you’re taking folic acid and monitoring your temperature every morning’ (Moorhead, 2014). Embroidered on each gown are images of thermometers, pregnancy tests, menstrual blood, and tears. Monitoring practices exemplify women’s bodies under intense medical surveillance. For IVF, women must also self-administer hormones that induce multiple oocyte maturation, then undergo imaging studies and blood tests to identify an appropriate moment for ‘retrievals’ (Hwang et al., 2016; Monash IVF Group, 2021). Moses’ gown acquaints the audience with the effects of these interventions. Her embroidered womb is punctured by a syringe. It contains an ovum and sperm, with a positive and negative pregnancy test result, surrounded by tears. A splash of stark red blood, stitched aggressively, breaks through the contained circle of the womb signalling miscarriage.
The Gendered Pathologising of Infertility
Infertility, according to the World Health Organization, ‘is a disease of the reproductive system defined by the failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse’ (Maung, 2019: 43). The diagnosis of ‘infertility’ as a disease offers an example of the preservation of agency in the context of subjugation. A diagnosis of infertility must be sought by a woman to explain her experience of not becoming pregnant (Duvnjak, 2012). Furthermore, infertility is diagnosed within a socio-behavioural context, and through the desire for a child.
Unlike other biological dysfunctions, infertility arises from two bodies (Johnson and Fledderjohann, 2012). Despite an equivalent incidence between men and women (Sternke and Abrahamson, 2015), a lack of attention to, and underreporting of, men’s infertility globally (Agarwal et al., 2015) has led to a focus on interventions for women. The couple has emerged as the site of treatment for men’s infertility, with women undergoing intervention for problems that previously belonged to their partners (Van der Ploeg, 2004: 156). This focus constitutes women’s bodies as the source of inadequacy, in line with dominant discriminatory social ideologies (Franklin, 2013). Thus, while infertility constitutes an ‘abnormal functioning’ of the body (Khetarpal and Singh, 2012: 338), social understandings have shaped the biomedical response, constituting infertility as an abnormal functioning of the woman.
Medical terminology used to describe women’s infertility is revealing. When a woman has challenges conceiving or carrying a pregnancy, her cervix is deemed ‘incompetent’, her uterus and cervical mucous ‘hostile’, and in the case of a ‘blighted ovum’, she is responsible for ruining the products of conception. In contrast, medical terminology used to describe male infertility has a different quality, and men’s body parts are not defined as lacking (Ven der Leun, 2018). Men suffer from ‘erectile dysfunction’, ‘low sperm count,’ or ‘premature ejaculation’, rather than incompetent erections or testicular hostility. Martin (1997) similarly draws on medical texts that marvel at the prolific male reproductive system, compared with the ever-declining female reproductive cycle. Menstruation is framed as a failure of reproduction – an expulsion of the waste and debris of the uterus. The passive ‘shedding’ of a single egg per month is compared with the ‘production’ of hundreds of millions of sperm each day. ‘Far from being produced, as sperm are, [eggs] merely sit on the shelf, slowly degenerating and aging like overstocked inventory’ (Martin, 1997: 86).
The language and focus of medical terminology identify and reproduce dominant relations of power, to exemplify how ‘medical space can coincide with social space . . . traverse it wholly and penetrate it’ (Foucault, 2003: 35). Hidden within biomedical discourses of infertility as pathology, dominant patriarchal relations of power over women are naturalised and extended. Bell (2010) proposes:
Not only does medicalisation participate in the construction of infertility, but it also results in the decontextualisation of that experience. Individualising the experience of infertility, [and] focusing on its treatment rather than its aetiology, ignores the fact that infertility is a social issue, situated in various contexts and shaped by social forces. (p. 635)
Because reproductive technologies exist, these women are compelled to engage with them, upholding normative, gendered social expectations (Vlasenko, 2016). British women described the pressure they felt, both from the media and society, as a social obligation to use the reproductive technologies available to them (Phillips et al., 2014).
Sandelowski (1993) proposed that infertility was rediscovered in response to reproductive technologies (p. 41). Following Donchin (1996), Bell (2010) argues:
The medicalisation of infertility assists in maintaining the norms of family and motherhood. It has redefined and further entrenched the role of motherhood within society by shifting the normative expectations surrounding fertility. Prior to . . . [assistive reproductive technologies], involuntary childlessness was constructed as a disappointing, inevitable act of nature, whereas it is now expected that infertility is something to be overcome. (p. 634)
Reproductive Agency
The Infertile Woman remains responsible for her infertility because it is understood as originating within her reproductive choices: to have sex; to use contraception; to have an abortion; and/or to prioritise a career and delay motherhood. However, women’s power to make choices related to fertility is contextual, existing in an assemblage of social factors (Cooke et al., 2012; Stabile, 2016).
Reproductive agency, while gendered, exists in ways that are shaped and enabled in hierarchical intersections of race, class, and sexuality (Madhok et al., 2013: 2). Figured as having made choices that have implications for her fertility, The Infertile Woman turns scrutiny away from a host of social determinants of fertility and infertility: access to secure housing, education, financial security, and other social resources (Martin, 2021); the power to decide who to have sex with; privilege that supports freedom from infectious diseases; relationship status and sense of safety in that relationship; work stress; exercise regimes; and environmental pollution (Duvnjak, 2012).
This assemblage may infer that women have limited reproductive agency. Indeed, a woman’s agency has been explained as her capacity to alter her self-concept so that she may actively participate in the objectification, naturalisation, and bureaucratisation of the body in some circumstances, while rejecting objectification in others (Cussins, 1998; Thompson, 2005). This point is made not to deny the disciplining and subjugating effects of some fertility enhancements, but to argue that the woman participates as a means to an end. ‘[O]bjectification and agency are co-constitutive . . . she is locally and temporarily reduced to a series of bodily functions and parts, working in a mechanistic way that forge a functional zone of compatibility with the means of medical intervention’ (Cussins, 1998: 191–192).
Similarly, Colombian women experienced their fertility enhancement journey as stages of objectification that generated multiple modes of embodied agency: women learned about their bodies and biological causes of their infertility and used this understanding to reduce their treatment anxieties, and they reconfigured the significance of their pain as purposeful (Shaw, 2021). Furthermore, Canadian women’s active role in decision-making about their IVF, and the difficulties they faced in their journey, empowered them with a new strength and confidence to face future life challenges (Parry, 2005).
In Ecuador, existential anxieties about IVF challenging agency were seen as less problematic. Because one’s existence was described as supported by God, and by other people, IVF was viewed as one more means of support. This was attributed to the cultural context of childlessness that could trigger a rupture in the continuity of the extended family structure. Perceptions about IVF and agency for Ecuadorians who experience life as ‘existentially precarious’ is, therefore, shaped by the greater value that is placed on interdependence and connection rather than individual autonomy (Roberts, 2013).
Systems of power and knowledge production politically constitute bodies, which in turn may reconfigure the relations and effects of power. For example, Palestinian women with husbands imprisoned in Israel gained access to fertility treatments, with their husbands’ sperm smuggled out of Israeli jails in an act of resistance to the occupation of the West Bank (Rexer, 2023).
The Socially Desirable Mother
The Infertile Woman targets women who ‘should’ be procreating but are not. These are women who fit within an ideal of motherhood: those who are married; heterosexual; mature; educated; affluent; and able-bodied. Pregnancy in young women is constituted as risky and irresponsible in Western society. Yet, women are stigmatised if they have not had children by their late reproductive years due to social values and beliefs that normalise motherhood (Suneeta et al., 2012). During the reproductive window in a woman’s life course, bodies and behaviours are, therefore, subject to intervention (Hamper, 2020). The figuration of The Infertile Woman locates these women without children outside of ‘normal’ (Throsby, 2004: 188), rendering them deviant and inadequate. In an American study, childlessness constituted a disruption to the prescribed life course of womanhood (Sternke and Abrahamson, 2015). Furthermore, Italian research explains a woman’s constitution of value within her reproductive work as existing within a binary, imposing redundancy if motherhood is not achieved. What is at stake is not just the loss of biological motherhood, but a loss of social value (Facchin et al., 2021). Unable to biologically do what a woman’s body ‘should’ be able to do in the context of social expectations and biomedical definitions, women seek the help of fertility experts and technologies that offer a ‘cure’, enabling them to fulfil their social responsibility.
Reproductive Exclusion
The Infertile Woman also contributes indirectly to the management of women who ‘should not’ be procreating: traditionally enforced through ideology, but now extended through inequitable access to fertility enhancement. For example, women have been excluded from IVF access due to their single or lesbian status (Millbank, 1997; Storrow, 2012). In this way, medicine participates in upholding the ‘moral regulatory power’ of societal governance, with the line between ‘dangerous’ and ‘docile’ crossed and uncrossed (Steinberg, 2015). Access to fertility enhancements is further limited to women with financial resources, often (although not exclusively) from wealthy countries, and remains inaccessible to most women globally (Rouchou, 2013).
The inclusion of the Ghanaian fertility figurine on Tabitha’s gown (see Figure 1), raises important considerations about privilege. Limited access to fertility enhancements is particularly evident for women of colour, whose fertility is often constituted within discourses of excess. Even in the United States, where fertility enhancements are widely available, women of colour share a disproportionate burden of infertility, yet have more barriers to accessing treatments (Cebert et al., 2020; Kissin et al., 2016).
Individual women’s bodies are affected by subjugation differently, with varying intensity and effects depending on intersecting axes of social position and power (Dolezal and Oikkonen, 2021). In Africa, South Asia and parts of Latin America, high rates of untreated reproductive tract infections lead to avoidable infertility, exposing women to marital breakdown, social exclusion, and physical and emotional abuse. In this context, the largely inaccessible fertility enhancements are proposed as a human right (Inhorn, 2009). Where economic and health resources are scarce, IVF is not only a low priority, but a ‘tacit eugenic view’ that people in low-income nations are not worthy of infertility treatment offers a means for global population control (Inhorn, 2009: 173; Inhorn and Patrizio, 2015: 413).
Reproduction and Neoliberalism
The ‘clinical labour’ of fertility enhancements is born of entanglements between women’s reproductive biographies, the global bioeconomy, and neoliberalist health systems (Perler and Schurr, 2021). In some countries, normalisation of individualised fertility treatments occurs through their inclusion in insurance or state-subsidised fee rebates. However, most subsidies support initial steps of testing to attain a diagnosis of infertility, but fall short of covering the fees of treatment, for example, in Australia (New South Wales Ministry of Health, 2021). Concerns have been raised about potential over-servicing by financially motivated physicians, and considerable diversity in the way fertility experts articulate options (Blakely et al., 2019). Substantial financial investments are associated with each procedure, with each step of fertility enhancement leading to another in what Ertman (2008) describes as ‘exchanging money for parenthood’ or what Haraway (1997) might describe as ‘nature enterprised up’ (p. 301). Williams et al. (2016) draw attention to the code of conduct that guides IVF doctors as employees of publicly listed companies: ‘they must recognise that (their) primary responsibility is to the Company and its shareholders’.
Reproductive Winners and Losers
Within tropes of success, many women experience a hidden burden of repetitive failures. The cumulative impacts of treatment mean women are torn between their emotional exhaustion and the ongoing need to fix their infertility and produce a child (Becker and Nachtigall, 2008). Throsby (2004) argues that ‘[w]here the dominant discourse is technology giving nature a helping hand to produce miracle babies, there is simply no space for any representation of treatment failure other than . . . a lack of persistence or of devastation’ (p. 187). De Lacey (2002) juxtaposes the idea of IVF as an investment versus IVF as a lottery. As an investment, IVF includes calculated risk-taking, and women as diligent workers using their agency to make the best use of their body and resources. As a lottery, IVF is a gamble that pits women’s bodies against the uncertainties of clinical intervention. The chips are public funds, or in many cases, women’s own funds, along with their emotions. The jackpot is the take-home baby.
The Infertile Woman produces two special identities for women who lose. First, The Uncommitted Infertile Woman who waited too long to start fertility interventions, who did not try hard enough, or who gave up too soon. Second, The Desperate Infertile Woman who is a ‘problem gambler’: she has tried for too long or obsessively, even recklessly, frittering away her financial resources in a ‘losing streak’ (De Lacey, 2002). Curiously, all three women in Investment avoided these constitutions of loss – all three successfully had a child. Yet despite their wins, their losses haunt the artwork.
The Indelible Nature of the Infertile Woman
The birth of a child does not necessarily cure infertility, nor do infertility ‘cures’ necessarily result in a child: this lack of closure may exacerbate a couple’s suffering (Sandelowski, 1993: 44). Fertility enhancements promise ‘hope against the odds’ (Peddie and Porter, 2007: 317), or even ‘false hope’ with American and UK research participants describing their expectations as unrealistic at the beginning of treatment (Becker and Nachtigall, 2008; Phillips et al., 2014). Women are enrolled within this hopeful promise with no easy exit points, often not even the birth of a baby (Throsby, 2004). For British couples who had a child using fertility enhancements, planning for a second child was a trigger for identity re-evaluation as couples balanced their emerging identities as parents with their identity as an infertile couple who may have to re-engage with fertility experts (Allan et al., 2021). In their narratives, both Tabitha and Melanie point to the indelible nature of The Infertile Woman: ‘Tabitha and her husband are no longer trying for another child; [. . .] Melanie and her husband are pausing their fertility treatment for now’ (Moses, 2014, exhibition notes).
Fertility identities are tenuous and fluid. In one study, American women did not consider themselves infertile even after multiple unsuccessful treatments/miscarriages, while others who became pregnant remain conflicted, and many continued to identify as ‘an infertile woman who inexplicably carried a baby’ (Johnson and Quinlan, 2017: 383). A researcher in her late thirties described herself as an ‘anticipatory infertile’: she had not tried to become pregnant but assumed infertility would become part of her story given her age (Johnson and Quinlan, 2017). Despite intense reproductive labour to undergo fertility enhancements, women cannot claim their own successes. Figuration as The Infertile Woman persists.
Conclusion
Tabitha Moses’ (2014) Investment reminds us of the power of the visual arts both as a means of intimate individual expression and as a critical tool to disrupt social assumptions, conventions, institutions, and power. Moses’ work offers an opening for critical questions, dialogue and analysis regarding the impacts of technological advances and medicalisation of fertility, the gendered pathologisation of infertility, and the constitution of women as socially desirable/undesirable mothers. Using the figuration of The Infertile Woman as a point of focus and a critical theoretical device, we view Investment as a point of resistance to patriarchal relations of power embedded within the discourses and marketisation of reproductive technologies. By engaging in the complexity and the loss depicted within the art arising from lived experiences, the layers of this analysis reveal the complex structures of technobiopower. This analysis offers a challenge to the dominant biomedical and corporate discourse that reproductive technologies are simply benign help for women to extend their ability to choose when to have children. Amid a promise of freedom from and ability to overcome the limits of women’s bodies through fertility enhancement, the intensification of social relations of power over women and their bodies is made visible. Investment brings our attention to a new form of reproductive labour within the context of fertility enhancements.