
Abstract
This article explores the impact of the COVID-19 pandemic on the relationship between bodies, risk and mobility. Drawing upon ethnographic data from India, it is argued that measures taken by the Indian government to contain the spread of the pandemic link mobile bodies to the notion of risk which has profound consequences for the way in which people access and engage with public spaces in Indian cities. In this process, a new type of body – the risky mobile body – is produced. At the same time, these measures run into problems due to the volatile nature of knowledge about bodies and diseases that they rely on. While the mobility of the COVID-19 virus is a subject of public debate, the fluidity and open-endedness of mobile bodies makes them difficult to regulate. This mismatch between governmental logics and unknowable bodies constitutes a significant challenge for the fight against the pandemic.
Keywords
The COVID-19 pandemic presents governments and societies around the world with a difficult task: How can one enable the mobility of people and goods while disabling the mobility of a virus? To this end, various technologies and practices of regulating human bodies are deployed that aim to minimize the risk of infections. Norms of safe distances between bodies are defined, body temperatures are checked in public spaces, officegoers are advised to abstain from everyday commuting between their homes and their workplaces and long-distance travellers are temporarily quarantined at their place of destination. As a result of these profound measures, the meaning of mobility has changed dramatically on a global scale, creating a paradoxical situation that gives rise to numerous questions: While bodily mobility is generally a cornerstone of contemporary life, the mobile body now poses a threat to society. How do governments and their citizens deal with this apparent contradiction? What measures are taken to fight the spread of COVID-19 and what problems do they run into? Is the COVID-19 pandemic a sign of a paradigm shift, signalling that the ideal of mobility has reached an impasse? These questions reach deep into core beliefs of our times and show the extent to which the COVID-19 pandemic unsettles sureties and exposes the fragile architecture of the global ecumene.
I will address these questions by drawing on data that I collected while conducting a research project on transformations of urban transport in India brought about by the emergence of platform-based service providers like Uber and Ola. This research project was significantly affected by the outbreak of the COVID-19 pandemic in early 2020 and the massive restrictions on mobility and public life that were caused by the Indian government’s measures against the spread of the disease. The findings that I present in this article are therefore the result of a kind of ‘Accidental Anthropology’ (Pieke, 1995) that deals with an interference in ongoing fieldwork through a far-reaching and unprecedented event but is still undeniably coloured by my initial research interest in urban mobility. The article is based on qualitative data that I gathered by following media discussions about the COVID-19 pandemic, conducting interviews with various interlocutors and engaging in participant observation in the Indian megacities Delhi and Mumbai between March and July 2020. Due to the restrictions imposed by the Indian government, my ethnographic account is limited to my own experiences and interactions with people who hail from a broadly defined middle-class background.
Witnessing highly frequented and dynamic public spaces of metropolises like Delhi and Mumbai turned into almost entirely deserted landscapes prompted me to reflect on the meanings and complex forms of mobility and the repercussions of its absence. Observing the setting up of manifold measures to contain the pandemic and experiencing the complicated implementation of them made me think about the complex practical requirements of gaining knowledge about bodies and diseases. In this text, I bring these two lines of thought together and draw on contributions to a special issue of Body & Society about ‘New Biologies’ (vol. 22, no. 4) to make sense of ways of dealing with the COVID-19 pandemic in India. I link concepts of mobility and the body to outline the emergence of a new kind of body politics in the times of COVID-19 which I refer to as the ‘risky mobile body’. The production of this new type of body is rooted in a number of measures that aim to regulate bodily movements in public space. I argue that these measures face problems because they assume a singular, clearly knowable body while producing multiple forms of knowledge about bodies.
To present this argument, I will first reflect on the ambivalent relationship between the body, mobility and modernity and clarify what constitutes the new quality of restrictions on bodily mobility that have been implemented in the wake of the COVID-19 pandemic. Here, I introduce the concept of the ‘risky mobile body’ which I then elaborate with reference to the Indian government’s measures to curb the spread of COVID-19 in the following section. I understand these measures as attempts to trace, diagnose, order and isolate risky mobile bodies. To analyse the particular problems that these measures run into, I then draw upon Latour’s and Mol’s works on the production of knowledge about bodies and diseases. In the final section, I apply insights gained from these works to understand the problems of the Indian government’s measures to contain the spread of COVID-19 as a mismatch between the modern state’s dependency on facts and fixity and the fluidity and open-endedness of bodies.
Bodies, Diseases and Mobilities
One important reason why a global pandemic like COVID-19 is widely understood and treated as a cataclysmic event is rooted in the transboundary nature of viruses. Viruses are unstable and mysterious entities that problematize not only practices of containment but also practices of categorization. Especially the ability of viruses to travel within and through other beings unsettles a fundamental assumption about bodies as individuated, bounded entities that is characteristic of the modern era. Viruses can only exist as parts of other entities and thereby fundamentally compromise the modern concept of the body. Nonetheless, biomedical responses to pandemics still rest on a notion of defending the body against outer threats and often evoke images of a fortress under attack (Haraway, 1991; Martin, 1994).
In his highly influential work on the history of the concept of immunity, Cohen argues that this understanding of the body and diseases emerged in the 19th century in tandem with ideas of liberalism and individuality (Cohen, 2009). Viruses became understood as hostile ‘invaders’ and ‘parasites’ that take over the bodies of their hosts and rob them of that which is understood to properly belong to them. Therefore, Cohen argues that viruses constitute both biological and political actors (Cohen, 2011: 19) that mediate relationships between various cellular beings, including humans
Another taken-for-granted element of modernity that gets fundamentally challenged by the COVID-19 pandemic is the ideal of mobility. Understood as ‘a complex assemblage of movement, social imaginaries and experience’ (Salazar, 2017: 6), mobility has assumed such an omnipresence in our world that it is widely accepted as a cornerstone of modernity. Mobility is desired by people around the world and entire economies depend on it. In particular, transnational mobility is considered as a marker of class distinction that sets certain people apart from their more locally rooted counterparts (Meier and Lange, 2009: 16). Cities depend on mobility and are widely considered as dynamic places that offer unique opportunities (Smith, 2001), while less connected rural areas are associated with stagnancy and boredom. States of immobility are often equated with being stuck, excluded or even imprisoned, while the ability to move is considered as a prerequisite for personal progress. Moreover, mobility patterns exercise a significant impact on various localities by inserting them into translocal, transnational or global networks of exchange that shape experiences and aspirations (Schielke, 2020; Verstappen, 2017). It is against the backdrop of such a dominant image of a world in motion that the restrictions on human mobility that have been imposed in the wake of the COVID-19 pandemic have sent shockwaves around the planet.
However, even before the onslaught of the pandemic, mobility had never been unquestioned or unilaterally welcomed. Defensive stances towards mobility are likely to emerge where mobility is experienced as a deeply threatening transformative force. Mobility is then viewed as a source of disruption and alienation for people who consider themselves as the autochthonous population of a specific locale. As Appadurai has argued, global mobility is at loggerheads with the idea of a ‘singular national ethos’ that informs nation states worldwide (Appadurai, 2006: 4). We can see here the similarities between the modern biomedical conception of the body as a fortress to be defended against intruding microbes and the concept of the modern nation state that has to be defended against various ‘others’ (Cohen, 2009). This leads to a rather uneasy and ambivalent relationship between mobility and modernity that Cresswell has captured in the following statement: Mobility is both center and margin – the lifeblood of modernity and the virus [emphasis added] that threatens to hasten its downfall. (Cresswell, 2006: 21)
Cresswell’s choice of words is revealing since it points towards the crucial role of the body in debates about mobility. The body is both a mobile entity and a conduit for various movements of other entities, such as blood and viruses. The more threatening aspects of mobility therefore often become manifest in anxieties about bodies that move. For example, immigrants have time and time again been associated with the spreading of diseases (Molina, 2006; Shah, 2001). Irrespective of them actually being the carriers of infections or not, migrant bodies are often considered as dirty and polluted by the population of the receiving locality. Being a favourite target of xenophobic propaganda, they become explicitly depicted as a health hazard that needs to be eliminated by closing borders, denying visas or imposing other restrictions on their mobility. Moreover, the capacity to be physically mobile is increasingly circumscribed by technology that distinguishes eligible from ineligible bodies. Biometric identifiers such as fingerprints, iris scans and facial images are being used to police national borders and to grant mobility or to keep people in place. These technologies limit movement by producing ‘disqualified bodies’ (Aas, 2011: 341) and particularly target the bodies of marginalized and voiceless populations such as refugees (Lemberg-Pedersen and Haioty, 2020; Madianou, 2019).
In what regard then does the current COVID-19 pandemic mark a distinctly new development in the history of bodily mobility? I argue that – apart from their extraordinary scale, planetary reach and duration – the multiple restrictions on personal mobility that have been implemented in the wake of the pandemic amplify long-standing anxieties in regard to mobile bodies and transcend social differences. While previously anxieties about migrant bodies were primarily directed at the poor and marginalized and much less at members of the privileged classes, the COVID-19 pandemic renders all types of bodily mobility as risky. This, however, does not mean that social differences do not play a role in the degree to which people are affected by the restrictions on mobility brought about by the pandemic. A crucial differentiating factor is the freedom to choose one’s movement, which highly depends on a person’s social position. As Salazar has put it, ‘the ability to move (and the freedom not to move) is spread unevenly within countries and across the planet’ (Salazar, 2013: 552). In India, this can be seen in the differences between the immense hardships faced by labour migrants and the middle classes’ rather seamless shift to the home office after the imposition of a nationwide lockdown in March 2020 as a countermeasure against the spread of the COVID-19 pandemic (Harriss, 2020). This shows that, while the COVID-19 virus does not discriminate along the lines of class, the measures taken to curb the spread of the virus do. They shed light on the highly unequal abilities of people to decide when they move and when they stay put.
Due to the fact that people from different social backgrounds are equally at risk of getting infected with COVID-19 when moving out into the public, a new type of body emerges in the wake of the pandemic which I refer to as the ‘risky mobile body’. Under the conditions of the pandemic, basically all bodies that are mobile beyond the confines of the home are considered as risky. People leaving their homes to buy food or other essential goods expose their bodies to the risk of becoming infected with COVID-19. Even more at risk are people who travel longer distances by car, train or airplane and thereby are in contact with other bodies that can act as transmitters for the virus. Bodies of people who live in densely populated environments or who have no home at all are considered as risky by default, since they are constantly exposed to movements of bodies and flows of exchange, being literally ‘forced into constant motion’ (Kawash, 1998: 327). The COVID-19 pandemic thus creates a scenario in which mobile bodies are generally suspected as potential carriers of disease.
It is precisely this potentiality, this residual unknown that constitutes the very character of risk and makes mobile bodies such a source of anxiety in times of the COVID-19 pandemic. Every stranger’s body encountered in public space appears as a potential transmitter of the virus, but a total retreat from public space is impossible, even for members of the middle classes. Measures to fight the spread of the pandemic therefore aim at rendering mobile bodies readable, transparent and knowable. To gain a better understanding of how this works, I will now present examples of various measures taken by the Indian government to fight the spread of COVID-19 in the country. These measures render the risky mobile body a constant presence and thereby transform people’s everyday engagement with public spaces in Indian cities.
Regulating Risky Mobile Bodies in India
Official numbers of people infected with the COVID-19 virus started to rise in China and several European countries in February 2020, prompting governments of those countries to impose restrictions on their citizens’ mobility. After the number of COVID-19 infections increased in India in early March, the Indian government announced a nationwide lockdown on 24 March 2020, introducing various restrictions on people’s mobility that effectively brought public life to a sudden halt. Soon enough the dismal effects of these unprecedented measures became visible: Labour migrants employed in the country’s large informal work sector were left stranded without income and food in locked-down cities, and the already struggling Indian economy collapsed. It has been argued that the sudden imposition of such a strict lockdown would have been possible in Western countries but was out of touch with the Indian scenario, especially in regard to India’s high population density, severe social inequalities and inadequate access to medical services (Mittal et al., 2020). Due to the failure of this nationwide lockdown, the Indian government did not even return to this measure when a second, much more lethal wave of infections hit the country in March 2021. Instead, the central government left it to state governments to decide over the imposition of restrictions on movement. As a result, subsequent lockdowns have been much less drastic, geographically limited and linked to the number of infections in particular regions and cities.
Since it was not only impossible but also unfeasible to entirely put a hold on 1.3 billion people’s bodily mobility, the Indian government devised a number of measures to regulate people’s movements. These measures were designed to achieve the difficult task of enabling the mobility of people and goods while restricting the mobility of the COVID-19 virus. They can be categorized as tracing, diagnosing, ordering and isolating risky mobile bodies.
I will first take a look at the strategy to curb the spread of COVID-19 infections by tracing risky mobile bodies. The most important tracing tool utilized by the Indian government is the mobile phone app Aarogya Setu (lit. Bridge to Health). Shortly after announcing the nationwide lockdown, the Indian government developed this app and advertised it as a key instrument in the fight against the spread of COVID-19. The app works by collecting information about users’ past and current movements by means of multiple-choice questions and position tracing. After installing the app, users have to answer a number of questions about their recent travel history and state if they currently suffer from symptoms of COVID-19 such as cough, fever or respiratory problems. Based on this information, the app develops a colour coded ‘risk profile’ that assigns the respective user to one of three categories: green means no risk, orange means medium risk and red means high risk of being infected with COVID-19 (see Figure 1). The app also asks users to keep position tracking and Bluetooth activated on their mobile phone to enable real-time tracing of the user’s movements. By scanning a database of known infection cases, the app records if a user has been in contact with a person infected with COVID-19 and adjusts the risk profile accordingly.
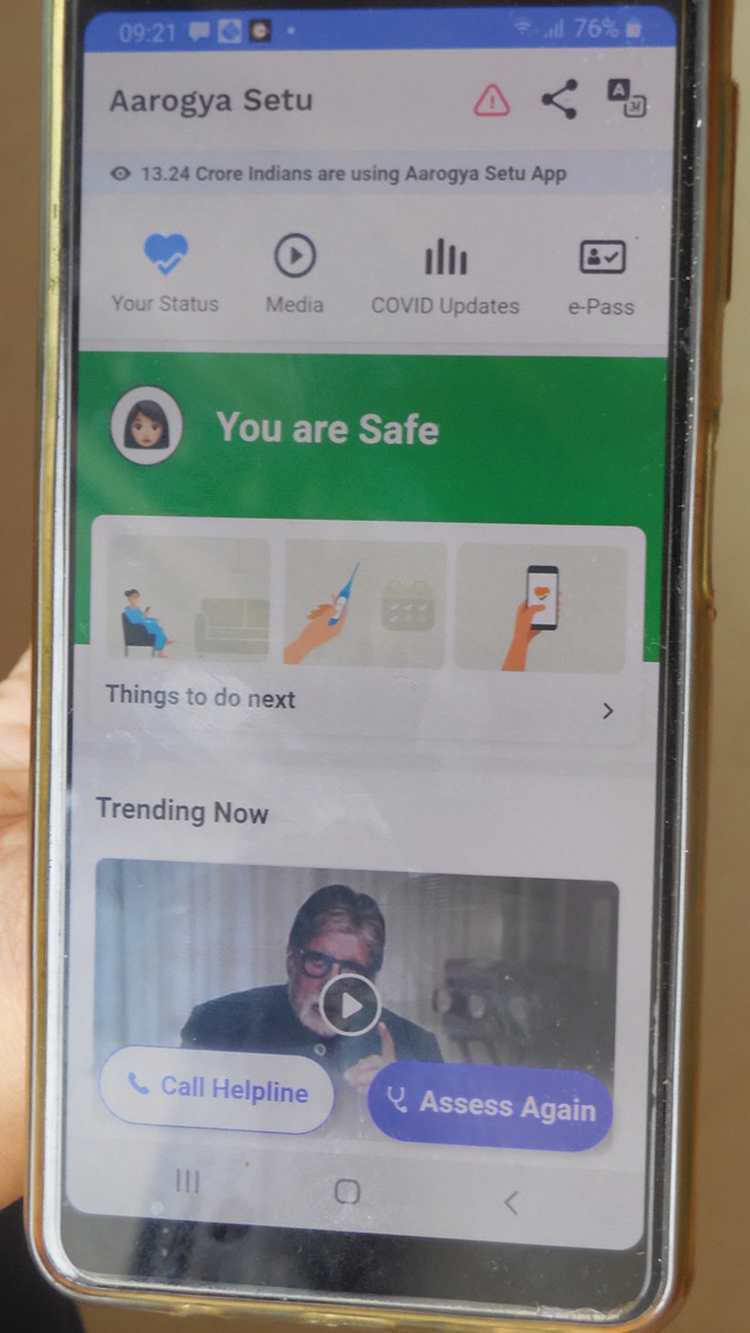
Aarogya Setu App showing the risk profile of the mobile phone user. (Photo: Author)
During the first phase of the nationwide lockdown that was declared in March 2020, the Indian government made it mandatory for all people residing in India to install the app on their mobile phone. While there was no mechanism of checking if people complied with this new rule, it effectively became mandatory for people who intended to travel long distances by train or airplane. When train services reopened in late May 2020, the government announced that travellers would only be allowed to board a train or airplane if they had installed the app on their mobile phones. Only if the app showed that the user was at low risk of having been infected with COVID-19 was he or she allowed to board a train. The app thus particularly targeted mobile bodies that were expected to be at a significantly higher risk of getting infected with COVID-19 during their journey than immobile bodies.
Another strategy against the spread of COVID-19 is diagnosing risky mobile bodies. To this end, body temperature checks are being undertaken at places where huge groups of people regularly congregate, including shopping areas, offices, train stations and airports. The body temperature of people who move through these places is usually checked by security personnel through the use of an infrared thermometer, a small pistol-like handheld device that is directed at the forehead or wrist of a person for some seconds to measure the body temperature (see Figure 2). Since fever is one of the common bodily symptoms of an infection with COVID-19, this practice is expected to provide a reliable indication if a person is infected with COVID-19 or not. This quick and non-invasive practice of checking the body temperature of mobile people has become a standard method of granting or denying access to public spaces in many Indian cities. It promises to assess the actual risk posed by individual mobile bodies in a comparatively short amount of time.

Body temperature of passengers arriving from Delhi getting checked at Mumbai Central train station in May 2020. (Photo: Author)
A third strategy of fighting the COVID-19 pandemic consists of ordering risky mobile bodies by enforcing the observance of social distancing rules. At the beginning of the nationwide lockdown in March 2020, the Indian government advised citizens to always maintain a minimal spatial distance of three feet to other people since most medical experts agreed that the COVID-19 virus was unable to cover a distance of more than three feet outside a host body. This measure is essentially a strategy of establishing a mode of ordering bodies in space with the aim of minimizing the risk of infections. It resembles previous measures taken to fight the spread of infectious diseases by targeting ‘pathogenic spaces’ where ‘the moving body is put at risk by its very proximity to the blood, sweat and discharge of currently or previously inhabited bodies’ (Newman et al., 2016: 157). One example of this strategy are new queuing practices that were quickly implemented after the start of the nationwide lockdown to ensure that social distancing rules would not be violated when people left their homes to buy essential goods like food or medicine. These new rules fundamentally transformed the usual shopping practices of Indians that gave little attention to the maintenance of spatial distance between bodies. Before the outbreak of COVID-19, shops in urban India were usually densely packed with customers who had no choice but to literally rub their bodies against each other to make their way through narrow lanes past other customers, helpers and salespeople. With the government’s order to follow social distancing rules, this practice of shopping was no longer feasible and had to be reformed, which spurred creative solutions. Shop owners, who were obliged by the government to ensure that their customers observed social distancing norms, marked positions where customers were to stand while waiting in line in front of shops with painted circles or stickers on the ground, each approximately three feet away from the other (see Figure 3). This mode of spatial ordering was expected to minimize the risk of infections by ensuring that the distance between mobile bodies exceeded the maximum distance that the virus could travel without a host.

Customers standing in a queue in front of a supermarket in Matunga, Mumbai in June 2020. Note the stickers on the ground marking the position where each customer is expected to stand. (Photo: Author)
A fourth strategy consists of isolating risky mobile bodies from non-risky immobile bodies by implementing different forms of quarantine. After the outbreak of the COVID-19 pandemic in India, the government used two modes of quarantine, institutional quarantine and home quarantine. Institutional quarantine was ordered when a person exhibited symptoms of COVID-19. People diagnosed with COVID-19 were usually quarantined inside hospitals, but due to the quick spread of COVID-19 in India and the resulting lack of spatial capacities in overburdened hospitals, other confined environments such as halls or large grounds were also used. The measure of home quarantine targeted risky mobile bodies. This type of temporary quarantine had to be observed by people who travelled long distances by train or airplane even if they did not exhibit symptoms of an infection. Since the incubation period of COVID-19 was calculated at approximately 14 days, travellers had to observe a 14-day quarantine in a hotel or at their place of residence upon arrival at their destination. If travellers exhibited symptoms of an infection with COVID-19 during their quarantine period, they had to report to the authorities and get treated. If they did not develop symptoms, they were allowed to leave their homes again after the end of their 14-day quarantine. When the responsibility of deciding over the imposition of anti-COVID-19 measures shifted from the central government to state governments in late 2020, quarantine rules started to differ significantly according to region and became subject to constant changes depending on the number of infections in a particular state or city. Just like the strategies described above, the strategy of isolating mobile bodies rests on the assumption that mobile bodies are at a significantly higher risk of getting infected with COVID-19 than immobile bodies that remain confined to non-public spaces.
These various measures are now applied to all mobile bodies in India. They enact the mobile body as a body that is perpetually at risk of getting infected with COVID-19 and is therefore in need of constant and strict regulation. This situation might lend itself to a rigid, top-down reading of Foucault’s concept of biopolitics (Foucault, 2008) exercised by an authoritarian state upon its population, but this would miss the fact that the Indian government’s measures against the spread of COVID-19 depend on practices of producing knowledge about bodies and diseases that are multiple, patchy and fraught with contradictions, omissions and blind spots. This volatility of knowledge production has been a core concern of works conducted in the interlinked fields of assemblage thinking, science and technology studies and actor-network theory. In the following section, I will draw upon two particular works by Latour and Mol that help to understand the predicaments of measures against the spread of COVID-19 in India.
Producing Competing Knowledges about Bodies and diseases
Assemblage thinking, actor-network theory and science and technology studies are terms that have been used to denote scientific approaches that differ in terms of their historical development and disciplinary location, but exhibit strong similarities in respect to their intellectual approach. While the roots of science and technology studies and actor-network theory can be traced to a common group of scientists interested in questions about the production of scientific knowledge (Bijker et al., 1987), assemblage thinking emerged as a separate intellectual endeavour pursued by the philosophers Gilles Deleuze and Felix Guattari (Deleuze and Guattari, 1987). Nonetheless, it has been argued that ‘there is little difference between Deleuze’s agencement (awkwardly translated as “assemblage” in English) and the term “actor network”’ (Law, 2009: 146). All of these approaches decentre the human and radically expand the notion of what can be considered as an actor, committing to relationality as a guiding principle in the structuring of worlds. These works ask how seemingly disparate entities form temporary associations that produce further associations.
The case of a virus infection like COVID-19 particularly lends itself to such an approach because it constitutes the perfect example of an assemblage or actor-network, defined as a productive association of heterogenous entities (Müller, 2015: 28–29). The association of a virus and a human body produces a sick body which, if getting in contact with other bodies by being mobile, produces further sick bodies. According to current scientific consensus about the pandemic, the bodies of humans (and possibly also animals) constitute the most effective device to mobilize the virus and allow it to spread across huge populations. Since a vaccine that prevents the COVID-19 virus to enter into a host–parasite relation with a human body did not exist at the time the pandemic broke out in early 2020, measures to fight the pandemic focused on practices of minimizing the opportunities for virus–body assemblages to emerge by regulating mobile bodies. Although effective vaccines against COVID-19 have been developed since then, vaccination drives of this order take time and large sections of populations worldwide still remain vulnerable to the disease. Therefore, at the time of revising this text in July 2021, implementing measures that aim at regulating mobile bodies still remains the dominant strategy to restrict the spread of the pandemic. These measures depend on knowledge about mobile bodies and about the mobility of the COVID-19 virus.
The crucial problem that haunts these measures is that they rely on knowledge that requires time and the mobilization of numerous actors and resources to assume the status of unquestioned facts. It also requires settings in which the number of acting entities that take part in the production of knowledge can be limited and controlled. These characteristics of knowledge-producing assemblages have been studied by Latour and Mol. Their works help to understand the specific challenges that complicate the fight against the spread of the COVID-19 pandemic.
For his influential study on the production of scientific knowledge, Latour conducted research in a laboratory in California. He applied a sociological perspective to the work of natural scientists and observed multiple processes of literary inscription, transcription and translation that transform suggestions and statements into ‘scientific facts’. He argued that science takes place in an ‘agonistic field’ (Latour and Woolgar, 1986: 237) in which various truth-claims compete with each other. In this messy and painstaking process, arguments are transformed ‘from an issue of hotly contested discussion into a well-known, unremarkable and noncontentious fact’ (Latour and Woolgar, 1986: 76). By the time a statement has been sufficiently stabilized to constitute a new truth, the social has been erased from the process of its construction (Law, 2009: 144). This practice of erasure – which Latour later referred to as the practice of purification (Latour, 1993: 10) – enables the claim that scientists do not produce knowledge but ‘discover’ allegedly universal laws of nature. The social aspect of producing knowledge thus disappears inside the ‘black box’ (Latour and Woolgar, 1986: 150 13n) of science and the confined space of the laboratory. Latour stresses that irrespective of this subsequent erasure of the social, the process of producing scientific knowledge is always deeply social.
The second work that helps understand measures against the spread of COVID-19 is Mol’s study of the production of knowledge about bodies in biomedical practices (Mol, 2002). Based on a field study conducted in a Dutch hospital, Mol argues that in biomedical practice, healthy and sick bodies are enacted through the use of various practices, technologies and instruments such as looking at blood vessels through microscopes, listening to narratives of patients or experiencing the sensation of pain. By paying attention to the production of various knowledges about bodies through different practices, Mol develops a praxiographical approach that considers disease as something that is never abstract from the practices that make it perceivable (Mol, 2002: 31–32). Instead, she focuses on the ‘practicalities of doing disease’ (Mol, 2002: 31) that hinge upon the cooperation of a multitude of human and non-human actors. These various practices of producing knowledge about a body often come to very different conclusions. For example, a patient may complain about pain in the legs, but a pathological analysis might come to the conclusion that there is no problem with the arteries in the legs. Such conflicting notions about the ontological status of a body can significantly complicate the therapy process, which is why disparate knowledges about bodies have to somehow be reconciled. The crucial point of Mol’s argument is that biomedical practices are multiple and always produce a patchwork of different knowledges about bodies.
In the wake of the COVID-19 pandemic, we are witnessing the expansion of two comparatively enclosed and controlled institutions into the public realm: Latour’s laboratory expands into public discourse and Mol’s hospital expands into public space. Both these expansions expose the messy and patchy practices of producing knowledge about bodies and diseases to a wider public. Additionally, these expansions complicate the identification of effective responses to the COVID-19 pandemic by including a plethora of acting entities into the process of knowledge production. The volatile interaction of various acting entities inside the setting of the laboratory and the hospital becomes a public affair long before these practices have been reconciled and translated into accepted ‘scientific facts’ and agreed-upon diagnoses. This makes the production of knowledge about mobile bodies and a mobile virus in times of the COVID-19 pandemic an especially uncertain and dynamic affair.
Let me illustrate these points by returning to the Indian government’s measures to fight the spread of COVID-19 by regulating risky mobile bodies in the following section. These measures grant citizens conditional mobility. They acknowledge people’s need to access public spaces but regulate the terms of access. However, the production of knowledge about risky mobile bodies is a highly dynamic interaction between various human and non-human actors that fosters various different ‘bodies of knowledge’. In the context of the COVID-19 pandemic, these interactions assume a particular dynamic because they do not take place in enclosed and controlled environments like laboratories or hospitals but involve various publics. This increases the likeliness of multiple different bodies of knowledge to emerge and act in conflict with each other.
Uncertain Bodies of Knowledge
The strategy of tracing risky mobile bodies through the Aarogya Setu mobile phone app has run into a number of problems since its inception. For one, data security experts have severely criticized the app for inviting misuse and impinging upon basic rights to data security (Kapur, 2020). In this regard, Aarogya Setu is just the latest initiative aimed at improving aid and governance through the use of digital technologies that have proliferated in India in previous years and provoke serious concerns about data privacy and security (Jacobsen, 2014; Sandvik, 2020). Moreover, the app is unable to trace risky mobile bodies if position tracking and Bluetooth are deactivated on the mobile phone. The risk status of a user is then calculated solely on the basis of the questions answered by the user after installing the app which cannot be verified. This leaves significant room for users’ agency in deciding which information they share with the app. Furthermore, the app is developed only for newer phones that use the Android mobile operating system. On older mobile phones that do not operate with Android, the app does not work. which makes it impossible for some people to get registered. Lastly, train passengers are seldomly checked if they have actually installed the app on their phones. When I travelled from Delhi to Mumbai during the nationwide lockdown in late May 2020, neither was I checked nor did I witness any other passenger getting checked for having installed the app on their mobile phone.
A particularly striking problem with the app concerns the question of what it considers as a body in the first place. The app is prone to produce inappropriate risk profiles due to its limited ability to trace actual bodily interaction. It calculates bodily proximity on the basis of the proximity of mobile phones. which runs into problems when applied to the spatial distribution of users’ bodies. For example, residential skyscrapers that have multiplied in Indian metropolises over the past decades constitute a particularly problematic environment for the app. If one person in such a building gets infected with COVID-19 and reports this in the app, other residents’ risk profiles also get adjusted if their mobile phones came into the Bluetooth range of the infected person’s mobile phone. Although residents’ bodies might have been separated by concrete floors and doors, the app records them as having interacted with each other. Conflating interactions between mobile bodies and data exchanges between mobile phones, the app produces ‘false positives’ (Clarance, 2020). To make bodies accessible for large-scale statistical analysis and logics of governance, the app creates ‘digital bodies’ (Lupton, 2017) but in this process of transformation, crucial elements of bodily interaction and spatial movement get lost. This leads to a mismatch of two different bodies of knowledge – big data and spatial movements – and consequently fosters distorted results. It is one example of the multiple ways in which measures to regulate risky mobile bodies rely on the production of unavoidably partial knowledges about bodies.
Many times, the checking of mobile bodies’ temperature also does not produce results that comply with the need for exact numbers and statistics. Since the temperature of a body changes according to the temperature of the environment through which it moves, the readings of infrared thermometers often produce unreliable data, as I learned from two cases in Delhi. Ritika, a 27-year-old woman who works in a public-sector office in Delhi, has to undergo a temperature check to enter the building in which her office is located. After the COVID-19 outbreak in India, the company had instructed its security personnel to check the body temperature of every employee of the company and deny entry to everyone whose temperature exceeded the limit of 100 degrees Fahrenheit. When Ritika wanted to enter the building to start her working day, the device showed her body temperature to be above 100 degrees Fahrenheit. Since she did not feel feverish, she concluded that her body temperature had increased due to the walk she had taken in the hot Delhi weather to reach her office. Nonetheless, the security guard said that he could not let her enter if her body temperature exceeded the defined limit. After sitting under the shade of a tree for a while, she underwent several further temperature checks until the infrared thermometer finally produced a reading within the defined temperature limit and she was allowed to enter. A similar account was given by Avinash, a man in his mid-50s who had travelled to his workplace in a taxi and sat next to a window which was exposed to the sun. Inside the taxi, his body had heated up so much that the thermometer of the security guard indicated its temperature to be above 100 degrees Fahrenheit. Like Ritika, he had to sit at the entrance of the office complex where he worked until his body temperature had decreased enough to produce a satisfactory reading.
These examples point towards a mismatch between modernity’s appetite for clearly defined boundaries and the porous relationship of bodies and their environment. Expecting a neatly compartmentalized and clearly readable body but encountering a much more complex, open-ended entity, the checking technology failed. Similar problems occur with biometric technologies such as fingerprint scanners that are increasingly used in various institutional settings in India (Rao, 2018). These technologies increasingly define what a ‘normal’ body is and governmental practices are adjusted to these norms (Lupton, 2017). Bodies that fail to match these norms produce ‘false readings’ and are rejected by the newly created socio-technical regime. The authority with which technoscientific assemblages are invested and the ways in which they present their results as beyond doubt makes it immensely difficult to challenge them (Amoore, 2019). At the same time, people constantly devise various ways of manipulating their bodies to navigate the blind spots of technologies, such as cooling down their bodies before check-ups to produce unsuspicious body temperatures. 1
Similar issues can be observed with the Indian government’s measure of isolating people who travel long distances by train or airplane. During the immediate response to the outbreak of the pandemic in May 2020, people who travelled across state borders were obliged to observe a 14-day period of home quarantine after the completion of their journey. At their destination, government officials marked the bodies of passengers by applying a stamp with the date of arrival on their hand. However, this technique of marking bodies was unreliable, as I personally experienced after travelling from Delhi to Mumbai on a train in late May 2020. After washing my hands two, three times, the stamp was barely visible anymore, leaving my risky mobile body unmarked for the remaining duration of my home quarantine. Again, we see here a mismatch between a technology that is expected to ascribe fixity and unambiguity to bodies, but gets rendered ineffective quite literally by their fluidity.
The establishment of new queuing practices is complicated by varying opinions on the mobility of the COVID-19 virus. As I have mentioned above, the new queuing practices that fundamentally transformed the shopping experience of Indians since the implementation of the nationwide lockdown are based on the assumption that the virus can only traverse a distance of up to three feet outside a host body. Ordering customers’ bodies to always maintain a distance of three feet was therefore expected to eliminate the risk of infections. However, soon after the new queuing rules were established, virologists started expressing doubts about the government’s social distancing norms. They argued that maintaining three feet distance to others’ bodies would not suffice to ensure safety and eliminate the risk of getting infected. Assuming that the COVID-19 virus travels via small droplets that infected bodies disperse through exhalation, some scientists argued that the virus was capable of travelling a distance of up to 20 or even 27 feet, rendering the newly established queuing practices ineffective. These differing opinions among scientists about the mobility of the virus were communicated via various media outlets, including social media (see Figure 4) and newspapers (The Hindu, 2020; Times of India, 2020), demonstrating that knowledge about the mobility of the virus was still subject to negotiations between various actors and had not yet settled into ‘scientific facts’. It also shows that various truth-claims that were formerly confined to a rather segregated scientific discourse now enter the public sphere where they play out in an agonistic field that is populated by a number of actors. In other words, the volatile practices of establishing ‘scientific facts’ in Latour’s laboratory are not contained anymore, but play out in the public sphere. Here, they mesh with popular conceptions of ‘network immunity’ or ‘immuno-cosmopolitanism’ that consider exposure of the body to microbes as a condition to achieve good immunity or regard the avoidance of infection as a futile endeavour to begin with (Davis et al., 2016). As a result of these multiple ideas about immunity and public contestations of various statements, uncertainty about the mobility of the virus and the likelihood of getting infected increases.
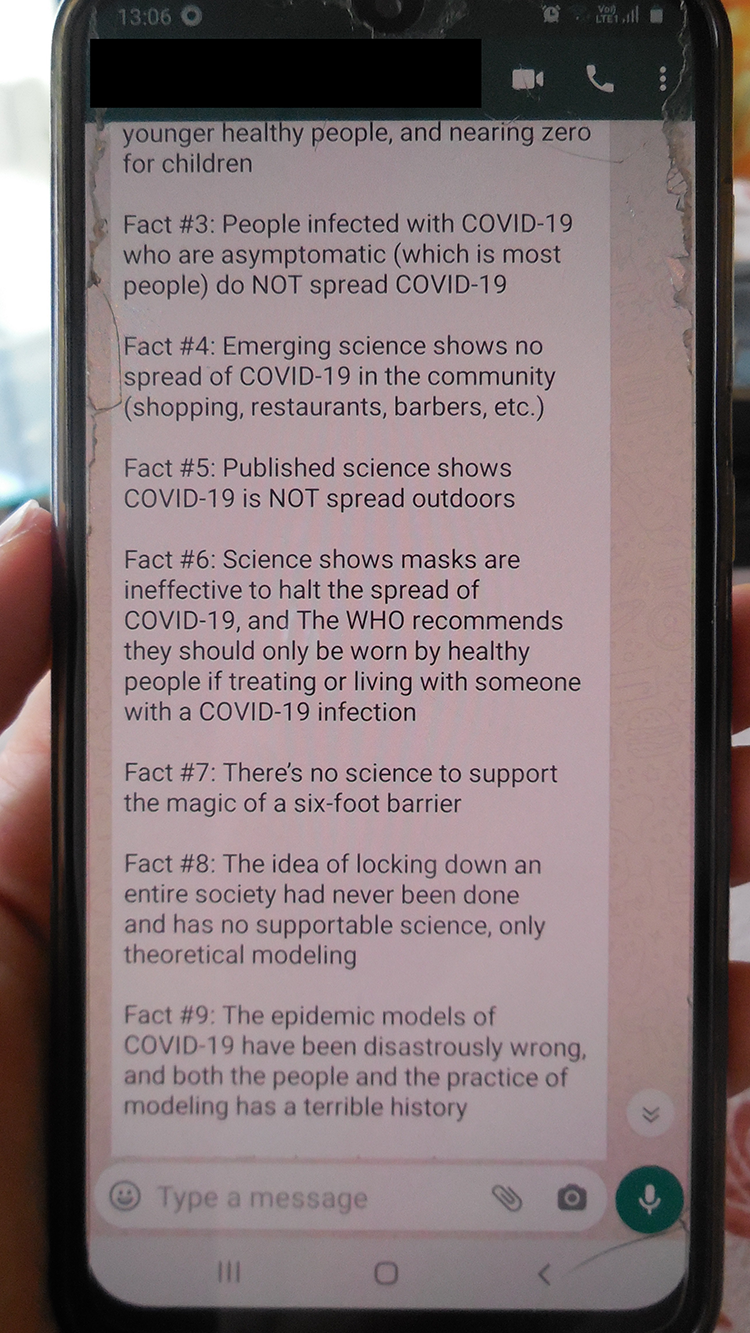
WhatsApp post shared by an Indian user in June 2020 that questions several knowledges about the COVID-19 pandemic, including social distancing norms communicated by the Indian government at that time. (Photo: Author)
These are just some instances of a severe dilemma that underlies anti-COVID-19 measures worldwide. Measures that have been devised to reduce the threat posed by the pandemic operate within the logic of modernity’s obsession with facts and fixity, but they encounter a world made up of flows, negotiations, exchanges and networks. The result is a Sisyphean attempt of delineating a clearly demarcated territory within a swirling ocean. Trying to reduce the risk of infections by producing knowledge about mobile bodies leads to the production of multiple bodies that are not easily reconciled and constantly come into conflict with each other. Faced with the task of unambiguously defining perpetually unruly bodies, the various measures to contain the spread of the COVID-19 pandemic often fall short of the immense expectations placed upon them.
Conclusion
The COVID-19 pandemic constitutes a threat to the health of millions of people worldwide, but in addition to the loss of lives, it causes lasting transformations in public life and state–citizen relations. At the heart of these transformations lies the body and the various practices of understanding, governing and using it. The COVID-19 pandemic fundamentally transforms established notions of bodily mobility, and the various measures taken to curb the spread of the disease involve wider publics in previously enclosed and controlled practices of producing knowledge about bodies and diseases. Both these processes heighten uncertainties because they unsettle foundational beliefs and unquestioned practices. The ideal of bodily mobility lies at the core of the contemporary global order and the authority and fixity of scientific knowledge forms the ideological basis of modernity. By heightening anxieties about bodily mobility and making scientific knowledge appear contradictory and patchy, the COVID-19 pandemic exposes the fragility of a globally connected world and the modern constitution.
In this text, I have outlined how the fight against the spread of the pandemic is complicated by two main obstacles. The first one is a basic need and desire for bodily mobility. Notwithstanding the risk of infections, people, localities and economies continue to depend on the movement of bodies and bodily interaction. This paradox turns quotidian bodily mobilities into a threatening endeavour and links mobile bodies to the notion of risk. The resulting anxieties about mobile bodies transcend differences of class that characterized long established anxieties about migrant bodies. I have referred to this new quality of anxieties about mobility as the emergence of a new type of body, the risky mobile body. This new type of body gets enacted in various measures that aim to contain the spread of COVID-19, for example, when a mobile phone app adjusts the risk profile of a user, when security personnel check the body temperature of officegoers at the entrance to their workplace or when bodies of customers are ordered to maintain spatial distance from each other according to new queuing norms. All of these interventions establish the risky mobile body as a new ordering principle of everyday life in the times of COVID-19.
The other obstacle in the fight against the spread of the pandemic is conflicting knowledges about mobile bodies. While practices of producing knowledge about bodies and diseases are already contested, multiple and contradictory in the contained environments in which they usually take place, the COVID-19 pandemic renders them especially volatile by exposing them to the wider public and an expanded range of actors. As a result, attempts to contain the pandemic are subject to changing knowledges about risky mobile bodies and the mobility of the COVID-19 virus. In this text, I have taken a closer look at measures taken by the Indian government and the specific problems they run into. These measures represent strategies of tracing, diagnosing, ordering and isolating mobile bodies that aim at immobilizing the COVID-19 virus. Their implementation is severely complicated by problems in producing reliable and unambiguous knowledge about mobile bodies and the mobility of the COVID-19 virus.
Irrespective of the dynamic trajectory of the COVID-19 pandemic since its sudden outbreak in early 2020 and its unforeseeable further development, there are some lasting and universally applicable insights that can be drawn from this tragic event. The various issues that haunt attempts to limit the spread of the disease demonstrate that bodies are not docile devices, but mobile, complex, multiple and open-ended entities that are difficult to domesticate. They reach out into their environment and remain porous to the various ebbs and flows of the world that they inhabit. Resisting governments’ demands for standardization, boundary making, enumeration and statistical fixity, they foster various improvisations on the ground. This tension between logics of governance and somatic realities will continue to complicate measures to contain the spread of COVID-19 not only in India, but in various countries around the world.