
Abstract
This article utilises feminist technoscience studies’ notions of bodily ‘materialisation’ and ‘ontological choreographies’, offering a cyborg feminist account of ‘bioavailability’ as embodied becomings, rather than a fixed ontological state of being. Drawn from 2 years’ ethnographic study in in vitro fertilisation clinics in Spain with migrant women who provided eggs to the cross-border in vitro fertilisation industry, this work explores how global understandings of race and inequalities, clinical practices and women’s own emotional and physical labours collectively produce bioavailability. Through examples from observations and interviews in in vitro fertilisation clinics, we examined women’s embodied stories to understand the ways in which bioavailability becomes. The article demonstrates a novel way in which to think about ‘bioavailability’, a concept which has already been of enormous use to the social sciences since its introduction by Lawrence Cohen. We examine recent configurations of bodily extraction in the reproduction–migration nexus that help us rethink the concept of bioavailability.
Introduction
[T]o be available for the selective disaggregation of one’s cells or tissues and their reincorporation into another body or machine. (Cohen, 2007: 83, emphasis added)
In the understated Barcelona premises of one of the largest networks of private in vitro fertilisation (IVF) clinics in Spain, under the watchful eye of one of the nurses, we met Daniela,
1
a tall, athletic, blonde-haired student originally from Colombia. In the span of 1 year, Daniela underwent ovarian hyperstimulation for the purpose of providing eggs four times, in exchange for 1000 Euros for each egg provision cycle. Each time, she would self-administer hormones daily by injecting them with a needle in her abdomen. This set in motion predictable hormonal processes that resulted in her body’s production of up to 30 oocytes. At the end of a month of doing this, she attended the clinic and underwent an anaesthetised oocyte extraction procedure called ‘aspiration’, involving transvaginal removal of the mature oocytes with a 30-cm-long needle and ultrasound probe. When we asked her how she started to provide eggs, she stated: [One day] I was at the university, exploring what to do with my life [laughs] . . . [this was] one year ago. And I saw a leaflet on the wall saying ‘Do you want to donate eggs?’ And I took one leaflet, but only because I was so curious . . . And I started asking myself if I could do it. And I started talking with my friends, and first I said ‘no no no no’ I am not going to give away my babies [laughs] . . . and then I decided to do it, and began to search on internet and this clinic was like the closest to my house. So I planned to ask if I could do it. And I came here and I asked and I liked it and I did it.
Although she painted it quite simply, the process of becoming an egg provider involves many more layers of embodied and emotional labour as well as socio-technical processes, such as an interview with the clinic, long consent forms, and a post-surgery physical examination before collecting the final portion of the payment. It involves an awareness of one’s racialised desirability in a world structured to prefer certain phenotypes over others, and phenotypic similarity between parent and child; where women learn to want to help other women, especially when it comes to creating an idealised ‘family’. These are some of the ways through which individuals like Daniela subject themselves to being materialised as bioavailable (Barad, 2003; Cussins, 1996; Thompson, 2005) that lead us to ask the following questions.
What does it mean, ‘to be available’? How precisely does bodily bioavailability come into being? In offering a response to these questions, we draw upon 2 years of ethnographic fieldwork with migrant egg providers in Barcelona, Spain. This work was conducted at a time of rising Catalan nationalism, high unemployment and labour precarity for young women, especially migrants, and when Europe was experiencing the highest levels of migration since the 1930s. Meanwhile, Spain provided around 50% of the oocytes in Europe in the latest data survey (Ferraretti et al., 2017; see also Molas and Whittaker, 2022). Far from being external to the study, this socio-political context is part of the fabric of ontologies of becoming bioavailable.
With over 15 million babies born in Europe alone from assisted reproduction (Ferraretti et al., 2017), the significance of these reproductive practices for understandings of ‘the body’ cannot be underestimated and have been studied by many (Almeling, 2011; Holzberg, 2018; Perler and Schurr, 2021; Thompson, 2005). Egg donation now comprises an industry of billions of pounds annually (Nahman, 2016) with 73,927 cycles performed in Europe in 2016 Consortium (EIM) et al., 2017. Meanwhile, in a quantitative demographic study, Pennings et al. (2014) showed that being a migrant was one characteristic that was significantly correlated with becoming an egg donor in Europe. 2 The kinds of gendered labour available to migrant women, and their value to local economies, as well as their experiences of identity and displacement offer a very useful vantage point for seeing both the broader issues that arise in egg donation and the challenges faced by migrant women, such as being subjected to greater amounts of domination/intervention and scrutiny when they are displaced from their country of origin and in medical care (Saharoui, 2020; Pallister-Wilkins, 2018, 2015) as well as the intersectionality of gender, race, nationality and class in migrant health (Viruell-Fuentes et al., 2012). This particular ‘reproscope’ or way of viewing reproduction (Nahman, 2016) is important in and of itself, in terms of how it homes in on the reproduction–migration nexus (Erel et al., 2016). But it also affords a more generalisable novel understanding of bodies as they become bioavailable that exceeds the concept of bioavailability’s previous articulations.
To demonstrate, we begin with a critical overview of bioavailability in the social scientific literature, and then elaborate on our theoretical framework. After a brief account of our methodology, we trace our argument through two main sections: (1) socio-technical becomings and (2) working on oneself. In sum, we are interested in mapping some of the affective, social, biomedical and economic processes and configurations that impinge upon and produce disaggregation of egg cells from migrant women’s bodies that make them bioavailable, to exemplify how bioavailability is not one thing but rather a series of techniques, events and encounters that bring it into being.
Being Bioavailable
In recent work in social studies of donation and assisted reproduction, the concept ‘bioavailability’, which Lawrence Cohen borrowed from pharmacology and introduced into the social sciences, has gained the currency of a term in regular use to refer to people who are relatively ‘disempowered’. In other words, it is used to refer to people whose positioning within biopolitics puts them at the disadvantage of being extractable (Bharadwaj and Glasner, 2009; Nahman, 2016; Payne, 2015; Rudrappa, 2015). Bioavailability has been seen in the work of Bharadwaj and Glasner (2009) as a corrective to ‘biosociality’, where the freedom and liberalism implied in this latter notion is less present in the former. In part, this move echoes Rose’s (2007) critique that ideas such as ‘biological citizenship’ and ‘biosociality’ are Euro-American constructions perhaps only relevant in those contexts. While Rose’s (2007) critique highlights the Eurocentrism of these terms, Schurr (2017), in turn, critiqued Rose’s (2007) argument in the context of assisted reproductive technology (ART), suggesting Rose did not address how ‘the global spread of the bioeconomy affects reproductive consumers and labourers in economic, political and social contexts outside of what he refers to as advanced liberal democracies’ (Schurr, 2017: 4). In one prominent work by sociologists of medicine, ‘bioavailable zones’ is a concept used to refer to the territoriality of this idea of availability (Clarke et al., 2010), in the sense that there are particular political and economic zones globally that are more likely to be zones of bioavailability. Areas such as the Global South, the margins of Europe and the Southern United States are particular ‘bioavailable zones’. Meanwhile, the special issue on medical migrations (Roberts and Scheper-Hughes, 2011) within this journal demonstrated the non-unilinear nature of these zones of bioavailability.
A more active interpretation of bioavailability has been assayed through the concept ‘clinical labour’ (Cooper and Waldby, 2014). ‘Clinical labour’ suggests a ‘new’ model of labour extending out of ‘post-Fordism’ of the 1970s, where women supposedly emerged out of the household and went into the workplace (Cooper and Waldby, 2014). Yet, we reject Fordism as a starting point for analysing economies of extraction. Our redefinition of ‘bioavailability’, instead, centres colonial and racially stratifying histories, which predate Fordism and are integral to present day experiences of ARTs (Vertommen et al., 2022a). In the Global South, for instance, women were always already engaged in clinical work of donating their reproductive services in ways that erased their humanity (Gillespie, 2022). As seen ahead, in this study, migrant women are part of a global majority of women workers whose position in the economy is made precarious by hostile border regimes and unstable economies, resulting in them having to find any means by which to exist. These things also shape their bioavailability. Hence marking the 1970s as a moment of elaborated change for these women would be a partial view that does not encompass historical and ongoing global economic and racial unevenness.
Our contribution to this debate rests, in part, on the question of the political, economic and geographic unevenness of bioavailability. The case of migrants who are already displaced from zones of bioavailability (i.e. poorer countries) and residing in and trying to earn a living in the West (in this case, Spain), complicates even further the question of the ‘reproscapes’ (Inhorn, 2011) of bioavailability. As we show ahead, bioavailability is a set of ontological and socio-technical processes and procedures, as well as emotional responses, that rest on women’s deep understandings of how global economies and racial stratification function. This deepens understandings of the forces that make people prepared to disaggregate a part of their body.
Becoming Bioavailable
In feminist and Science and Technology Studies (STS) theory of bodies, it is established that bodies are corporeal entities that resist Cartesian dualism (Grosz, 1994) and at the same time are processual assemblages (Latour, 2004) that are racialised and gendered, through active discursive, material practices (Butler, 1990; Yang, 2015). They are not discrete entities, but rather embodiment is processual (Blackman, 2010). Meanwhile, in the conventional pharmacological definition of bioavailability, there is the notion that whatever is being absorbed by the body has an active effect. Borrowing from this original scientific manifestation of bioavailability (a feminist STS move that we borrow from Haraway (1997 [1985]) and others), we suggest a perspective that attends to ontologies of bodies’ bioavailability. 3 Like Barad’s (2003) noting of the ontological turn in STS, bioavailability’s materiality comes into being through discursive practices. Furthermore, the processes and accounts detailed ahead suggest what STS scholar Annemarie Mol has argued, that is, if we look in fine detail at the practices of the production of a particular form of embodiment we understand how it is brought into being. In terms of cross-border reproduction in clinics, we outline various processes by which women are ontologically made available, how the carefully staged processes, the emotional negotiations are all choreographed, as feminist STS scholar Charis Thompson showed deftly with respect to IVF in the United States (Thompson, 2005). These steps are crucial to grasping bioavailability itself.
Mol (2002) and Thompson (2005), influenced by the ontological turn in STS and notions of materialisation (Barad, 2003), drew out the importance of exposing the enactments of specific bodily conditions or states (hormones, eggs, veins). In her foundational work on the production of artherosclerosis, Mol shows how this condition affecting lower leg veins is a produced one – its naming, the processes of identifying it and of treating it are all produced, in various micro and macro social and technical processes and encounters. And crucially this type of perspective affords a holistic appreciation of artherosclerosis. Similarly, we outline enactments of egg donation, through clinical strategies and women’s processes of becoming donors, their narratives and bodily strategies that make them bioavailable. In so doing, we show that just as gendered, racialised and maternal/parental bodies are produced through discourses and practices (e.g. ‘ontological choreographies’; Thompson, 2005), so too, egg providers’ bodies are not simply pre-existing available resources, but they become so through the processes we outline. This feminist STS cyborg account denaturalises bioavailability by bringing together a hybrid of theoretical perspectives from feminist political economic theory of labour and value, with (queer) affect and theories of embodiment, which together make a hybrid (cyborg) account of ontologies of bioavailable becoming. This very specific account of the bioavailability of migrant egg providers has broader implications for understanding all bodies that are, or rather, become bioavailable.
We suggest that this ontological, processual, understanding of bioavailability offers a greater opportunity for analysis of the unequal, racialising and colonising dimensions of global fertility chains (Vertommen et al., 2022b). Migrant women become bioavailable as egg providers through an interaction of larger global forces of geographic unevenness, economic processes such as state financial crises and job precarity, racialised commodification of ‘whiteness’ and ‘post-colonial whiteness’ (Lopez 2012), as well as through their being gendered as women and therefore suitable for care and domestic labour, or as migrants perceived as suited to other low waged labour, and through everyday practices such as the ‘emotion work’ of making one’s bodies, time and presence available. These ontologies of becoming bioavailable are woven through the examples we offer in this piece.
Voices and experiences, including clinical and medical processes and ‘reproductive biographies’ (Perler and Schurr, 2021), are centred, as a way of arguing that ontologies of bioavailability are best expressed by those who are being materialised as such. 4 Crucially, women’s bodies are not self-evidently bioavailable. In the context of egg provision, women become bioavailable in a way that is mediated through embodied gendered and racialising socio-technical practices that make it possible for them to become so, in order that their bodily extractions be reincorporated into another’s body. Similar to bodies themselves and the conditions that affect them, bioavailability is both a lived bodily experience and a series of socio-technical processes that produce it (Barad, 2003; Blackman, 2010; Mol, 2002).
Methodology
Building on our research into cross border egg donation in Israel/Palestine, Romania and Russia, a 2-year study 5 of reproduction and migration was conducted in which we examined the experiences and practices of cross-border egg provision by ‘migrant’ women in Spain. Barcelona was selected as the main research site as it is one of Spain’s most popular destinations for seeking reproductive treatment with donor eggs. Across four short-term ethnographic visits 6 in Barcelona, between April 2016 and September 2017, we recruited two clinics and 11 egg providers (see Table 1 for details). The clinics supported participant recruitment by disseminating our recruitment call to interview migrant women who acted as egg providers to women under the clinics’ care and served as ethnographic observation sites; egg providers who consented to meeting the researchers were then introduced to us and given detailed information about the study. Weis and Nahman conducted all of the interviews, either together or separately. To accommodate the potential language needs of non-Spanish egg providers, we provided participant information sheets in English, Russian, Romanian and Spanish. We recruited n = 8 participants via clinics, and a further three after participants passed on our research call to other migrant egg providers. The latter three provided or considered providing their eggs in additional IVF clinics in Barcelona and Madrid. Interviews took place in privacy on clinic premises, in cafes across Barcelona and over Skype. The interviews were semi-structured, with the opportunity for women to ‘tell us their story’ and lasted between 45 and 100 minutes. They were conducted in English, Romanian, Russian, Spanish and German. All interviews (n = 17 in total, including 6 follow-up interviews) were transcribed verbatim and translated into English. 7 All participants were offered the chance to see transcribed interviews for comment, and one participant took up that offer; no changes were made. The data were thematised and coded. An initial reading of the transcripts was conducted, discussed and final themes agreed upon by the researchers. Upon agreeing on a final coding framework, the interviews were then coded in Nvivo.
Interviewee Details
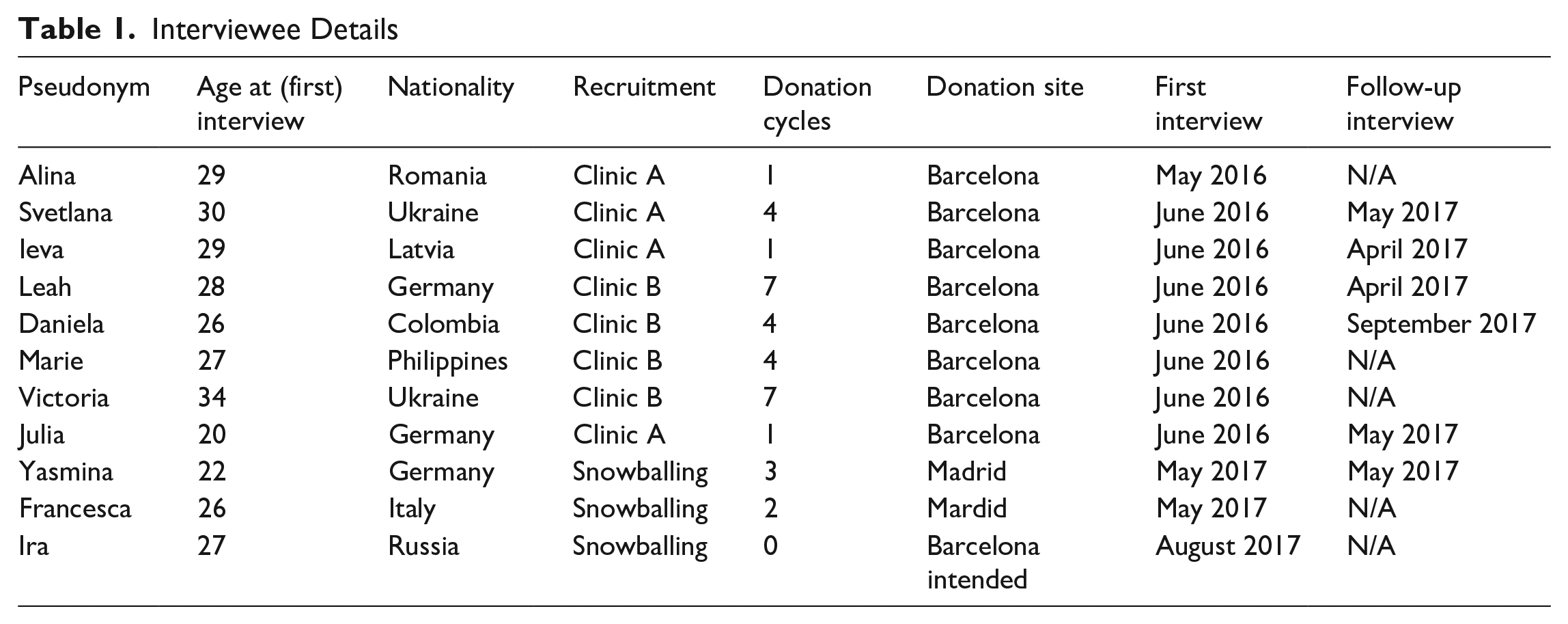
All women who had provided eggs had come to Spain between 7 months and 14 years before their first donation; five women came seeking work, three women came as teenagers following family migration and two women came for higher education. They only considered providing eggs after arrival in most cases in contrast to the more common travelling for egg provision seen in other examples (Pande and Moll, 2018; Weis, 2021a). A Russian woman, Ira, was in Barcelona on holiday when she took the opportunity to inquire about donation and the option of temporary visits to implement the donation. Furthermore, the women in our study shared the experience of migrant precarity and phenotypical desirability (Russell, 2015) that facilitated their becoming egg providers.
Socio-Technical Becomings
We begin with six socio-technical processes on the part of IVF clinics that produce the bioavailability of women and oocytes. First, through investing capital in producing highly relatable advertisements on familiar conduits of information such as popular social media platforms. Second, through stretching legal guidelines of who is a permissible donor. Third, by creating clinical spaces that are inviting and feel safe. Fourth, through a form of emotional labour on the part of staff, involving a pleasant demeanour. Fifth, through creating a ‘romance’ of doing something to make others happy. And sixth, by producing medical compliance in providers. While several of these have been noted in research around egg donation, surrogacy and IVF more widely, we focus here on how they help make women bioavailable within the migration and Spanish context.
Before egg providers even enter the clinic, the work to produce their bioavailability has already begun. One of the socio-technical layers that produces willing egg providers is advertising on social media, such as Facebook, Instagram and Spotify, that works to secure a willing, local pool of women. This first promotes a sense of normalcy and safety for the recipient, and finally creates medically compliant bodies.
Ieva (29, Latvia, one donation) told us: I mean, I was listening to my music, as always, and I heard an advertisement [saying] ‘do you want to be a donor?’ – yeah! On Spotify! It’s incredible! You know, Spotify is the biggest website to listen to music. . . . . Can you believe it . . . . So I said, ‘oh, it’s a good thing, a normal thing, nothing strange, nothing bad, everything will be secure and you know . . . ’ stuff like that. And then I saw the hospital, because this is a very important and very good hospital. So said, everything will be alright. I can do that.
8
Their advertising on platforms such as Spotify made the clinics seem safe, approachable and reputable, especially to a population who is displaced or has uncertain citizenship. This was not a back-street deal they were about to conduct, but rather, a highly safe medical procedure, at a renowned clinic. Furthermore, the professional appearance of the advert and the procedure gave an additional feeling of safety. Clinics invested capital, in the form of thousands of Euros, to produce highly branded advertising and online spaces. This is a first step in producing the bioavailability of all egg providers. But migrant women, in particular, may be susceptible to this, given how different forms of media (Spotify, Twitter, Instagram) offer relatable and familiar spaces. These spaces, especially for those not in their ‘home’ country, help people to feel they are part of a larger global collective, where the unfamiliarity of the country of settlement may be made familiar and homely by the seamless continuity of social and other media forms (Bonini, 2011).
Stretching the legal guidelines is another mode of producing bioavailability in migrant women. Medical staff or representatives at our two Barcelona-based clinics assured us that to be eligible to donate, all women had to be residents of Barcelona or the surrounding areas. This was overwhelmingly the case at the two clinics where we were based. Yet a third clinic, where we did not conduct interviews, was reportedly accepting non-Spanish-based donors. Ira, who considered providing her eggs while on holiday, took the opportunity to inquire about donation at this clinic, and was told not to worry about not living in Barcelona, as long as she was in Barcelona for the treatment. The clinic told her to return the following day for all required testing. If the test results found her to be suitable, she had approximately 6 weeks to return to Barcelona and start her injections. She was told to book this ‘subsequent holiday’ for 2 weeks to allow enough time. Thus, at least one clinic in Barcelona not only worked with local donors but also wanted to attract a mobile donor population.
The next layer of producing bioavailability happens with the design and décor of the spaces of the clinic. These spaces produce a sense of exclusivity that embraces the donors, who generally would be outsiders in such spaces. The production of bioavailability is increased by giving donors a sense of welcome, but also potentially of the expertise and elitism of biomedicine as embodied in the spaces of the clinic themselves. Here we describe one of the three clinics in more detail as we encountered it ethnographically. 9
In clinic A, you walk into a large, glamorous, and airy modern building. The sliding glass doors are all embossed with the clinic’s logo. They move effortlessly aside as one walks through them. To get to the egg donation wing, one takes the lift or stairs to the first level and is welcomed by a friendly receptionist. The discreet manner of the receptionists ensures privacy between patients by ringing through to the clinic behind them and directing patients to one of several waiting rooms. These rooms are uniform, with leather seats, arranged in a square, walls bearing posters of IVF treatment in pale pastel colours. Along the corridor are various treatment rooms and offices, most with doors closed and people in white coats entering and exiting busily. In this clinic, donors and recipients may be sat in the same room with one another, waiting. While the guessing game of who was a donor and who a recipient was an interesting pastime for the researchers, as we were waiting, sometimes for a long time, it is likely that the discretion of the reception staff and medical doctors worked to conceal donors and recipients from each other. In Clinic B, donors and recipients were seen in completely separate buildings.
Apart from the physical space of the clinic, the warm welcoming demeanour of the staff, a form of emotional labour, helped produce bioavailability. Egg providers in all clinics were impressed with the attention they received from the clinics; this may be in contrast to how migrants experience other social institutions that may be more hostile to them as workers, students or patients. Daniela, the Colombian donor, explained that she did not have many friends to confide in regarding her donation experience and her aunt refused to accompany her to appointments after witnessing Daniela’s discomfort and pain. ‘But the nurses are very nice’, she added, she felt taken care of. Francesca (26, Italy, two donations) told us how the nurses made her feel comfortable by accommodating her needs. Not only did they answer all her questions, but also: There were some things that I didn’t understand because they use these medical words. I speak Spanish, but I do not understand these medical words very well, but the nurse solves any doubts I could have.
Yasmina (22, Germany, three donations), who donated in the same clinic, added that the nurses were very accommodating with non-native Spanish speakers and ‘tried to explain everything [clinical] . . . simplified’ so she would understand.
Clinics create a kind of heteronormative ‘romance’ 10 of egg donation by presenting ideas of making a ‘happy family’ (Ahmed, 2010; Mohr, 2014; Nahman, 2013; Schurr and Militz, 2018). As Thompson (2011) has argued in this journal in relation to ‘medical migrations’, transnational reproduction is ‘enabled by discourses and practices that have powerful affective dynamics’ (p. 207). Acknowledging multiple ways of conceptualising affect, with different political ‘grammars’ or outcomes (Holzberg, 2018), the accounts of women we interviewed lead us to conceptualise it through a view of the operationalisation of the affect of a heteronormative romance that produces women’s extractability in the global chains of reproductive commodification (Vertommen et al., 2022b) through a narrowly proscribed heteronormative nuclear family, which the donors themselves may or may not also have. 11
One of the egg providers, Alina (29, Romania, one donation), recalled a radio advert thus: ‘If you want to help another woman, you can come and donate’. That’s it.
The romance played out for Victoria (Ukraine, seven donations) through making another woman happy, I see my own little ones, and I think that somewhere out there similar ones are born to someone, and this woman will be happy. In the beginning you don’t understand this, you think ‘this is my child, somewhere there, out there’ –later you begin to think ‘that is not my child, that is [the child of] that woman who carries and gives birth to that child. Though there will be my genes, but – she carries him, she gives birth, that means, if she came here, she really needed this [help] – and [it] changed my view – here I am making somebody happy. And if there are 10 [children], then 10 times better. How many people can be happy with that! That moment! Those people who are searching . . . they can be made so happy with this gift. So, I think, more or less, of all these women, who are thankful and happy, because of me, because of others like me.
While being happy with making others happy may be gendered female, being happy with being a progenitor of another woman’s children may be a kind of queering of affect (Ahmed in Almeling, 2011; Holzberg, 2018). Concommitantly, this kind of gendered queer romance of making another woman happy is another element in which she makes herself medically compliant.
There were various strategies employed by clinics to produce compliance, relying on economic and demographic inequality. While the migrant egg providers who we interviewed were inclined from the start to be medically compliant, the unequal relationship between them and the clinic, economically and socio-culturally, the prestige of the clinics and women’s need for money to supplement low incomes was a palpable contrast. Ira (27, Russia), on holiday in Barcelona, attended Clinic C for an intake interview but decided against providing eggs. She described how the clinic downplayed side-effects and highlighted economic benefits of donation. Ira told us that she suspected the intake nurse, herself a former donor, downplayed any possible side-effects such as breast tenderness and enlarged ovaries: one friend donated many times and was ‘uncareful’ and rode a motorcycle. And the ovary ‘turned’ and she had to have surgery to turn the ovary back. The nurse told her, ‘A lot of girls write a lot of nonsense on online forums about side effects they had but this is all nonsense. They don’t have any experience because I was a donor 20 years ago and I have been able to have a child and no side effects. They make sure at the clinic that there aren’t side effects. If you do what we tell you to do, nothing [bad] will happen to you’.
Finally, she added, ‘There’s no evidence of long term side effects’. All risks were conveyed to Ira as individual cases, not a general risk – ‘really exceptional’.
In economic terms, this same nurse was direct with Ira: Theoretically you came here to help. But people don’t come here to help, they come for the money. If you follow our instructions exactly, all will be fine. We don’t guarantee you that you won’t have any side effects, like spots on your face, gaining weight, hormonal imbalances. [She said she had] a friend who was an 18-time donor years ago. And she was fine, and today she is a mother who has a child. (Ira, quoting the nurse)
The nurse told Ira that she could come donate at the clinic up to six times officially, but that the clinical staff would have oversight of how many local babies were born. Thus, if a recipient gave birth outside Spain, Ira could potentially donate up to 10 times. 12 Ira’s ‘biodesirability’ or racial desirability (see below and study by Payne, 2015), with green eyes and light hair, she was told, would make egg provision a reliable source of income. Ira decided against donation, feeling inadequately informed of the risks and medical procedures.
One final way in which medical compliance was produced is through withholding partial payment until post-donation health checks are conducted. Clinic A paid 750€ (75% of the final payment) on the day of oocyte extraction and the remaining 250€ on the final post-operative checkup a few days later. In what some women may have viewed as a paternalistic approach by the clinic, who viewed ‘this class’ of women to be less responsible for their own health and wellbeing, such a measure was meant to make sure that the proper standards of care were delivered.
From pre-entry into egg provision to exit, bioavailability is a process rather than a thing. Clinics, medical techniques, medicines and women produce it based on a balance of concerns for good care, and a reliance on global mobility, state policy, inequality and gender divisions.
Working on Oneself
Observing some socio-technical ontologies of bioavailable becoming above, it is important to note that women themselves strategically self-objectify, by making their biogenetic body available (as Thompson (2005) showed with respect to IVF patients). Broadly speaking, they do so through mobilising their racial desirability, pragmatic emotion work, negotiating time and creating a ‘romance’ around donation. These are routes to bioavailability that we map in this section. Even before any clinic encounter, and often unconsciously, women recognise their phenotypic or racial desirability, which is confirmed by clinics. Women accept their need for money and try to find ways acceptable to themselves to earn money, and pragmatically do the emotion work 13 on themselves to make this possible. They then engage in the practices that lead to egg provision, such as attending pre-donation counselling, taking hormone regulating pills to manage their cycle, self-administering the injections to stimulate oocyte growth and attending appointments to monitor this growth, and finally, by having their eggs extracted, all while having to make excuses to their employers and families around where they are going. And as seen in the clinical encounters, a ‘romance’ around donating helps them maintain the will to provide eggs and ameliorate it for themselves.
A key aspect of the process of making oneself ontologically available for extraction is having a deep, usually unspoken, understanding of global race inequalities and hierarchies, as well as one’s position within them. Women are usually aware of their phenotypic desirability to the clinics and commissioning parents. While there are many complex pairings that take place between oocyte recipient and donor, which are multi-layered and have been analysed elsewhere (see the studies by Kroløkke, 2013; Nahman, 2006, 2013; Schurr, 2017), here we focus on one aspect of stratified reproduction, which is ‘biodesirability’ (Payne, 2015). Or what we prefer to call racial desirability.
Leah who is blonde-haired ‘knew [I] was desirable’ due to her light skinned, light haired appearance. This knowledge of where one fits in to the global stratification of phenotypic desirability is coupled here with an understanding that one possesses a commodifiable body. Many women in this study were Eastern European, and as such were positioned, racially, in a complex way vis-à-vis the clinics and prospective mothers. Ieva (from Latvia), aware of the reproductive cross-border travel to Spain and recipients’ quest for resemblance (Kroløkke, 2013), expected her donation would be matched with a recipient from Northern Europe. Although they were desired for light skin and hair, their Eastern Europeanness is both a form of ‘post-colonial whiteness’ and a ‘minoritised whiteness’ (Lopez, 2012). This makes their desirability contradictory at times.
Egg providers from Latin American backgrounds were also contradictorily desired. If they possessed phenotypes resembling Europeanness, they were likely to be accepted. But we learned in the course of our research that women from Latin America were more likely to be declined from the outset, and those who looked too ‘indigenous’ or ‘Latina’, as they were characterised by one clinician, were even less in demand.
Racial desirability does not always reside with a European phenotype. Marie, who is from Barcelona but whose parents migrated from the Philippines, was told by her friend, similarly an egg provider, ‘they need people like you’. The implication is that some cross-border commissioning parents come not just from Central and Northern Europe but also from other parts of the world where matching a South East Asian phenotype is desirable. Marie felt desired but also obliged in this instance to help others.
It has been suggested that women doing egg donation are seen as ‘biodesirable’ (Payne, 2015) for their physiognomic features that make them appealing to commissioning parents who want a child who they feel resembles them. Yet the ‘bio’ in this instance of global migrant women may be overstated (Birch and Tyfield, 2013). It is not their ‘biological race’ that is desirable but rather their position in global racial hierarchies, or their imagined race (see also studies by Nahman, 2006; Weis, 2021a). To suggest the ‘bio’ is what counts is perhaps playing into a biologisation of race. If we remove the ‘bio’ from ‘biodesirable’ we are left with ‘desirable’ and what is desired is ‘race’ – a social rather than biological thing. We suggest that donors are desirable, and therefore bioavailable, for their phenotype and, at the same time, for being a kind of precarious and cheap commodifiable worker.
Women’s reproductive, embodied labour is crucial for the biotechnological industry, but remains undervalued because the productivity resides in their bodily tissues and capacities (Cooper and Waldby, 2014: 59). Feminist political economy discussions of embodied forms of labour have argued the centrality of women’s biological bodily labour to the creation of value (Mezzadri et al., 2021). Their bodies are the primary site of value creation under capitalism and therefore their own accounts of this value are crucial here as they sometimes get forgotten in discussions of the bioeconomy (Nahman, 2018; Newman and Nahman, 2020).
Yasmina and Ieva had both donated blood prior to providing eggs. They likened the two kinds of providing to one another, explaining that for them egg donation was just another opportunity to give a bodily substance they had in surplus (to receive money), with no use or other value. Yasmina (22, Germany, three donations) stated: I wanted to know what else I could donate, and I saw in the internet that one can donate hair, organs, and eggs, and so I searched for more information about eggs, and so – well, I couldn’t [donate] hair, because I have dreadlocks, and one cannot donate organs while alive and so eggs were left and so I looked for information in the internet, to have more information, and well, kinda like that. (. . .), it’s a bit of my body that I don’t need at this moment and can help another [person] with – It’s not like I am going to miss it.
The majority of women in our sample turned to egg donation because of the financial compensation of 1000€ per donation, and did not desire to know too much about potential risks involved; this would help them to engage in the ‘romance’ detailed in the previous section and ahead. They did not want to be deterred. Making and keeping one’s body and bodily substances available for extraction and the incorporation in other women’s bodies requires that egg providers perform a laborious form of emotion work (Hochschild, 1979), one form of which is comparing egg donation to blood donation as above. Meanwhile, pre-donation counselling was seen as just procedural rather than useful to them.
Alina, who spoke to us after an ultrasound procedure, which monitored her ovulation before her first extraction, emphasised a few times that, ‘I don’t think, I just . . . do it’. Ieva, similarly, tried not to think about possibly negative side-effects of injecting hormones and hyperstimulating her ovaries, things which she had been informed of by the clinic and through her own online research process. She reiterated to herself that the process and outcome would be okay. Speaking to us a week following her first donation, Ieva (29, Latvia, one donation) said: Everything depends on how you think. Because when you think everything is ok, everything is OK. If you are not afraid, nothing happens to you. Nothing bad happens to you. I felt very . . . (She signals bloating around her belly) . . .Very! But I said it is normal. I didn’t start to panic.
Her awareness of her affective response and trying to shape it structures her embodied bioavailability here as a process in practice (Blackman and Venn, 2010).
Once women passed the obligatory counselling and genetic testing, and started injecting hormones, they continued to try to shape their feelings towards egg donation as a process that was ‘nothing to worry about’. Hochschild (1979: 562) emphasised that ‘“emotion work” refers to the effort – the act of trying – and not the outcome’. This effort can be perceived in both Alina and Ieva’s statements above. This form of emotional labour worked in many cases. Three women in our sample stopped providing their eggs after the first time, while the remaining continued to provide eggs up to six more times.
To maintain bioavailability and source of income, women pragmatically adjusted their view that the children conceived from their egg were not their own children, despite being their biogenetic offspring, because they never had the intention to raise them. Nevertheless, as Victoria (34, Ukraine, seven donations) illustrates, internalising this idea can be a process: In the beginning you don’t understand this, you think ‘this is my child, somewhere there, out there’ – later you begin to think ‘that is not my child, that is [the child of] that woman who carries and gives birth to that child’. Though there will be my genes, but – she carries him, she gives birth.
Svetlana, who donated four times, explained: ‘Well I don’t want [to think about the donation-conceived children]. Because they are mine [laughs]. And then it would be hard to part. No’. Thinking about the potential children could make her feel tied to them, and possibly regretful for having provided her eggs. She needed the self-disciplining process of ‘not thinking’. Or rather thinking very hard about detaching her knowledge of genetic and cultural understandings of kinship, from new ways of conceiving of these relations under assisted reproduction.
Svetlana (30, Ukraine, four donations) stated that she did not ask whether her donations had resulted in any children: ‘But it is of course possible to express interest and find out. But I never was interested and didn’t ask. It’s interesting, but I somehow decided not to ask’.
In comparison to other European countries where egg provision is practised, women in Spain tended not to know what happened with their eggs (Weis et al., 2019). Svetlana’s comment reveals another strategy of emotion-work, which some egg providers put in place consciously or unconsciously: Egg providers did not want to think about the children potentially conceived from their eggs because it helped them remain bioavailable. Leah (28, Germany, seven donations) explains: You are signing that you don’t want to [know]. That way they are certain that you accept that . . . It is not ‘we don’t allow you [to ask]’. But if you want to know who those children are, then you don’t donate.
By being complicit with the protocol, egg providers present themselves as good donors to be asked for further donations.
A distraction from (not) wanting to know what happens to their eggs is a focus on the ‘romance’ of donation. As argued in the previous section, clinics promote a narrative in print, online media and in pre-donation instructions of the egg providers creating happy families. This supports the egg providers themselves to adopt a similar narrative romance around donation to another woman and creating nuclear families. Rather than being dupes to clinics’ persuasion, we see women taking this up as a strategy to help them in assisting reproduction.
Prior to beginning hormone treatment, Alina told us: I am a bit scared, but now that I put myself there, I need to continue. (. . .) I am also thinking about the other person, the person who receives. As far as I have understood, as far as they have explained, they don’t take your eggs until they have found you a recipient (. . .).
It is rather unusual for a donor to be used for a specific recipient unless she is of a rare phenotype, which Alina (29, Romania, one donation) was not. So this is clearly something she was led to believe and which helps her to overcome her fear. This queering of affect – a specific woman is waiting just for her – promotes her bioavailability. She continues: Hence, I also think about the other person, knowing she cannot have a child, and they tell her ‘we will have an egg donor for you in a month’ . . . ‘and you will have an egg’ and then [If I dropped out], they would have to tell her ‘no’, because she [the donor] has run off. That would be upsetting. (. . .) I wouldn’t like that.
Alina imagines it just like a romantic relationship with the emotive language of ‘running off’ and upsetting the prospective recipient. The narrative that helps her to emotionally invest in giving her egg to a specific woman depends on the information the clinic provided. She expected there to be one single recipient for her eggs and began to feel connected and responsible to help this woman achieve motherhood.
The egg providers we spoke to also romanticised their opportunity to give a gift to the recipients. Marie, who had donated four times at the time of our interview and intended to continue donating, stated, ‘It is a nice experience that you are able to give’. Victoria, who had been a donor seven times, reflected: And if there are ten [children from my donations], then ten times better. How many people can be happy with that! That moment! Those people who are searching . . . people they can be made so happy with this gift. So, I more or less think of all these women, who are thankful and happy, because of me, because of others like me.
As discussed earlier, while maternal giving is often gendered as female (Almeling, 2011), giving a woman a gift of a baby may be seen as a queer relationship between the two women, or the traditional heteronormative script around reproduction.
Finally, becoming bioavailabile requires that women migrants negotiate the challenging terrains of making themselves present in body and in time at clinics. This, far from being simple for women in precarious labour situations or complex family arrangements, is a challenging thing. It makes their bioavailability all the more a process of ontological becoming: negotiating schedules, capitalist and biological timings and kin relations. Alina (29, Romania, one donation) explained that it is difficult to anticipate the exact course of the donation, making it challenging to manage employment as a hostess and parenting her toddler. Once she started self-injecting hormones and had an ultrasound appointment to monitor follicular growth, she was notified of the extraction appointment, which depended on the development of follicles containing oocytes. Each woman’s ovaries respond differently to the treatment, and doctors cannot provide a schedule in advance to make arrangements. Therefore, she needed to make and keep herself available to attend these appointments.
I needed to tell them [at work about where I am going when I have to take off for the appointment]. I have explained to them that I am in this project [egg donation] . . . . I need to go.
Daniela (26, Colombia, four donations) felt she could not tell her boss. She, therefore, scheduled appointments during her lunch breaks and skipped lunch to make time for them. Leah (28, Germany, seven donations) avoided any problems with having to justify to anyone where she was going, or any interruptions to work by focusing her donations in the summer, when work was less busy. Meanwhile, for Ieva (29, Latvia, one donation) and Julia (20, Germany, one donation), there was limited availability. Ieva was to start her air hostess job and Julia flew back to Germany and had her tickets booked already. In both these cases, the clinic had to work with the women’s own schedule and accommodated them by performing the donation while they were in Barcelona and not working. It is notable that these women in particular were accommodated, whereas other women might not be, due to their phenotypical desirability. Being present in the clinic for a donation is enabled by all these different forms of labour.
Hence from the perspective of women ‘working on themselves’ becoming bioavailable involved a mixture of racial desirability, emotion work involving queer affective labour and a narrative of ‘romance’ with careful negotiation of their work precarity and relations with the recipients, their oocytes, their (re)productive bodies, employers and family relations.
Conclusion
What we offer here is a novel account of bioavailability informed by understandings of how bodies come into being in multiple ways and in different configurations, and marginalised commodified subjects’ centrality to this process of becoming. Redefining bioavailability involves a feminist critique that recalls Haraway’s feminist cyborg who appreciates global inequalities, gender, race. The hybridity of the cyborg is manifest here in the theoretical conjoining of feminist STS with understandings of embodiment as a process, and debates around affect, emotion work as well as understandings of labour coming from Marxist feminist political economy. This has involved looking at how clinics help create conditions for bioavailable becoming, while capitalism, racism, histories of colonialism, gender and stratified reproduction already laid out the conditions for that. When put together with the strategies and voices of migrant women we encountered in Spain, we hope to offer a more in-depth picture of what bioavailability means and how it can be utilised in other arenas of analysis.
With an ethnographic view into the socio-technical and individual worlds of migrant egg provision, as well as global and national conditions of inequality, we offer the suggestion that one could not simply ever just be bioavailable. We are grateful for the immense work that went into bringing this concept into the social sciences by Lawrence Cohen and others, because it has been such an important contribution to our own and many others’ thinking.
Whereas ‘bioavailability’ has been a concept that has been usefully employed in the literature to critique the bioeconomy’s use of precarious labour/bodies, little has been done to theorise the ontological aspects of the effort and process of becoming bioavailable. What we have found in our analysis of migrant women egg providers is that bioavailability involves a lot of work, similarly to gender, race and embodiment. Unsurprisingly perhaps, being gendered female, being racialised and being bioavailable are highly correlated. Indeed, gendering and racialising seem to be strategies used in making bioavailability. Histories of colonial extraction bear this out as well (Vertommen et al., 2022a). We hope to have helped extend bioavailability’s usefulness to the social study of bodies and of science and technology.
What the specific example of migrant egg providers gives us is also a sense of the deeply contingent nature of what we call the bioeconomy more broadly. A large part of the reproductive bioeconomy depends, and in many senses is determined by, the presence of women who are willing and able to provide eggs. This indicates how crucial it is to get deep into the ethnographic and interview detail, as we have done here, of their understandings of making another woman happy, not thinking, racial desirability, the safety of the clinic. We suggest that offering accounts of the processual nature of bioavailability produces the conditions for a ‘truer’ account of the reproductive bioeconomy and of the production of value therein. We do not use the concept of ‘truth’ lightly here, but call forth Haraway’s injunction that the feminist cyborg tells truer stories of biological practices – that is, those which question the truth claims of science, medicine and technology and also treat the experiences of people in/with medicine as having scientific value and political/analytical primacy. Without the geographic, historical, emotional and economic processes that led to their bodies being present, precarious and in need of financial support, there would be no incorporation into another body. That the concept of bioavailability is elastic enough to expand and be made more specific, as we have done here, is an indicator of how robust, relevant and accurate it is for the arena in which it was first introduced by Cohen.
Footnotes
Acknowledgements
The authors would like to thank the women who offered their accounts to us and to the clinics that opened their doors and supported this research. We are also very grateful to the reviewers and Editorial Board for their generous feedback.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was made possible through the generous funding of the Social Science Research Group at the University of the West of England, Bristol.