
Abstract
Medical schools are among the most important spaces for the history of the body. It is here that students come to know the anatomical bodies of their future patients and, through a process of cognitive and embodied practice, that the knowing bodies of future clinicians are also shaped. Practical and theoretical understandings of medicine are formed in these affective and historied buildings and in collaboration with a broad material culture of education. Medical schools are, however, both under-theorised and under-historicised. This article integrates ‘materialist’ considerations of the body with Henri Lefebvre’s philosophy of space and rhythm in order to compare two markedly different spaces – the 19th-century Anatomy Department at Semmelweis University in Hungary and the mid-20th-century ‘skills laboratory’ at Maastricht University in the Netherlands. This comparison suggests that biomedical bodies are variously shaped by the agential and affective material histories present in the everyday experience of contemporary medical education.
Introduction
As Antal Szerb (2015: 5) explained to a rather unexpected visitor, in Budapest, ‘the beings that really matter are the houses’. Writing in 1935, Szerb’s gently surreal love letter to the city emphasises the architectural imposition of the late 19th century. As imposing vestiges of historic ideas and ideals, buildings bind us to the past in numberless ways. We navigate, fill, and function inside of and around spaces that were built for people and practices far removed from the rhythms of everyday life in the 21st century. One remarkable site that was missed out of Szerb’s tour, but which has made an impression on many generations of young medical students, is Semmelweis University’s Department of Anatomy, Histology, and Embryology. As with medical schools the world over, this imposing building has, since its construction in the late 19th century, been a central site for the discovery and dissemination of biomedical understandings of the body. This article considers these historied buildings – and the historied materials which fill them – and asks how student understandings of medicine are affected by the many pasts that remain present in the broad material culture of the modern medical school.
In order to do this, this article compares the material culture of two noteworthy but markedly different spaces – the Anatomy Department at Semmelweis and the ‘skills laboratory’, or Skillslab, at Maastricht University’s medical school, a much newer faculty in the south of the Netherlands. Drawing on a breadth of material – including printed and material sources, photographs, oral history interviews, and ethnographic insights generously provided by Rachel Vaden Allison and Anna Harris, who have conducted extensive anthropological fieldwork at Semmelweis and Maastricht respectively – this article contributes to the historicisation of debates around the configuration of bodies in biomedicine (e.g. Hirschauer, 1991; Johnson, 2008; Michael and Rosengarten, 2012; Taylor, 2005).
Its history stretching back into the 18th century, Semmelweis is Hungary’s best-known medical school, with the Anatomy Department the main space in which students are introduced to the body. Here, an exhaustive introduction to anatomy derives from extensive cadaveric dissection. Semmelweis’ material construction speaks to the early history of biomedicine, its emergence from 19th-century laboratory sciences, and its intellectual basis in Enlightenment thought. Maastricht, by contrast, drew from the social radicalism of the 1960s as an explicit attempt to break free from earlier approaches to medicine and, through community and clinical integration, to instead inculcate a fuller understanding of the social determinants of health. Where Semmelweis’ Anatomy Department is a commanding monument to modernist science, Maastricht’s buildings have tended to be more modest, indicative of a self-reflective moment in the history of medicine. Opened in the mid-1970s, Maastricht embraced and helped develop a novel pedagogy that focuses on the early development of clinical skills. Anatomy, here, is learned through real-life problems of patient care. As such, students’ first formative years centre around the Skillslab, a series of learning spaces that were initially intended to be more closely integrated into the teaching hospital but which have since moved into a purpose-built simulation of the clinical environment. As extant materialisations of distinct periods in the history of medicine, these two schools have remained dependent on distinct materials cultures of education and offer distinct conceptualisations of the body as a result. The knowing bodies of future practitioners and the known bodies of their future patients are made here, and are made differently, shaped in place by the old ideas and past practices which endure in the distinct material episteme of each school (Nott and Harris, 2020, 2022, 2023).
Although employing markedly different pedagogies, these two schools are bound by the struggle to teach students about the body and its workings. This challenge is met with teaching tools that tend to imbue the patient body with the sort of ontological assuredness necessary for students to pass exams and, later, to treat patients. However, as Annmarie Mol’s work has made particularly clear, there is not one universal, standardised body that medical students can come to know. Instead, patient bodies are made knowable through practical engagement with ‘everything and everyone that is active while being practiced’ (Mol, 2002: 32). In our case studies, for instance, the vascular anatomy which a student at Maastricht encounters while learning to take blood is ontologically distinct from the same vein under dissection at Semmelweis. Similar conclusions have been extended to consider the broader, socio-material emplacement of bodies in biomedical spaces. As Alice Street has shown in her ethnography of the Mandang Hospital in Papua New Guinea, medicine is enacted differently in public and private wards. Attending to the spatial distribution and socio-material complexity of medical infrastructure shows ‘a place of deep ontological uncertainty and instability, where knowledge of oneself and others cannot be taken for granted’ (Street, 2012: 13). Rarely, however, does the material culture of medical education attend to these inconsistent and innately social bodies. Indeed, the surety of these educational, epistemic technologies actively works to deny this sort of material fluidity (Nott and Harris, 2020, 2023).
In this respect, our comparison illustrates the relevance of material history for those post-phenomenological studies of medical perception which consider how knowledge derives from embodied, sensory interactions between people and things, rather than simply from the conscious evaluation (e.g. Hardy, 2013; Harris, 2016; Prentice, 2013; Vinson, 2020). Materials are, of course, routinely used in teaching, but ideas and practices are also shaped by everyday encounters in these unusual and affecting environments. Recent research in biomedical settings (e.g. Street, 2012; Underman, 2015, 2020) has mobilised ‘affect’ as a vital force that directs clinicians and their patients around and against the spaces, bodies, and tools of the clinic. The affective quality of these spaces is always ‘engineered’ (Thrift, 2007: 235), a product of unique and individual histories, of epistemic traditions and of the political economies from which they derive. Despite this, it is rare for theorists of affect (e.g. Thrift, 2007), or its emplacement as ‘atmosphere’ (e.g. Böhme, 2018), to extensively engage with the historical determinants of their subjects (a similar concern is articulated in Brown et al., 2019). Although seldom employed within affect theory, the broadly Marxist, historical-materialist underpinnings of Henri Lefebvre’s (1901–1991) critique of the spaces (1991) and rhythms (2013) which culture everyday experience allows us to consider the affective weight of our historied surroundings. In general, Lefebvre’s influence on affect theory has come through the mobilisation of rhythm as ‘a vehicle for experimenting with [contemporary] experience’ (McCormack, 2014: 6). However, and although Lefebvre begins from a similar analysis of contemporary experience as later writers on affect, his work also emphasises that a holistic consideration of the body in space offers a means to first understand and then to resist the embodied imposition of historied materialities. Integrating Lefebvre’s philosophy with the social study of medicine in particular allows for new questions to be asked about the spatial and material production of bodily difference (Kinkaid, 2020), but it also provides a means to consider the various affective histories which direct practices and epistemologies within contemporary medicine.
Space, Rhythm, and the Affect of History in the Modern Medical School
Lecture halls, libraries, laboratories, seminar rooms, and dissection theatres shape students’ formative experiences of medicine; students navigate these spaces in rhythm with classes, examinations, clinical rotations, and graduations. Here, cosseted by the material and epistemic time-space of the medical school, students begin their critical consideration of the medicalised body. Envisioned as a means of studying the relationship between the cosmic rhythms of the natural world and the rhythmic processes humanity has constructed to fit within it, Henri Lefebvre’s rhythm analysis was intended as a way to detail the affective relationship between the body and its material surroundings (Lefebvre, 2013). Although the body produces and is affected by natural cyclical rhythms – by breaths, heartbeats, days, nights and seasons – we are also affected by the mechanical and industrial, the linear rhythms which make up the dominant temporality of capitalist modernity. It is only as a result of material and technological change – the expansion of cities or the development of artificial lighting – that human bodies have become estranged from the cyclical rhythms of the natural world. The steady professionalisation of health and death care since the 18th century has also meant that industrialised populations have never been further removed from our own corporeal rhythms. Like hospitals, nursing homes, hospices, and morgues, medical schools contribute to a collective, societal estrangement from the rhythms and textures of the body. The history of medical education is then part of a broader historical decorporealisation of space, an ongoing process which has contributed to ‘the spiriting-away or scotomization of the body’ (Lefebvre, 1991: 201).
The body, in Lefebvre’s inherently historical-materialist approach, exists in a dialectical relationship with the spatial and material environment (see, on this point, Kinkaid, 2020; Simonsen, 2005; Stewart, 1995). ‘Every shape in space, every spatial plane, constitutes a mirror . . . within each body the rest of the world is reflected, and referred back to, in an ever-renewed to-and-fro of reciprocal reflection’ (Lefebvre, 1991: 183). Historical materialities are, then, reflected in our modern bodies. Although these ideas have previously been implemented with a mind to history (e.g. Highmore, 2002; Vergunst, 2010), they have seen limited application in medical settings or among scholars of the body in biomedicine. This is, in part, because the body is never fully conceptualised in Lefebvre’s work. Although recognising the irrationality of the body, Lefebvre also imbues it with enough ontological stability to allow for a close analysis of its rhythms; it is the ‘total body’ that offers a means to fully engage with the ‘practico-sensory realm’ (Lefebvre, 1991: 201, 405). The romantic holism of Lefebvre’s body might, in this respect, gain something from the more recent, materialist understandings of the body found in medical anthropology and Science and Technology Studies (STS) (Kinkaid, 2020: 183). At the same time, Lefebvre’s work provides a vehicle to consider the enduring agency of historied materials and the ways in which – through spatial and rhythmic imposition – their pasts contribute to affective experiences of the present.
Although this article only touches on these potentialities, as a primary space in which bodies are consciously considered, the medical school is an apposite site to begin considering the mutual enrichment of Lefebvre’s historical materialism and new materialist readings of the biomedical body (on the necessity of this approach more generally see Choat, 2018). At Maastricht and Semmelweis – two very different schools – the ontologically unstable bodies of medical students confront the ontologically unstable bodies outlined by their teachers; the lived, social bodies of our everyday selves confront the anatomical, object bodies that are being taught. Here, student’s explicit attention to the cyclical rhythms of the body – of breathing, heartbeats, digestion – is mediated by the shifting, linear rhythms of technological development and material change. The social scotomisation of the body is progressively undone, mediated by the material application of medical pedagogy, as well as by more mundane, everyday encounters in these affective, historied spaces. Yet, as we will see, neither the modernist medical education practised at Semmelweis nor the postmodern simulations offered at Maastricht provide absolute insight into the ‘total body’ of the patient. Necessarily abstracted from the social space of the everyday, the patient can only ever be partial. Likewise, the embodied attention of the student is never absolute but is necessarily refracted by the technologies which are used to introduce anatomic form and function. Understanding the nature of this refraction requires consideration of the material and conceptual origins of these objects.
The Department of Anatomy, Histology, and Embryology at Semmelweis University, Budapest
The belle-époque was more apparent in Budapest than, perhaps, anywhere else in continental Europe. Between the establishment of the Dual Monarchy of Austria-Hungary in 1868 and the start of the First World War, Budapest emerged as one of Europe’s great cultural capitals. The considered expansion of modernist infrastructure built during this relatively short period of political and economic stability included the oldest metro-system in continental Europe and, in 1898, Semmelweis University’s Department of Anatomy, Histology, and Embryology (on the history of medical education in Hungary see Molnár, 2019; Simon, 2010). The Anatomy Department was one of a number of medical school buildings constructed in an outlying part of the city which was soon dominated by the ‘Klinikák’, or ‘Clinics’, the name by which the whole area is often now known. Some 10 years after their establishment, The Lancet claimed ‘without exaggeration, that the Budapest clinics are among the best-equipped institutions . . . on the continent’ (Budapest: from our own correspondent, 1909). Anatomy training has continued largely uninterrupted in these same buildings, in the material apotheosis of a late 19th-century approach to medical education (Figure 1). These ‘old world’ surroundings are part of Semmelweis’ contemporary allure (Schuetze, 2013), but they also contribute to the contemporary enactment of 19th-century anatomies, largely defined by mechanistic understandings of ‘the body proper’ (Lock and Farquhar, 2007). As an idealised space in which students can unpick the complex clockwork of an enduring ‘Cartesian’ construction of the body (Hacking, 2007), Semmelweis’ Anatomy Department also reproduces a tradition of scientific authority over the bodies of the patient public (Foucault, 2003 [1963]).

The main lecture theatre, Semmelweis Department of Anatomy in 1909 (a) and 2018 (b). (a) taken from International Medical Congress (1909), (b) courtesy of Rachel Vaden Allison.
In order for students to access the biomechanical body, both the Anatomy Department and the entire curriculum are built up around the study of human remains. Although an imposing, five-storey structure – one designed in close collaboration with Géza Mihálkovics, a professor of anatomy who brought architects on factfinding tours of similar institutes abroad (Molnár, 2019: 37) – it is what happens underground that defines anatomy education here. Cadavers enter the Department through the basement and are distributed along either wing of the horseshoe-shaped building (Figure 2). The west wing contains the First Institute, which deals with gross anatomy, the study of anatomical superstructures, the musculoskeletal system, the nervous system, and the organs. In the east wing, the Second Institute focuses on microscopic structures, histology, and embryology. Allocating half of its total space to the study of microscopic anatomy reflected the relatively recent application of laboratory methods to the question of medicine (Hopkins, 2020). Following this division, cadavers were ascribed to either the First or the Second Institute, where they were then processed, moving along separate but mirrored hallways. The various rooms along these corridors are where bodies were variously washed, frozen, injected, macerated, drained, and dissolved. Although the layout of the building and the function of its various rooms have changed somewhat over the years, the architecture is still oriented around the preparation, storage, preservation, and presentation of cadavers. In this respect, Semmelweis represents something like the ultimate decorporealisation of space (Lefebvre, 1991: 201).
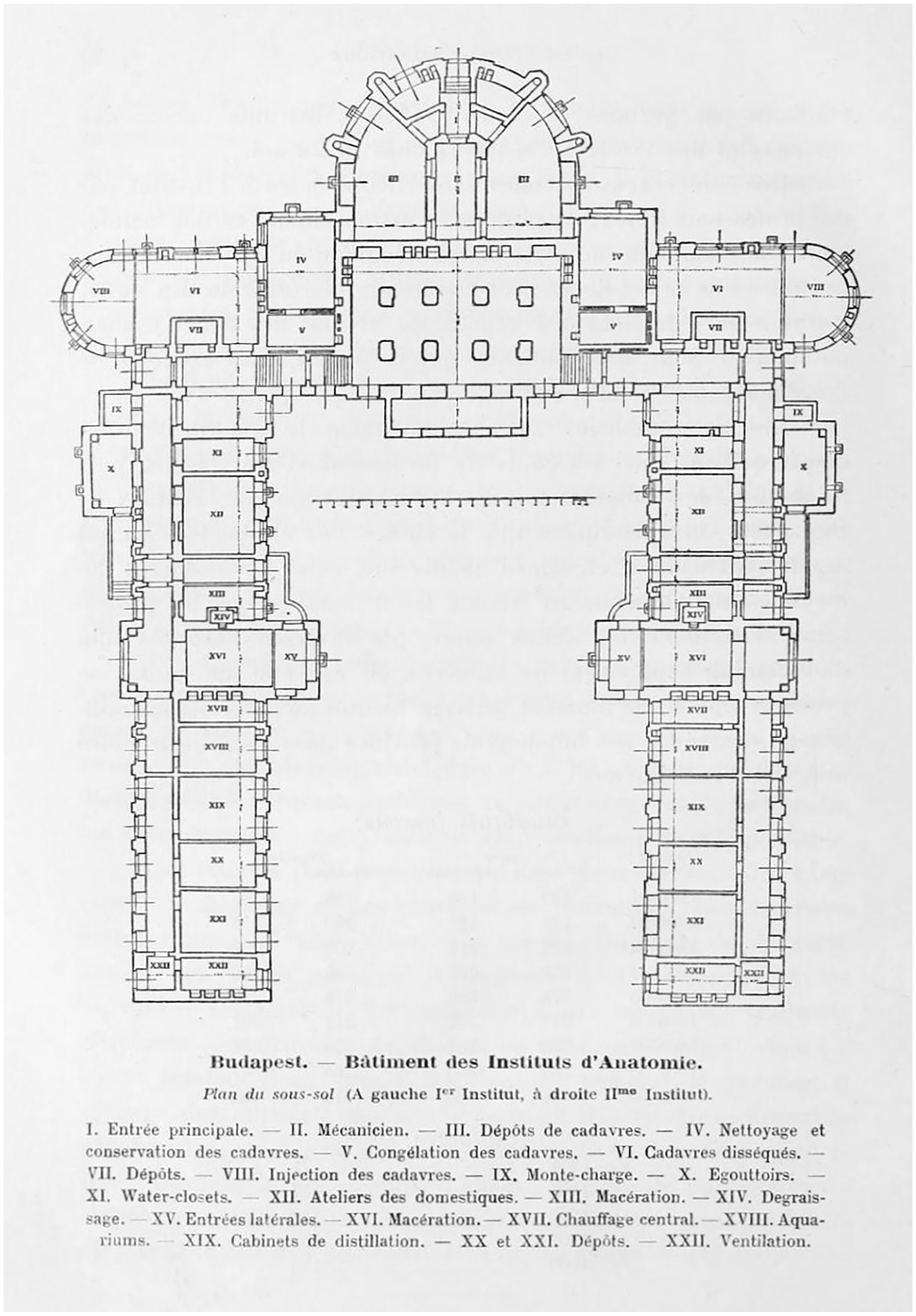
Basement plan, Semmelweis Department of Anatomy, 1909 (International Medical Congress, 1909).
In previous times and other places, difficulties preserving cadavers combined with cultural anxieties regarding the body after death in order to constrain their use in medical education (e.g. Richardson, 1988). By the mid-19th century, however, Vienna had become a burgeoning international centre for medical education, largely because of ready access to cadavers. Here the tolerant stance assumed by the Catholic Church, the influence of Southern European cultural assumptions around the body and soul after death, and the weak position of individuals in the absolutist state contributed to a notable permissiveness of cadaveric dissection (Buklijas, 2008). Tied, as it was, to Austria during this period, Semmelweis’ Anatomy Department represents an even more marked shift away from both ethical and material constraints on student use of cadavers. The Department’s capacity to process and preserve the recently deceased (and to ameliorate the unpleasant affect of dissection) benefitted from recent developments in architecture and engineering. Alongside basement machinery for the ‘degreasing’ and freezing of cadavers, central heating, ventilation, drainage, and lift systems were all mechanised throughout the building (International Medical Congress, 1909). This was, however, a period of experimentation. The placement of the ventilation systems, for instance, ‘did not give good results, because we often smell . . . the macerators’ (International Medical Congress, 1909: 23). Recent attempts to address this, through the addition of external air conditioning units, have been stymied by ‘heritage status’ of the building’s façade. Chemical advancements in embalming – in particular the 1869 discovery of formaldehyde and, from 1893, its commercial production as liquid formalin – complemented mechanical means to prevent decay (Brenner, 2014). The sharp smell of formaldehyde, the way that it burns eyes, irritates throats, and lingers on hands and clothing remains part of an enduring, affective culture of anatomy education. After remarking on the youthful countenance of one Professor Emeritus, he replied that the secret was a long career spent drinking embalming fluid. A similar encounter detailed by Rachel Prentice suggests that this is an old joke in the field of academic anatomy (Prentice, 2013: 48).
The interruption of the corporeal rhythms of the body after death has always been integral to anatomy instruction. However, the mechanised, modernist anatomy which endures in the material culture of Semmelweis forms part of a distinct material and epistemic break from an earlier tradition, one which required greater artistic or scientific intervention to preserve, reproduce, or represent anatomical bodies (e.g. Alberti, 2009; Berkowitz, 2013). The pedagogic value of these material assemblages – or what Daston and Galison (2010) describe as their ‘epistemic virtue’ – instead lay in their use of automatism as a means to achieve a more ‘mechanical objectivity’. With dissection rooms, histology laboratories, a photography studio, and museum, Mihálkovics made space to embrace scientific and laboratory ways of knowing the body. First preserved, then atomised, and ultimately understood, 21st-century cadavers move through 19th-century spaces, but always in collaboration with the technologies which they house, and the knowledge practices which they promote.
Anatomy instructors are, of course, aware of the problem that, in their subsequent practice, students will not often encounter bodies after they have died. Teaching, therefore, also involves something like a recorporealisation of the Department. While modernist methods of preservation have contributed to the primacy of ‘mechanical objectivity’ at Semmelweis, an older tradition of scientific illustration provides a means to restore the body’s vitality (Daston and Galison, 2010). Today, as in the early 20th century, hand-painted renderings of anatomic structures still hang on either side of the blackboard in the lecture theatres and are swapped in and out according to the topic of the lecture (Figure 1). Lecturers routinely point to the idealised forms which are presented here or which are drawn on the large blackboards in the middle of the room, and in almost every other teaching space throughout the building. Used in conjunction with cadavers, chalk drawings add dynamism to the anatomic material seen in dissection or under microscopes. Students are encouraged to copy down the coloured chalks and firmer lines are used to emphasise movement, texture, or variation – the mutability of living bodies which is absent from cadaveric anatomy (Allison, 2022).
As these contradictions suggest, cadavers occupy a liminal space between dead and alive, objecthood and personhood, the universal and the particular. Recent ethnographies of medical education explain that these ambiguities present a valuable ‘ontological duality’ and a ‘moral laboratory’ for student doctors (Olejaz, 2017; Prentice, 2013), and jars somewhat with earlier anthropologies (e.g. Good, 1994; Hafferty, 1988) which emphasise dissection as a process of objectification, one in which the violent destruction of flesh contributes to the simultaneous erasure of the person. To this end, Elizabeth Hallam (2017) has suggested that a ‘relational anatomy’ exists in modern British medical schools. Here, students recognise both the individuality and the social emplacement of the cadavers they are learning from; recognition of the tell-tale scars, painted nails, or dyed hair contributes to a relationship. A flexible concept, relational anatomy, is subject to variation across time and space. Today, Semmelweis makes use of many more cadavers than most British universities, this is one of their main selling points to overseas students (Schuetze, 2013). Most are donated as a means to defray funeral expenses – the university arranges the memorialisation and interment of cadavers after dissection. The individuality and social emplacement of the dead is, however, more apparent when, as is increasingly the case (see Vinson, 2020), dissection is only supplemental to other forms of anatomy education. When, as at Semmelweis, the Department and curricula are built up around dissection, a more distant relational anatomy emerges. Students routinely share space with the dead, they rest their notes on dissected bodies, and handle them distractedly while searching for the answer to a question in an oral examination (Figure 3). This does not mean to question the ethics of Semmelweis’ practice, or the service which the school offers the community, but to instead emphasise a distinct relational anatomy, one which builds upon a specific cultural history, and which is enacted in collaboration with the historied material construction of the medical school.
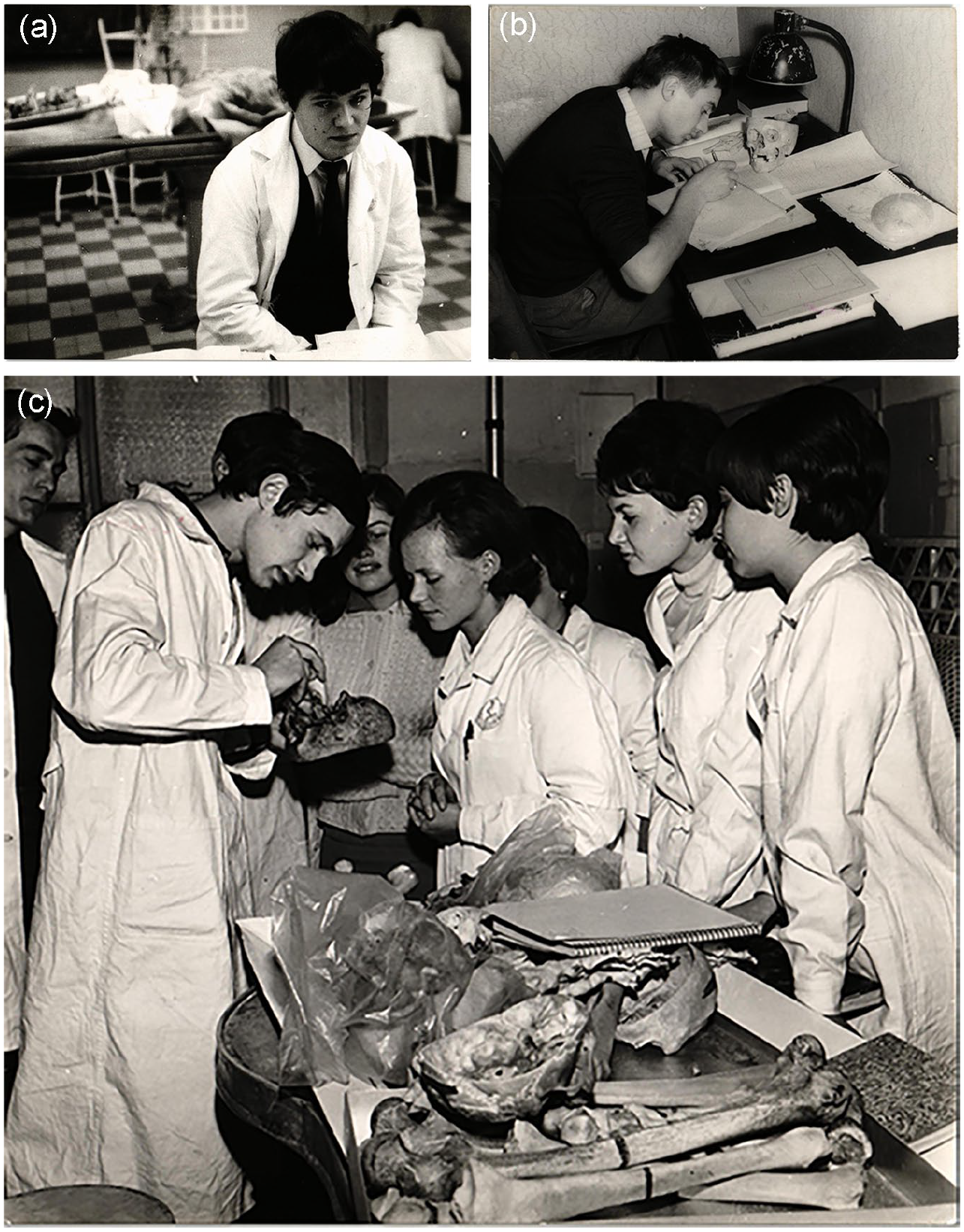
(a) Anatomy examination at Semmelweis, c. 1970s; (b) studying with anatomical specimens in the department museum, c. 1970s; (c) an anatomy tutorial, c. 1970s.
This tradition of medical education derives from an attendant history of state building in the late-19th century, binding Semmelweis in the present with the Foucauldian ‘birth of the clinic’ and the consolidation of governmental interest in and influence over population health (Foucault, 2003 [1963]). Indeed, the grandeur of the late 19th-century Klinikák was, like other architectural and infrastructural landmarks built during these years, a testament to Budapest’s newfound status as the second city of an emergent European monarchy. Budapest’s successful bid for the 1909 International Medical Congress and the government’s prideful advertisement of its medical infrastructure speaks to the political capital of medical education (International Medical Congress, 1909). As we will also see in Maastricht, the political economy of medical education can never be entirely disregarded from the affective encounter. Semmelweis’ earlier westward gaze was somewhat reoriented following the Second World War – portraits of Lenin, Marx and Engels watched over students studying in the library and Russian language classes and Soviet political science and philosophy were mandatory (SOTE, 1974) – but Soviet influence was relatively restrained in these years. The stability of the 19th-century buildings, traditions, and philosophies did not readily acquiesce to political change. It was only after the attempted revolution of 1956 that the Soviet central state offered significant intervention into the spaces and rhythms of medical education at Semmelweis. In order to expand teaching capacity in the now-crowded university, a competition to design the Theoretical Building at Nagyvárad tér opened in 1963. Located a few hundred metres from the Anatomy Department, the high-modernist, 23-storey tower was lauded in the architectural press for the way in which it ‘governs the whole area’ (Gyula, 1963; Magyar, 1979). Only the Hungarian parliament building, and two cathedrals, stand taller anywhere in the country.
Today it is the Theoretical Building, rather than the Anatomy Department, which is beginning to fade; staff complain of problems with infrastructure, lifts, or air conditioning breaking down. This may be analogous to the material and infrastructural ‘imperial debris’ (Stoler, 2008) which has been seen to convey an affective disaffection in biomedical spaces across the postcolonial world (Street, 2012). Unlike many postcolonial spaces, Semmelweis rests on the weight of its earlier, 19th-century construction. This has significant ramifications for students learning medicine here today. The methods, technologies, and philosophies which were built into the Department in the 1890s have continued to influence both teaching and learning. The primacy of dissection, in particular, allows for a visceral and affective understanding of anatomical structures. Yet, and unlike in some other contemporary medical schools (Olejaz, 2017), the liminal position of the dead is less readily apparent here. This is, perhaps, because Semmelweis is a truly modernist space – in the philosophical rather than architectural sense – and as Lefebvre explains, ‘this modern space has an analogical affinity . . . with the Cartesian tradition’ (Lefebvre, 1991: 201). Although the Cartesian tradition may have lost its imperious standing in medicine, in both practice and in theory, its philosophies remain present in the materials and technologies produced under its reign. The material affect of 19th-century practices and epistemologies of anatomy means that, at Semmelweis, it is a universalist object-body that tends to come to the fore in the present too.
The Skillslab at Maastricht University
The Skillslab at Maastricht University emerged out of very different circumstances than Semmelweis. Its material construction, and the ideas which underlie it, provide students with a radically different approach to the knowing and known body. Where Semmelweis is a standalone institute for medical education, and Hungary’s flagship medical school, the medical faculty at Maastricht is part of a large regional university that was initially established to provide tertiary education and economic stimulation to the province of Limburg, a geographically and economically peripheral part of the Netherlands. Opened as Rijksuniversiteit Limburg in 1974, and with only 50 students, the university was built up around the medical school and the explicitly experimental pedagogies that it pioneered. These experiments have since defined the university’s attempt to position itself as a centre of innovation in the increasingly competitive global market for higher education (Klijn, 2016; Knegtmans, 1992; Wachelder, 1992). While the Skillslab has moved through several buildings since its establishment in 1977, it has remained at the heart of medical education in Maastricht as the primary space in which undergraduate students begin to engage with the medicalised body. From their first week, students are introduced to the clinical skills which they will later be expected to use on real patients. This focus on clinical skill has meant that, unlike at Semmelweis, living anatomies are the basis of the curriculum. While learning to take a pulse, listen to the heart or lungs, assess reflexes, estimate cervical dilation, or perform a prostate exam, students are encouraged to confront the vital rhythms of health and disease, as well as the social rhythms which contribute to patients’ actions – the personal histories, pains, and anxieties that brought them into the clinic in the first place.
This approach emerged in response to the social pressures and discontents of the 1960s and as an explicit challenge to traditional medical curricula. The problems posed by the baby boom, post-war class formation, middle-class prosperity, and the Netherland’s increasingly well-educated patient base led to concerns that there were not enough General Practitioners (GPs) and that they were not properly equipped to care for this changing patient public (Klijn, 2016; Wachelder, 1992). As medicine became more and more specialist over the course of the 19th and early 20th centuries (Weisz, 2005), general practice was widely regarded to sit at the bottom of an increasingly diverse professional hierarchy. Fewer young doctors saw general practice as a route to professional advancement; there was no specific training in family medicine and no way to specialise as a GP.
Some considered this an overtly political issue; medical achievements were better than ever but there was a growing concern (e.g. Foucault, 2003 [1963]) that medicine could be both dehumanising and coercive. The conceptual basis and material constitution of the Skillslab emerged, in part, from the radicalism of the 1960s. Maastricht’s Basisfilosofie Achtste Medische Faculteit (1972) drew inspiration from the French anti-capitalist and student-led May 68 protests, specifically from a white paper in which the Comité de Synthèse des Étudiants en Medicine de Paris argued that they had ‘to develop from passive consumers of a curriculum composed outside of them’ (quoted in Wachelder, 1992: 240). Somewhat coincidentally, Henri Lefebvre was both an important intellectual influence on the French left prior to May 68 and, subsequently, one of the protests’ most notable analysts (Lefebvre, 1969; Stanek, 2008). Lefebvre’s later work and the resulting changes in medical education speak to a shared heritage, not just in terms of resistance to the Foucauldian clinic but also in their attempt to rehabilitate the ‘total body’ (Lefebvre, 1991: 201, 405), inclusive and considerate of the social determinants of health.
This focus on problem-solving and student self-direction was not entirely new, but it chimed with the cultural revolutions of the late 1960s. Drawing from similar conclusions, an emerging pedagogy, Problem-Based Learning (PBL), was adopted by and adapted in Maastricht (Servant, 2016). The blurring of the distinction between student and teacher was extended to the doctor–patient relationship. A later university directive went on to highlight three principles that were to underlie the medical curricula at Maastricht: greater integration with extant health provisioning; focus on patient-oriented problems rather than basic scientific knowledge; and an emphasis on pathology rather than normal anatomical function (Wachelder, 1992: 250). Instead of adhering to a strict biomedical model, Maastricht embraced the psycho-social conditions that drove patients to and from their encounters with medicine. Around the same time, new methods for the testing of students’ skills were also being developed. The Objective Structured Clinical Examination (OSCE) proposed the evaluation of students’ performance in choreographed scenarios as a means to assess their clinical skills in terms of physical examination (taking blood pressure, detecting the pulse and lung sounds) but also their professional behaviours, lines of questioning, and ability to develop rapport with a patient (Harden and Gleeson, 1979).
Then, as now, anatomy was taught in conjunction with clinical skills, rather than as a standalone subject. PBL tutorials were to complement free and supervised study in the Skillslab which, from 1977, offered a dedicated space that students could access at any time to practice physical exams on their classmates or on the ever-growing population of anatomical models and mannequins. Skillslab tutors also produced teaching materials to support these ends, including educational films on good and bad interview technique, how to deal with ‘empowered’ patients, or the observation of non-verbal behaviours in patient consultations. The university also facilitated the first student manual for the learning of clinical skills. Illustrated with photographs of clinicians without the white coats which then signified professional status, Maastricht’s youthful educators worked to actively reduce the material distinction between doctor and student, patient and practitioner (Lodewick, 1978). These changes were evident in the initial construction of the medical school or, more accurately, in its relative lack of formal construction. In the late-1970s, the small student intake – and the idea that learning should be focused on extramural health environments, on GPs’ surgeries and the small hospitals already operating around the region – meant that the medical school was fit into a few rooms in a converted Jesuit monastery close to the city’s St Annadal hospital (Wachelder, 1992: 239).
Today, however, the Skillslab and the rest of the medical faculty stand apart from the city, across the river from Maastricht’s medieval centre, in an area known as Randwyck. Since the early 1990s, Randwyck has been home to the Maastricht University Medical Centre (MUMC +), a sprawling conglomeration of the large academic hospital built to take over from St Annadal and Maastricht University’s expanded medical faculty (Klijn, 2016; Knegtmans, 1992). Despite a degree of resistance, the Randwyck site broke ground in the early 1980s, and the Skillslab was among the first departments to move out of the city proper, taking up residence in a small red-brick building described to the author as being in ‘the middle of nowhere’. With the support of many clinicians, as well as the region’s political lobby, an ambitious new dean, Jacobus Greep, drove the construction of an advanced academic hospital (Klijn, 2016: 61–62). Those more involved in the teaching and learning of medicine were more sceptical. Students and faculty worried that this relocation betrayed the Basisfilosophie on which the university was built, in part, due to the school’s removal from the social space and vitality of the city. A vocal campaign group formed against the threat of a ‘concrete temple on Randwyck’ and the end of interdisciplinary cooperation (Bartholomeus et al., 1977: 5–6). The danger of Randwyck was that it would ‘hardly [be] in use outside office hours’ (Bartholomeus et al., 1977: 8). Instead, the group argued for greater integration with extant hospitals in Limburg, all of which should be involved in teaching and researching the fundamentals of primary care (Bartholomeus et al., 1977: 15).
There was radicalism in the early history of the Skillslab which has been somewhat betrayed by material and spatial changes to the medical faculty. The expansion of both the hospital and the medical school has necessitated a progressive movement away from the affective influence of first-line care and, instead, into an increasingly simulated version of clinical space. Following the construction of the teaching hospital, the Skillslab moved from its standalone red-brick building and into a number of rooms at the heart of the hospital complex. Students were able to access these spaces at any time, moving through the hospital in order to get there. This space was, however, reclaimed by the hospital and, in the mid-2010s, the Skillslab moved into its current home, a multi-storey, standalone building which had previously been used for hospital administration, and which is somewhat removed from the clinical spaces of the hospital. Designed with the express purpose of facilitating skills training, its pale green walls are adorned with anatomical illustrations, one of the few suggestions that this is a place for learning about the body. Both the common spaces and the teaching rooms were instead built to closely resemble the professional spaces that students are being trained to fill (Figure 4). Those involved with its design intended for this Skillslab to stimulate in students identification with the standards of the modern profession, ideals somewhat antagonistic to the more fluid doctor–patient distinctions imagined by the original designers of the Skillslab.

(a) Art in the corridors of the new Skillslab, c. 2019; (b) a simulated consultation room in the Skillslab, c. 2019. Both images courtesy of Anna Harris.
Today, students can no longer just come and go. Locked reception areas with sliding glass windows speak to increased reverence for patient privacy – a concept which has only crystallised since the late 20th-century – as do the thick curtains which hang inside the doors of the larger teaching rooms, the room dividers beside each of the examination tables within these spaces, and the lights which shine outside them in order to indicate whether rooms are in use. Practice rooms have been built to simulate a generic consultation room and are filled with all the materials necessary for primary care consultations. Best practice regarding hygiene is presupposed in the provision of disposable gloves, paper coverings for the examination table, disinfectant, and hand-wash stations (Figure 4). The only obvious difference between these educative spaces and the clinical spaces of the attendant hospital are the video cameras poised to film student practitioners for future review and critique of their consultations. Unlike at Semmelweis, the patient is an abstract presence in the Skillslab, even if they are only simulated by manikins or impersonated by other students.
Also unlike Semmelweis, laboratory skills and dissection are tangential elements of the curricula. Today, dissection courses are available for interested students but places are limited, tied to a specific PBL module (such as circulation and lungs, the musculoskeletal system, or the abdomen), and are taught in tandem with clinical considerations, imaging technologies (X-rays, magnetic resonance imaging, and CT scans) and surgical interventions (Maastricht University, n.d.). The post-vital body as a means to understand anatomical function abstracted from pathology or clinical intervention is absent in Maastricht and does not carry the same affective weight as in Budapest. As at Semmelweis, there is a haptic geography of the body, but Maastricht’s basis in clinical skill encourages students to move from the outside in, rather than the other way around.
Various approaches to patient simulation facilitate the development of clinical skills in conjunction with basic anatomical and physiological knowledge. When auscultating the heart or lungs, taking pulses, or testing reflex actions, students usually stand in for real patients – generally, following group introduction to the problem of the day, students move in pairs to the examination tables, taking turns to play patient and practitioner. Student reflection on their own bodies was initially intended to trouble the distinction between doctor and patient, illustrating students’ own potential for pathology. Introductions to more invasive procedures – such as techniques for effective blood taking, or gynaecology, obstetric, prostate, and breast exams – are routinely practised on manikins instead (Figure 5). In some cases, and usually only after extensive practice on these manikins, ‘simulated patients’ are introduced. They are specially trained to guide students’ hands during internal examinations and to advise them on both their physicality and communication.
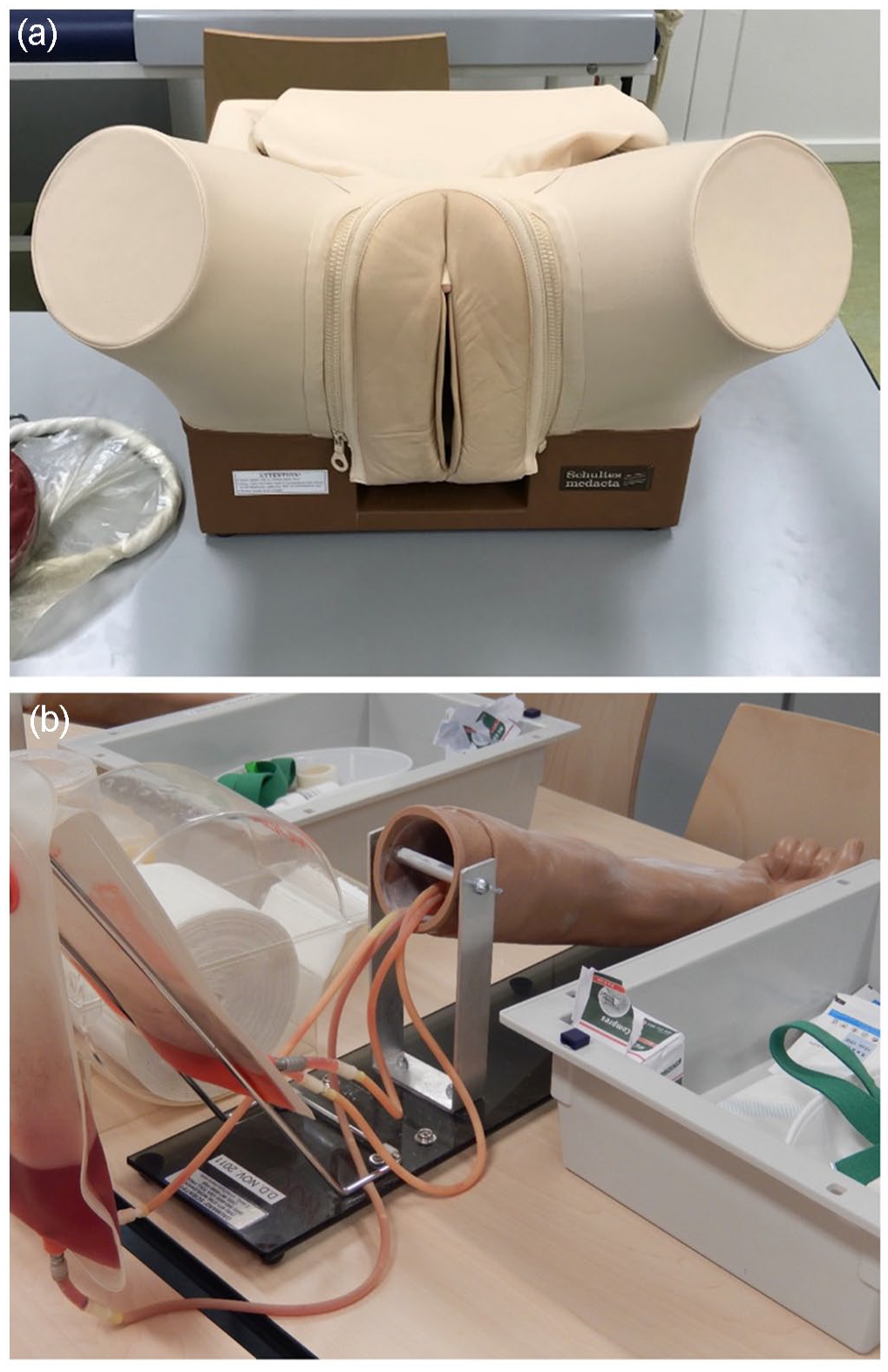
(a) Schultes Medacta obstetrics manikin, c. 2019; (b) simulator used for tutorials on taking blood, c. 2019. Both images courtesy of Anna Harris.
As is the case with the building itself, the material culture of medical education at Maastricht is entirely structured around simulation. As simulation assumes a more significant role in medical education, lively debates have grown up regarding its ethical and pedagogic value, including some consideration of the material affect of simulation (e.g. Underman, 2015, 2020). Despite claiming to offer a degree of universality, material simulations provide specific enactments of the body. As has been shown in Ericka Johnson’s (2008) work on obstetric manikins, the spatially specific enactment of obstetric practice is readily reflected in the material construction of medical simulators. As simulators travel, in this case between Sweden and the United States, they also bring standards and encourage practices that may not correlate with standards and practices found elsewhere. A similar juncture between clinical practice and the practices and epistemologies contained within teaching materials also occurs as these technologies age (Nott and Harris, 2020).
A rich vein of ethnographic research has likewise suggested that simulated patients and students simulating patients have the potential to present unreflexive and sometimes conflicting enactments of the patient body (e.g. Taylor, 2011). In this respect, medical simulation can only ever be partially successful in its mission to develop and assess embodied, sensory, and emotional judgement. This, as Ivana Guarrasi (2015: 114) has explained, is relevant in part because ‘the nonrepresentability of affect is at odds with the rational medical categories used to construct the simulated encounter’. Any such categorisation is necessarily bound to an imagined body and is informed by necessarily historic imaginaries of the body politic. In their performance of these publics, student bodies, simulated patients, and the inert bodies of manikins ignore the determinants of health and drivers of health-seeking which exist beyond biomedical frameworks. As Janelle Taylor (2014) has explained, simulated patients brought an end to frustrating encounters with patients in the clinic, interactions with those ‘‘‘crocks” [of shit] with plenty of complaints but no discernible pathology, and from whom students could not learn anything substantial’. Yet this also means that students only learn to attend to substantial, clinical concerns; precisely the opposite of what had been hoped for by the instigators of the Skillslab.
The pervasion of simulation in medical education complements Jean Baudrillard’s (1983) influential suggestion that the 21st century is the age of the simulacrum. As a seductive replacement of reality, simulation progressively erodes recognition of any external reality. This has a deeply dehumanising potential. Drawing from these ideas, Bleakley and Bligh (2009: 381) suggest that, in medical education, ‘simulation can act as a defence, against both the power of complex, live clinical environments and the reality of patients’ individualities that populate those environments’. The rhythmanalyst might, however, argue that while simulation intends to provide students with the means to attend to the cyclical rhythms of the living, social body, the socio-material spaces and practices of the Skillslab have actually limited students to a medicalised, linear abstraction of the corporeal and social rhythms of health and disease.
Conclusion
The histories of education at Maastricht and Semmelweis illustrate the various, unstable enactments of the body in biomedical education. Anatomy learned through cadaveric dissection is materially, practically, and ontologically distinct from that which is introduced alongside the clinical examinations of living participants, or simulations of them. Teaching materials, and the buildings which house them, encourage specific understandings of the patient body, but they also contribute to the production of the skilled, knowing bodies of clinicians, directing students in space, through movement and tradition. At times, the material cultures of medical education provide particular affordances which are difficult to change, or which leave limited space for alternative practices. Elsewhere, materials and spaces provide a symbolic reminder of the expectations which are placed upon young doctors. Developed, as a matter of course, in a previous time and another place, materials bind future practices to old epistemes. The architectural imposition of these two schools – and the ways in which their material histories continue to influence pedagogy – contributes to an enduring historical affect which effects and directs practice in the present. The known and knowing body, distinct but interacting bodily forms, are made in response to these material surroundings, and are made differently as a result.
Disconnection from our corporeal selves might be understood as a defining element of modern life and modernist medicine. Appropriately, at Semmelweis, a decorporeal epistemology of anatomy education is reified in materials and spaces, and in the pedagogies which they support. It is tempting to assume that all this provides is an affective introduction to a biomedical body that is alienated from the students’ own sensory perception, but this would deny the reflexivity of pedagogic practices at Semmelweis, as well as the distinct forms of embodied knowledge which derive from them. Despite this, the primacy of dissection and the material presence of post-vital bodies encourages the continued enactment of Cartesian philosophies of the body as well as Foucauldian histories of the clinic. Following Baudrillard’s 1977 essay of the same name, and in view of the trend towards simulation in medical education, Bleakley and Bligh (2009) have suggested that we might begin to ‘forget Foucault’. But when, as at Semmelweis, 19th-century ideals are palpably present in the material surroundings of the medical school, any such suggestion is clearly premature.
As a reaction to these historied materialities, and indicative of what he saw as the broader decorporealisation of space, and the attendant alienation of the body, in 1973 Henri Lefebvre wrote that ‘we need a kind of pedagogy of the body, its rhythms . . . a poetic practice, that attempts to vivify the entire body with all its rhythms and senses’ (Lefebvre 2014: 34–35). The medical school at Maastricht emerged from similar conclusions, initially siting its practice within the community and with greater attention to the social rhythms which were seen to contribute to ill health. Maastricht drew from the radicalism of the 1960s in an explicit attempt to break free from earlier approaches to medicine and, through community and clinical integration, to instead inculcate a fuller understanding of the body in society. Where Semmelweis’ Anatomy Department was constructed as an imposing statement of faith in the potential of biomedicine, the Skillslab’s more modest buildings are indicative of a self-reflective moment in the history of medicine. Although these ideals have been eroded by the development of the neoliberal university, the material construction of the Skillslab pre-empted and contributed to an ongoing trend in medical education, one which places greater emphasis on what student doctors can do rather than what they know. Simulation allows for this but was always intended to complement community integration. As a result of various pressures, patient simulation has, however, become increasingly prominent.
What links these schools is a shared struggle to teach the body in all of its slippery multiplicities. In medical education, as often in clinical practice, there is a broad material episteme that offers the material fixity and ontological assurance necessary for students to pass exams and, later, for physicians to treat their patients. Yet this material culture also interrupts sensory engagement with inconsistent, vital, social bodies. Attention to the ‘total body’ of the patient via the ‘total body’ of the clinician is fundamentally incompatible with the materials used in education, and the spaces in which it is taught. Access to the patient body is impaired by its necessary removal from social space, while the clinician’s embodied attention is necessarily refracted by epistemic and clinical technologies. What the modernist material pedagogies employed at Semmelweis and the postmodern simulations at Maastricht share is their necessary reliance on materials for the illustration of human form and function, as well as their inevitable shortcomings. Engaging with the historical affect of the medical school helps illustrate the implications of this. Although medicine is made in experiential relation to the material history which supports its reproduction, learning medicine also requires learning to submit to the historied spaces, places, and materials which do so much to shape medical futures.
Footnotes
Acknowledgements
For their openness and generosity, I am hugely grateful to the present and former staff and students at Semmelweis University’s Department of Anatomy and at Maastricht University’s Skillslab. Thanks, in particular, to Professor Andrea Szekeley for her hospitality in Budapest and for gifting me this book by Antal Szerb. Assistance from Valentine Delrue, Andrea Varallyay, Miklós Molnár, László Molnár and the staff at the Semmelweis Egyetem Központi Levéltár, and László Magyar and the staff at the Semmelweis Orvostörténeti Könyvtár és Levéltár was invaluable throughout. This article has benefitted greatly from the thoughtful consideration of colleagues at Maastricht University – Anna Harris, Rachel Vaden Allison, Andrea Wojcik, Dani Shanley, Joeri Bruyninckx and Jacob Ward all read earlier drafts – thank you all.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted as part of the ERC-funded ‘Making Clinical Sense’ project at Maastricht University (https://www.makingclinicalsense.com/, grant no. 678390). The revisions were completed while employed as part of the ERC-funded project ‘The Epidemiological Revolution’ (![]() , grant no. 947872).
, grant no. 947872).