
Abstract
A central goal of physical education (PE) is to empower students to be physically active in a health-enhancing way. Therefore, using a competence-based approach, the objective of the health- and fitness-related PE intervention ‘Promotion of physical activity-related health competence in PE’ (GEKOS) was to address practical and theoretical content regarding training, fitness, and health. The aim of this person-oriented study was to examine differential effects of the GEKOS intervention on control competence and related knowledge, skills, abilities, and motivation. A total of 860 ninth graders were randomly assigned to an intervention or control group. Intervention group students received six PE lessons that combined practical and theoretical content regarding training, fitness, and health. Measurements were taken before, directly after, and with a follow-up after 8–12 weeks. Students completed a knowledge test and a fitness test, and filled out scales considering motivation and perceived control competence. Latent profile analysis and multinomial logistic regression were estimated. Five patterns of outcome measures were found. Intervention group students transitioned significantly more often to patterns with improved outcome values. The intervention was especially effective for a subgroup of students who initially had rather low outcome values. For a small proportion of students, the intervention entailed a loss of health-related motivation. The study indicated that students with low control competence and related knowledge, skills, abilities, and motivation can benefit from the GEKOS intervention. Future studies should investigate modes of actions and interventions that explicitly address motivation and vary the content and methods used in PE.
Introduction
Background
Physical activity (PA) has numerous effects on adolescents’ health (Poitras et al., 2016). As PA behavior develops in adolescence and often continues into adulthood (Telama et al., 2014), promotion of health-enhancing PA of adolescents is crucial. For this purpose, physical education (PE) is considered to be an ideal setting, as all young people, especially less physically active students, can be reached (Kriemler et al., 2011). In this context, a central goal of PE in many countries is to promote knowledge, skills, abilities, and motivation to initiate and maintain a healthy, physically active lifestyle throughout the lifespan (Ptack and Tittlbach, 2018; Tremblay and Lloyd, 2010).
Reviews already show the effectiveness of school-based interventions to promote PA behavior and physical fitness (Demetriou and Höner, 2012; Dudley et al., 2011; Kriemler et al., 2011). In addition, interventions report consistently positive effects on movement skills and health-related fitness knowledge (HRFK) and diverse effects on psychological determinants of PA, such as attitudes and enjoyment (Demetriou and Höner, 2012; Demetriou et al., 2015; Dudley et al., 2011). However, there are shortcomings in existing studies. These include: (1) knowledge, skills, abilities, and motivation are rarely addressed together (Cairney et al., 2019; Demetriou and Höner, 2012), which is surprising, given that these elements are the aforementioned central goals of PE; (2) the practical significance and sustainability of learning effects achieved by theoretical elements in PE remain unclear (Demetriou et al., 2015); (3) most studies are not rated as high-quality methodological studies (Demetriou and Höner, 2012; Demetriou et al., 2015; Dudley et al., 2011); and (4) in general, interventions are predominantly examined for global effects (Lapka et al., 2011). Therefore, little is known about the differential effectiveness of health- and fitness-related interventions in PE.
Against this background, we investigate whether knowledge, skills, abilities, and motivation associated with competencies for a healthy, physically active lifestyle can be promoted by combining theoretical elements regarding training, fitness, and health with practical elements like running and jumping activities or small-sided ball games in PE. With this aim, we evaluate the differential effectiveness of a PE intervention by applying a person-oriented approach (Bergman and Magnusson, 1997) for the analysis of a cluster randomized controlled trial (CRCT) with two post-measurements covering up to 12 weeks after the intervention.
Theoretical underpinning
There are a number of approaches available for determining how competencies for a healthy, physically active lifestyle can be promoted. One of these is the model of PA-related health competence (PAHCO) (Sudeck and Pfeifer, 2016). In recent years, this model has gained interest as a basis for interventions in different settings of PA promotion (Carl et al., 2020). The PAHCO model is located at the interface of health literacy and physical literacy (Carl et al., 2020; Edwards et al., 2017; Sørensen et al., 2012). It contributes to closing the gap between the rare consideration of PA-related aspects in health literacy research and the subordinate role of health in initial physical literacy concepts (Edwards et al., 2017; Fleary et al., 2018). Based on a functional–pragmatic competence approach (Klieme et al., 2008), the PAHCO model distinguishes three sub-competencies: movement competence, self-regulation competence, and control competence. These interrelated sub-competencies each contribute to coping with the specific demands necessary for initiating and maintaining health-enhancing PA (Sudeck and Pfeifer, 2016).
In the current study, we focus particularly on control competence as the students’ ability to make health-related decisions regarding their PA and to be able to plan and carry out their own PA in a health-related manner. The importance of control competence for health-promoting PA lies in the fact that adolescents who are empowered to lead healthy, physically active lifestyles must be able to cope with the demands of structuring and pacing their own PA in a health-enhancing way (Carl et al., 2020; Haible et al., 2020). This control competence for physical training requires HRFK, certain body-related skills and abilities, and health-related motivation (Sudeck and Pfeifer, 2016). Thus, adolescents with high control competence would be able to apply HRFK in order to optimize health benefits and minimize health risks of their PA behavior. HRFK implies, for instance, knowledge about principles of exercise and health-related fitness as well as health benefits of PA (Volk et al., 2021b). In addition, adolescents would be able to perceive body signals and to use them to regulate the amount of physical strain they experience (Carl et al., 2020; Sudeck and Pfeifer, 2016). Motivational elements, such as health-related interests and attitudes, are conducive factors for adolescents engaging with topics regarding training, fitness, and health (Chen, 2015; Krapp, 2002). In accordance with the model's assumptions, control competence for physical training is linked to physical fitness, not simply to the amount of PA. This implies that, in addition to a general increase in the volume of PA, special attention must also be paid to how PA is carried out (Haible et al., 2020; Sudeck and Pfeifer, 2016).
Against this background, to promote control competence for physical training and related HRFK, body perception, health-related motivation, and physical fitness, neither a pure theory transfer nor mere physical training in PE is sufficient. It is rather a matter of combining theoretical and practical elements, that is, combining physical experience in training with cognitive learning (Carl et al., 2020; Schön, 2002). Thus, we developed the GEKOS intervention (abbreviation of the German title: Förderung bewegungsbezogener Gesundheitskompetenz im Sportunterricht (Promotion of PA-related health competence in PE); Haible et al., 2019; Volk et al., 2021a) as a health- and fitness-related PE program. This PE program combines theoretical and practical components through the concepts of learning tasks (Leisen, 2010) and reflective practice (Schön, 2002; Serwe-Pandrick, 2013). Learning tasks (Leisen, 2010) represent an important part of competence-oriented teaching (Pfitzner et al., 2012) and are comparable to constructivist learning approaches (e.g. Bybee et al., 2006; Ennis, 2015). Learning tasks are mainly characterized by cognitive activation (i.e. the student must actively think about the tasks’ solutions), student orientation (i.e. students are actively involved in the learning process), and social interaction (Pfitzner et al., 2012), among others. In detail, they consist of subtasks of a topic or problem (e.g. perception of acute physiological responses to PA) that build on each other and which the students have to solve consecutively. This can be accomplished through the principle of reflective practice (Schön, 2002; Serwe-Pandrick, 2013); for example, through reflection in action (i.e. specific assignment to perceive body signals during specific running activities or strength training) or reflection on action (i.e. reflecting on perceived body signals from previous activities). While solving these tasks, students and teachers discuss the physical experiences of the practical phases.
Person-oriented evaluation of the GEKOS intervention
To investigate differential intervention effects using a person-oriented approach, it is valuable to take a closer look at subgroups of students who may differ in their responses to PE interventions. For the GEKOS intervention, this was done as part of a CRCT that examined short- and mid-term effects on control competence for physical training, HRFK, cardiorespiratory and muscular fitness, and health-related interests and attitudes in ninth graders compared to regular PE classes (Haible et al., 2019). Effectiveness of interventions in CRCTs is usually evaluated on an aggregated global level using a variable-oriented approach, and this has already been done for the GEKOS intervention by Volk et al. (2021a). However, in addition to variable-oriented analyses and moderator analyses with a priori defined groups, such as gender, complementary analyses employing a person-oriented approach allow for identification of subgroups through empirical exploration (Lapka et al., 2011).
The person-oriented approach comprises theoretical and methodological assumptions, two of which are crucial for our study (e.g. Bergman and Magnusson, 1997). First, the person-oriented approach assumes that development is a complex process that is partly individual-specific. On this basis, the person-oriented approach identifies and describes subgroups of individuals who share similar patterns of values regarding variables of interest. In the present study, we investigate which prerequisites students have with regard to typical patterns of control competence for physical training, HRFK, physical fitness, and health-related motivation.
In this context, we can describe patterns of student characteristics according to the relative manifestation (e.g. low, medium, and high) of variable values as level or shape patterns (Morin and Marsh, 2015). In level patterns, values across all variables are aligned on the same level (e.g. low). In contrast, in shape patterns, values of the different variables are not aligned, and instead are on different levels (Clark et al., 2020; Morin and Marsh, 2015). For instance, students within a shape pattern could be physically fit on average, but with low HRFK, perceived control competence for physical training, and health-related motivation.
Second, the person-oriented approach assumes that various factors of an individual do not develop independently of each other, but rather in a complex reciprocal interplay. For a competence-oriented intervention that combines practical and theoretical elements of training, fitness, and health, this would ideally mean that several outcome variables may change together, and thus different transitions in patterns may be observed in the subgroups. For instance, students characterized by a low-level pattern may transition to a medium-level pattern when they improve across all variables. If they only improve in particular variables, such as physical fitness, they may transition to a shape pattern that shows low HRFK, perceived control competence for physical training and health-related motivation, and medium or high physical fitness. There are also likely to be students who remain in the same pattern, since intervention-related changes in outcomes may not always be sufficient for a transition. Knowing this allows us to identify individual-specific change patterns across outcome variables and thus analyze differential effects in specific subgroups.
The present study
The purpose of this person-oriented study is to build upon the already published results of the variable-oriented evaluations of the GEKOS intervention (Volk et al., 2021a), which referred to intervention effects based on statistical group means and which examined differential effects merely on the basis of moderator analyses applying gender as a predefined moderator of intervention effects.
Therefore, based on a person-oriented perspective, we aim to examine the differential effects of the health- and fitness-related GEKOS intervention in PE on its targeted range of outcomes; namely control competence for physical training, HRFK, cardiorespiratory and muscular fitness (physical fitness), and health-related interests and attitudes (health-related motivation) in ninth graders. This allows us to investigate which outcome variables change together on a person-specific level, and thereby generate insights into intervention-induced transitions in patterns typical for different subgroups. While the variable-oriented evaluation examined both forms of the GEKOS intervention separately, we, in contrast, consider one comprehensive intervention group for the person-oriented evaluation, encompassing the common features of the intervention content and teaching methods. This enables us to apply adequate person-oriented evaluation strategies, which subsequently allow for meaningful findings in comparison to the control group of regular PE.
The study aim is achieved by empirically identifying patterns that reflect the students’ prerequisites for the six outcome variables by using latent profile analyses and investigating students’ transitions in patterns over time (short- and mid-term), depending on their group assignment (intervention vs. control group). In terms of intervention goals, we expect that students in the intervention group transition more often to patterns with relatively higher values regarding the six outcome variables compared to the control group students.
Methods
Design and procedure
The CRCT was conducted with ninth-grade students to examine the effects of the GEKOS intervention program (Haible et al., 2019). Overall, 48 gender-segregated PE classes in secondary schools took part. 1 The 24 female and 24 male PE classes and their PE teachers were recruited by the heads of the regional school boards of Baden-Württemberg, who informed schools about the study via mail. Interested PE teachers and their students were given detailed information about the study and given instructions on how to indicate their interest in participating. The classes were then assigned randomly to either the intervention (cgirls = 14, cboys = 13) or wait-list control (cgirls = 10; cboys = 11) condition in the run-up to the three study waves (first semester 2017–2018, second semester 2018 and first semester 2018–2019). The main investigators informed participating PE teachers as soon as the allocation process was completed. Students were tested before the intervention (T1), after the intervention of six PE classes (T2), and 8–12 weeks after the intervention (T3). At each measurement point, students completed a paper-and-pencil questionnaire (90 min) in the classroom and a physical fitness test (90 min) in the gym. Trained research assistants, who were not informed about the group assignment, collected data using a standardized manual. The research assistants were present throughout the entirety of the tests; afterwards, they collected the questionnaire booklets and rated the results of the physical fitness tests on test protocols. They also transferred the data into a secured electronic database and double-checked the information.
We received approval from the Ethics Committee for Psychological Research at the University of Tübingen. Written informed consent was given by students, parents, and teachers. Descriptions of the study design, sample recruitment, sample size calculation, randomization process, and data management are also provided in the published study protocol (Haible et al., 2019).
Participants
In total, 860 ninth graders from both urban and rural areas took part in the study. After baseline assessment of the 48 PE classes, one intervention class (n = 19, female) was unable to continue taking part in the study due to their teacher taking sick leave. Of the final sample of 841 students (Mage = 14.20, SD = 0.51), 472 students (53.8% girls) were in the intervention group and 369 students (47.7% girls) were in the control group.
The loss of the randomized sample (overall attrition) was at 3.0% at T1, 7.8% at T2, and 13.2% at T3 for the paper-and-pencil test and at 7.0% at T1, 17.0% at T2, and 29.0% at T3 for the physical fitness test. The difference in attrition between the intervention and control group students was between 1.2% (paper-and-pencil test, T1) and 6.4% (physical fitness test, T3). In consideration of the What Works Clearinghouse standards (WWC, 2020), the combination of overall and differential attrition could be regarded as low and the degree of expected bias tolerable. For the physical fitness test at T3 alone the comparison of overall and differential attrition did not meet the WWC (2020) standards.
Intervention
The special feature of the GEKOS intervention is the combination of its methodical approach to address knowledge, skills, abilities, and motivation, and its content focus on health and fitness. This is based on a strong emphasis on cognitive and reflective competencies, as well as the importance of topics related to health and fitness in recent German PE curricula (e.g. Ministerium für Kultus Jugend und Sport Baden-Württemberg, 2016).
Teachers in the intervention condition taught six PE lessons (each 90 min) combining theoretical content on health and fitness with either running and jumping activities or small-sided ball games. The lessons emphasized health and fitness, both theoretically and practically, using the two main topics of perception of physical load and control of physical load and physical training. The individual lessons focused on content that included: (1) perception of physiological responses to PA, (2) perception and measurement of heart rate, (3) perception and measurement of perceived exertion, (4/5) health-related fitness: strength training and cardiovascular endurance, and (6) application of skills and knowledge.
Each of lessons 1−5 contained a learning task (Leisen, 2010) that included five consecutive subtasks: after the teacher presented the topic (e.g. perception of physiological responses to PA), (a) the students were first asked to express their ideas and assumptions about the topic based on their prior knowledge (e.g. assumptions about changes in the body during PA); (b) then, to gain information about the topic, students were instructed to perform specific PA (e.g. running activities or 3 vs. 3 soccer games) and reflect (e.g. individual physiological responses to PA) either in or on action (Pfitzner et al., 2012; Schön, 2002; Serwe-Pandrick, 2013); (c) subsequently, the learning experiences were discussed with other students and the teacher and then (d) related to the previous assumptions from the beginning; and (e) in subsequent lessons, students were encouraged to apply and practice this newfound experience and knowledge. In lesson 6, students applied their new knowledge and skills by selecting, planning, and instructing a game/drill with adequate intensity and time to affect cardiovascular endurance. Detailed content of the five learning tasks in each lesson can also be found in the study protocol (Haible et al., 2019).
Teachers in the control condition taught six PE lessons focusing either on running and jumping activities or on small-sided ball games. Despite the emphasis on cognitive and reflective competencies in the German PE curricula, in regular PE practice, a focus on learning sport-specific skills is still pronounced (Pühse et al., 2011). Therefore, they were not given any further instructions on the methodological or content-related orientation of their lessons.
Before the start of the intervention phase, all teachers in the intervention group received training on the methods and content related to the GEKOS intervention. They also received a detailed treatment manual with the exact description of the lessons and all materials needed. To ensure treatment validity, the following measures were taken: (1) After each lesson, intervention and control group teachers completed a self-report form that described whether they were able to conduct lessons as planned. (2) After each lesson, intervention group teachers sent a photograph of the poster with the main results of the lesson. (3) Each intervention class was visited and observed once by the main researchers (Haible et al., 2019).
Measures
Control competence for physical training was measured at T1, T2, and T3 using six Likert-scale items (e.g. ‘I can use my body signals (pulse, breathing speed) very well to gauge and regulate the amount of physical load’) which have been validated for adolescents (Haible et al., 2020). The Likert scale ranged from totally disagree (1) to totally agree (5). The internal consistency of the scale was good (T1: α = 0.79; T2: α = 0.82; T3: α = 0.79).
HRFK was assessed at T1, T2, and T3 by the same performance test (Volk et al., 2021b). The test addressed knowledge of the principles of exercise and physical fitness, knowledge about risk reduction, the prevention of injuries related to PA and exercise, and knowledge about the health benefits of PA. The performance test contained 27 complex multiple choice, matching and sorting items, as well as open-ended questions, which were coded by trained researchers. We estimated the HRFK score using the unidimensional generalized partial credit item response theory model (Muraki, 1992) with weighted maximum likelihood estimates (WLEs; Warm, 1989). The HRFK test achieved satisfactory psychometric properties for group comparison, as defined in previous studies (WLE reliability = 0.65; rtt = 0.70, time interval: M = 11 weeks; Volk et al., 2021b).
Cardiorespiratory fitness was measured at T1, T2, and T3 through a 20 m shuttle run (Léger et al., 1988). The protocol started at 8.0 km/h, increasing to 9.0 km/h after a minute and afterwards by 0.5 km/h every minute. Results were reported at the running speed (km/h) at the last completed stage, and scores were standardized using age- and sex-specific values (Tomkinson et al., 2017).
Muscular fitness was assessed at T1, T2, and T3 by measuring three strength and strength endurance exercises (standing long jump, push-ups (40 s), and sit-ups (40 s)). The students had two attempts each, of which the better one was scored. The three tests are part of a standardized German physical fitness test (Deutscher Motorik-Test (DMT) 6–18; Woll et al., 2011). Results were standardized by age and sex, using national reference data, and were combined into a muscular fitness score. The internal consistency of the score was reasonable (T1: α = 0.62; T2: α = 0.65; T3: α = 0.68).
Interest in training, physical fitness, and health was assessed at T1, T2, and T3 by four items (e.g. ‘I’m interested in learning about fitness, and health’; Haible et al., 2019), which were developed based upon the PISA 2006 Technical Report (OECD, 2009). The response format was a 5-point scale ranging from 1 (‘totally disagree’) to 5 (‘totally agree’). The internal consistency of the score was rated as good (T1: α = 0.79; T2: α = 0.84; T3: α = 0.85).
Attitudes toward the health effect of PA were measured at T1, T2, and T3 by four affective items (e.g. ‘I feel better and healthy after being physically active’) and three cognitive items (e.g. ‘regular exercise is healthy’; Steinmann, 2004). For this analysis, we combined all seven items into a total score, which has been done in previous studies with adolescents (Demetriou, 2013). The response format was again a 5-point scale ranging from 1 (‘totally disagree’) to 5 (‘totally agree’). The internal consistency of the score was satisfactory to good (T1: α = 0.75; T2: α = 0.76; T3: α = 0.77).
Statistical analyses
For the person-oriented evaluation, we excluded 14 students (n = 8, control group) after conducting multivariate outlier analyses (Mahalanobis distance as χ2 at p < 0.001; Tabachnick and Fidell, 2014). Therefore, the analyses presented in this paper were based on a final sample of 827 adolescents (intervention group: n = 466 (53.6% girls); control group: n = 361 (47.9% girls)).
Over all three time points and with respect to the six outcome variables, 12.1% (T1: 5.7%; T2: 11.7%; T3: 19.6%) of the data was missing. Several students’ profiles contained missing data on all variables at one time point (T1: n = 12; T2: n = 31; T3: n = 86). We replaced the missing data in advance of the latent profile analysis (LPA) in SPSS with the expectation-maximization (EM) algorithm. 2
Descriptive statistics (mean, standard deviation, skewness, and kurtosis) and correlations of all six outcome variables are provided in Appendix A, Tables S1A and S2A.
The evaluation of the main question was done in three steps. In the first step, we grouped students into patterns using an LPA. We conducted the LPAs based on the six main outcome variables separately for each time point (T1, T2, and T3). We used the following statistical indicators to select the optimal number of patterns: the Akaike information criterion (AIC), the Bayesian information criteria (BIC), and the sample size-adjusted BIC (aBIC). A lower value supports a better model fit. The criteria were used to compare the relative fit of models with different numbers of latent profiles. We also referred to the elbow criteria of the illustrated BIC values. Furthermore, we used the bootstrapped likelihood-ratio test (BLRT), which compares a k-pattern model with a k − 1 pattern model. Also, entropy (absolute model fit) indicates the precision with which the cases are classified into patterns. A value close to 1 indicates fewer classification errors (Masyn, 2013; Morin and Wang, 2016). An indication for reliable pattern classification is the average latent class probability, which is supposed to be >0.80 (Morin and Wang, 2016). Additionally, we also used content-related indicators, such as the principle of parsimony and the interpretability of the identified patterns, to decide on the optimal number of patterns (Masyn, 2013; Morin and Wang, 2016).
In the second step, we checked the stability of the five patterns over time and between groups by assessing measurement invariance. Here, we compared the configural and similarity models by reviewing χ2 difference tests using the maximum likelihood estimator (MLR) with the Satorra–Bentler scaling correction. Non-significance indicates measurement invariance and, therefore, similarity between the models. Furthermore, BIC, aBIC, and AIC were compared (Morin et al., 2016; Morin and Wang, 2016).
In the third step, we looked at transitions between patterns over time. 3 Prior to this, we checked the baseline equivalence of group allocation in patterns. In a main analysis, we compared transitions between control and intervention groups using multinomial logistic regression, weighting cases by treatment allocation in each subgroup at T1 (dependent variable with three categories: positive, no, and negative transition; predictor: treatment allocation). We also looked at pattern changes within intervention and control groups using a Wilcoxon signed-rank test. To further investigate pattern-specific transitions, we compared in post-hoc analyses affiliations with patterns of intervention and control group students at T2 and T3 by performing a separate Fisher’s exact test for each pattern at T1.
For main statistical analyses (steps 1–3), we used Mplus Version 8.4 using maximum likelihood estimation with robust standard errors (MLR; Muthén and Muthén, 1998–2017) considering the special features of nested data (in Mplus: type = complex). For the Wilcoxon signed-rank test and post-hoc analyses, we used SPSS Version 26 (IBM, New York, NY, USA).
Results
Identifying patterns
Two to seven latent-pattern solutions were tested and reported separately for T1, T2, and T3 (Table 1). In general, aBIC and AIC constantly declined when patterns were added. However, BIC and the elbow criterion supported a five-pattern solution. The BLRTs were significant throughout, which means that each model fits the data better than the model with one less pattern. Entropy values of all pattern solutions were consistently around the recommended value of 0.70. Yet, pattern sizes supported the five-pattern solution, and the average latent class probabilities were close to 0.80 or higher, except for pattern 3 (latent class probability: T1 = 0.73; T2 = 0.70; T3 = 0.75). The content-related inspection of the patterns also endorsed the five-pattern solution for T1, T2, and T3, as these patterns were theoretically interpretable and parsimonious.
Latent patterns of outcome variables: Models for two- to seven-pattern solutions.
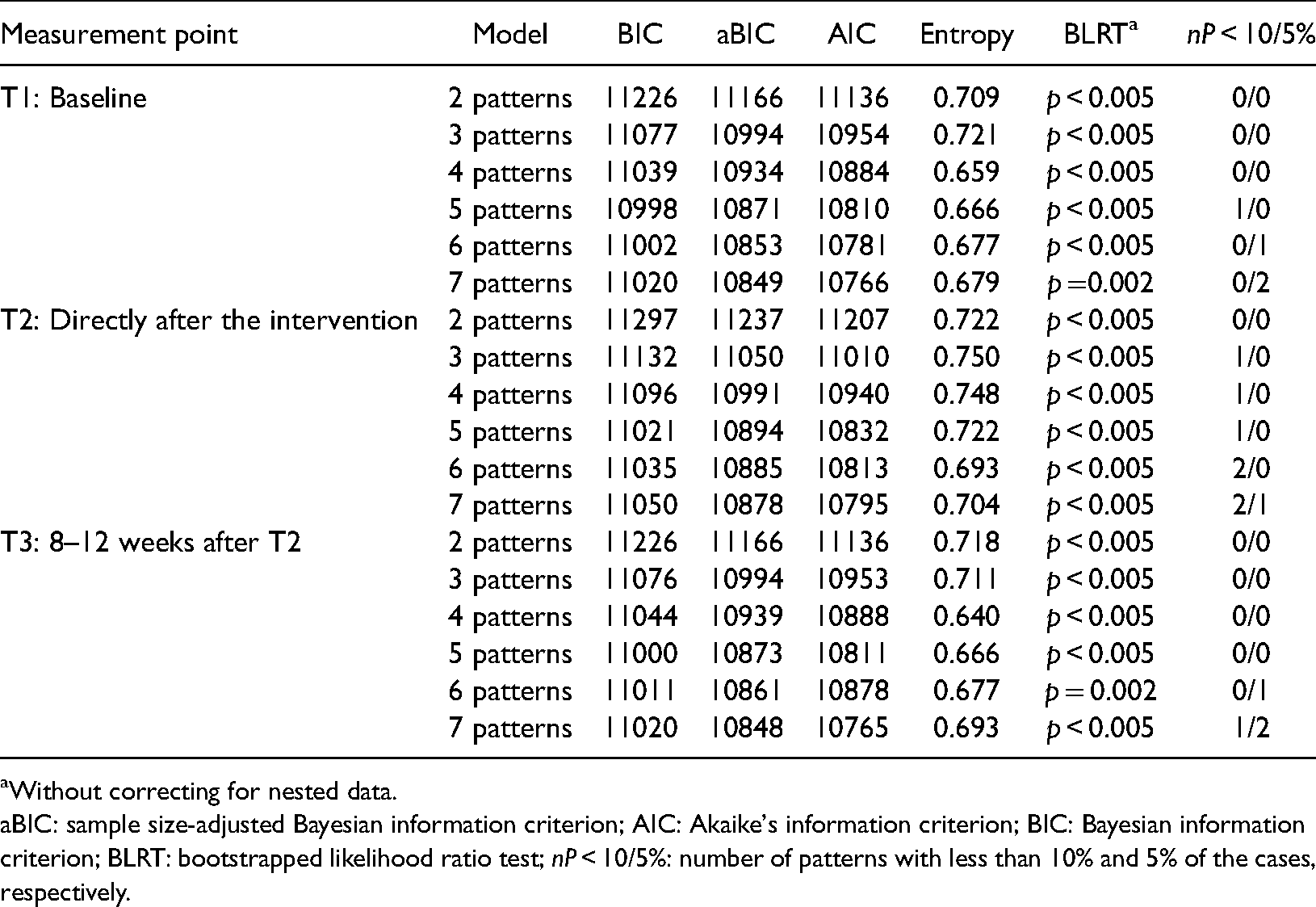
Without correcting for nested data.
aBIC: sample size-adjusted Bayesian information criterion; AIC: Akaike's information criterion; BIC: Bayesian information criterion; BLRT: bootstrapped likelihood ratio test; nP < 10/5%: number of patterns with less than 10% and 5% of the cases, respectively.
Describing identified patterns
The five patterns, which are characterized by six indicators, are illustrated in Appendix A, Table S3A for all three time points and for T1 in Figure 1. Table 2 shows the categorizations of the indicators for T1 based on their relative values in low, medium, and high. Pattern 1 (shape: very low to medium) was characterized by generally low to very low values, except for HRFK (medium). Pattern 2 (shape: low to medium) demonstrated low values in HRFK and physical fitness and medium values in control competence for physical training and health-related motivation. Pattern 3 (level: medium) was marked by medium values throughout. Pattern 4 (shape: medium to high) was characterized by medium values in HRFK and physical fitness and high values in control competence for physical training and health-related motivation. Pattern 5 (level: high) was characterized by the highest values across all variables.
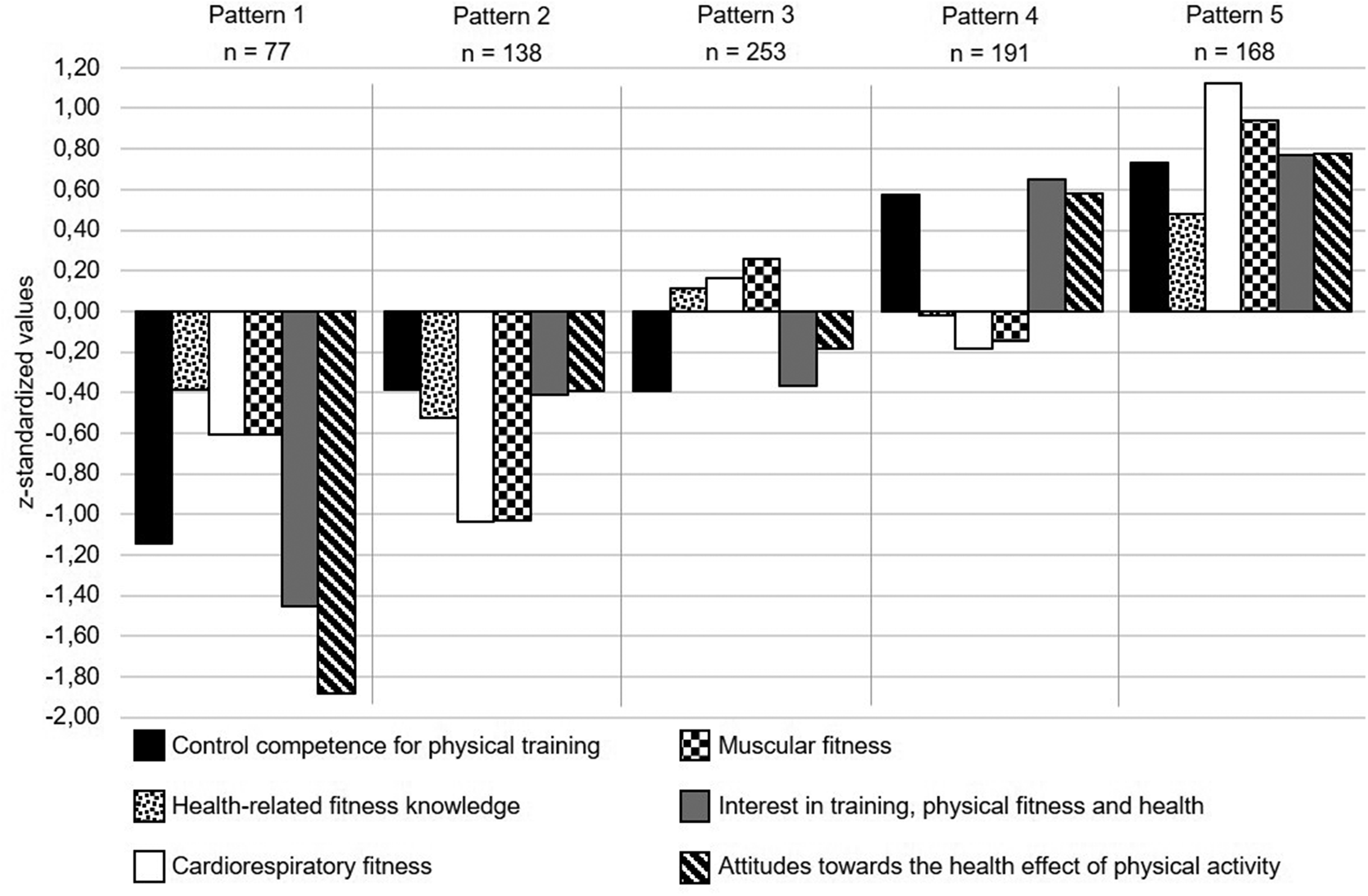
Z-standardized patterns 1–5 for the first (T1) measurement point (n = 827).
Categorized relative values of the six indicators in the identified five patterns at T1.
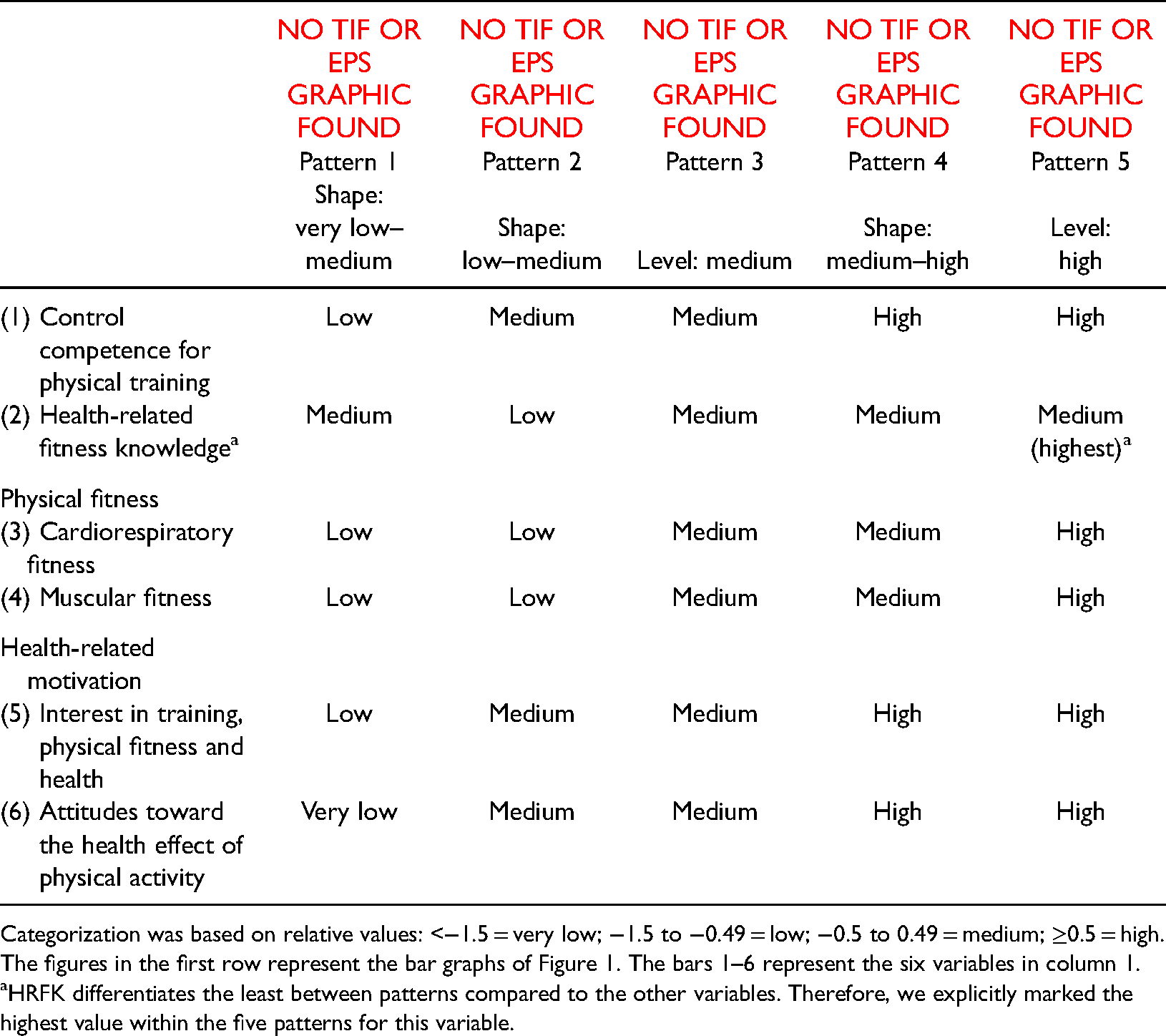




Categorization was based on relative values: <−1.5 = very low; −1.5 to −0.49 = low; −0.5 to 0.49 = medium; ≥0.5 = high. The figures in the first row represent the bar graphs of Figure 1. The bars 1–6 represent the six variables in column 1.
HRFK differentiates the least between patterns compared to the other variables. Therefore, we explicitly marked the highest value within the five patterns for this variable.
Examining the five-pattern solution over time and between groups
The measurement invariance test over time showed that the five-pattern solution is similar across all three time points. The measurement invariance test between groups showed that the five-pattern solution was also similar across the intervention and control group samples. Detailed results can be found in Appendix A, Tables S4A, S5A and Figure S1A.
Examining pattern transitions over time
We categorized pattern transitions of students from T1 to T2 or T1 to T3 into positive, no, and negative transitions. Transitions to patterns with higher values across all or in certain variables, such as from pattern 1 (shape: very low to medium) to pattern 3 (level: medium), are considered to be positive. Conversely, transitions to patterns with lower values, such as from pattern 5 (level: high) to pattern 4 (shape: medium to high), were categorized as negative. Students who remained in their pattern were classified as having no transition.
Based on this, we compared the transitions of intervention and control group students from T1 to T2 and T1 to T3 (Table 3). Because we found a significantly higher number of intervention group students compared to control group students in pattern 1 (shape: very low to medium) at T1 (z0.95 = 3.49; p < 0.001), we performed the main analyses weighting by treatment allocation. No other significant differences were found, either in the other patterns or at the other time points.
Description of pattern transitions (positive, negative, and no transition) from T1 to T2 and from T1 to T3, as well as comparisons of intervention and control group students’ positive transitions from T1 to T2 and T1 to T3 to no and negative transitions using multinomial logistical regression models.
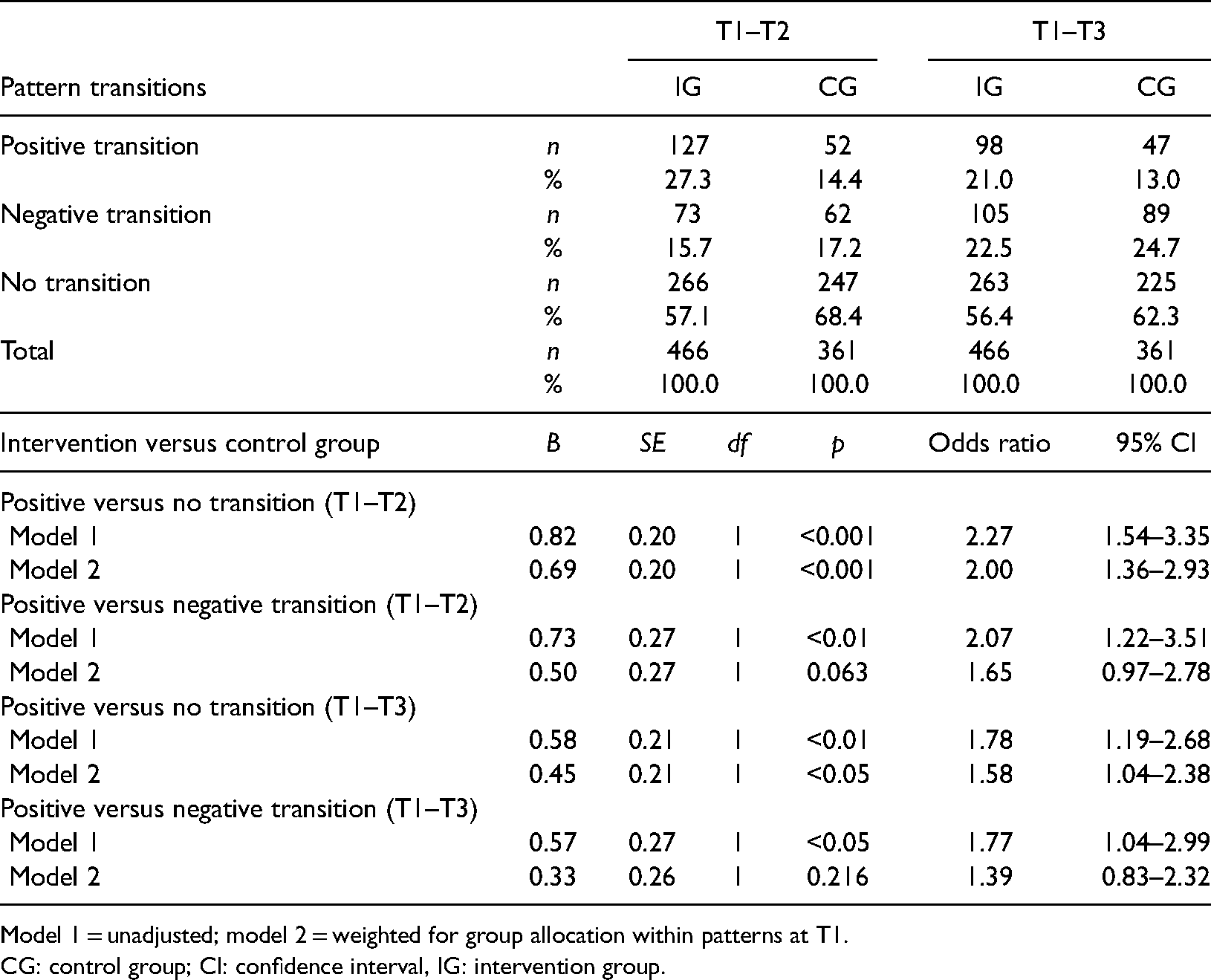
Model 1 = unadjusted; model 2 = weighted for group allocation within patterns at T1.
CG: control group; CI: confidence interval, IG: intervention group.
Differences in pattern transitions between intervention and control group from T1 to T2
From T1 to T2, compared to students in the control group, the students in the intervention group transitioned significantly more often positively than not (odds ratio (OR) = 2.00, confidence interval (CI95%) = 1.36–2.93; Table 3). However, there were no differences between positive and negative transitions (OR = 1.65, CI95% = 0.97–2.78).
Within-group analyses in the intervention group were significantly in favor of positive transitions (Z = −3.68, p < 0.001), while there was no significant difference between positive and negative transitions within the control group (Z = −1.03, p = 0.302).
Based on pattern affiliation at T1, Fisher’s exact tests compared pattern affiliation at T2 between the intervention and control groups (Appendix A, Table S6A). These post-hoc analyses showed a significant difference between pattern transitions of intervention and control group students of pattern 2 (shape: low to medium; p < 0.001) and pattern 5 (level: high; p = 0.049). No significant differences were found for students of patterns 1, 3, or 4. The pattern-specific transitions are shown in Table 4. The rows indicate the pattern allocation at T1, whereas the columns indicate pattern allocation at T2 (upper table) and T3 (lower table). The values in the diagonal represent the number of students with no pattern transition. Above the diagonal, positive transitions are displayed, whereas negative transitions are reflected below the diagonal. For instance, intervention group students, compared to control group students, of pattern 2 at T1 (shape: low to medium) transitioned significantly more often positively; for example to pattern 3 (level: medium; 36% vs. 14%) and pattern 4 (shape: medium high; 16% vs. 5%) at T2. Intervention group students, compared to control group students, of pattern 5 at T1 (level: high) transitioned significantly more often negatively; for example to pattern 4 at T2 (shape: medium to high; 16% vs. 7%).
Cross tables for pattern affiliation T1 and either T2 (upper cross tables) or T3 (lower cross tables) separated for intervention and control group students.
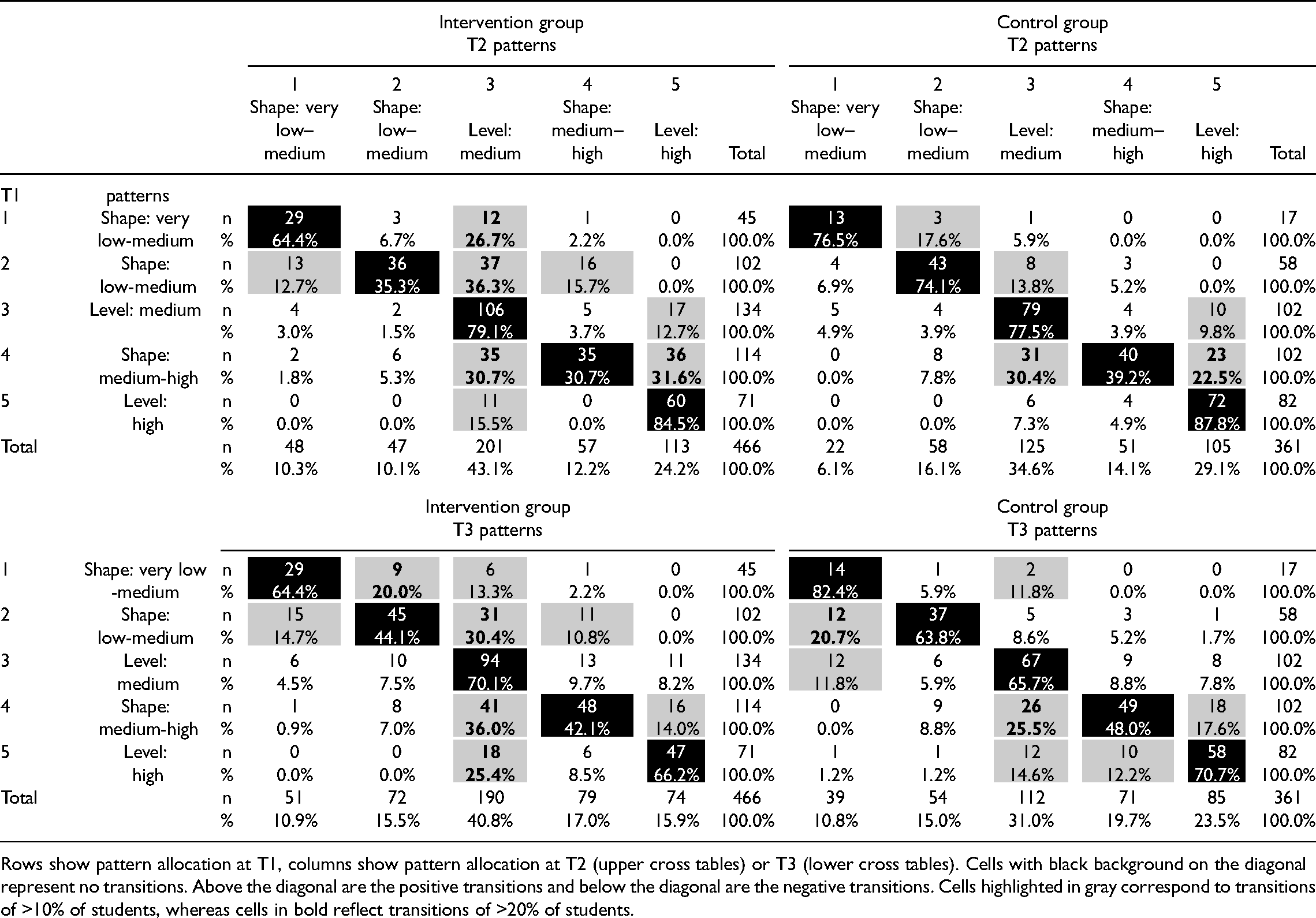
Rows show pattern allocation at T1, columns show pattern allocation at T2 (upper cross tables) or T3 (lower cross tables). Cells with black background on the diagonal represent no transitions. Above the diagonal are the positive transitions and below the diagonal are the negative transitions. Cells highlighted in gray correspond to transitions of >10% of students, whereas cells in bold reflect transitions of >20% of students.
Differences in pattern transitions between intervention and control group from T1 to T3
From T1 to T3, compared to the control group, the intervention group students transitioned significantly more often positively (OR = 1.58, CI95% = 1.04–2.38; Table 3) than not, but there were no differences between positive and negative transitions (OR = 1.39, CI95% = 0.83–2.32). Within the intervention group, positive and negative transitions were equally evident, so the Wilcoxon signed-rank test is not significant (Z = −0.56; p = 0.574). Within the control group, statistically significant transitions were shown in favor of negative transitions (Z = −3.69, p = < 0.001). This is in line with the results shown by the multinomial logistic regression (Table 3) that more positive transitions remain in the intervention than in the control group. Post-hoc analyses (Appendix A, Table S6A) showed that, based on pattern affiliation at T1, intervention group students compared to control group students of pattern 2 (shape: low to medium) transitioned significantly (p < 0.001) more often positively, for example, to pattern 3 (level: medium; 30% vs. 9%; Table 4) or pattern 4 (shape: medium to high; 11% vs. 5%). No significant differences were found for students of patterns 1, 3, 4, or 5.
Discussion
Using a person-oriented approach, we tested the short- and mid-term effects of the health- and fitness-related GEKOS intervention on control competence for physical training, HRFK, physical fitness, and health-related motivation of ninth graders in PE within a CRCT. The GEKOS intervention combined theoretical content on health and fitness with practical elements like running and jumping activities or small-sided ball games. The specificity of this approach is that one can investigate which outcome variables were jointly affected by the PE intervention and whether this led to intervention-related transitions in empirically identified subgroups with unique patterns of variables. Further, we explored whether intervention-related pattern transitions occurred in specific subgroups. This contributes to developing a better understanding of the differential effectiveness of the GEKOS intervention.
Short- and mid-term intervention-related transitions in patterns
Regardless of treatment condition or time point, in total, stability was more common than transitions. Since students’ properties had been developed over several years and because transitions require several substantial changes in outcome variables, transitions did not appear as often in the context of an intervention consisting of six PE lessons.
Nevertheless, overall, we found statistically significant differences in pattern transitions between the intervention and control group students. In the short-term, compared to the control group, the intervention group students transitioned 2.0 times more often positively than not. At the mid-term, the intervention effects partially remained and only slightly diminished. Specifically, compared to the control group, students in the intervention group transitioned around 1.6 times more often positively than not. Additionally, while at the mid-term, within the intervention group both positive and negative transitions occurred with similar frequency, the control group showed significantly more frequent negative transitions.
The positive short- and mid-term results are particularly evident in the transitions shown by intervention group students of pattern 2 (shape: low to medium). These students were the least physically fit and had the lowest HRFK compared to students in other patterns. Their control competence for physical training and health-related motivation was at a similar level to those of pattern 3 (level: medium). In the short-term and mid-term, intervention group students of pattern 2 showed two main improvement pathways. First, a majority of pattern 2 intervention group students improved their physical fitness and their HRFK, and also slightly improved their perceived control competence for physical training; they transitioned to pattern 3 (level: medium). Second, over the short term, some students of pattern 2 in the intervention group were positively affected across all outcome variables. They transitioned to pattern 4 (shape: medium to high). This effect across all outcome variables was also observed in about a third of the students in pattern 1 (shape: very low to medium; Table 4) in the intervention group, who transitioned to pattern 3 (level: medium).
In the context of this study, we did not causally investigate the extent to which a certain mode of actions was a possible reason for why students in these patterns in particular were affected by the intervention. Therefore, we can only offer initial assumptions that refer to both the teaching method (learning tasks and reflective practice) and the content (health and fitness).
Students in patterns 1 (shape: very low to medium) and 2 (shape: low to medium), who tend to be characterized by lower values in terms of health- and fitness-related knowledge, skills, abilities, and motivation, seem to respond positively to this type of PE class. One reason for this could be that, methodologically, the type of instruction, which involves learning tasks and reflective practice, could open up the possibility for them to get more involved than in regular PE classes, which are often focused on physical aspects and athletic performance (Pühse et al., 2011). In terms of content, theoretical and practical exposure to physical responses to PA allowed them to learn that they are able to affect their own physical fitness (Fisher et al., 2006). Both aspects may have provided experiences of competence (Chen, 2015; Fisher et al., 2006).
However, compared to these positive improvement pathways, there were also students, especially in pattern 5 (level: high), whose values deteriorated in relation to the outcome variables. Although short-term statistical differences between pattern 5 intervention and control group students did not persist at the mid-term, there were considerable observations regarding negative transitions at both time points. Negative transitions of intervention group students were especially interesting in comparison to decline in control group students. While negative transitions in control group students to pattern 4 (shape: medium to high) were predominantly characterized by changes in HRFK and physical fitness, intervention group students decreased across all outcome variables, but especially in control competence for physical training and health-related motivation and transitioned to pattern 3 (level: medium).
Regarding students in pattern 5 (level: high), who tend to be characterized by the highest values in terms of health- and fitness-related knowledge, skills, abilities, and motivation, we assume that they are probably among the students with good PE grades. As PE students might be more used to lessons that emphasize physical aspects and athletic performance, these students may be less motivated by the increased focus on theoretical content (Kastrup, 2011), especially with reference to health. This could explain the differences between the transitions of the intervention and control group students. In general, we are less likely to assume that students actually deteriorated in terms of physical fitness and knowledge over the short period; therefore, we suppose that in both groups, this deterioration is motivational due to repeated measurement. Thus, the specific difference is that, especially for the intervention group, students’ health-related motivation and perceived control competence for physical training decreased, which could be related to altered health-related content and methods.
This may indicate a special role of health-related motivation, especially in relation to perceived competence. As described above, some students of pattern 1 (shape: very low to medium) and pattern 2 (shape: low to medium) improved not only in HRFK, physical fitness, and perceived control competence for physical training but also in health-related motivation. Following assumptions and investigations from learning psychology (e.g. Zhang et al., 2016), teaching and acquiring knowledge could have led to increased interest and thus higher health-related motivation in these students. These students also significantly increased their control competence for physical training, which reveals that a parallel change in HRFK and health-related motivation may promote competence-based integration processes of knowledge, skills, abilities, and motivation (Baartman and De Bruijn, 2011).
These results underline the added value of complementary evaluation with the person-oriented approach. While the variable-oriented analyses of the GEKOS intervention in both types of PA showed a zero effect on motivation (Volk et al., 2021a), this study has shown that motivation can have both a positive and negative influence on competence acquisition. This would also indicate reasons for why motivationally inconsistent findings are often observed in PE (e.g. Kelso et al., 2020). According to our results, we conclude that future health- and fitness-related interventions must address motivational aspects more explicitly, as has also been proposed by Chen (2015). On the one hand, this could reinforce positive effects in the competence-oriented interplay of knowledge, skills, abilities, and motivation. On the other hand, it might also reduce the negative effects experienced by specific groups of students.
Strength and limitations
This study investigated with a person-oriented approach a competence-based PE program, linking theoretical and practical content of training, fitness, and health using a CRCT design. The implementation of the program was standardized and various actions to ensure treatment validity have been realized (Haible et al., 2019). For the present analyses, however, there is the limitation that no rating of the actual quality of intervention fidelity was included. The large sample size allowed us to analyze the effectiveness of the intervention in distinct subgroups while controlling for clustering. The follow-up showed sustainable results that only diminished slightly. This enables us to identify individual pattern transitions regarding competence-based knowledge, skills, abilities, and motivation and, to some extent, describe different ways of competence acquisition.
The identified patterns proved to be structurally stable over the three measurement points and between groups, meaning that they were similar over time and between groups. Despite the overall stability of the patterns, pattern 4 (shape: medium to high) showed some instability over time. Some aspects might have affected pattern allocation including that we used a subjective measure of competence. It would be desirable to go beyond subjective measures in the future. Regarding the results of the HRFK test, repeated measurement may have led to higher test scores in the follow-up measurement, but also to lower test scores, due to loss of motivation. These possible biases apply to both study conditions; however, the study design enabled controlling for these biases by the repeated use of the same HRFK test.
Further, the muscular fitness score showed only reasonable internal consistency, which might have increased errors in pattern allocation and limited the detection of intervention effects. This inconsistency could also be due to the recording procedure of the fitness tests. As we could not guarantee repeated measurement by the same research assistants, interpersonal differences may have occurred. Nevertheless, within the patterns, muscular and cardiorespiratory fitness were constantly on a similar level, which indicates positive measuring properties of the muscular fitness score. Furthermore, the impact of using EM estimation on allocation and transition is not known. However, we could provide a sound sensitivity analysis using a full information maximum likelihood (FIML) procedure.
Unfortunately, we could not use the sound subgroup identification for transition analyses, which would have been available when applying latent transition analyses. Therefore, we could not benefit from latent transition probabilities and had to accept a possible higher impact of measurement errors for pattern transitions on a manifest level. Although we were able to include a large overall sample in the intervention study, the statistical power for the pattern-specific analyses was rather low. This limits the statistical validation of intervention-related pattern transitions. Furthermore, within the longitudinal design, the regression to the mean phenomenon may have contributed to both positive and negative pattern transitions. Although this phenomenon affects both groups, the baseline differences were initially in favor of the hypotheses. However, by weighting cases by treatment allocation, the effects remained largely constant.
Finally, the generalizability of our effects can only be assumed for ninth graders in German gender-segregated PE classes. Future studies should address the generalizability in other age groups and/or for students in different education systems.
Conclusion
In conclusion, our results demonstrated differential effects of the health- and fitness-related GEKOS intervention in PE on control competence for physical training, HRFK, physical fitness, and health-related motivation of ninth graders. In doing so, we took into account that students experience the intervention differently. We were also able to identify students who benefited from the intervention, as well as some students who were negatively impacted by the intervention. This highlights the heterogeneity of students, suggesting that it is worth looking at subgroups in lesson planning. While it is not possible to address the needs of all students at the same time, it is important for teachers to be aware of this.
Therefore, based on the results, we would advocate for more integration of health-related content with corresponding methods in PE. For a long-term acquisition of health- and PA-related competencies, such as PAHCO with regard to knowledge, skills, abilities, and motivation, we would suggest distributing the health- and fitness-related content of PE over a longer period of time and setting the specific learning tasks over several lessons. This is also supported by the international discussion about PE and health content, highlighting the importance of having both the physical and educative parts of PE (Mong and Standal, 2019; Quennerstedt, 2019). However, regarding our differential results, it is evident that content and teaching methods should be varied (Brophy, 2002) to meet the different needs of students.
Supplemental Material
sj-docx-1-epe-10.1177_1356336X211037432 - Supplemental material for Promotion of physical activity-related health competence in physical education: A person-oriented approach for evaluating the GEKOS intervention within a cluster randomized controlled trial
Supplemental material, sj-docx-1-epe-10.1177_1356336X211037432 for Promotion of physical activity-related health competence in physical education: A person-oriented approach for evaluating the GEKOS intervention within a cluster randomized controlled trial by Stephanie Rosenstiel, Carmen Volk, Julia Schmid, Wolfgang Wagner, Yolanda Demetriou, Oliver Höner, Ansgar Thiel, Ulrich Trautwein and Gorden Sudeck in European Physical Education Review
Supplemental Material
sj-docx-2-epe-10.1177_1356336X211037432 - Supplemental material for Promotion of physical activity-related health competence in physical education: A person-oriented approach for evaluating the GEKOS intervention within a cluster randomized controlled trial
Supplemental material, sj-docx-2-epe-10.1177_1356336X211037432 for Promotion of physical activity-related health competence in physical education: A person-oriented approach for evaluating the GEKOS intervention within a cluster randomized controlled trial by Stephanie Rosenstiel, Carmen Volk, Julia Schmid, Wolfgang Wagner, Yolanda Demetriou, Oliver Höner, Ansgar Thiel, Ulrich Trautwein and Gorden Sudeck in European Physical Education Review
Footnotes
Acknowledgments
We thank all the schools, teachers, and students who participated in our studies. Furthermore, we thank our research assistants and the regional council of Tübingen (Department 7, Sport) for their support. We also gratefully acknowledge the support of the Deutsche Forschungsgemeinschaft.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Deutsche Forschungsgemeinschaft (Grant no. 397847999).
Supplemental material
Supplemental material for this article is available online.
Notes
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.