
Abstract
Early parenting programmes which promote nurturing care for children aged 0–3 years are popular in community-based primary health care settings. However, little research has explored the causal and theoretical assumptions underpinning these programmes. This paper outlines a programme theory evaluation which was conducted to explore the change principles inherent in a complex early parenting intervention, the parent and infant programme, which aims to support parents and infants aged 0–2 years. A documentary analysis and qualitative interviews (n = 19) with key stakeholders were undertaken to describe programme components, outline intervention objectives and identify the mechanisms assumed to be important to programme success. The interpretation of the findings was informed by the Consolidated Framework for Implementation Research, within which we explore and describe the theoretical perspectives that underpin the programme and guide its operationalisation and delivery. The importance of attending to the causal mechanisms underlying early parenting interventions is outlined.
Keywords
Introduction
There is an increasing international political consensus that public investment in universal, proportionate support for parents and children aged 0–3 years can help to break a cycle of inequality and disadvantage while also yielding significant economic benefits (Heckman et al., 2010). Parenting interventions focus on enhancing the interactions between parents and children to improve outcomes. The approach to change adopted within these kinds of interventions is influenced by their theoretical foundations, which can include social learning theory (Patterson, 1982), family systems theory (Cowan et al., 1998) and/or attachment theory (Ainsworth and Bowlby, 1991). A small number of studies have examined the ways in which the theoretical foundations of parenting interventions can shape their development and influence their implementation (e.g. Forgatch and Domenech Rodríguez, 2016). However, to date, the evaluation of the effectiveness of early parenting interventions has been limited by a lack of clearly delineated implementation protocols and little information on the proposed mechanisms of impact (Bakermans-Kranenburg et al., 2012; Hurt et al., 2018). An inadequate articulation of the behaviours underpinning the implementation of early parenting interventions, can undermine our understanding of how and when they can be most effective, as well as the specific ingredients necessary for their success (Williams and Beidas, 2019).
Innovation in healthcare delivery systems, including children’s service settings, has frequently failed to pay attention to the theory underlying service improvement efforts (Davidoff et al., 2015; Olofsson et al., 2016). The development and testing of causal theories aimed at understanding the relationships between determinants and implementation outcomes and has been identified as an area of priority for implementation science within child psychology and psychiatry (Williams and Beidas, 2019). Understanding the (potentially) active ingredients of universal, preventive early parenting intervention provides crucial information for decision-makers and service providers who wish to develop, embed and sustain the effective delivery of these kinds of programmes in child and family service settings (Kilburn et al., 2017). Identifying the theory underpinning an intervention enables decision-makers to understand what the intervention is made up of, its likely outcomes and the issues or dysfunction which it targets (Leviton and Trujillo, 2017). A theoretically guided focus can also help to identify factors which facilitate or inhibit programme success, thereby helping to guide the development of more informed practice and policy (Davidoff et al., 2015). Furthermore, there is significant heterogeneity across early parenting interventions (Hurt et al., 2018) and, therefore, the identification and description of change mechanisms can promote greater comparability across interventions, thereby enhancing our understanding of when and why programmes are effective.
This article reports on the early stage of a detailed process evaluation of a group-based early parenting intervention programme, the parent and infant (PIN) programme (Hickey et al., 2016). The overarching aim of this study was to develop a model to demonstrate the way in which the PIN programme is intended to work, highlighting the change mechanism that underpins the programme.
The PIN programme
The PIN programme is a complex, group-based early parenting intervention which combines a range of developmentally appropriate PIN supports that are delivered in a single intervention process from birth to 2 years of age (Table 1). Parents are offered the Incredible Years Parent and Baby Program (IYPBP) in conjunction with information, awareness raising and practical workshops and classes (e.g. baby massage classes, weaning workshops, first aid, child health and safety). At later points in the child’s developmental progression, tailor-made play, oral language and healthy eating workshops, as well as the Incredible Years Parent and Toddler Program (IYPTP) are also offered to parents.
PIN programme overview.
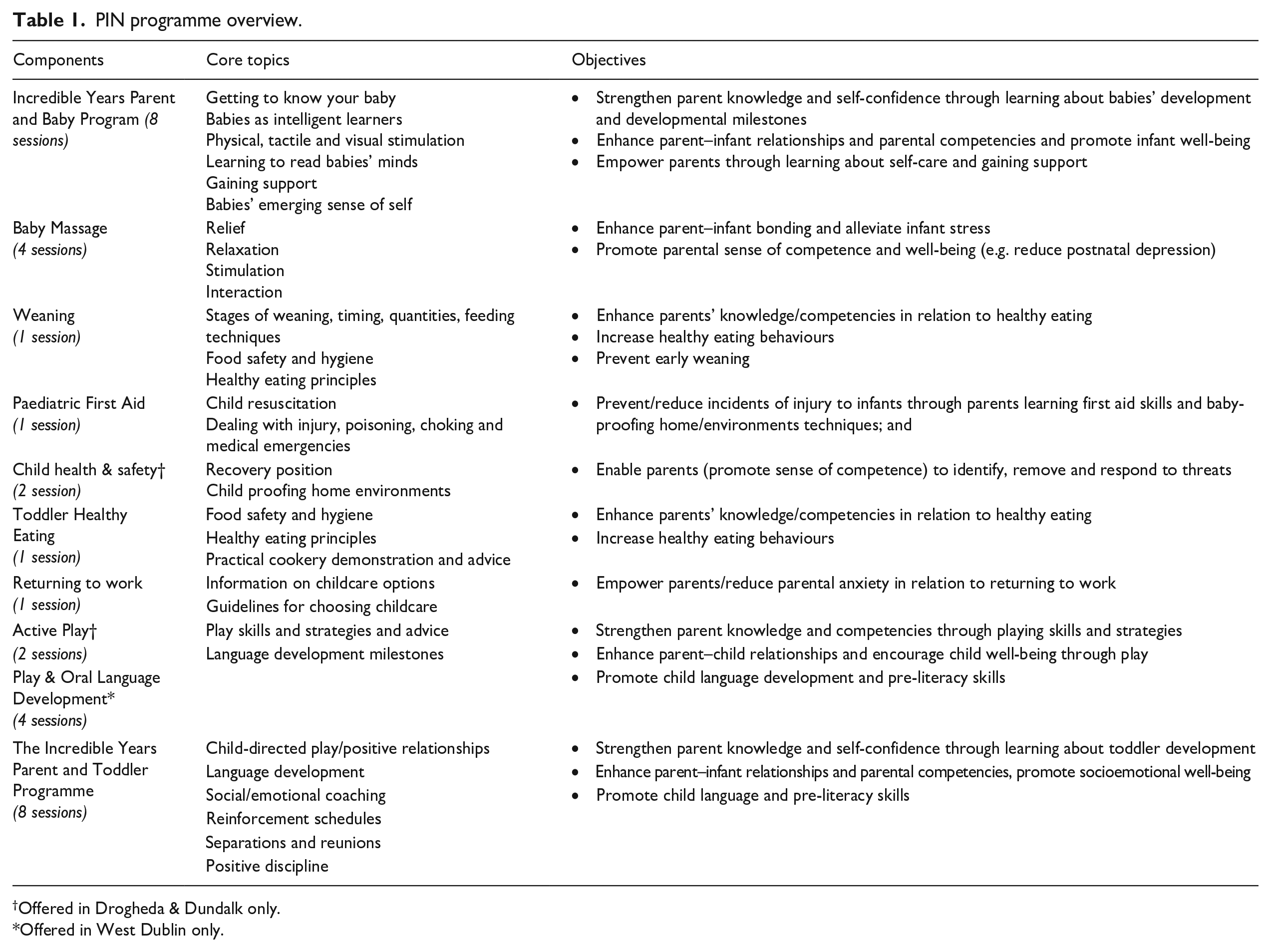
Offered in Drogheda & Dundalk only.
Offered in West Dublin only.
The PIN programme is delivered collaboratively through usual primary care and community-based services in the West Dublin and Drogheda/Dundalk (Northeast) regions of the Republic of Ireland. Programme facilitators include public health nurses (PHNs), family support workers, local development workers and parent volunteers.
Study background
This evaluation was conducted within a larger research programme (Hickey et al. 2016) which incorporates a non-randomised effectiveness trial and economic analysis of the PIN intervention (Hickey et al. 2020). The overarching aims of the PIN process evaluation are to gain an understanding of the active ingredients of the programme, explore how implementation is progressing and systematically evaluate the processes and conditions which influence programme implementation and effectiveness (Hickey et al. 2016). Importantly, this research was carried out by an independent research team who were not involved in programme development or implementation. The specific objectives of this research – conducted in line with the Medical Research Council (MRC) framework for process evaluations (Moore et al., 2015) – were to: (1) describe the programme components; (b) outline the programme objectives and intended outcomes; and (3) detail the activities, resources and factors considered to be necessary to achieving programme outcomes. Overall, the process evaluation will involve an in-depth exploration of programme implementation.
Methods
Methodological framework
Data reported here were collected during installation (prior to implementation) and early implementation stages. A systematic ‘model’ of the pathways, processes and activities involved in the PIN programme and the ways in which these are assumed to influence outcomes had not been developed. To address this gap, we aimed to identify the theoretical assumptions underpinning the PIN programme. We drew on a programme theory approach to examine how and why the PIN programme is intended to work (Coryn et al., 2011; Hickey et al., 2015). Weiss (1997) draws an important distinction between ‘programme theory’, which refers to a ‘theory of change’ or the hypothesised causal links between the mechanisms of an intervention and their anticipated outcomes, and ‘implementation theory’ which involves the identification of what is needed to translate objectives into service delivery and programme operation. Logic models often focus on implementation without necessarily demonstrating the causal mechanisms that are intended to be produced by an initiative. Programme theories, on the other hand, represent a systematic modelling of the assumptions underlying a given intervention; they can vary in complexity from simple and linear to highly complex and detailed, but they are typically presented as a diagram that describes relationships and interconnections between programme actions, context and outcomes (Rogers, 2008).
In this study, we aimed to articulate the theory of the PIN programme by documenting its underpinning causal mechanisms. Here, we define change mechanisms as the causal pathways that explain how implementation efforts achieve desired results (Lewis et al., 2022). This perspective frames causal mechanisms and change pathways as the interrelationships among implementation strategies and outcomes within a given implementation/intervention context (Lewis et al., 2018). These change pathways should help to articulate the conditions which explain how the outcomes targeted by a given intervention are achieved and, in turn, should enable predictions to be made in relation to the implementation strategies that are likely to lead to desired outcomes in a specified context (Lewis et al., 2020; Williams and Biedas, 2019). This process was informed by programme theory (Funnell and Rogers, 2011) which helped to guide the study methodology (e.g. development of interview questions and data collection tools used in the documentary analysis). The benefits of this approach lie in its ability to forefront stakeholder perspectives and identify underlying assumptions and intended implementation mechanisms, all of which are crucial to building knowledge of how and why an intervention is expected to work (Lawless et al., 2018).
Subsequently, we drew on the Consolidated Framework for Implementation Research (CFIR; Damschroder et al., 2009) to guide data analysis. The CFIR was selected to guide analysis as it aims to specify the type and nature of factors which shape implementation (Nilsen, 2020). It brings together learning from a range of other implementation frameworks and offers a typology of constructs believed to influence implementation, allowing it to be used to identify causal mechanisms as part of theory development (Breimaier et al., 2015). The CFIR comprises five domains including: (1) the intervention characteristics; (2) the outer context of programme delivery or the economic and social factors in which an organisation resides; (3) the inner setting, which comprises the structural political and cultural context in which implementation occurs; (4) the individuals involved in implementation and their various characteristics, beliefs and values; and (5) the processes which are aimed at achieving individual and/or organisational use of the intervention; these processes constitute a set of interacting and interrelated events or activities which involve individuals and may occur in the inner and/or outer context. Within each domain, a subset of constructs (39 in total) likely to influence implementation, have been identified. These range from the perceived complexity of the intervention to external policies and the networks or norms present within an organisation, as well as the planning or leadership present to support an innovation (Damschroder et al., 2009).
In line with programme theory evaluation, we adopted a theory-building approach to the use of the CFIR (Kirk et al., 2015). The framework was not applied in its entirety; rather, we adopted only those constructs relevant to the PIN programme and its implementation. In this way, we aimed to unpack the complex, dynamic influences at play within the intervention and identify the proposed mechanisms that are intended to lead to outcomes.
Developing the programme theory
Data collection
A multi-method, qualitative study was undertaken which involved a number of one-to-one and small-group interviews, as well as a documentary analysis. Data were collected between January and December 2017. A purposive sample of 19 stakeholders was recruited from across the range of agencies/organisations involved in programme implementation (including community-based services and public health nursing and primary care services). Key informants were approached to take part in the research (via email) and all agreed to take part in one-to-one or small-group interviews (2 participants per group). Small-group interviews were conducted when prospective participants were collaboratively involved in programme implementation (e.g. facilitated programme components together). Participants included personnel involved in programme development, implementation planning and support/facilitation and/or programme delivery and included community-based service managers (n = 4), Public Health Nurses and Nurse Managers (n = 6), family support workers (n = 9) (Table 2). All participants were provided with information sheets prior to participation in interviews and provided written informed consent. Consent was obtained prior to data collection.
Breakdown of Interview Participants’ Roles in the PIN Programme and Occupational Background.
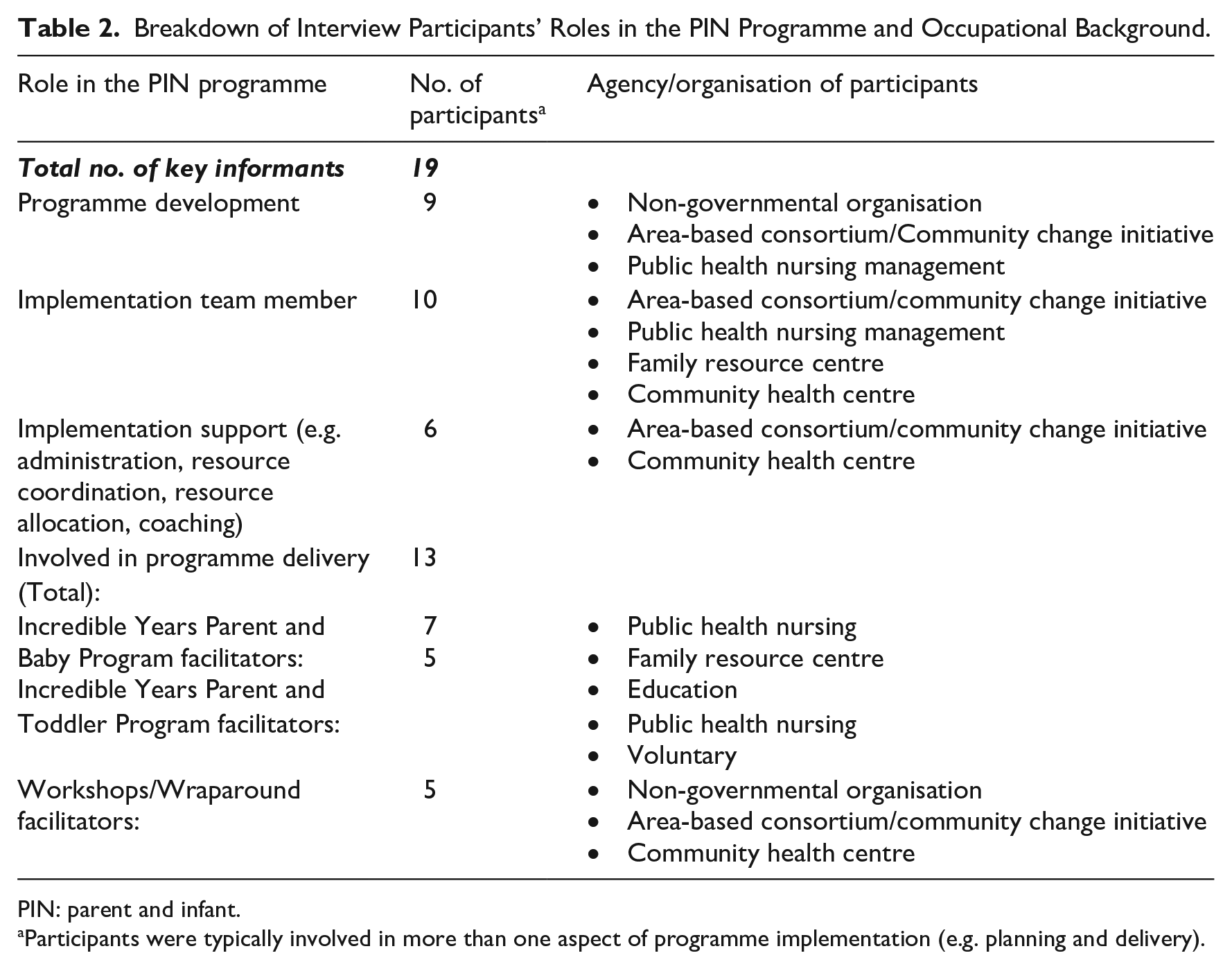
PIN: parent and infant.
Participants were typically involved in more than one aspect of programme implementation (e.g. planning and delivery).
Interview schedules were devised to guide interviews and ensure the commonality of subject matter during data collection. Information was gathered on stakeholders’ perceptions and experiences of the PIN programme. Data collection was conducted in stakeholders’ place of work, lasted on average 45 minutes and were audio recorded (with consent) and transcribed verbatim.
Documentary analysis was undertaken in parallel to the interviews to provide insights into programme content and delivery/implementation processes and practices. Reviewed documents included: programme manuals (n = 4), implementation protocols and details (n = 3) or delivery materials (n = 7); materials/handouts for parents (n = 9); minutes from implementation team meetings (n = 12); minutes from meetings between the research team and programme coordinators/developers (n = 20) and delivery reports produced by programme developers (n = 4).
Data analysis
Data were analysed using thematic analysis. This approach, conducted by the first author, consisted of line-by-line coding of transcripts/written materials. Codes were then integrated into larger themes and examined against the CFIR to define and categorise themes into core implementation domains. We assessed the data against all 39 constructs contained within the CFIR framework; this led us to identify 18 constructs which were perceived to be important causal mechanisms in respect of the PIN programme. We did not find data to support the relevance of three constructs within the ‘intervention characteristics’ domain including intervention source, trialability and costs; In respect of the ‘inner and outer setting of programme delivery’, a number of constructs were excluded due to their non-applicability to the theoretical assumptions underpinning the PIN programme. These included: patient needs and resources and peer pressure; structural characteristics; tension for change; compatibility; relative priority; organisational incentives and rewards; goals and feedback; and learning climate. The ‘processes’ considered irrelevant included opinion leaders/implementation leaders, champions and external change agents.
Within the ‘individual’ domain, key stakeholder skills were identified as a crucial causal mechanism underpinning the impact of the PIN programme (including knowledge and belief about the intervention, self-efficacy, personal attributes and stage of change). However, identification with the organisation was not identified as important. These factors may exert an important facilitative/inhibitive influence on implementation, but they were not identified here as being change principles inherent in the PIN programme and anticipated, therefore, to bring about programme success – which, ultimately, involves the attainment of intended programme outcomes for the parents and very young children who participate in the programme (i.e. positive parenting and developmental outcomes).
Data analysis was supported by the use of MaxQDA. Consolidated criteria for Reporting Qualitative (COREQ) research guided the presentation of findings (Tong et al., 2007). A stakeholder workshop attended by programme developers and implementers (n = 8) was held to facilitate respondent validation and obtain feedback on the development of an initial programme theory. To ensure participant anonymity, transcripts were allocated identifiers; ‘Ix’ represents findings from interviews (‘I’ denotes interview and ‘x’ an allocated participant number); documents are identified as ‘Dx’.
Results
A model of the PIN programme was developed which outlines the anticipated outcomes of the PIN programme and drivers which are expected to bring about these outcomes across different levels of programme implementation (Figure 1). These are outlined in more detail below.
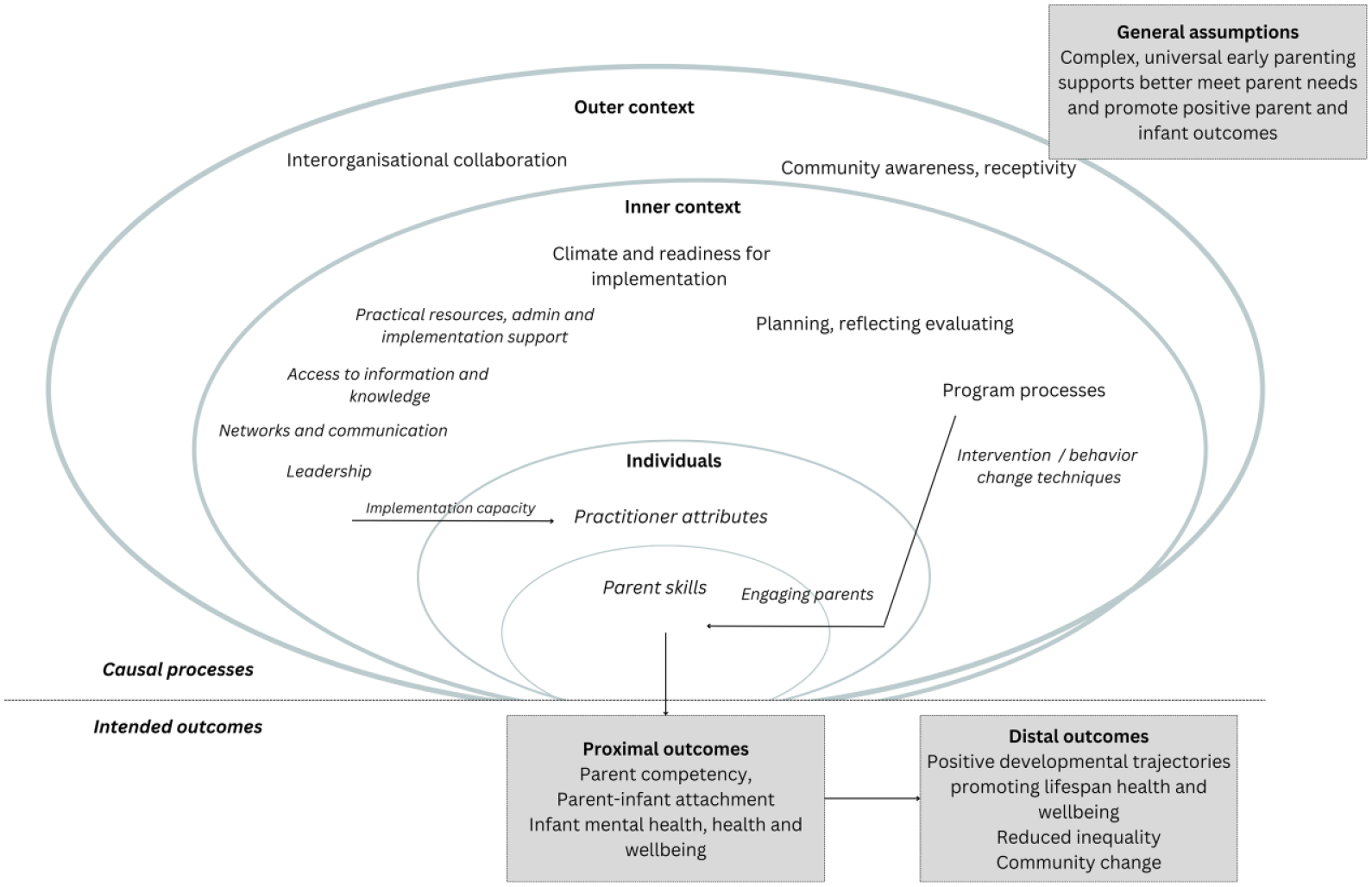
The theory of the PIN programme.
PIN intervention anticipated outcomes
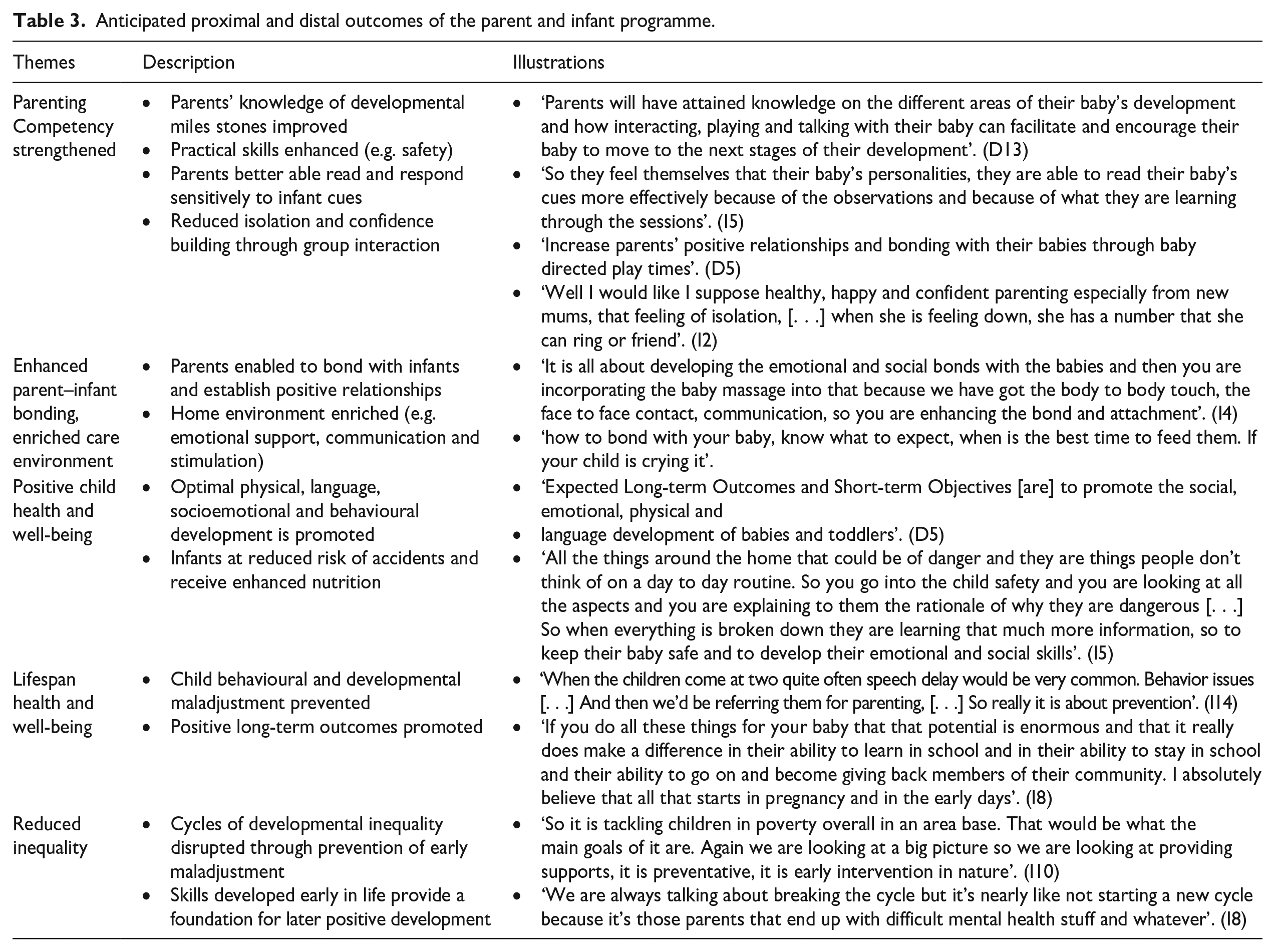
The analysis highlighted several intended outcomes of the programme which were categorised, respectively, into proximal and distal outcomes; these are described in brief below, while an additional detail is provided in Table 3.
Anticipated proximal and distal outcomes of the parent and infant programme.
Proximal outcomes
The PIN programme was developed to help strengthen parent knowledge, skills and confidence and, in turn, to promote sensitive, responsive parenting and positive parent–infant relationships. The PIN programme was seen as helping to promote a nurturing and stimulating home environment, while projected outcomes for children included the promotion of child safety and positive physical, cognitive and socioemotional and behavioural development. Programme participation was also perceived as enhancing the social support available to parents, thus helping to improve parent well-being.
Distal outcomes
The PIN programme was perceived as helping to prevent negative developmental trajectories and promote long-term positive outcomes for children. Furthermore, it was understood to be the kind of intervention which would ultimately help to ameliorate and prevent developmental disadvantage and inequality. In a broad sense, the PIN programme was seen as a long-term community change strategy.
Intervention characteristics
Relative advantage, evidence strength and quality
Stakeholder reflections suggest that the PIN programme was perceived as an effective intervention which would lead to positive outcomes for the local community. Furthermore, the programme was seen as needs-based and as offering a holistic model of support for families which would enhance local services for parents and young children by: (1) developing practitioner capacity; (2) enhancing community engagement; and (3) promoting interagency service delivery: I think that you may not have as many mums falling through the net. [. . .] I think it is actually linking up a lot more people and even the community centres [and] I think there is a lot more communication in the services. (I2, program facilitator)
Programme complexity and design
The PIN programme was seen as a complex intervention, and this was understood to be a positive attribute because such multidimensionality was considered necessary to meet the varied and evolving needs of parents and infants. In line with this perspective, the collaborative delivery of supports within a joined-up, coordinated process of intervention, was also understood as important in positively influencing parenting outcomes: People are coming in the door with different needs and yet the program is able to respond to those needs of individuals in a group setting. (I8; program developer)
Despite the perceived complexity of the intervention, the programme was viewed as an attractive package of supports: It is the first time the Public Health Nurses have delivered and they are finding that the p is of great benefit, not just for the parents, but for their own practice as well. (I4; program facilitator)
Causal processes and implementation facilitators
Individuals
There is a wide range of stakeholders involved in PIN programme implementation, including practitioners, service providers and managers, as well as parents and infants who participate in the programme. Individual-level facilitative processes and factors are described below.
Parent and infant skills
Parent and child outcomes were identified not only as intervention outcomes but also as important causal processes. Positive parenting outcomes were seen as providing a foundation for positive child socioemotional, behavioural, language and cognitive development. Infant well-being was also understood, in turn, to provide a foundation for positive outcomes in later life. The fostering of proximal skills and well-being, therefore, was understood to be central to distal outcomes and the long-term success of the programme: If parents only realised how much they can shape and influence what these little people grow up and become and take ownership for their part in it . . . it kind of gives you the kick start in a positive supportive way. (I1; program developer)
Practitioner attributes
The skills of individual programme facilitators were also identified as important in achieving positive programme outcomes. These included both ‘hard’ skills (e.g. knowledge of programme delivery) and ‘soft’ skills (e.g. facilitators’ ability to build positive relationships with parents). Positive practitioner attitudes and specifically, commitment and buy-in for programme implementation, were further identified as helping to foster high-quality implementation practices: I think it depends on what type of person you are in terms of your delivery skills and how . . . You have to be a people person. (I18; program facilitator)
Inner setting
Climate and readiness for implementation
There was strong consensus among key stakeholders that a supportive climate for innovation was important. Resources important to generating a climate conducive to implementation are outlined in the sub-themes below:
1. Practical resources, administration and implementation support. Practical resources (e.g. appropriate venues, materials and technology/equipment) and administrative support, supplied by dedicated support staff and an implementation team, were identified as important facilitators of intervention delivery and programme effectiveness:
So that structure [Implementation team] has helped us to keep people informed, keep people on board. I suppose look at some of the issues that is coming up as well and try and address some of those implementation issues . . . (I8; program developer)
2. Access to information and knowledge. Training and facilitator support were understood to be critical to promoting ongoing, high-quality service delivery and, in turn, positive outcomes for programme participants. For example, all practitioners involved in the delivery of the Incredible Years (IY) components are trained (i.e. certified after attending 2–3 days training in the IYPBP/IYPTP) or accredited, while training in baby massage and first aid was also provided. Ongoing peer support and coaching are also provided for IY facilitators to strengthen facilitator skills and confidence:
I suppose we do a lot of hand holding initially because we want that support to be in place. (I10; program developer)
3. Networks and communication. The capacity of programme providers and the quality of delivery were seen as being strengthened by working alongside professionals with differential skills:
. . . you have two PHNs and a community worker facilitate in each group. [. . .] there is obviously conversations happening and links being made. (I2; program facilitator)
4. Leadership. Leadership was considered to be crucial to cultivating a receptive and positive implementation climate (e.g. buy-in for implementation and positive attitudes towards the intervention). Leaders included practitioners with strong commitment to implementation, as well as other strategically positioned personnel (e.g. service managers, programme staff). This kind of systems-level support for the programme was seen as enabling access to resources and facilitating collaboration, as well as buy-in for programme delivery:
Without that [leadership] I think it would have been like every other training, or lots of other training that people do and never use it but we were I suppose really supported through that. And that came from at the time my line manager and her passion for the program . . . (I12; program facilitator)
Programme processes
Processes that were identified as important intended causal mechanisms within the inner setting of programme delivery, included: (1) engaging parents; (2) intervention/behaviour change techniques; and (3) planning, reflecting and evaluating.
Engaging parents
Parents are recruited to the PIN programme via routine public health and community-based services. Relationship building between programme practitioners and parents was identified as key to engagement, particularly for ‘harder to reach’ parents. Home visits and support calls, as well as additional transportation and participation supports (e.g. childcare) were identified as key to overcoming barriers to engagement. Venue accessibility, comfort and attractiveness were also viewed as important facilitators of programme participation: When you have a personal relationship with someone it makes it much easier to work with that person. (I4; program facilitator)
Intervention/behaviour change techniques
The PIN programme is delivered through a combination of interacting and dynamic change processes which included behavioural and social learning techniques as ‘core’ causal processes within the PIN service model. Behavioural and social learning theories propose that the experiences of children and parents influence their skills and behaviours, while the parent-child relationship and interactions are also crucial in determining outcomes (Patterson, 1982). Specific behavioural techniques used within the PIN programme include role-plays and reinforcement to strengthen parenting skills and, in turn, influence child behaviour. A collaborative, facilitative approach to programme delivery is also used, whereby parent learning is promoted through a problem-solving approach (operationalised by parent-led group discussions). This approach focused on empowering parents to develop their own solutions to parenting challenges: The course is based on well-established behavioral/cognitive/social-learning, child development and relationship principles that describe how behaviors are learned and how they can be changed. At the core of this approach is the simple idea that people change as a result of the interactions they have on a daily basis with one another. (D5)
Creating a non-judgemental environment was also considered a critical causal mechanism within the PIN programme. Steps to generating a positive, supportive intervention context involved cultivating positive intra-group relationships and parents are encouraged to actively support one another both within and beyond the group sessions through buddy calls and/or social media/group messaging platforms and ‘meet-ups’ outside the group sessions: It’s a more collaborative way of working at the problem rather than me sitting dictatorial telling the person this is how you should do it all the time. So, it’s more positive I think. (I13; program facilitator)
Planning, reflecting and evaluating
Ongoing assessment of programme delivery processes, feedback on implementation and reflective service planning were identified as important to ensuring successful and sustained implementation of the PIN programme. Parent and facilitator feedback on programme delivery were gathered on a routine basis and used to inform service planning and development: We can reflect on what’s working and what isn’t working – what’s been good, what worked for some . . . (I15; program developer)
Outer setting
Three key themes were identified as relevant to the external implementation climate, including (1) community awareness and (2) inter-organisational collaboration.
Community awareness
Parent/community members’ awareness of, and positive attitudes towards early parenting supports/community-based services were understood as a mechanism for generating participation in the PIN programme and, over the longer run, engagement with community-based child and family supports: I would absolutely expect that once people are linked in and know there are services in the community that they’ll keep going that they’ll get very comfortable seeking out services and not because there’s anything wrong, simply because they’re there. (I9; program developer)
Interorganisational collaboration
Positive interactions and collaboration between organisations were understood to be a significant factor in proactive, efficient implementation planning. Interorganisational links were perceived as facilitating a flow of information and support within the early years/family service systems, while also improving coordination, understanding and links across various community-based organisations, thereby contributing to a broader process of service reform and the promotion of joined-up/interagency service delivery: These services are now beginning to communicate together. We have cross referral systems – there has been a significant shift in terms of how things run here. (I6; program developer)
Theoretical underpinnings of the PIN programme
An examination of the PIN programme reveals the utilisation of a mix of approaches aimed at changing parent and infant outcomes. The programme is informed by attachment theory (Ainsworth and Bowlby, 1991), bioecological theory (Bronfenbrenner, 1979) and behavioural and social learning theory (Patterson, 1982). For example, the PIN programme aims to foster attachment security, emotional well-being and cognitive development in children by achieving changes in parental sensitivity and responsiveness and fostering physical closeness between parents and infants. It also aims to change parents’ mental representations regarding their infant and in so doing, help to build parental understanding of their children’s state of mind. The model and its implementation can also be aligned with an ecological process-oriented approach to parenting and child development. Perspectives on the PIN programme reflect an emphasis on parent–child relationships and interactions which are seen as an important ‘engine of change’. The PIN programme also targets micro- and macro-level factors to influence child development; thus, parenting is understood as being multiply determined and the psychological resources of parents and contextual sources of stress ultimately influence their functioning and competence. Finally, the PIN programme applies behavioural and social learning theories through the use of specific behavioural techniques and peer-led approaches in the delivery of the PIN programme and by teaching parents to shape and influence child behaviour and development.
The PIN programme theory
The PIN programme theory (Figure 1) illustrates key assumptions underpinning the intervention. In brief, underpinning the programme is the assumption that universal, group-based early parenting intervention can help to promote positive outcomes for parents and their infants in the short-term, including parental competency, parent–infant bonding and positive infant health and well-being. In turn, these skills provide a foundation for ongoing positive developmental growth. Complex and multidimensional supports better meet the multiple and varied developmental needs of new parents and their infants and promote positive child developmental outcomes. Awareness of, and interest in, the PIN programme exists within the community and can facilitate parent engagement.
The model further illustrates an emphasis within the PIN programme, on a collaborative, multidimensional approach to programme delivery, as well as the use of implementation planning and reflective and evaluative practice, to drive high-quality implementation. Delivery processes which are rooted in peer-led, strength-focussed learning and behavioural and social learning principles, can help to strengthen parent well-being and competency and enable positive parenting. The role of resources, training and coaching, leadership, buy-in, inter-organisational networks and communication, and practitioner skills and qualities in generating high-quality programme delivery and intervention outcomes, are also addressed within the model. Finally, the theory indicates that the implementation of the PIN programme can, over the longer term, act as a change strategy and contribute to a process of community development and tackling inequality.
Discussion
This article describes the development of a programme theory for an early parenting intervention. The theory-building approach adopted here, enabled us to identify and describe the facilitative processes and factors by which the PIN programme attempts to promote positive parent and child outcomes. The application of the CFIR in the development of the PIN programme theory outlined here, also helped to frame the analysis within the broader implementation science literature, thereby enabling comparisons with other intervention studies. This, in turn, can help to build a broader understanding of the mechanisms that are important to the success and effectiveness of early parenting interventions and how they may play out in different contexts.
The PIN programme may be best described as a blended intervention model, combining multiple theoretical perspectives. Indeed, the programme offers a range of supports and aims to meet multiple parent and child needs over the course of an approximate 2-year period. It is vital, as with any programmes of this nature, to question whether and how this kind of lengthy and theoretically diverse programme can positively impact outcomes for parents and their young children. Indeed, one of the key assumptions inherent in the PIN programme theory, is that universal, broadly focussed interventions which address multiple needs over a longer period of time, are better able to address the challenges faced by parents in their parenting role (including more vulnerable and ‘hard to reach’ parents) than other shorter stand-alone interventions. In practice, this means that parents and their children with different levels of need and/or disadvantage should respond to, and gain benefit from, the intervention, while parents who engage with such a programme over a longer period of time will be satisfied with the programme and/or perceive it to adequately meet their needs.
There remains, however, much debate over the optimal type, nature and intensity of universal early parenting interventions. For example, brief, more-focussed interventions have been argued to be better for effecting change in parental behaviour (Bakermans-Kranenburg et al. 2012; Leijten et al., 2022). By contrast, other studies (e.g. Lindsay and Totsika, 2017) have argued that longer interventions have more favourable outcomes. However, our understanding of what constitutes best practice in early parenting interventions has been continually hampered by a lack of attention to the theoretical underpinnings of these kinds of interventions, as well as a lack of protocols for their implementation (Bakermans-Kranenburg et al., 2012). Importantly, the research outlined here, helps to address this gap, while the development of the PIN programme theory also allows for a more ‘contextualised’ critique of the effectiveness of the PIN programme theory, whereby the logic of the intervention can be assessed against current knowledge and existing literature. This allows for further exploration, whereby the moderating effects of contextual barriers on intervention outcomes can be explored.
It is widely recognised that stakeholder perceptions of, their responsiveness to, and meaningful engagement with, a new programme or practice are important to implementation (Greenhalgh et al., 2004; Laws et al., 2016). The findings outlined here highlight key stakeholders’ perceptions of the PIN programme. A programme theory such as the one developed here provides important insights into the extent to which a programme may be properly understood by key stakeholders, as well as the degree of consensus around the ingredients, actions and processes necessary for programme success. Notably, there was strong agreement among stakeholders regarding the importance of programme implementation, training, coaching and administration support. This finding is important. Knowledge and ‘know how’ in relation to an intervention are vital to effective implementation as is high-quality delivery and have been found to be crucial vital to programme effectiveness (Metz, 2013). However, some differences in understandings of the PIN programme and how it works, emerged across the various stakeholder groups. Notably, certain stakeholders – specifically the PIN programme developers – were more likely than other groups (i.e. facilitators) to identify certain implementation drivers, processes and practices as important levers for achieving programme outcomes. Thus, differing understandings of some elements of the PIN programme were apparent and varied in relation to participants’ roles vis-à-vis the programme.
In addition, programme evaluation and monitoring have been shown to be vital in ensuring effective delivery of evidence-based interventions (Fixsen et al., 2013). However, in the context of the PIN programme, the importance of programme monitoring and evaluation were more likely to be identified as important drivers of implementation and programme effectiveness by stakeholders involved in programme administration and development, than programme facilitators (i.e. practitioners involved in delivering the programme to parents and infants). Gaps in practitioners’/programme providers’ understanding of the role of programme monitoring and evaluation in programme implementation, may undermine the quality and effectiveness of programme delivery or contribute over time to programme drift (Aarons et al., 2011). It should be noted that conflicting perspectives regarding programme monitoring and evaluation were not in evidence in the current study (i.e. programme providers did not suggest that reflection and evaluation were unimportant to programme implementation).
It is also important to recognise the inherent complexity and multi-dimensionality of universal early interventions, such as the PIN programme and the many factors that influence their implementation (Birckmayer and Weiss, 2000; Powell et al., 2015). Importantly, implementation activity within the PIN programme involved a range of determinants and processes. Causal implementation processes which were seen as important to achieving anticipated programme outcomes, operate at both micro and macro levels within the PIN programme ecosystem, and interconnections between different levels of the PIN programme must be noted. Processes and outcomes at one level can be seen as interacting with and influencing, processes and outcomes at other levels within the programme ecosystem. This kind of multi-dimensional approach is important as it helps to promote a deeper understanding of how interactive factors, contexts, processes and practices are intended to shape programme outcomes and, ultimately, contribute to programme success (Davidoff et al., 2015; Durlak and DuPre, 2008). For instance, the PIN programme theory outlined here illustrates how decisions regarding administrative support and implementation planning at a macro level can help to build commitment and buy-in for implementation among programme providers involved in the micro-context of programme implementation. These capacities and skills of programme providers can contribute, in turn, to parent engagement with the programme. Reciprocal interactions between actors within the intervention environment play a crucial role in shaping programme outcomes. These interactions may be bidirectional and can occur sequentially, highlighting the importance of context for programme effectiveness. Overall, proximal and distal stimuli ranging from individual stakeholder’ characteristics to the broader socio-political context, can impact implementation within early years and family service settings.
Study strengths and limitations
The programme theory described here reflects the perspectives of programme providers rather than programme users. Later stages of the evaluation and exploration of programme implementation and causal mechanisms will involve the analysis of both qualitative and quantitative data obtained from parents, as well as a broader sample of practitioners involved in programme delivery. This component of the research helped towards the development of a theory underpinning a complex early parenting intervention but did not explore the effectiveness of the theory. An accompanying non-randomised trial will explore the impact of the PIN programme on the outcomes for parents and their young children. Additional ‘case study’ exploration to gain a deeper understanding of the mechanisms underpinning the PIN programme and their likely impacts was not carried out due to practical and resource limitations.
This study was based on a range of data sources to build an in-depth understanding of the PIN programme, as well as the ‘real-time’ collection of data encompassing the early stages of intervention delivery. Purposive sampling was used to ensure validity and trustworthiness (Lincoln and Guba, 1986), while respondent validation was also employed in the development of the PIN programme theory. The assumptions underpinning complex interventions, their intended outcomes and how those outcomes will be achieved, is not always clear at the outset of programme delivery. The guidelines outlined in the MRC framework for process evaluations, underscore the importance of developing a theoretical understanding of the likely process of change in the earliest stages of evaluation; they further emphasise that this should be undertaken regardless of whether the researcher is developing the intervention or evaluating an existing one. Here, in line with these best practice recommendations, we developed a programme theory which helps to highlight the theoretical underpinnings and causal assumptions inherent in the new PIN programme. The approach outlined here may also serve as a guide which can help researchers and programme developers elsewhere in understanding and producing programme theories. The development of this model can also serve to guide the development and prioritisation of research questions regarding how programme components, implementation processes and contextual factors interact, thereby helping to build a better understanding of how these kinds of programmes work. For instance, the programme theory here highlights the practitioner knowledge, skills and qualities as important change mechanisms. In turn, this informed the development of further research questions focused on interactions between practitioners and parents. However, it is also vital to recognise that these interactions occur within and are influenced by the inner context of programme delivery. From this perspective, the boundaries between implementation and context are blurred and contextual factors can be seen as driving forces required for successful implementation (Nilsen and Bernhardsson, 2019; Squires et al., 2015). For example, practitioners’ skills and capacities to successfully engage parents and promote behaviour change are intertwined with the training and coaching they receive, as well as the resources and supports available to them. Where contexts vary, implementation efforts will likely yield differential outcomes. Overall, this highlights the importance of considering context and how contextual factors interplay with and influence programme delivery and outcomes during programme development and implementation planning phases (Li et al., 2018).
Conclusion
This article describes a theory-driven approach to understanding the causal mechanisms underlying a complex group-based early parenting intervention programme. Innovation in child and family services is a considerable challenge and there remains a lack of theoretically guided research exploring the processes, factors and conditions which influence the success (or otherwise) of evidence-based early parenting interventions (Olofsson et al., 2016). Theory-driven evaluation can assist in understanding the applicability of parent support innovations to child and family service settings while also helping to address some of the current gaps in the literature regarding the effectiveness of early parenting interventions. The development of the programme theory outlined here represents an important step towards, first, identifying patterns of interaction between the programme, the stakeholders involved, and the context in which the programme is delivered, and second, the extent to which these interactions shape, either positively or negatively, the implementation and impact of the programme.
Footnotes
Authors’ note
This work was carried out in Maynooth University Department of Psychology.
Data availability statement
Data are available from the authors upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research is funded by the Health Research Board in Ireland through its ‘Collaborative Applied Research Grants scheme in Population Health and Health Services Research 2012’ which was awarded to Sinead McGilloway as the Principal Investigator (CARG/2012/17).
Ethical approval
Ethical approval for this study was obtained from Maynooth University Social Research Ethics Sub-Committee and the Health Service Executive (HSE) North East Area Research Ethics Committee. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Written informed consent was obtained from all participants in the study.