
Abstract
Recently, several authors have called for a critical assessment of the normative dimensions of evaluation practice. This article responds to this call by demonstrating how evaluation practice can be enriched through deliberate engagement with care ethics. Care ethics has a relational and practice view of morality and places caring relationships and responsibilities at the forefront of our being in the world. We will demonstrate how care ethics, in particular Joan Tronto’s moral-political theory of democratic caring, can help evaluators to reshape our way of working by placing caring and relationality at the centre of our evaluative work. Care ethics as a normative orientation for evaluation stretches beyond professional codes of conduct, and rule- or principled-based behaviour. It is part of everything we do or not do, how we interact with others, and what kinds of relationships we forge in our practice. This is illustrated with two examples: a democratic evaluation of a programme for refugee children in Sweden; and a responsive evaluation of a programme for neighbours of people with an intellectual disability in The Netherlands. Both examples show that a caring ethos offers a promising pathway to address the larger political, public issues of our times through the interrogation of un-caring practices. We conclude a caring ethos can help evaluators to strengthen a caring society that builds on people’s deeply felt need to care, to relate, and to connect within and across communities.
Introduction
Evaluation is a practice at the interface between academic science and society, and has a practical intent; it aims at the solution of practical questions, and requires multi- and interdisciplinary approaches. It builds upon scientific knowledge, and adjusts to the scientific communities and validity criteria. However, the practice of evaluation is more than just a scientific and technical enterprise. Evaluation also has a normative content and character. This normativity of the evaluation practice is our focus. More precisely, we aim to examine the ethics of the enterprise of evaluation itself. Relevant questions are ‘What actions and impact in evaluation are good and desirable? How should evaluators act?’ What are the aspirations of the practice, for example, to produce evaluative knowledge, contribute to democratic decision-making, enhance critical thinking about values, and advance social justice?
House (1993) was among the first who pointed out that in a capitalist society, public organizations increasingly needed to justify their practices through formal evaluations based on standard criteria such as efficiency and economic productivity. He criticized evaluation practices confined to assessing whether objectives were realized, because these cannot take into account moral questions concerning the public good and good public policymaking (House and Howe, 1999). So, House made it clear that the enterprise of evaluation needed to reflect on its own normativity, which we could not deny by referring to objectivity. He also pointed out that engagement with external stakeholders, among them commercialized parties, implied a responsibility to include and protect critical voices. Likewise, others (e.g. Schwandt, 1997, 2005; Dahler-Larsen, 2012; Greene, 1999) have paid attention to how current modes of governance and evaluation practices shape and affect welfare practices. For example, evaluations can reinforce a dominant and measurable notion of quality in welfare service and create a need for measuring performance of services recurrently (Noordegraaf and Abma, 2003). However, introducing new public management and evaluation systems in, for example, eldercare, can be highly contested due to moral and ethical disagreements about their value in eldercare services and programmes (Szebehely and Trydegård, 2012).
As an alternative to the scientific and claimed value-free evaluation practice, Ernest House and Barry MacDonald proposed to advance democratic ideals as a normative orientation for evaluation. Importantly, House and MacDonald argued that the normative orientation of evaluation should not be denied and acknowledged (House and Howe, 1999). Drawing significantly on their mentors, Greene and Simons (2018) have argued that evaluation may not fulfil its democratizing vision if it is not prepared to deliberately take into account a broad and inclusive array of perspectives and values, in particular, social justice and equity. The concern that economic values are usually privileged over other values in evaluation practice, and also considered normative, led a group of evaluators and ethicists to explore the potential of care ethics to enrich the evaluation practice (Visse and Abma, 2018).
The purpose of this article is to explore the enriching value of an ethics of care as a normative orientation for the practice of evaluation. Such a normative orientation is grounded in a particular moral-political theory arising out of a literature on care ethics (e.g. Held, 2006; Tronto, 1993, 2010, 2013, 2016). In short, we will discuss how care ethics as a moral and political theory offers a new way of understanding the moral purpose of evaluation in society.
After presenting how others have addressed the normativity of evaluation, we will offer a portrait of care ethics and its recent history, what its main ideas are, and what it has to offer our field as a ‘new’ normative orientation. This portrait will be illustrated with examples, followed by a discussion of issues that need further examination.
Concerns over the normative orientation of evaluation
We are not the only ones calling for reconsidering the normativity of our practice. Stame (2018) argued that ethics in evaluation are related to critical and moral dimensions of the public good, including the values at stake for the people involved in the evaluation, as well as the general public and citizenry. Indeed, much of our work uncritically reproduces dominant societal values and norms and thereby privileges white and male values, individualism, and rationality (Ofir, 2018). Schwandt (2018a) also called for the need to acknowledge that evaluation is not only a technical enterprise but also that its ‘goodness’ is an ethical matter. This stretches beyond professional codes of conduct, and rule-or principled-based behaviour. It is part of everything we do or not do, how we interact with others, and what kinds of relationships we forge in our practice.
Also, outside our field there is a discontent about how our current neo-liberal ideologies are penetrating our personal lives and the broader society. Sociologist Bauman and Donskis (2014) in a critical essay pointed to the dominance of market values: ‘A consumerist attitude may lubricate the wheels of the economy, but it sprinkles sand into the bearings of morality’ (p. 150). Philosopher Kunneman (2012, 2017) is concerned that our rationality and science-based knowledge cannot pay adequate attention to the important moral and existential issues of our times. In another field, a group of psychologists is ringing the alarm bell with their concerns about the rising amount of depression, violence, and signs that people feel lost and alienated from others and even from their own selves. This ‘crisis of connection’ is indeed worrying and part of our globalized, patriarchal, and hyper-individualized world (Way et al., 2018). The unease is especially felt in those parts of society that are less well-off, for example, among those who are vulnerable or sick, old or in need of financial, emotional, loving support.
Care ethics, an emerging interdisciplinary field of inquiry, stresses the importance of being listened to carefully and heard with respect (Fisher and Tronto, 1990; Leget et al., 2019; Tronto, 2013). Care ethics directs our attention to the need for responsiveness in relationships, and for paying attention to needs, listening, and responding to people on their own terms and in their own right. Politically, care ethics urges us to act with mindfulness of the broader structural power constellations that reproduce oppression, marginalization, and exclusion (Engster and Hamington, 2015; Tronto, 2013). In this regard, care ethics has much in common with democratic, participatory, and responsive approaches within the field of evaluation (Visse and Abma, 2018). Yet, we think that caring and care ethics have more to offer to the evaluation field, and that this contribution is distinctive and important as a normative orientation for the practice of evaluation. Therefore, in this article, we explore how the vocabulary and ideas of care ethics may critically enrich evaluation, and guide and inspire us to revitalize the moral and human dimensions of our practice and theory.
Care ethics: Theoretical background
Care ethics departs from the critical notion that caring is essential to being alive (as a human being) which is reflected in the broad definition of caring stated below: We suggest caring be viewed as species activity that includes everything that we do to maintain, continue and repair our ‘world’ so that we can live in it as well as possible. That world includes our bodies, ourselves, and our environment, all of which we seek to interweave in a complex life-sustaining web. (Fisher and Tronto, 1990: 40–41)
People and other species can only develop and flourish in caring relationships (Held, 2006; Tronto, 1993). There is no beginning or endpoint in caring, because it is part of what it means to be alive, and thereby also part of our responsibility. Valuing care as fundamental to life is part of a feminist critique on the structural undervaluation of care – both paid and unpaid – in our society, in terms of money, status and recognition (Hamington, 2018). Care as a pivotal activity is inclusive of all caring activities, not just cooking and nursing, but also activities such as caring for our planet, our natural habitat, and the education of our children. Many care ethicists are concerned that the gendered work that is necessary to reproduce our lives gets more and more undermined by economic profit, more hours of work and less state support for social welfare.
Another critical issue in care ethics is the notion that every human being is vulnerable, yet also biologically carries the disposition to care, rooted in the natural qualities of care (Jaggar, 2000). This expectation challenges the prevailing Western idea that people are fully autonomous because they are free from interference from other people (Verkerk, 2001). Relational autonomy – the idea that people are autonomous because of their interdependency and relations with others – is proposed as an alternative to autonomy as self-determination. Relational autonomy recognizes that we are fully social, relational and affective beings, and that few of us can live up to the norms of autonomy and self-sufficiency for our entire lifetimes (Kittay, 2011). The relevance for evaluation is illustrated with an example: A team of evaluators who evaluated self-management programmes for older people started conversations with healthcare professionals and service-users on the meaning of self-sufficiency. Soon it appeared that many older people could no longer attend social activities, because they were too tired of self-caring activities. It was the support of the nurses that enabled them to be autonomous. This opened the eyes of the policymakers and managers that care and autonomy are not opposites, but that care actually constitutes autonomy.
The theory of care ethics is also a response to traditional ethical theories that are based on universalist and abstract principles and rules, and rational considerations as the sole and main guidance to make ethical decisions. Within care ethics the notion of ethics – what should be done to live well and what a ‘good’ life entails – is more than a rule-based affair or a matter of following principles. Care ethicists acknowledge that situations are often more complex than ethical principles and codes can capture, and someone sometimes needs to break the rule to do justice to the situation (Gilligan, 1982). The following example shows the relevance for evaluation. In the evaluation of a day care centre for various service-users (people with mental and physical disabilities) it was noted that due to conflicting laws and bureaucratic regimes, participants received different services. This was felt as unjust by the participants, including the staff, who responded by small acts of solidarity and everyday activism, like sharing coffee and costs. Although they violated the rules the evaluators made, a case to their commissioners that this was actually an ethically sound response to an unjust situation.
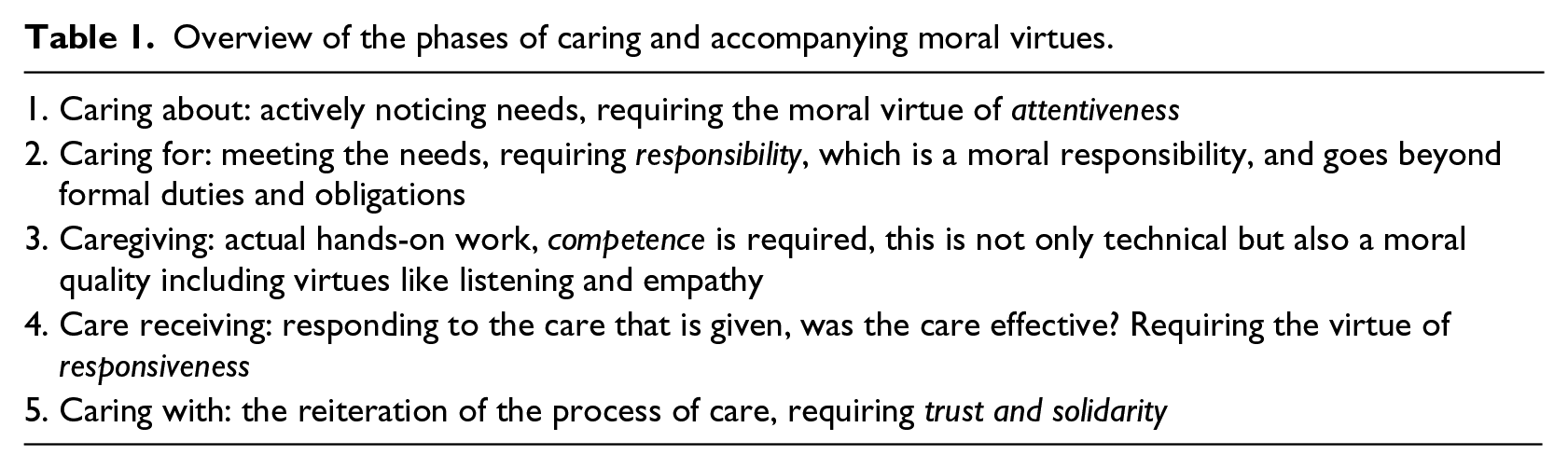
Care ethics is political, because it centrals the critical evaluation of care. Not all care is morally good, and care ethicists have developed ideas on what good caring means (Barnes et al., 2015). Tronto (2012), for instance, has specified that good caring implies intersubjectivity; good care is the outcome of a dialogic process between caregiver and care-receiver, and cannot be decided upon for someone. Good care is attuned to needs and the outcome of a joint, democratic decision (Tronto, 2016). As care needs may change, good care is conceived as a cyclical process which requires moral virtues (Tronto, 1993, 2013) like attentiveness, responsibility, competence, responsiveness and solidarity (see Table 1 for overview). There are also dangers and risks to good caring, including paternalism, parochialism, sentimentalism, and inadequate conditions for care. And as we will show below, these critical notions about the moral goodness of care are helpful as a normative orientation to our evaluation practice.
Overview of the phases of caring and accompanying moral virtues.
More recently this political nature of care ethics has been further stipulated in Tronto’s (2013) plea to redefine democracy as developing shared understandings of caring responsibilities: Democratic politics should centre upon assigning responsibilities for care, and for ensuring that democratic citizens are as capable as possible of participating in this assignment of responsibilities. (p. 30)
Others followed this reconstruction of care ethics as a political construct (Hankivsky, 2014; Robinson, 2015; Vosman and Niemeijer, 2017; Zembylas et al., 2014), seeking to influence caring institutions and policy contexts through a critical interrogation of inequities in carers’ pay, working conditions and access to resources. These politically engaged actions parallel the work of democratic evaluators who democratize findings in order to influence the policy debate to pay attention to epistemic justice and to accord more resources to programmes of demonstrable democratic worth.
Care ethics as a normative orientation in the practice of evaluation
In the previous section, we presented care ethics in theory. Translating these ideas into a normative orientation for the practice of evaluation creates a number of issues. The first is linked to power and to the political issue of ‘who determines what good care is, and who benefits from good care?’ Is the evaluator in charge of this judgement, or is this a collective decision among the participants, including the broader public? A second is the need to think about the normative question of what ‘goodness’ means and how we decide, on what grounds and values, that the caring approach we have taken in our evaluation is responsive to the needs and interests of all. Furthermore, we need to decide whether we wish to focus on the micro-relations of caring when we evaluate, or take a more organizational perspective, which might include caring institutions, or take an even more socio-political perspective on caring societies and structural inequalities. Stakeholders in an evaluation may have different ideas on how to create a caring context and how to deal with the plurality of perspectives and the values which under pin them.
In response to these challenges, we suggest locating our perspective in Tronto’s conception of good care and democratic caring, and integrating this perspective with democratic evaluation (Greene, 2006; House and Howe, 1999; Mertens, 2009; Simons, 2015), in tandem with the related approaches of responsive and participatory evaluation (Abma, 2006; Abma and Widdershoven, 2008; Visse et al., 2015). Tronto (2016) makes a useful distinction between protective and democratic care. Protective care fits into a hierarchical framework in which certain highly placed people protect those who are assumed to be weak and vulnerable. In contrast, Tronto (2016) conceptualizes democratic care as follows: What caring democracy equalizes, then, are not acts of caregiving, but responsibilities for care – and as a prerequisite, the discussions about how those responsibilities are being allocated . . . and assuring that everyone can participate in those allocations of care as completely as possible. (p. 6)
The focus on responsibility and joint decision-making in democratic caring has much in common with democratic, responsive and participatory evaluations. Democratic evaluation sets out to engage with and advance democratic values within the very process of the evaluation, making sure that all those with a legitimate interest in the evaluation have their perspectives heard and represented (Greene, 1997, 2006, 2010; Greene and Simons, 2018; Mertens, 2009; Simons and Greene, 2014). With this comes the ambition to ensure that all beneficiaries and citizens have access to the results of evaluations so they can engage in debate about the issues at stake. Argumentation and deliberation are often part of democratic evaluation during and after the evaluation process (Hanberger, 2006, 2018). Responsive evaluation is anchored in a hermeneutic tradition and strives for heightened personal and mutual understanding among those involved through dialogue. It is concerned with moral learning and relational responsibilities (Abma et al., 2017; Abma and Widdershoven, 2008; Schwandt, 2002; Visse et al., 2012).
Generally, a caring orientation in evaluation implies conceiving and accounting for care as it manifests itself in our own practice and the practices we evaluate. Taking a leaf from the broader political purpose of care ethics promoted by Tronto, we contend that action to promote a democratic caring society can and needs to enrich and expand evaluation practices. We will further this line of thought through two case examples.
Democratic caring and discursive democratic evaluation
In practices of supporting the refugee children, it soon became clear that some caregivers perceived the children as vulnerable, traumatized, and in need of psychiatric care. Others adopted a more skeptical attitude by suggesting that the children should not get too many services and support. It would make them spoiled: ‘We create small request machines of these young persons’. Furthermore, some caregivers considered them as strong, resilient individuals, and as a potential resource to society. With this view, the challenge was how to support them to become responsible adults: ‘You have to understand and explain that they are children that need support and coaching, not treatment and care’. The children appreciated empathy, practical support, and caregivers who were engaged.
This vignette comes from Hanberger (2018) and is based on a discursive democratic approach to evaluation of an integration programme for refugee children in Sweden. It reflects not only a highly sensitive topic but also the various, even conflicting, perspectives on care for young people with a refugee and minority background (Hanbeger, 2010). It is crucial to notice that these perspectives are grounded in various values endowed to and related to what good care is, and will thus lead to different evaluations of the practice by the different stakeholders.
The values of care conflict here and relate to different notions of the needs of the children. We will show that care ethics helps to understand these varied values and conceptions of good care. There are those who think the children are in need of medical or psychiatric care and hence focus on problems and treatment of these problems. They perceive the children as traumatized and believe these traumas need to be worked out individually. In contrast, there are those who are convinced that the children just need support (versus medical specialized care). These people perceive the children as strong, resilient persons and the challenge is to support and encourage them. These viewpoints and underlying value commitments conflict. The first approach – to offer specialized treatment – is more or less paternalistic and can even be stigmatizing. It decreases the power of care users, because there is a focus on medical solutions offered by and controlled by professionals and experts. The resilience approach focuses on identifying general resources to handle tensions and adversarial circumstances in life. The focus is on staying healthy and being well rather than on disease and illness processes. Power remains in the hands of people themselves.
Still another approach can be recognized, one that starts from distrust and the idea that children from abroad may misuse the care and support given to them. Perhaps this standpoint is also informed by racist and nationalist ideas. Care should only be available for our ‘own’ children; here we see the risk of what Tronto (2016) calls parochialism. If the youngsters are conceived as ‘spoiled’, the problem is understood as a ‘cut down problem’; youngsters should, for their own best interest, be offered less care and services, and taught to take more responsibility. Care becomes a disciplinary activity.
All these approaches to care, but in particular the first and the last, run the risk of turning into what Tronto (2016) has called protective (versus democratic) care. As we have seen, protective care fits into a hierarchical framework where some higher placed persons protect those who are assigned, and thereby perceived to be, weak and vulnerable. Protective care is informed by masculine values and may lead to resistance and non-cooperation. Non-cooperation can occur when care-receivers are not satisfied with the care they receive. Hanberger and his team heard the fear for noncompliance and disobedience in this kind of response among some of the caregivers. The evaluation team accepted the responsibility that is part of the normative orientation of an ethic of care to zoom in on the moral issues that stem from unequal relationships, in this instance, the dependency of the youngsters. The evaluators were well aware that ideas about care were part of a political context, and they acknowledged that care patterns are the outcome of socio-political configurations that need not just be taken for granted when one is striving to attend to caring needs of young people. As pointed out before, democratic care is a joint and intersubjective activity. Hanberger (2018) as evaluator noticed that joint decision-making about caring responsibilities fit better with the focus on resilience of the children, because resilience acknowledges that even vulnerable children have their strengths and are thus capable of sharing power to make decisions concerning their lives and well-being. In that way, he challenged other notions of good care. Furthermore, democratic caring included the willingness to reflect on interactions with the children and reflexively investigate how the attitude of the caregivers led to acts of resistance and recalcitrance among youngsters. Hanberger et al. (2016) concluded that democratic caring was enacted when caregivers deliberated on how to manage various challenges and joint-responsibilities in networks for youngsters.
In line with the democratic approach Hanberger adopted in this study, the voices of the children and their perspectives were also included. Indeed, the children had multiple ideas on what they needed, especially what they liked or not in terms of how the professionals interacted with them. They were pleased with most of the physical spaces where they stayed, with a few exceptions. A lack of natural meeting-places with Swedish youths and obstacles to get in touch with them were perceived as problematic. What was highly valued by the children, and thus conceived as good and genuine care, was if the staff were engaged, showed empathy, demonstrated caring, encouraged the children, and provided practical support. The children also underscored that caregivers should have the appropriate education and experience to provide good care and support. This resonates with Tronto’s virtues of good care, including attentiveness, responsibility and competence.
From this example, we can see how an ethics of care orientation can be adopted and integrated in the discursive democratic evaluation approach. Ethics of care helped to illuminate the various perspectives on what good care meant and to articulate underlying assumptions. It offered a moral compass to deepen the dialogue among stakeholders and offer new perspectives on what good care can entail in this particular situation. So, working from an ethics of care, the evaluation team felt a responsibility to foster these dialogues and deliberations.
Finally, Hanberger pointed out that for him, while care was an important orientation, it was not the only one. Safety and security were also included as values, as well as the organization of care within legal and human rights frameworks, including the Convention on the Rights of the Child. This shows how care and justice were combined.
Caring as a relational responsibility to create space for silent voices and address epistemic injustice
Harry is one of the most fascinating characters I have ever met. He has a small, hunching posture and two remarkably blue eyes. In his neighbourhood, Harry is well known for the way in which he frequently initiates physically intimate contact with people he meets on the street. After establishing eye contact, he tends to approach them rapidly with an excited smile on his face, grab their hand or arm, and give them a long, piercing look from very close range. While doing so, he never speaks a word. Instead, he tends to moan, grunt, or make bark-like sounds. The first time we met, I was utterly confused and alienated by Harry’s candid advances. I felt a strong urge to push him back and walk away. How was I supposed to communicate with him in a reciprocal way?
In the above vignette, Gustaaf Bos introduces how he wrestled to relate to and include in research, the voice of a person who hardly speaks.
This auto-ethnographic reflection was written as part of a responsive evaluation of a reversed integration programme (Bos, 2016). It concerns Dutch long-term care institutions that invite citizens to live on the institutional property, and become neighbours of people with an intellectual disability. The mix of unease and value Bos endowed to bodily experiences is striking, and well represents Dahlberg’s (2018) phenomenological approach to understand people and their needs well: Let us stay some more in the question of how we perceive other persons and their emotions without having direct access to their intentionality, and look at an approach that is often referred to as a way to understand others, namely empathy . . . in empathy (Einfülung) [we] form a ‘sphere of ownness’ from which we understand ‘an-other’ as another self, as an alter ego. . . . The sphere of ownness, which is prior to any understanding of empathy as well as to all other higher forms of social consciousness, serves as the bodily framework from which we understand another person. (p. xx)
Likewise in care ethics, it is considered very important to pay attention to emotions. This is grounded in the notion that good care requires the embracing rather than ‘glossing over’ of feelings. The latter implies a superficial engagement with the emotional complexities of caring and responsibility; what is required is a much deeper and emotionally challenging engagement that redefines our relationships (Zembylas et al., 2014). In his ethnographic work, Bos experienced feelings and emotions as intelligent phenomena that required thoughtful emotional work, which, in turn, helped him to understand what Harry needed and to establish their relationship.
Bos (in Bos and Abma, 2018) reflects that he was repeatedly reminded of the hegemonic position that academic knowledge and rationality tend to hold in the contemporary (care) discourses. Many care professionals, family members, volunteers, and new residents treated him as if he, as an academic evaluator, would know what was best when it came to encounters between people with and without intellectual disabilities (‘You are one of the smart guys’). This prejudice was at odds with the dialogical character of responsive evaluation and the pursuit to produce shared knowledge in a horizontal way. It was due to moments like those described in the vignette that Bos became especially aware of the impact of asymmetrical relations and the fragile relation of trust among the stakeholders in a responsive research project. Bos experienced that power was at play, and that people with a disability did not always feel safe to share their experiences. He reflects, All this urged me once more to take as much time as possible to get ‘acquainted with’ the perspectives of the people involved, with special attention for those who were at the highest risk of being ignored, stigmatized or marginalized. (Bos and Abma, 2018: 168)
We interpret this as a caring attentiveness to inequalities and epistemic injustice (Fricker, 2007; Greene and Simons, 2018). Epistemic injustice refers to a situation when a human subject is wronged in her capacity as a knower (Fricker, 2007). We further interpret this as one of the phases of Tronto’s care ethics, namely caring about, that is often valued highly by patients and service-users, but not always given equal weight in the practice of caring.
Getting to know and understand Harry required Gustaaf Bos to leave his comfort zone (his scientific distance and verbal weaponry) and to respond viscerally to the context. He did this by following Harry more intuitively, without the aim of catching him in one of his (academically created) frames of reference. This ‘open’ attitude immediately changed the interaction with Harry: While making some photos of the jumpy goats, I suddenly notice Harry in the middle of the pasture, some 30 metres ahead. He is running around between the goats, making yelp-like sounds. As soon as he sees me, he hurries in my direction. I keep looking at him. Harry runs towards the fence that surrounds the pasture and leniently climbs over it. He grunts and walks towards me, with an expecting expression on his face. When I cannot stand the awkwardness of this situation any longer, I knock on the wooden bench beside us and sit down. Harry immediately sits down next to me. I squeeze my eyes, enjoying the brightness. Looking beside me, I see that Harry is also squeezing his eyes in the sunlight. After a while, he looks back at me, smiling. I return a smile. When I look into the pasture again, he does the same. And when I look back at him again, he acts likewise. We keep exchanging gazes and smiles, without words or sounds. (Field notes 27 January 2012: 38–39 in Bos and Abma, 2018: 171)
Bos and Abma (2018) learned to enter a relational-experimental space, that is, a space wherein, it is acknowledged that strangeness is not an essential quality of another person but always the product of a ‘ourselves in relation to this person: no one is ever strange on his own’ (p. 174). This relational character of strangeness is crucial, because this inspires an interpersonal quest for more genuine encounters. From a care ethical perspective, we can see that in the story of Harry and Gustaaf the spark of energy between them began to flow when Gustaaf opened himself up by becoming aware of his own vulnerability or disability. Through a reflexive stance, Gustaaf learned that he had to give up his control over the situation – his privilege – in order to come to know and appreciate how to develop an authentic relationship with Harry. This rebalancing of power created a situation for mutuality, where both were giving and receiving affectionate attention, and this created a feeling of mutual belonging and interconnectedness, and generated what is called ‘pathic’ (including empathic, compassionate) knowledge (Van Manen and Shuying, 2002).
These encounters between the evaluator and Harry shed light on some of the limits of our current evaluation approaches and social scientific research more in general. Verbal and cognitive borders needed to be crossed. Dialogue was redefined as both interaction and motion, where participants responded to each other, each other’s position and each other’s particularity – by means of their language, bodies, attitudes and/or emotions (Bos, 2016). Dialogue was re-enacted as a ‘dia-logos’ (literally: between logics) with an ‘intercorporal’ character. Thus, when we desire to understand someone else for the purpose of caring and evaluation, we need not only attend to words but to everything that happens in-between.
This example shows the potential of an ethics of care to refine our notions of what it means to evaluate, and the relational responsibilities this brings especially when there are asymmetries and epistemic injustice. Epistemic injustice relates the value of knowledge to power structures, in which certain speakers and certain forms of knowledge are more valued than others. Especially clients and service-users run the risk of not being acknowledged as credible knowers because of cognitive or other limitations, like in the example of Harry. When a human subject is wronged in her capacity as a knower, then we are all wronged in our capacity as knowers.
The example shows that all too easily we are drawn to accept the status quo, shun uncomfortable situations or hide behind theatrical performances in order to protect ourselves from strangeness (Bos and Abma, 2018). This not only leads to feelings of alienation and inauthenticity, but also reiterates existing power relations. Perhaps, it is what Tronto would call parochialism; attending to the interests and needs of those we understand because they are close to us socially. To be real, authentic and genuine in the relationships we generate in evaluation is daring and requires courage. People like Harry or children immediately sense when we are unreal or pretending, and they lose trust in us. Many examples show that if we invest in the relational, we are not only supporting a critical human value but also advancing the scope, relevance, and actionability of our evaluation work. Such work creates room moral and existential issues, the kind of knowledge that is often silenced in scientific or commercialized fields of inquiry wherein economic and political interest tend to prevail (Kunneman, 2017).
Discussion
The field of evaluation is ‘alarmed’, to phrase Schwandt (2018b), ‘at excessive emphasis on evidence-based best practices and at efforts to assign the highest value to empirical evidence gathered in an apolitical, technical fashion’ (p. vii). While this may help the economy and ever increasing individual competition (Way et al., 2018), it leaves us bare on issues of morality and human-ness (Kunneman, 2017). This article has explored the enriching value of an ethics of care as a normative orientation for the practice of evaluation. This orientation is grounded in the moral-political theories on ethics of care that endow an ethical meaning to relationships. It is in relationships that people express their needs, communicate and receive care and recognition. As such an ethics of care offers a normative orientation, widens the scope of values that matter to people, and encourages deliberation and dialogue about what good care and caring means. This is in line with ongoing calls to rethink and critically reflect on the normative nature of evaluation practice (Greene, 1999; Schwandt, 2018a; Stake, 2004; Stame, 2018).
We have set out how a theory of care ethics (mainly adopted from Tronto) can inform evaluation and how it can be practised. Caring evaluation, as we view it, is grounded in the relational caring advanced by Tronto (1993, 2013) and in democratic evaluation (Hanberger, 2018; Simons and Greene, 2014, 2018) as well as responsive evaluation (Baur et al., 2017; Bos and Abma, 2018; Visse et al., 2015). An ethical-relational approach is needed which puts relationships at the centre to balance the dominance of certain methodologies in evaluation and to restore connections and fragmentation in our societies (Way et al., 2018).
Caring as a normative orientation for evaluation practices promotes a democratic caring society, anchored in caring norms and values that are fundamental to all living beings and should be the responsibility of every human being. Care complements and also challenges democratic and human rights principles, rules of law, and the 2030 agenda for sustainable development (Engster, 2007). Care ethics as a normative orientation fosters empathy, interdependence and connection. Care ethics offers a broad epistemological repertoire of feelings and emotions, as well as concrete and contextualized answers to morally complex situations (Gilligan, 1982). In evaluation practice, these could well be highlighted and explored more than at present.
Evaluators may not consider their work as a form of care, and assume that care and caring are confined to caring work to help the sick, the weak and the poor. We contend that care and caring are important in all contexts that involve human action or interaction or engagement. Our case examples were taken from the social fields of health care and social well-being, but we see possibilities to integrate a care ethics approach in the evaluation of other domains, including our environment and natural habitat. Recently, more scholars have adopted a care ethics view in disciplines like education (Isserles, 2018; Lerttharakul, 2018; Noddings, 1984; Freeman and Hall, 2012), technology (Cassidy, 2018; Goerisch, 2018; Wynsberghe, 2016), and the fields of business and economics (Folbre and Smith, 2017), sustainability leadership (Nicholson and Kurucz, 2017) and care for our natural environment (Whyte and Cuomo, 2017). As many of us are working on sustainability issues the work done by Whyte and Cuomo (2017) on care ethics for our natural world can serve as a source of inspiration. These authors stress the importance of empowering communities to care for themselves and the social and ecological communities in which their lives and interests are interwoven. They have demonstrated how care ethics offers a rich ground for rethinking and reclaiming the nature and depth of diverse relationships as the fabric of social and ecological being. Evaluators may translate such an orientation to their work.
Following the broad relational and socio-political interpretation presented here, care and evaluation at least overlap. Evaluators (like all good caregivers) are relational beings just like any other person. Their evaluation practice entails a careful socio-political process of building and maintaining relational webs with stakeholders and programme participants. They acknowledge the asymmetrical power relations they have with stakeholders, and reflexively attend to power, being alert not to dominate, while simultaneously using difference consciously and productively. Both care professionals and evaluators need to be willing to engage in relational acts of care, in order to become familiar with the lifeworlds of the people with whom they interact, what matters to these people, and why. This being said, there are still differences in role and responsibilities which are likely to lead to different decisions and practices in our respective fields – of evaluation and caring. As Simons and Greene (2018) point out, ‘there are certain parameters of our fields that require different codes of practice and that have different consequences for people in our respective professions’ (p. 100). What the specific responsibilities of evaluators are and where the boundaries of our caring responsibilities lie, will require more dialogue and debate among ourselves as well as with scholars from other disciplines and our public partners.
We have proposed a particular way to bridge evaluation and care ethics, one that is grounded in a synergy between democratic caring and democratic and responsive evaluation. Hanberger (2018) used Tronto’s (2013) political care theory to deepen the understanding of the conflicting values and caring perspectives on refugee children in Sweden. The notions of ‘protective’ versus ‘democratic’ caring offered a new lens to understand the deliberative dialogue among stakeholders on what was the right care and support for the refugee children in Sweden at the time. Bos and Abma (2018) used care ethics to critically reflect on the relationality of the evaluation practice itself. Caring evaluation in this context meant challenging dominant values like deliberation, rationality and control in order to include people without language. Both case examples showed that integrating a democratic caring commitment in evaluation entails more responsibility for vulnerable individuals and groups. If good and accountable care is conceived as situated in concrete situations for concrete people, evaluation will pay attention to local conditions and the plurality of caring values, voices and capacities of those involved. Yet, there may be other ways to bridge the disciplines of care ethics and evaluation, and these need to be explored in the coming years.
Conclusion
We have presented care ethics and caring as a normative orientation and new way of thinking about the normativity of the evaluation practice. We have demonstrated that the care ethics in Tronto’s theory of democratic caring in particular offers us a new orientation, one in which relationships, morality, and care are central. More importantly, care ethics can inspire us to develop a new professional ethos; an ethos in which we relate and attend in a caring way to people and practices in the light of a caring society. We believe this is a healthy resistance to a society that values self over relationships, individual success over the common good, mind over body, and thinking over feeling (Way et al., 2018). A caring society builds on people’s deeply felt need to care, to relate, and to connect within and across communities, human and nonhuman (Whyte and Cuomo, 2017). Caring evaluation, as we have shown, is not confined to private troubles, but builds on the personal woes of people to address the larger political, public issues of our times through the interrogation of un-caring practices. Adopting an ethics of care in evaluation inspires us to imagine and build a caring and sustainable world, one that acknowledges the humanist values of interdependency, reciprocity, and solidarity.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.