
Abstract
Health committees link formalised health services and the community. However, ‘how, why, and for whom’ health committees work warrants further exploration. This article presents the development of a middle-range theory for how health committees work for building community capacity for health. Resulting programme theories from a realist evaluation in Uganda were synthesised for demi-regularities and supplemented by four key informant interviews – substantive theories were used to help explain the findings from the case studies to develop the final middle-range theories. Eighteen existing programme theories and 47 supporting context-mechanism-outcome configurations were synthesised into four middle-range theories for how health committees work for community capacity building for health at the individual, organisational, community and societal levels. The middle-range theories developed in this study provide important insight for those implementing health committees. Given the little guidance available for developing and refining middle-range theories, this study provides transparent methodological processes, which may assist future research.
Introduction
Community engagement and participation in health activities are essential to support programming that is both user-friendly and acceptable (Dada et al., 2023). Health Committees (HCs) – otherwise known as community coalitions, village committees and community groups (George et al., 2015) – are health-focused community groups, which serve as a formal link between the community and health services. They serve to manage and coordinate health activities and civil society strengthening (George et al., 2015; Karuga et al., 2022). The primary purpose of HCs is thus to facilitate the participation of community members in decision-making on the provision of health services, towards achieving better health outcomes within their communities (Gilmore et al., 2016a; Karuga et al., 2022).
HCs have grown in numbers over recent years. Today, HCs are prevalent in many low-income country contexts, having been introduced by governments and/or organisations (McCoy et al., 2012). The scope of HCs can vary, spanning family planning (Capurchande et al., 2015), safe motherhood (Brazier et al., 2015), HIV programming (Lunsford et al., 2015; Mburu et al., 2013) and/or water and sanitation (Waterkeyn and Cairncross, 2005). However, HCs are not limited to a particular health condition, and their mandate is often based on the needs of a given area. For example, some HCs focus on community accountability (Molyneux et al., 2012), community monitoring (Svensson and Bjorkman, 2007) or health facility governing (Kessy, 2008). While the purpose and scope of an HC may vary depending on health condition or context, HCs commonly share a formal structure; include representatives from the community, health facility, and local leadership; manage the relationship between health services and the community (George et al., 2015; Karuga et al., 2022); drive community involvement with health activities; and assist with supervision and support of the health centre and its community-level activities (Abimbola et al., 2016).
The benefits of HCs are well-documented throughout the literature. For example, HCs have successfully advocated for resources, negotiated access to healthcare and monitored the use of funds and quality of care, thus ensuring a feedback mechanism between the health provider and service users (Karuga et al., 2022; Lodenstein et al., 2017b). Studies have also shown that HCs can be effective in raising awareness, health promotion education, referrals and follow-up, workload diffusion among community health actors and in making community workers feel more supported (Lunsford et al., 2015). The factors that influence the effectiveness of HCs, however, are complex. For example, a recent review by Karuga et al. (2022) highlights the complexity of power dynamics, and equitable gender participation and representation within HCs, as challenges when implementing HCs. While the potential benefits of HCs are evident, the explanation of how, why and under what conditions HCs work warrants further exploration.
Building community capacity for health or increasing ‘community groups’ abilities to define, assess, analyse and act on health concerns of importance to their members (Labonte and Laverack, 2001) is viewed by many as a critical step to addressing health inequities at the community level (George et al., 2015; Khan et al., 2021; Lodenstein et al., 2017a). Specifically, community capacity building for health is seen as a way to strengthen health service delivery by, for example, increasing community members’ capabilities in accountability and governance. Accordingly, community capacity building for health can be viewed as an intended outcome and a by-product of well-implemented community programmes (Gibbon et al., 2002).
Given the growing frequency of use of HCs across varying health conditions and contexts, and the role of HCs in brokering the participation of community members in decision-making for health services, there is a need to understand better how and why HCs work (or not) for capacity building for health. Moreover, there is a need to understand how contextual factors influence how HCs work across different settings (Brazier et al., 2015; Lunsford et al., 2015). Exploring the theories of how and why HCs function, in particular, may lead to a deeper understanding and more practical recommendations for the implementation of HCs across the diverse settings in which they are used. Furthermore, ensuring that theory is developed in such a way that it is easily transferable across the settings in which HCs are implemented could generate transferable learnings for how to maximise the potential of HCs globally.
Building on the methods reported by Gilmore et al. (2016b, 2019), Gilmore (2018), and previous results in the form of programme theories (PTs) of how HCs work (see: Gilmore (2018)), this study presents the final phase of a realist evaluation (RE) process by exploring how HCs work across two case studies in North Rukiga, Uganda. Specifically, synthesis and refinement of PTs across these two case studies are used to develop a middle-range theory (MRT) for use across diverse settings where HCs function. In addition, while there exist quality standards and reporting guidelines for completing REs (see for example, RAMESES II, Wong et al. (2016, 2017)), there remains a lack of guidance for how an MRT should be developed within RE. Therefore, this study also sought to provide a transparent description of how an MRT was developed, as well as reflections that may prove useful for the development of an MRT within future RE. A quick reference of all abbreviations used in the article can be seen below (see Box 1).
Quick reference box for abbreviations used.
Methods
To explore how HCs work and build community capacity for health, an RE was undertaken across two case studies in North Rukiga, Uganda. RE is a theory-driven form of evaluation that focuses on discovering ‘what works for whom in what circumstances’ (Pawson and Tilley, 1997). RE thus allows for uncovering an explanation of how interventions work, or not, by the development of theory in the form of PTs and, in some cases, MRTs (Pawson and Tilley, 1997). PTs seek to explain how an intervention may work within specific context or circumstances (Pawson and Tilley, 1997). To develop PTs, the conceptual tool of Context Mechanism Outcome Configurations (CMOCs) is used to identify under what contextual conditions mechanisms are triggered to generate a given outcome (Wong et al., 2017). These CMOCs are then synthesised to develop and refine PTs.
An MRT, on the contrary, sits at a higher level than day-to-day theories (i.e. PTs), but below the level of substantive theory (Merton and Merton, 1968; Wong et al., 2017; see Figure 1). MRTs can explain ‘what works for whom in what circumstances’ in a way that may be transferable and generalisable across settings (Wong et al., 2017). MRTs allow for further testing and refinement in future applications and research (De Brun et al., 2019) to capture a wide spectrum of possible circumstances. There is, however, no specific guidance to be followed within MRT development. However, the approach of applying substantive theory to RE findings, to allow for deeper understanding and explanation, was previously demonstrated by Jack and Linsley (2021).
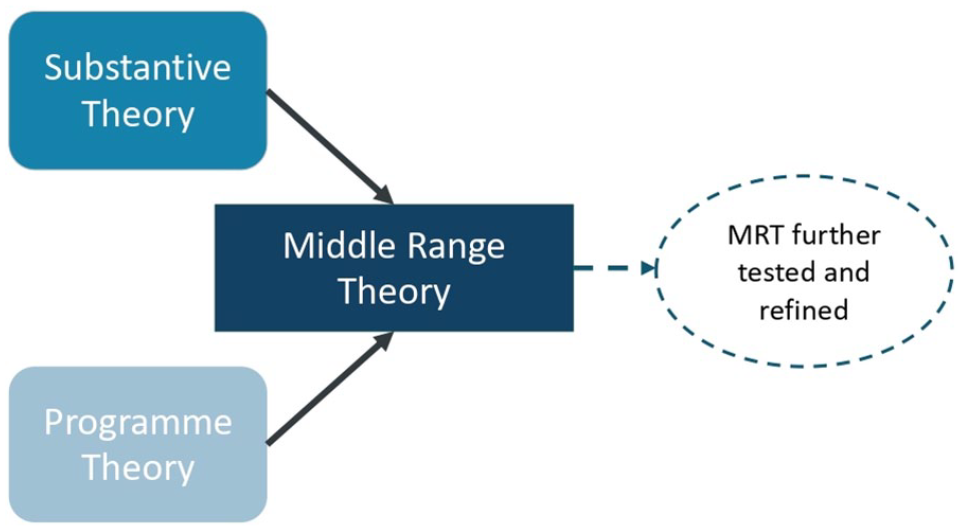
Conceptualisation of middle-range theory (MRT) within this RE.
Given that HCs constitute a complex health intervention and the lack of theoretical research into how and why HCs work, RE was considered an ideal fit for examining this complexity. In addition, considering the variation of scope and contexts in which HCs are used, the importance of developing an MRT which may be applicable across settings was seen as an important aim for this research. While there are quality standards (Wong et al., 2017) and reporting guidelines (Wong et al., 2016) for completing REs, there remains a lack of guidance for how an MRT should be developed. To this end, an approach was selected for this study, constituting three main stages (outlined in more detail below). It should be noted that this research developed an MRT that can be viewed as an early MRT, or first step, towards ongoing refinement and testing across different settings in future to further enhance its generalisability and applicability.
Overview of methods for the RE
This RE took place over several phases with the methods described in greater detail in the studies by Gilmore et al. (2016b, 2019) and the study by Gilmore (2018). In brief, the RE began by eliciting initial PTs (IPTs), which involved literature and document review along with four key informant interviews (KIIs; Gilmore et al., 2016b). The field study was then designed (see Gilmore, 2018) based on these IPTs, and two case studies took place in North Rukiga, Uganda, to test and refine these theories (see Gilmore et al., 2019). For case study 1, this data collection took place in Kutinga including: observation and field notes, document review (including HC meeting notes, correspondence between HC and non-governmental organisation (NGO), Ministry of Health (MoH) reports), semi-structured interviews with six HC members, two further interviews with a local chairperson and a community health worker and three focus groups (n = 10 female community members, n = 8 male community members and n = 10 community health workers); for more details, please see the study by Gilmore (2018). Case study 2 took place in Kashambya, with data collection involving observation and field notes, document review (including HC meeting notes, NGO and MoH reports), three semi-structured interviews with health committee members and one with a community health worker, three focus groups (n = 7 male community members, n = 12 female community members and n = 8 community health workers); for more details, please see the study by Gilmore (2018). In this study, the resulting refined PTs for each case study are taken forward in the latter phase of the RE, where they are synthesised to develop an MRT to explain how HCs work and how they can build capacity for health (see Figure 2).
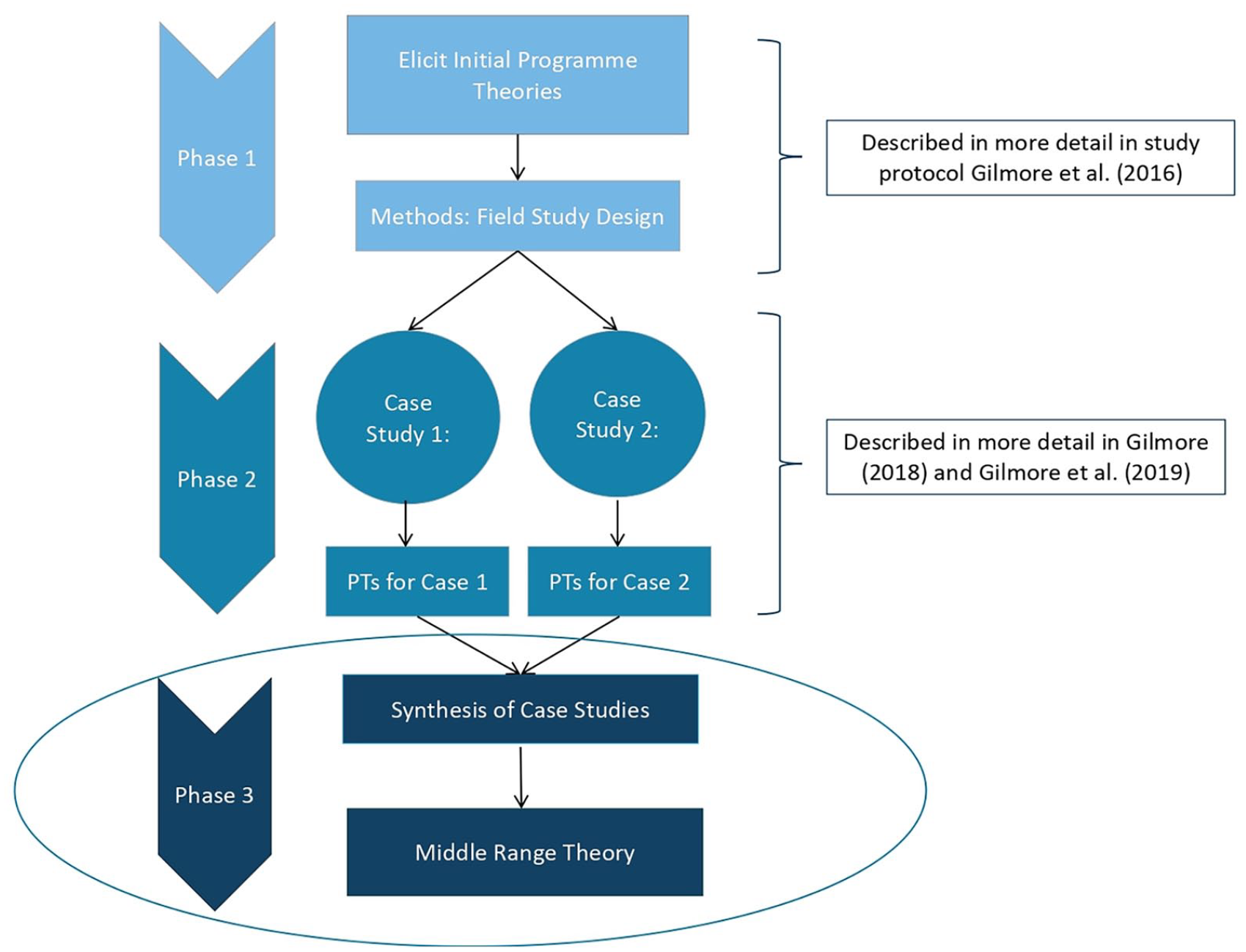
Overview of phases in RE. The focus of this article is methods and results from the final highlighted phase, which led to the development of MRT.
Methods for the development of an MRT
The methods to develop and refine an MRT took place across three stages: (1) searching for demi-regularities (i.e. semi-predictable patterns in the data (Wong et al., 2017)) between refined PTs (and their corresponding CMOCs); (2) conducting four KIIs to support or refine developing MRTs; and (3) situating the findings in the existing literature, including linking these to substantive theory, to refine the MRTs further. An overview of these stages is provided in Figure 3.
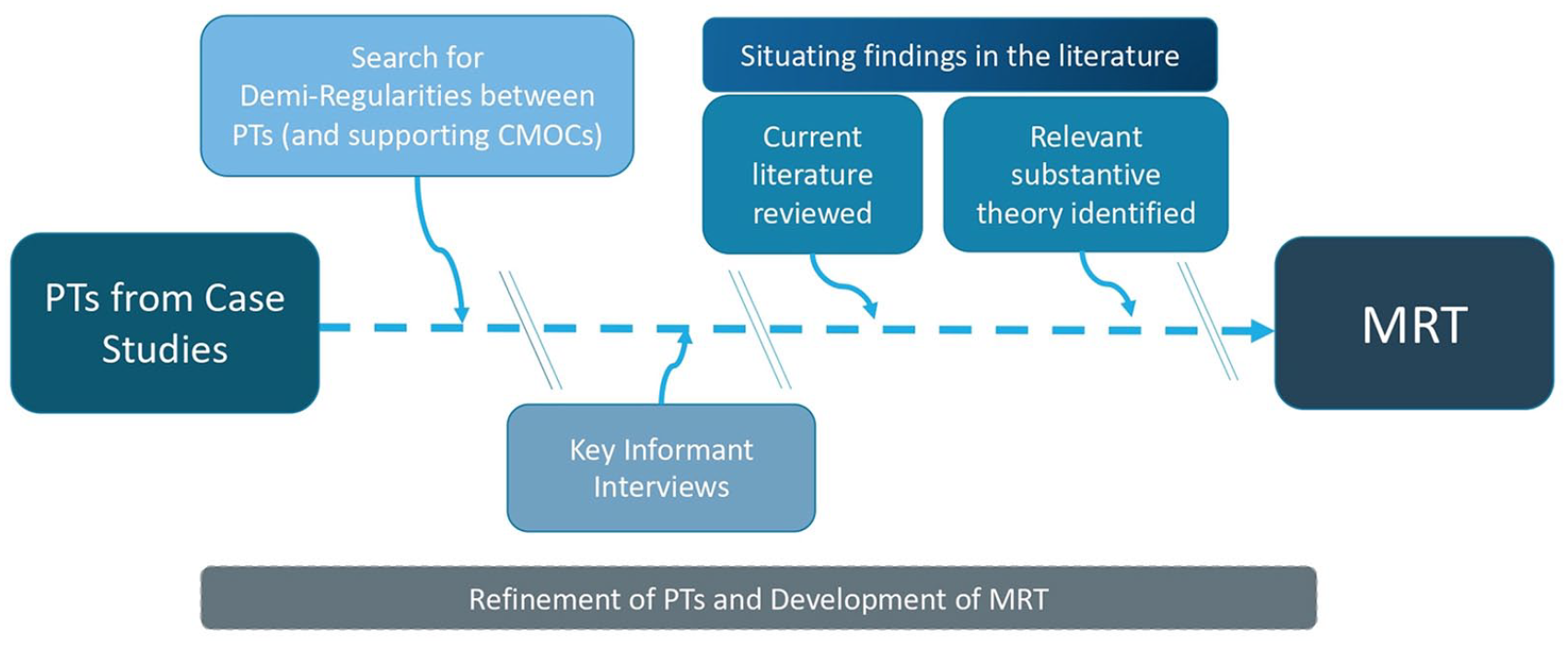
Progression from PTs to MRT.
Stage 1. Searching for demi-regularities within the refined PTs from case examples
A total of 18 PTs and 47 of their supporting CMOCs (Gilmore, 2018) were searched for demi-regularities, that is, semi-predictable patterns within the data (Wong et al., 2016). Synthesis of PTs was completed manually as per the following procedures and as outlined in the study by Gilmore et al. (2019). First, the 18 PTs were printed on coloured paper using a different colour for each case study. PTs were then reviewed and grouped/organised according to their similarities, yielding nine demi-regularities. The CMOCs within each demi-regularity were then reviewed again to see if they further explained the emerging findings. A modified socio-ecological model consisting of (1) individual level, (2) organisational level, (3) community level and (4) societal level was then used to organise and classify the identified demi-regularities. By doing this, initial MRTs began to develop (see Supplemental File 1). As detailed below, these theories were further reviewed with each subsequent stage.
Stage 2. KIIs
Four KIIs were conducted, using realist style interviewing, with individuals involved in implementing or overseeing the Access to Infant and Maternal Health (AIM-Health) programme, which as one component implemented community HCs. Overall AIM-Health aims to improve health services at the community level through the introduction of task-shifting cadres, while also working to increase community knowledge, power and autonomy over health and health-related decisions. Participants included a (1) health education specialist, (2) health programme manager, (3) health inspector and (4) an accountability programme manager. The MRTs developed in stage 1, and the KII interviews were then uploaded and coded in NVivo with memo notes used to document thinking and refinement of theory, following the process outlined in the study by Gilmore et al. (2019). Of note, these interviews were not used to elicit new CMOCs, but to support and refine the initial MRTs. They also served to provide more contextual support for implementation factors (for example, supportive community health policies) occurring at the societal level. This stage of the analysis led to a further addition and refinement of the MRTs developed during stage 1.
Stage 3. Situating findings within substantive theory
Following the KII interviews, the refined MRTs from stage 2 were situated within the existing literature. This included an exploration of relevant substantive theories to clarify, support or provide further explanation and refinement for the findings. To note, this search was specifically for substantive theories to aid explanation of the emerging MRTs and not a wider search to seek further individual studies on how HCs worked. This search for substantive theories also served as a ‘plausibility check’ (Marchal et al., 2010) to further triangulate the emergent findings. From the refined MRTs from stage 2, the main concepts were identified based on demi-regularities found, for example, ‘Motivation’, ‘Respect’, ‘Power’ and ‘Altruism’. These concepts were then individually explored in the literature to identify relevant substantive theories that further support the MRTs and to draw connections between these key concepts based on theory. This was the final stage of the process and led to the resulting MRTs being proposed for this RE.
Ethical approval
Ethical approval was provided by: Health Policy and Management/Centre for Global Health’s Research Ethics Committee (Trinity College Dublin); Makerere University School of Public Health, College of Health Sciences (Uganda; ref: HDREC 338); and Uganda’s National Council for Science and Technology (ref: SS 3933).
Results
Four overarching MRTs, each corresponding to one of the four domains from the modified socio-ecological model, emerged for how HCs work for community capacity building for health. These MRTs were developed and refined across the three stages of (1) demi-regularity search between the PTs (and supporting CMOCs) within the case studies, (2) analysis of KIIs and finally (3) situating within the substantive theory and existing literature. The early iterations of the MRTs following stages 1 and 2 can be seen as Supplemental File 1. The following substantive theories were then used to inform the further refinement of the MRTs.
Theories of cooperation and collective action
Given the use of HCs as an organising intervention, where multiple actors come together to work towards a common goal, we first turned to substantive theories of cooperation and collective action to deepen our understanding of the HCs. Van Vugt et al. (2012) suggested the term cooperation to involve multiple actors who work to alleviate a structural problem by sustained and ongoing actions. Those who ‘cooperate’ typically would also benefit from their work. They noted two classifications of targets for cooperation: common resource problems and ‘common good’ problems. Within North Rukiga, HCs work towards a common good, and due to their involvement as a collective, they can be termed ‘a cooperation’ or ‘collective action’ (Van Vugt et al., 2012). For more details on the specific goals and outcomes for the HCs in these case studies, please see the study by Gilmore et al. (2016b).
The findings from the case studies, however, did not support several substantive theories in the field of cooperation and collective action, including, for example, theories concerning rational choice, notably Olson’s (1965) ‘collective action’ and Hardin’s (2009) ‘tragedy of commons’. Common to these theories is the concept of ‘freeriding’, where, if possible, an individual will not contribute to a common good. Similarly, Hardin et al. propose that action relates to self-interest and can be in opposition to the common good. In contrast, our findings suggest that the HCs readily and voluntarily take collective action to achieve a common good. Further to this, and while the cost–benefit (e.g. personal gains) can be an influence, the decision to be an active member of an HC was found to be determined by multiple factors such as one’s altruism and motivation through both intrinsic and extrinsic sources (Gilmore, 2018). Thus, and consistent with Van Vugt et al. (2012), the reason(s) why HCs
cooperate for the benefit of the collective is not simply determined by a calculation between immediate costs and benefits of cooperation: it is also influenced by a variety of different norms and values that people bring into these dilemma situations (p. 10).
Social identity theory
Next, social identity theory (SIT; Tajfel and Turner, 1979) was considered concerning the findings of the case studies given its widespread application to social mobilisation, collective behaviours, leadership between and within groups, marginalisation of out-groups, group norms and social influence (Hogg, 2016). SIT relates to inherent social classifications individuals group themselves and others into, which can, for example, be based on age, gender or religion (Hogg and Turner, 1985). SIT, therefore, involves individuals identifying themselves and others within society and requires both aspects of cognition (i.e. a sense of awareness) and evaluation (i.e. a sense that awareness is related to value; Tajfel, 1982). Should this occur, SIT proposes that individuals order their environment, allowing one to define others. Then, through this ordering, individuals identify themselves within their social world (Ashforth and Mael, 1989). Therefore, SIT recognises both one’s personal identity (individual traits) and social identity (group classifications; Ashforth and Mael, 1989). A process of self-categorisation takes place, where individuals can identify with particular groups (called ‘in groups’) by categorising themselves and others, resulting in the formation of one’s identity (Stets and Burke, 2000).
Turner (2010) classifies social groups as involving two or more people. In addition, these groups are interdependent, for reasons such as need satisfaction, attainment of goals and/or validation of values and attitudes. This interdependence and identification see individuals defining themselves primarily at the collective group level instead of a personal level, especially in highly cohesive groups (Van Vugt et al., 2012). SIT, therefore, aligns with cooperation in that it proposes that individuals undertake collective action for a common good because they evaluate their fate to be tied to this social identity (Brewer and Kramer, 1986; Van Vugt et al., 2012). Turner (2010) further elaborates on this in relation to cooperation and altruism by noting that
altruism is primarily an intragroup rather than interpersonal phenomenon, that its main necessary condition is the perception of ‘we-group ties’ between individuals [dependent on common social identification] and that it represents behaviour based on the cognitive extension of the self, not its abolition. We help others, apparently selflessly, because we perceive their needs and goals as those of our social category and hence as our very own (p. 31).
Thus, SIT advances our understanding of how HCs work by explaining why individuals, particularly those closely connected to their communities, may cooperate for the good of the ‘social’. Mechanisms of altruism or volunteerism within this study, triggered by their ‘community centeredness’, as a common context across several domains within the PTs (Gilmore, 2018), are therefore supported and expanded upon by suggesting that community centredness may be tied to one’s perceived identity. For example, in case study 2, where HCs were less connected to communities due to geographical range, the HC group was less active and showed limited signs of community altruism. In contrast, the HCs in case study 1 were very close to communities, allowing for a greater social identity between HCs and the individuals they serve to be formed. In turn, these HCs were noted as being more well-functioning. Applying SIT to these findings led to the understanding that when HCs are closely connected to communities and have positive community relationships, they may share a common social identity, which can improve collective action and ‘altruistic’ motives for HC involvement. This may also result in increased relatedness, which can improve autonomous motivation.
SIT can also help explain how ‘managerial processes/roles and regulations’ (roles and values) influenced how HCs worked within the case studies. SIT discusses that there will be an awareness of an ‘out-group’, with those who share social identities within the ‘in-group’ treated more fairly than those in an ‘out-group’ (Tajfel, 1982). Thus, applying SIT at an organisational level supports that having clear roles and responsibilities may situate HC members within the ‘in-group’ and may re-enforce shared social identities, cohesion and commitment.
Self-determination theory and motivation
While SIT greatly assisted in explaining some of the findings from the case studies within the RE, it is essential to note that social identity is not the only explanation relating to how HCs may function. Motivation was also commonly seen as important at the individual level to explain how HCs work across the PTs (and supporting CMOCs). Motivation can be defined as the forces and drivers acting on or within an individual that results in initiating or continuing behaviour (Snyder and Cantor, 1998). When synthesising PTs from the case studies, those relating to motivation were the most prevalent. To widen the understanding of how HCs work for capacity building for health, formal theories relating to motivation were thus looked to for further insights.
Self-determination theory (SDT), as proposed by Deci and Ryan (1985) was applied to the PTs from the case studies concerning motivation. SDT suggests that motivation can be classified as autonomous or controlled. According to Ryan and Deci (2014) ‘autonomous motivation encompasses intrinsic motivation and well-internalised extrinsic motivation, whereas controlled motivation encompasses regulation by external factors such as externally administered rewards and punishments or by partially internalised (i.e. interjected) contingencies . . .’ (p. 5755). Therefore, it was understood that through autonomous motivation, people experience volition or self-endorsement of their actions, while controlled motivation relates to feelings surrounding expectations for behaviour (Deci and Ryan, 2008).
SDT explains some of the findings from this RE, in that motivation is influenced by autonomous factors, such as HC members’ pride in their work, and controlled factors, such as financial reward. Further to these two concepts, the concept of relatedness within SDT further assisted in explaining findings from the case studies (Deci and Flaste, 1995). Relatedness can be described as feeling connected to one’s social world and the individuals within it and provides a foundation where more autonomy is likely to develop (Deci and Flaste, 1995). This supports the importance of ‘community centredness’ and the feeling of shared identity previously discussed through the lens of SIT. Both theories suggest HC members’ level of connection to the community is an important influence on group identity, commitment and relatedness, and thus their motivation.
Along with the prevalent mechanism of positive re-enforcement, the PT synthesis from the case studies evidenced the need for visible actions as a prevalent contextual factor. Therefore, another key concept within SDT of autonomous motivation through the promotion of competence was seen in the PTs. However, the counter of this (i.e. rival theory) was also found: If a negative result of actions is seen, this can cause amotivation through decreased perceived competence (Gagné and Deci, 2005). This finding was highlighted in case study 2 by the KII, where male community members were reported to have had little value-add and influence on the HCs within their health facility. This led to the understanding that autonomous and controlled factors influence motivation for engaging within an HC. Whereas controlled factors included financial compensation and/or reimbursements and training (extrinsic), autonomous factors included positive reinforcement that influences competence and community recognition of services. Should HC members observe visible changes because of their work (intrinsic), these motivational factors can lead to a rationalisation for volunteering through offsetting cost–benefit relationships.
Cultural and social capital
To further deepen the understanding of how HCs work for capacity building for health, the concepts of social and cultural capital were also explored (Bourdieu, 1986; Coleman, 1990). This lens helped explain the findings from the case studies, particularly the importance of respect at an individual level and power at an organisation level, both of which influenced how HCs worked for capacity building.
Bourdieu (1986) has been influential in the work of cultural capital and thus guided our understanding of how HCs worked at an individual level. Lamont and Lareau (1988) completed a review on the topic. They proposed a definition that ‘cultural capital is institutionalised, i.e. widely shared, high-status cultural signals (attitudes, preferences, formal knowledge, behaviours, goals and credentials) used for social and cultural exclusion’ (p. 156). Furthermore, Kingston (2001) suggested that cultural capital is a resource that holds ‘market value’ and is widely accepted and is also exclusionary, being only available to a select ‘elite’. With this understanding, cultural capital can be viewed as context-dependent, as ‘the elite benefit because “their” particular cultural signals, not others, are rewarded’ (p. 89) within their setting. Thus, through exclusion principles and stratification, cultural capital can inform social hierarchies, with these hierarchies greatly influencing societal power relations (Gaventa, 2003). Therefore, cultural capital can convert to other forms of capital, such as social capital or economic capital (Bourdieu, 2003, 2011).
The work on social capital by Bourdieu (1986), Coleman (1990) and Putnam (1993) was used to facilitate an understanding of how HCs work. Within their work, social capital would be attributed to a group, not necessarily an individual. For example, Bourdieu (1986) suggested social capital as where benefits can be attributed to networks or groups, which can, in turn, be used to leverage economic advancement. This was further expanded upon by Putnam (1993) where social capital could mean shared values, trust and norms, which could work for mutual benefit through cooperation. Notably, a review of social capital by Portes (1998) found that social capital was used as a catchall phrase with different meanings. To strengthen a shared understanding of social capital, Portes (1998) proposed three basic functions: that social capital is a source of (1) social control, (2) family support and (3) benefits through extra-familiar networks. Benefits through extra-familiar networks would also be in keeping with Bourdieu (1986), with social capital seen as the ability to get benefits through relationships and membership in social networks or structures. Portes (1998) also noted that social capital influences trust within groups by the shared contribution to activities being contingent on the trust members in a group have in each other. Without trust, which may have been generated by shared social capital, organisational engagement may be reduced.
Further to the above understanding of social capital, the work by Woolcock and Narayan (2000) on social capital further informed this study. They suggest one view as synergistic, where governments, cooperations and civic groups need to complement each other in order to achieve sustainable development. The level of linkages, coproduction and participation between actors in these groups may allow for enhancement of community organisations’ ability to function. Thus, for the purpose of this study, it emphasises the importance of wider support, for example, from government, in order to create supportive partnerships and environments for HCs. Woolcock and Narayan (2000) suggest that when this synergy is effectively supported, it can increase social capital through the repetition of interactions infused with shared norms and trust.
The findings which emerged from the case studies were then further explained with the understanding of cultural capital at an individual level and social capital at an organisational and community level. For example, HC members who were seen as educated, knowledgeable and responsible had these ‘cultural signals’ rewarded with cultural capital. This could be in mechanisms of respect, perceived capabilities and trust. Furthermore, cultural capital in this study was facilitated by contexts of ‘social hierarchies’, which influenced the triggering of these mechanisms. The case studies found that the HC group needs power, that is, an ability to connect and influence, which can be triggered when the HC members are respected and trusted. Therefore, cultural capital that can lead to respect (at an individual level), can in turn influence the group’s social capital by increasing external stakeholders trust of the HC group. This may allow for power and positively influence their ability to function. This finding also aligns with Putnam (1993), who suggested that when a group has high social capital (i.e. influenced by respect, trust, norms and cooperation), they can more easily work through intra- and inter-group relations.
At a community and societal level, the synergistic view of social capital further helped to explain the findings in the case studies where synergistic relationships and buy-in from other stakeholders could further re-enforce the social capital of the HC. This explanation was supplemented by drawing on the work of Evans (1996, 1997) about government–citizen action. Evans suggests that the effectiveness of government-citizen action is linked to complementarity and embeddedness. Complementarity concerns existing supportive relationships and policies, which could mean, for example, existing community health worker policies (Woolcock and Narayan, 2000). Embeddedness relates to the connectedness and linkages between citizens and government individuals (Evans, 1996; Woolcock and Narayan, 2000). These two concepts build off pre-existing social capital (Evans, 1996) and, in turn, they also promote and re-enforce it. Applying this to how HCs work at a community level within the case studies was helpful to explain that when there was a context of pre-existing relationships (i.e. embeddedness) and clear roles and responsibilities (i.e. complementarity) between the HC members and the MoH and NGO, this influenced linkages between the partners and shared trust. Where these synergies existed, HCs could benefit from increased resources and support, and partners also saw the mutual benefit through the HC’s actions contributing to their agendas. This concept of complementarity can also apply to how HCs work at the societal level. Supporting policy environments and implementing partners with relationships in the setting can create a positive context for HCs to function.
Following synthesis of the PTs (and their supporting CMOCS), input from KIIs and incorporating the above learning from SIT, SDT and cultural and social capital, the MRTs on how HCs work for capacity building were developed and refined at the individual, organisational, community and societal levels. These MRTs are presented in Boxes 1 to 4 below.
Results: MRTs
MRT 1. How HCs work for community capacity building for health at the individual level
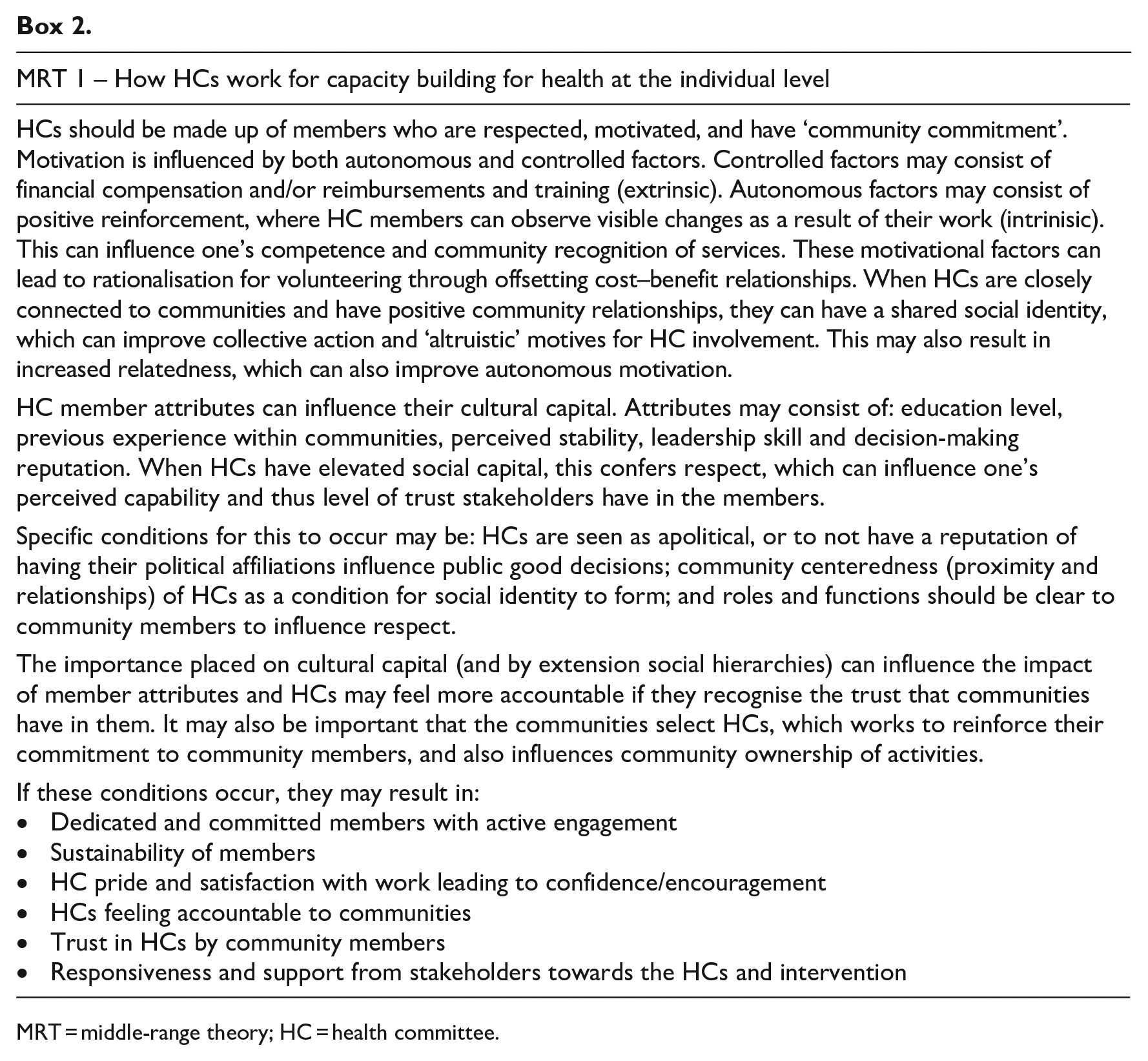
MRT = middle-range theory; HC = health committee.
MRT 2. How HCs work for community capacity building for health at the organisational level
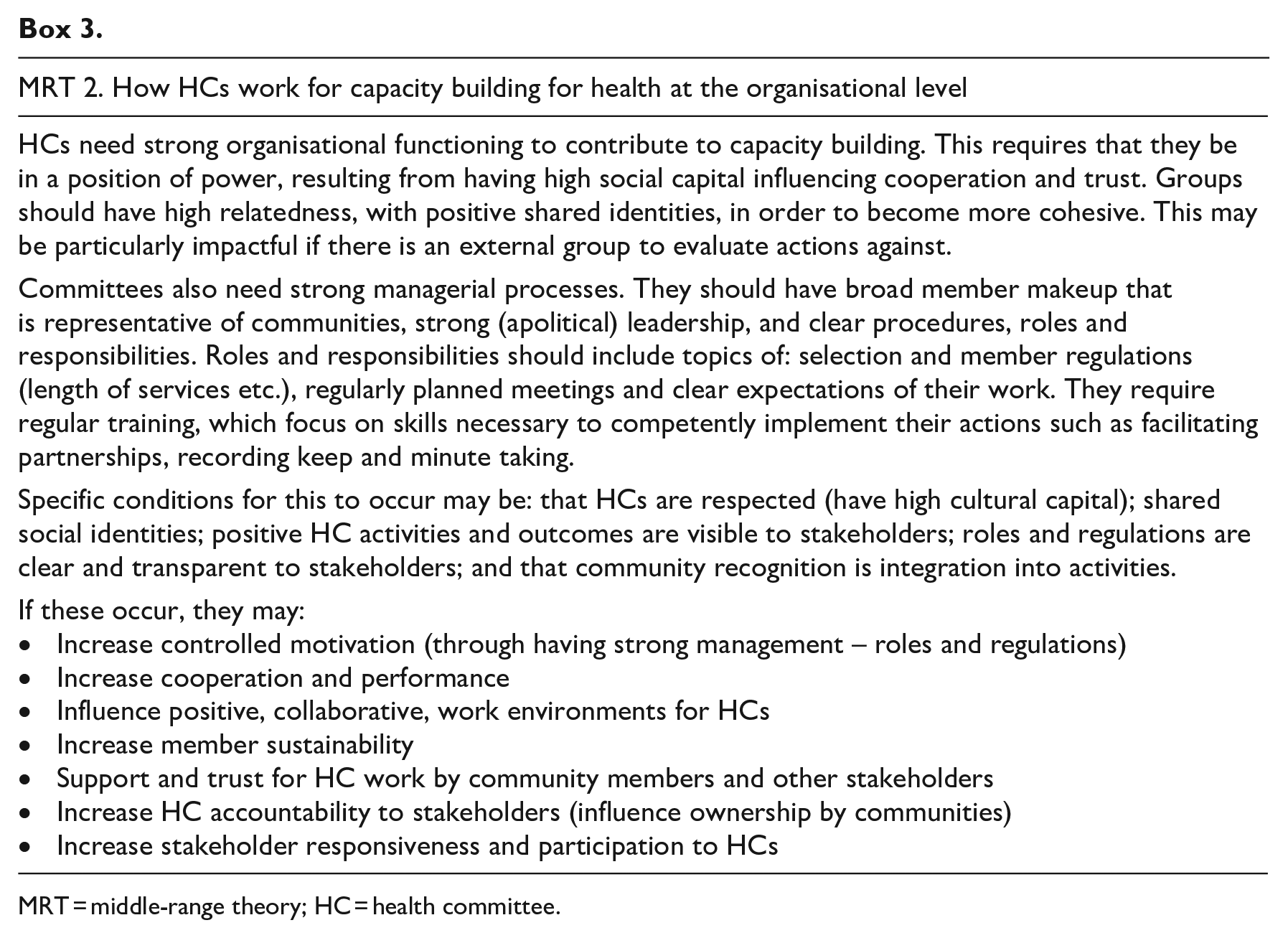
MRT = middle-range theory; HC = health committee.
MRT 3. How HCs work for community capacity building for health at the community level
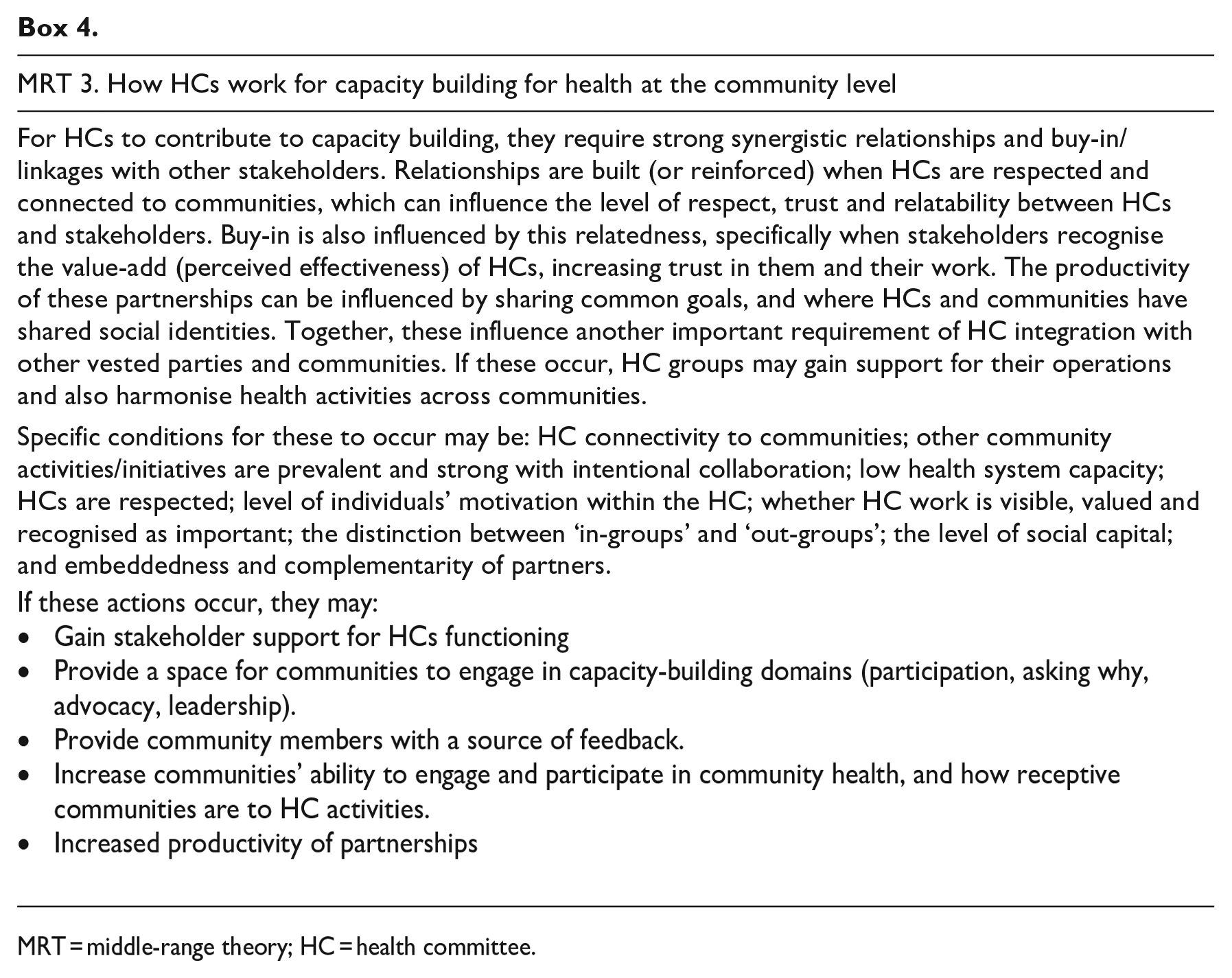
MRT = middle-range theory; HC = health committee.
MRT 4. How HCs work for community capacity building for health at the societal level
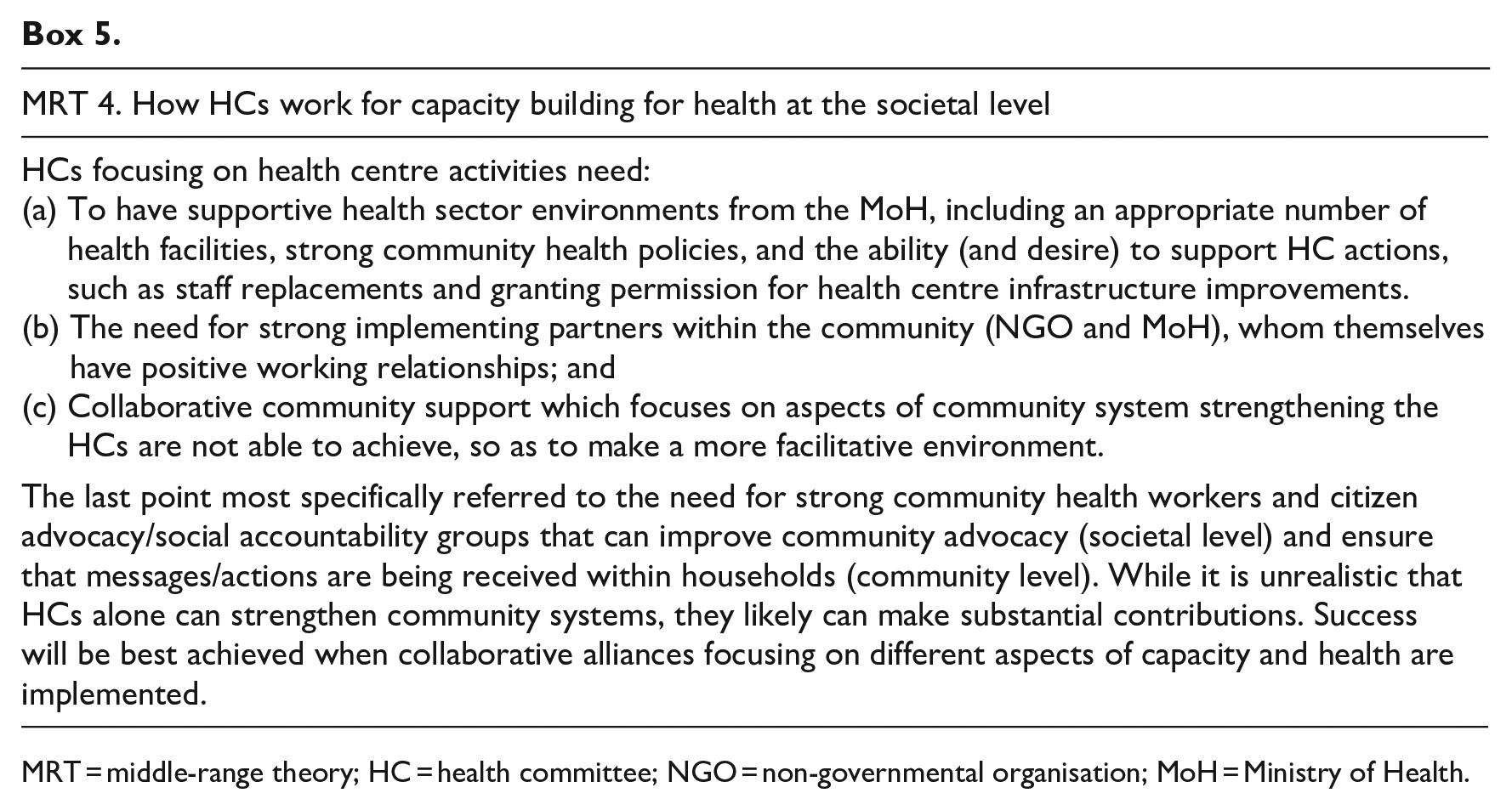
MRT = middle-range theory; HC = health committee; NGO = non-governmental organisation; MoH = Ministry of Health.
Limitations and reflections
These MRTs serve as a first step towards a greater understanding of how HCs may work across varying contexts. However, it is important to acknowledge that these could be viewed as early MRTs, which can be taken forward for further refinement and testing. An identified limitation of developing this MRT was that while the case studies are part of a wider RE taking place within Tanzania and Uganda (for results, see Gilmore (2018)), only two case studies from Uganda were synthesised in this study. In addition, data collection for the overall study was iterative and had PTs being fed back to participants for further refinement and/or confirmation, however, due to logistics and time frame of the study, the final MRTs presented did not have an opportunity to be fed back to participants. A suggestion for future studies may, therefore, be to allow for a further round of refinement of the MRTs with the wider participant group, where possible.
The literature contains limited examples of how to develop and present MRTs. This lack of guidance made it challenging to decide when or how to review and refine an MRT. Within this RE, the MRTs were initially developed in their first draft following a synthesis of the PTs from the two case studies (this first stage of the MRT can be seen as Supplemental File 1). Following this, a natural time point to review and refine the PTs was after the KIIs, where further learning took place (findings from KIIs, which were incorporated into the MRTs can also be seen in Supplemental File 1). Leading on from this, the literature, namely substantive theory, was explored in detail and applied to the findings. At this stage, the MRTs were reviewed and refined again, where necessary, with the refinement consisting of providing additional insights or explanatory information into the theories while also not changing their meaning. This process led to the proposed MRTs. However, this sequence could be altered (i.e. with the literature review occurring first), depending on the needs of the RE, and may offer alternative benefits or insights into the theories. However, a limitation which needs to be highlighted is that due to the PTs and resultant MRTs being informed by a limited number of case studies from a similar geographical region and social and cultural context, the generalisability of the theories outside of these settings is yet to be tested. As such, these MRTs could be further strengthened through future research with further rounds of testing and refinement across different geographical, social and cultural settings making the resultant MRTs more generalisable. This could be completed through further literature review, and also through RE case studies.
The lead researcher for this study has a background in global and maternal and child health research, and when not completing field work, is based in a high-income country. Other members of the research team are based in academic positions in Uganda and Tanzania. This study was carried out in Uganda, but the theories that influenced MRT refinement were largely developed from what Henrich terms WEIRD theories, as those largely developed in Western, Educated, Industrialised, Rich and Democratic contexts. Henrich et al. (2010) has previously discussed the use of Western theories and questioned their global applicability, and this point is reflected in the study by Gilmore (2019). To address the risk of applying potentially contextually irrelevant theories within RE, substantive theories were deliberately not used to identify IPTs or refine PTs but rather to provide further explanatory power and clarity to the MRTs, and as a ‘plausibility check’. In other words, the substantive theories did not drive the refinement and were only used once the theories were already refined. As the lead researcher was not from the local setting, learning from the knowledge of key informants who operationalise HCs, was an important step to deepen understanding and to ensure that the MRTs remained relevant to practice. While KIIs may not be necessary for all REs when refining an MRT, it was an important part of MRT development in this study. In addition, it is hoped the KII input for MRT development may have helped to mitigate the bias of a Western lens to ensure the MRTs were relevant to the contexts in which HCs are used.
While the approach used for developing and refining the MRTs in this study may not be relevant to all REs, it is hoped that the transparency of the methods used may guide and inform other studies as relevant to their needs. Overall, researchers are encouraged to report the MRTs arising from their REs and detail how they were developed to improve theoretical awareness of the interventions of study and to support further research study processes. While the resulting PTs from the case studies (Gilmore, 2018) present programmatic findings to support implementation considerations, it is hoped that the MRTs provide additional explanatory details at a level of abstraction relevant to HCs across many contexts.
Conclusion
The MRTs developed through this study provide insights for those implementing HCs on how HCs may work for capacity building for health. Numerous important factors were identified for how HCs work, including the importance of altruism, motivation and cultural capital at the individual level; power and organisational processes; synergistic relationships, buy-in and connectedness within the community; and supportive societal environments with strong partnerships, health policies and infrastructure. It is hoped that HC programme implementers can apply the findings of this study to better understand how and why HCs may work within their settings. Furthermore, while there is no one approach for MRT development, this study details an approach others can draw on to develop an MRT for a complex health intervention.
Supplemental Material
sj-docx-1-evi-10.1177_13563890231223182 – Supplemental material for Developing middle-range theories within a realist evaluation of how health committees support community capacity for health
Supplemental material, sj-docx-1-evi-10.1177_13563890231223182 for Developing middle-range theories within a realist evaluation of how health committees support community capacity for health by Brynne Gilmore, Jessica Power, Nazarius Tumwesigye, Henry Mollel, Eilish McAuliffe and Frédérique Vallières in Evaluation
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project has received funding from the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie Grant Agreement No. 713279.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.