
Abstract
Objectives
Horizontal integration of health and social care in England is frequently supported by multi-disciplinary (MDT) case management focused on high-risk older people with multiple chronic conditions living in the community. This paper analyses MDT working in two of the 25 areas participating in the Integrated Care and Support Pioneer Programme in England. The analysis aims to understand the experience of frontline staff in such MDTs of working with professionals and staff from multiple sectors, and their perceptions of their roles and the benefits of integrated working.
Methods
We conducted semi-structured interviews with a purposive sample of 54 frontline staff from a range of professional backgrounds working in 11 community-based MDTs in two Integrated Care and Support Pioneers. A largely inductively developed coding frame was used to thematically code and guide analysis of verbatim interview transcripts from audio recordings.
Findings
Staff conceptualised the team as a cohesive yet ‘porous’ entity, able to evolve a shared sense of purpose to deliver holistic care that helped to level traditional professional hierarchies, enable collective problem-solving and share responsibility for patient care. MDT working was seen as benefiting staff and patients. Despite strong similarities between the MDTs in members’ understandings of the role and purpose of a MDT, each MDT was adapted to its context and the needs of the population served. The process of working through inter-professional tensions seemed to strengthen relationships within the team and enhance its ability to work effectively in the local health and care system. However, without performance or outcome measures, these perceptions were driven by ‘soft’ intelligence alone.
Conclusions
Frontline staff accounts of MDT working demonstrate their strong commitment to this way of working, as a mechanism enabling them to deliver more holistic care with perceived benefits to patients.
Introduction
In England, integrated care is currently regarded as the most cost-effective way of managing multimorbidity whilst enhancing patient experience for a resource-constrained National Health Service (NHS) serving an ageing population. 1 Integration can be implemented at various levels in health and care systems, most importantly coordinating the professional and service inputs at the patient or client level (henceforth, ‘patient’). 2 For older people in the UK, living in the community with multiple chronic conditions, integrated care is primarily delivered through multi-disciplinary teams (MDTs).3,4 Yet, these teams have seldom been studied in detail from the perspective of the staff involved.
The analysis in this paper forms part of a wider national evaluation of the Integrated Care and Support Pioneer Programme (2013–2018). The 25 volunteer Pioneers were tasked with delivering person-centred care by taking a ‘whole system’ approach to local integration across health, social care, the voluntary sector and other public services. 5 Most deployed similar initiatives, community-based MDTs being among the most widely reported. 4
The aims of the MDT component of the wider evaluation, undertaken in two volunteer Pioneers, were (1) to examine the long-term impacts and cost of providing health and social care through community-based MDTs supporting people aged 55 and over living with multiple chronic health conditions; and (2) to explain any observed differences between Pioneers, considering their local system contexts and characteristics of the patient populations they served.
We have written elsewhere about the perceived obstacles to integration at strategic and managerial level in the Pioneer local health and care systems 6 and the contribution to case management of multidisciplinary team meetings. 7 In this paper, we draw on interviews with frontline MDT staff to understand their experience of working with professionals and staff from other disciplines and sectors, and their perceptions of the aims, functions and benefits of integrated working.
Setting
The four models of MDT working in the two Pioneers (n = 11 MDTs) analysed in this paper are described in detail elsewhere.6,8 The first Pioneer (P1) covered an inner-city area, with a coterminous NHS Clinical Commissioning Group and the local authority. P1 hosted eight MDTs, which operated to broadly the same model. Local acute services were provided by two hospitals. Pioneer 2 (P2) covered a mixed urban-rural area whose NHS Clinical Commissioning Group spanned the whole of one local authority and parts of two others with social services responsibilities. P2 hosted three MDTs, each with a different operating model. The population of P2 was 30% bigger than P1. Another difference between the two Pioneer sites lay in the populations they targeted. P1 set out to respond to complex cases with multiple needs, including people living with disabilities, mental health problems and multiple social needs, and P2 focusing more exclusively on older people with multiple long-term health conditions and on care home residents.
Following piloting in P1, the Pioneer adopted a model relying on weekly face-to-face MDT meetings chaired by local integration leads. In P2, three different models of integrated MDT care were established to reflect the different histories, service systems, needs and development opportunities across the area. The P2a model had been developed in a large general practice to prevent hospital admissions and facilitate discharges. The second model (P2b) was also primary-care led. It was designed by a general practice, in partnership with the manager of a residential home, to improve general practitioners’ (GPs’) access to beds in the home to avoid admissions and facilitate hospital discharge. The third model (P2c) was introduced by the local NHS Acute and Community Trust with the purpose of enabling hospital discharges and supporting patients at home.
Methods
Data collection
Forty-five face-to-face and remote (telephone or video conference) semi-structured interviews and one face-to-face focus group (at the request of staff) were conducted with 54 frontline staff members between December 2018 and March 2021, before and after the first pandemic lockdown in England. Staff reflections on MDT working during the pandemic as well as its legacy for future integrated service delivery are explored elsewhere. 9 The interviews were conducted by GW, ND, AP and LT using a purposive sampling strategy. All staff working in the MDTs within the data collection period were contacted and invited to participate. Efforts were made to secure interviews with all the different types of staff involved in the MDTs.
Respondents’ job roles across Pioneer sites, by number.
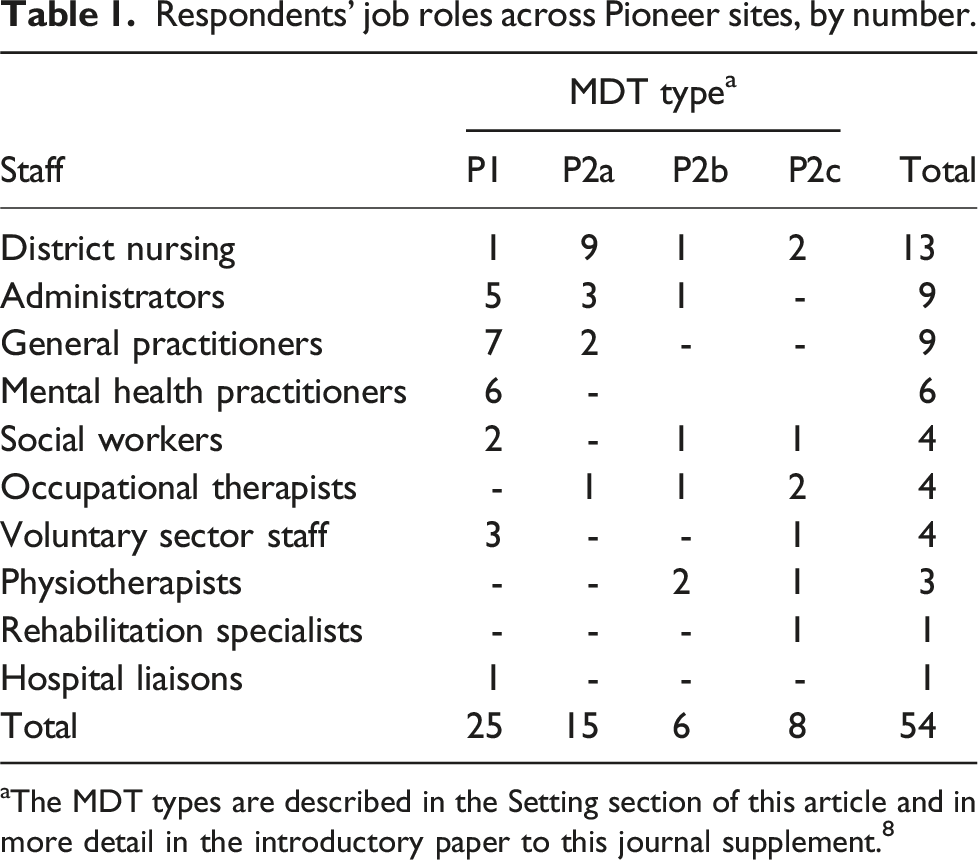
aThe MDT types are described in the Setting section of this article and in more detail in the introductory paper to this journal supplement. 8
Analysis
A coding frame and theme definitions were generated (by LT and GW) from the preliminary inductive coding of a subset of six interview transcripts, and later refined through team discussions (see S1 and S2 in the Supplement B). Coding in NVivo and interpretative thematic analysis was conducted (by LT, AP, LR, MAD, GW, and NM) on the full dataset in stages: initial coding of transcripts, grouping of codes and memoing, preliminary construction of sub-themes and themes, memo and theme refinement, and structuring themes.
Reflexivity
The analysis was performed by team members diverse in terms of age, ethnicity and gender, with firsthand experience of interviewing the participants, attuned to the meaning-making of participants. 10 whilst able critically to interpret their face-value accounts. 11 Other team members acted as ‘critical friends’.
Results
Various sub-themes were organised under five higher order themes, and are presented in the following sections: (1) aims of the MDT; (2) team membership, identity, parity of esteem, and leadership; (3) barriers to MDT working; (4) perceived facilitators of and incentives to MDT working; and (5) relationships with other teams locally.
Aims of the MDT
Staff identified two categories of aims that motivated the work of their MDT: (1) the original aims that the MDTs were commissioned to address; and (2) the day-to-day pragmatic purposes MDTs had developed in response to individual needs.
Original aims set for the MDTs
Staff reported three overarching original local system aims derived from national policy: reducing avoidable hospital admissions; identifying and caring for high-risk patients; and integrating social and health care (discussed in more detail elsewhere).
6
Initially, the role of MDTs was to implement an innovative multidisciplinary approach for people identified as high risk or likely to deteriorate. Interviewees suggested this focus went hand in hand with preventing avoidable hospital admissions and readmissions. Operationalising this aim meant providing care in the community, fostering independence, acting as a first point of contact (especially in P2, a mixed urban-rural area), and redirecting patients to primary care to reduce need for unnecessary emergency care: I would say the goal of the MDT … is to avoid preventable hospital admissions and to promote independence for individuals within the community. (Occupational therapist, P2)
A holistic person-centred approach to care was identified as a fundamental commitment within teams that informed and guided daily practice. Essential to this approach was the use of multi-disciplinary expertise to provide more comprehensive assessments and a group approach to problem-solving, providing broader perspectives on patients’ needs including their home environments and social needs: We can help, along with all the other professionals in the [MDTs], give people a holistic support and guidance. We’re looking at every angle. (Voluntary sector staff member, P1)
In practice, this approach often highlighted the need for greater social care input: A lot of the issues we discuss about [high risk] patients are to do with social care issues rather than medical, I have to say. (GP, P1)
Day-to-day pragmatic purposes MDTs
Frontline staff experienced some tension between the official MDT aims and supporting the wellbeing of specific patients. While staff endorsed the preventive orientation, avoiding hospital admission was not always considered helpful to patient wellbeing. Some staff questioned the premise that MDTs should always work to reduce hospital presentations: It’s too blunt an instrument to say we’re trying to avoid hospital admissions. That’s not exactly it, is it? We’re trying to help people live better for longer and to address health inequalities, and for that you have to work differently. And that will mean trying to get people medical attention that they need, not just trying to keep them out of hospital. Similarly, it’s not always best that people stay in their own homes. (Community matron, District nursing, P1)
The original aims were perceived as requiring adaptation by MDTs in order to respond more proactively to the immediate needs of individual patients, often formulating novel solutions which entailed ‘going above and beyond’ usual professional roles: It’s a lot of vulnerable patients who can’t make the phone calls or return the letters or keep up with their appointments. And they get really overwhelmed, so we take over that for them. (Administrator, P1)
Alongside such ‘low level’ needs, they also recognised that more proactive approaches to care included pre-empting potential deterioration through additional service inputs. By utilising their wider skill base, MDTs were able to assess the often-complex needs of patients and their carers, and to address needs that would otherwise have gone unmet: As I first saw him I realised a static commode wouldn’t be suitable for him ... I spoke to the GP, told her about my concerns and she then said, ‘Well, we’ve had some bloods back, they’re not great, I think we should get him into hospital,’ and I totally agreed with her … That patient went to the acute hospital, whereas initially he came to us because he needed a commode. (Occupational therapist, P2)
Thus, MDTs allowed staff to exchange information and mutual support about complex cases that would otherwise have required multiple referrals and delays in care. Interviewees also thought MDTs better enabled staff to care for patients who did not fit neatly into service or diagnostic boxes, including acute patients whose learning disabilities had not been recognised. GPs acknowledged that the holistic approach filled a gap by providing a wider range of services and care options to individuals than they had time to investigate and action themselves.
Team membership, identity, parity of esteem and leadership
Four subthemes relating to intra-team factors comprise the second prominent higher order theme. Together they elucidate team membership, members’ sense of belonging, parity of esteem as well as the influence of leadership.
Team membership
Staff reported that MDTs usually had input from social workers, GPs, nurses, acute care liaison staff, and administrators. P1 (conurbation) teams and one in P2 (mixed urban-rural) had representation from mental health services and the community and voluntary sector (CVS), including social prescribing. All P2 teams contained an occupational therapist, and one also included reablement workers and housing representatives, while GPs attended that team only occasionally.
There was consensus about the value of diverse MDT skill mixes within MDTs, and/or their ability to access such inputs, to overcome limitations of individual professionals’ knowledge and skills, and thereby enable more holistic approaches to care. The contribution of social care and, where applicable, mental health staff was particularly acknowledged: I think if the mental health team’s not there, it’s a shame. If social services aren’t there, it’s a disaster - that’s really fundamental. We are missing the community matron at the moment and that makes a big difference … I think it’s a good spectrum. I don’t think there’s anyone who’s superfluous and I think everyone is really necessary. (GP, P1).
However, staff highlighted limitations associated with a lack of specialist input - in particular, housing, learning disabilities, the management of specific chronic conditions (e.g. Parkinson’s disease, diabetes), pharmacy, community therapists, dietetics and end-of-life care. Perceptions of ‘missing’ professional input indicated the complexity of local population needs.
The membership of the MDT was seen to be ‘porous’, enabling each of the 11 MDTs to flexibly reconfigure their team as required at times on a case-by-case basis, while maintaining a generally stable ‘core’ membership. In some MDTs, invitations were extended to professionals outside the MDT ‘core’ when particular expertise was needed: We can invite guests. So, if we’re discussing a patient and they have misuse in drugs and alcohol, for example, we can always invite a liaison officer from [Trust’s addiction and substance misuse service]. (Administrator, focus group, P1).
There was some variation in who attended MDT meetings, how often, or for how long. For example, in one P2 site, GPs and district nurses attended only a specific part of the meeting where their expertise was required. The main reasons given for variable attendance were lack of time and pressures of day-to-day jobs, and the length and frequency of meetings. Thus, staff weighed up the perceived value of attending, particularly when their input was limited: They want value for what they’re doing. So, if they can just ring and check in and it takes a five-minute phone call, obviously travelling to the MDT, spending anywhere up to an hour at the MDT and then going on to their workplace, you’re taking a couple of hours out of their day … To do that on a regular basis is a big commitment, and I think that’s probably why it’s dried up. (Lead nurse, District nursing, P2).
Staff distinguished ‘core’ and peripheral team members by frequency of attendance at MDT meetings. This seemed to raise questions for participants about the extent to which professionals considered themselves or others to be part of the team, whether the team was truly multidisciplinary, and whether its members worked in an integrated way: I think the fact that it’s called an MDT meeting when it might occur between a nurse, an administrator and a GP. I don’t see that that’s true MDT, because multidisciplinary isn’t just medical professionals, it’s therapy as well. … I think to make it a holistic approach and to make sure it’s an effective service for patients, if you’re entitling it an MDT you need to have an occupational therapist, a physiotherapist, a GP, a nurse and a social worker. I would say they would be the core people involved to make it an MDT. (Occupational therapist, P2).
Uncertainty around the utility of attending MDT meetings may have contributed to less frequent engagement by more experienced staff. Such absences were seen by a few as potentially unfair on their patients who may have missed out on access to services made available to others. Some professionals (e.g. GPs) circumvented the issue by establishing a rota for attending meetings. However, apparent variations in commitment to meetings could also be interpreted as an efficient use of the expertise of professionals who were needed on an irregular basis.
Members’ sense of belonging
The degree to which staff felt that they belonged to the team seemed to vary, particularly among those who were periodic attendees. By contrast, those identifying as ‘core’ members tended to value the sense of belonging and support they felt in working in the team: Having relationship-based care improves work satisfaction, improves enjoyment, improves people’s wellbeing. And the people who attend regularly love it and feel quite protective and possessive of it. [That’s] because it’s a joy to work with other people, to have both relationships, as well as case discussion. ... It does build bridges. (GP, P1)
Staff participating from different services meant that different professional cultures and regulations were brought into the teams. Whilst benefitting from belonging to the MDT, professionals retained and drew on their ‘external’ professional identities. Indeed, some saw MDT participation as ‘extracurricular’ while also recognising that the mutual support they received in managing complex cases was an incentive to engage. However, MDTs were sometimes associated with ambiguities around responsibilities for tasks, duplication of work, or role crossover: It was around the community team, obviously, and the GPs. There was a little bit of friction, maybe to start off with, about roles and responsibilities. But I think they’ve ironed that out … I think it was around expectations probably. (Social worker, P2).
Instances of disagreement particularly related to decisions about including patients on statutory registers or the escalation of cases in emergencies – what was urgent from one professional/service perspective might not be from another. Open and honest communication, equality of voice within the team, and respect for differing disciplinary opinions both supported the resolution of personal frictions, and provided a ‘safety net’ for team members: It can have its challenges, definitely. But I think if you’re the sort of person that’s open, and understanding, … if you respect each other’s limitations and have a good awareness and acceptance and a tolerance of those things, then you can generally work well together. (Community matron, District nursing, P2)
The sense of belonging reported by staff in all MDTs seemed to develop through the experience of navigating staff frictions over time, resulting in improved working relationships and greater awareness of individual remits. Being able to voice an opinion, listen to each other, and engage in productive, regular discussions helped break down any initial interpersonal barriers. Attending MDT meetings and getting to know other members also made it easier to develop reciprocal trust and support for managing complex cases: It’s taken time to develop. At first, when I used to come to the meeting, I used to feel a bit like an outsider, I suppose, and I wasn’t quite sure what I could contribute. But as time has gone on I suppose I feel more part of the team now. But it has taken time, because we work for different organisations. … But we’ve all got the same aim. (Community team leader, District nursing, P2).
Furthermore, this way of working seemed to improve professional satisfaction and motivation, and reduce staff isolation and silo-working: I often felt, prior to [MDT], I was just sending kind of ‘help’ signals into the vacuum. And I think it’s felt very different to channel them into a system that felt alive or responsive. (GP, P1)
Parity of esteem
Staff viewed the MDTs as comprising a range of experienced professionals who were competent and able to make and act on decisions, even in the absence of formal directions. This helped make teamworking more balanced and value for money: I think we’re very lucky because we’re fairly experienced clinicians. … Other people might look and say, ‘It’s a lot of money,’ but I think it’s money reasonably well spent. (Community matron, Mental health practitioner, P1).
In comparison to their experience of other teams, MDT staff generally described feeling valued and heard irrespective of their seniority, profession, or job description. In particular, some staff highlighted the absence of obvious medical hegemony, with the MDTs being far less hierarchical than other teams: It’s a small team and everybody gets on. There’s not the GPs on a pedestal. … Those days have gone and everybody just works together. (Community care coordinator, District nursing, P2).
A commitment to equity regardless of seniority and experience level contributed to a sense of cohesion and mutual respect, even when some members seemed to be more dominant at meetings or in terms of finalising decisions: It’s really interesting, I guess, about power within those groups and who decides what. I think that GPs are the dominant force in there. But in some ways, I think, actually having quite senior people in from lots of different places has meant that it’s much more even. ... I don’t know if that reflects a boundary change, if you like, but it certainly doesn’t feel like we’re clashing with each other so much as on the same page and just trying to come up with a solution. So it’s a bit more collegiate perhaps. (Nurse consultant, Mental health practitioner, P1).
Influence of leadership
Team leaders’ levels of professional experience and skills were seen as important for championing strategic vision and driving sustained efforts towards more integrated working: I think that leadership is essential for these sort of projects … It can be centrally held and you can bring in leaders who work with the PCN [Primary Care Network] to do it. But I think you need champions and you need people who get it and have a vision to make it happen. (GP, P2)
Organisational management was also reported to be essential for effective teamworking. For example, one P2 team initially lacked a formal management role but the appointment of a manager helped clarify roles, streamline processes for dealing with inter-staff issues, provide support to individual members, and foster the team’s sense of direction: When I started there was not much good management, … The whole team was all over the place. …Everybody was the manager … I would say, ‘What is each person’s job role? What to do, what not to do?’ Everybody used to take their own initiative. Now, being under one manager, who is the one who can guide everyone, that works well … So, now we have a named person to go to when you have a problem. (Physiotherapist, P2).
A good manager was perceived as someone who understood and appreciated all the team’s disciplines, and whose style of management was approachable, respectful, and supportive. This instilled a sense of equality amongst staff so that team members felt valued and included. By contrast, the rigid leadership style in another team was seen to impede its ability to collectively reflect on and challenge maladaptive practices.
Barriers to MDT working
Staff reported a number of challenges to MDT working, particularly in terms of the sharing of information between staff and services, varying patient service eligibility criteria, limited resources and high staff turnover.
Sharing of information between staff and services
Imperfect, or absent, links to different services were seen as continuing to hinder progress towards horizontal integration. Although MDTs improved staff’s awareness of available services and resources, established channels of communication remained necessary. Community health and care services were often difficult to navigate because of poor collaboration among these services and a lack of knowledge of their different eligibility criteria: What was typical which was that you had a service that you refer into and it wasn’t something that was necessarily created collaboratively or delivered collaboratively. So, it was more that we were just asked to refer into that service, and actually my sense is it hasn’t been very successful … because it’s really hard to make the case for something if you don’t really know it and you don’t know what’s on offer. (Nurse Consultant, Mental health practitioner, P1)
The main day-to-day problem was accessing records and clinical systems. This was often due to slow systems and no or poor Wi-Fi connections sometimes preventing information sharing in meetings, impeding the flow of meetings and causing care delays. In addition, staff suggested that a universal system linking health and social services would improve efficiency, though it was accepted that data protection and patient consent rules made this impossible. However, the lack of shared access to information could on occasion threaten patient or staff safety. For example, an administrator who visited patients at home for assessment purposes reported the following about a patient who had a number of weapons on display in their house: It would be fantastic if there was somewhere on that system that … [warned of such potentially dangerous environments] … Occasionally you go to a patient, and it’s not until you get in there and realise that actually you probably shouldn’t have gone on your own. (Administrator, P2)
Varying patient service eligibility criteria
Staff also reported a lack of flexibility in the eligibility criteria of some of the services to which the MDT referred patients, especially in allowing for the complexity of individual cases - some patients would be identified as too complex for one team but insufficiently complex for another. There was also a reported lack of flexibility to provide extended free care after hospital discharge beyond the then 6-week window of NHS community-based support. Where referrals were required to go through GPs, social services’ inability to refer patients directly to MDTs was criticised, and prohibitive, lengthening the process. Nonetheless, there was a general understanding that referrals had to be prioritised to manage demand.
Limited resources and high staff turnover
Staff suggested that there were insufficient resources within some teams to optimise the potential for reducing avoidable admissions. For example, having a housing representative in P1 MDTs, where senior social workers were responsible for both the social care and housing liaison roles, would have been especially helpful. Staff tried to make incremental improvements to patient well-being, but were often forced to recognise that readmission was inevitable for some people as it was not possible to sustain the required range and intensity of support at home: I think they’ve just got too much work on and constraints with budgets, they can’t always find the package of care for the patient, and the time to ring a therapist up and tell them what’s happening is time when they can be out assessing another patient. So, I understand the problems that they have, just I think sometimes the frustrations are there. (Occupational therapist, P2)
High levels of staff turnover was reported to disrupt team dynamics. Staff continuity was seen as essential to enabling strong intra-team relationships: It’s a very functional team and one of the ways it works so well is because we’ve worked together for a long time and we know each other well and we can bypass and shortcut with our communication, but when new people start it’s a bit complicated having to start that again, but I don’t suppose we can do anything about that really. (GP, P1)
Perceived facilitators of and incentives to MDT working
Staff reported a range of mechanisms through which their roles were made more efficient and their efforts more effective. These have been identified in sections above, and are expanded upon in the sections below. They are summarised in S3 in Supplement B.
Perceived benefits to staff
MDT discussions often centred on what the best solution might be for the patient, drawing on a wide range of perspectives and expertise. MDT meetings enabled professionals to share knowledge from the different professionals and services previously involved in the patient’s care, including their understanding of the patient’s wishes. Collectively, they would identify opportunities to provide support by coordinating a tailored care package: It was through the MDT [that] everyone could put their piece in of the jigsaw to help make sure that he [the patient] was getting the support he needed to help his life be a bit easier. (CVS Navigator, Voluntary sector staff, P1).
However, a few staff questioned the extent to which patients’ views were accurately obtained and adequately influenced care planning during MDT discussions. It was viewed as impractical to have patients and/or their carers attend the MDT meetings as they were not individual case conferences, but rather fast-paced reviews of cases. As a result, on occasion, differing opinions concerning the patients’ and carers’ wishes had to be resolved. Despite the logistical difficulties, some staff felt that patient perspectives should be better represented at MDT meetings: I think in a way key workers may be a step towards that because they’re very strong about stepping into the shoes of clients and advocate strongly for the client perspectives. I guess there’s a challenge because it’s a short sharp meeting. … So, actually, it’s probably not the place for the patient to be there, but is there a way to feed in their views and their priorities? (Nurse consultant, Mental health practitioner, P1).
MDT meetings were seen as enabling better coordination of care, shared responsibility and faster access to services by reducing the number of referrals that would otherwise need to have been made: I think for me it’s better coordination and improved care, because you’ve got a lot of different professionals, different skills in the same room all thinking about one person and how to manage the situation. For me also it is access to the service as well. It quickens how you access service for someone, because you’re not going to another referral again. (Community matron, Mental health practitioner, P1).
The interviewees also reflected that MDT working helped demystify other professionals’ remits, as well as the referral and intervention criteria and capacities of other services, thereby setting more realistic expectations about the nature and level of support that different services could provide: What might be perceived to be obstructive or unable to help us has changed as I got to know the remit of each team. As I got to know that better, it felt like less of a barrier and it was more about moderating my expectations. (GP, P1).
Perceived benefits to patients
Most interviewees suggested that MDTs enabled improved accuracy and speed in meeting individual needs in a coordinated way. Team decisions were more likely to result in positive action for the patient when individual members were clearly responsible for specific tasks. In addition, the need for repetition of patient and carer ‘stories’ was greatly reduced. In particular, staff reported a more efficient process for securing social care support for patients when all the relevant information could be collated and presented to the senior social worker who was then able to make decisions regarding social care packages: I would say that they would see that things are so much more joined-up, that people don’t have to repeat their stories, that they should in theory be getting the right care from the right clinical people or social care people. (Mental Health Liaison, Mental health practitioner, P1)
Improved access to different community services was described as especially important for ‘harder to engage’ patients. For example, a P1 administrator described the usefulness of having the local CVS and housing department working collaboratively, the feeling being that some patients were more likely to accept CVS than statutory help: We have a lot of patients that aren’t aware or that don’t really like to engage, and we have more of a culture of, ‘We’re going to bring that information to you. You’re vulnerable, you’re worried, you can’t seek that information yourself or don’t have the capacity to seek that information yourself. So, we are going to do that on your behalf, to provide you with the information to be able to improve your quality of health.’ (Administrator, P1)
Assessing benefits to patients
Staff generally reported either the absence of formal patient experience or outcome assessments to enable them to assess their MDT’s performance or their inability to access such data. Some teams reported using questionnaires, documenting patient feedback in patient notes, or requesting cards or emails to be shared with the team. A few acknowledged the complexity of assessing patient outcomes of MDT service provision and suggested this might be unquantifiable.
As a result, staff were largely guided by their own perceptions of patient experience and occasional patient or carer testimonials when interpreting the effectiveness of their collective efforts. Some staff appeared to rely on their observation of MDT discharges and a reduction in use of the MDT by ‘revolving door’ patients as evidence of success: From the [MDT] perspective, I don’t think they see a revolving doorway by one client that we’ve dealt with and who is brought back again and again and again, apart from when we are trying to do some follow-up. So, to me with that it seems that there is some gain. … [It is unclear] whether that is actually evidence, because, if not, I think there would probably be a revolving door of the same people who are just being brought back after a while with the same issues. (Mental health matron, Mental health practitioner, P1)
Some staff reported ignoring hospital use data, believing it irrelevant to the holistic improvements to patients’ lives and wellbeing which they sought to achieve: Creating team-based personalised care … [of] the patient’s medical problem and in the context of their lives, that’s what it’s doing. And I think that for me way outweighs the impact on hospital admissions and A&E attendances. It’s about getting patient-centred. (GP, P2)
Relationships with other teams locally
Initially, some MDTs were said to be regarded with caution within the wider system because they competed for resources with existing services and were perceived to risk blurring professional and organizational boundaries unhelpfully. Making evident the value of collaborative working by highlighting the patient-related benefits of MDTs, communicating complementary rather than competitive intentions, and gaining trust over time helped in overcoming some of these reservations: I think people thought we were going to replace existing services, and I think they thought we would muddy the waters. I think it was challenging some of their ideas, showing them that we aren’t there to replace them, that was a real big thing initially, that we’re to work alongside, and that actually we’re of value. So, once they saw we’re of value to what they’re doing, then obviously that makes their life easier. (Lead nurse, District nursing, P2).
However, the MDTs were still continuing to develop their external relationships, with other teams described as either not knowing about the MDTs or confusing them with other teams: The main thing that I have found is a problem is that nobody knows who we are and what we do. (Administrator, P2).
It was sometimes challenging for MDT staff to know who to speak to in the local health and care system, due to a lack of mutual familiarity and established relationships. Problems mentioned included overlapping functions with other teams and a need for better coordination to reduce the number of different teams involved: Looking at the district nursing teams, there’s quite a lot of overlap between [a community team] going in, district nurses going in, [MDT] going in, me going in. So, they can have four different teams potentially. So, that all needs tidying up. (Community care coordinator, District nursing, P2).
The differences in flexibility of roles and boundaries between the MDTs and other services sometimes created challenges relating to remit - for example, when other teams felt that a particular case fell within their ambit and wanted to take it on. Conversely, staff in P1 recognised the need for, and importance of, developing a stronger relationship and shared responsibilities with housing services, which they felt was vital for serving their population.
Discussion
Staff views were consistent across the four MDT models in the two sites regarding the nature and benefits of the ‘team’. The team was conceptualized as overwhelmingly driven by a shared sense of purpose to deliver holistic care, especially to the most vulnerable patients. MDT working was seen as benefiting patients and staff. Staff described the team as a leveller of traditional professional hierarchies, and a mechanism for collective problem-solving and sharing responsibility for patient care. The sense of team ethos, good relationships and equality of voice were seen as integral to successful MDT functioning, its case management decisions, and job satisfaction, while the team leads’ leadership skills were key to championing teams’ strategic visions.
By being porous, team membership allowed MDTs to adapt to meet local need. Yet, there were also constraints associated with team membership, the inability of certain team members to attend team meetings and staff turnover. Working through inter-professional ‘tensions’ and managing their responsibilities within the inherent constraints seemed to strengthen relationships within the team, enhancing the ability of the MDT to work effectively in the local health and care system.
The divergence among the MDTs in their composition, objectives and ways of working echoes a wide-ranging-mixed method evaluation of similar MDTs for people living with chronic conditions in London. 12
Despite this divergence, the egalitarian team ethos reported across the teams is in line with previous work on effective team working in community settings - for example, in primary care MDTs in the United States. 13 The current findings add to the literature by showing that navigating intra-team relationships and tensions in terms of role crossover and mutual responsibility takes continuous effort, but doing so may enhance a sense of shared purpose and responsibility, and identification with the team.
In the current study, the involvement of experienced professionals from different disciplines was associated with dissolving, in large part, the traditional medical hegemony over decision-making. This is in contrast with previous studies, which had suggested the persistence of a hierarchy and/or conflicts between medical and non-medical approaches to case assessment and management. 14 Our study revealed demand for more non-medical input than was available locally from social care, housing and specialist services (e.g. drug and alcohol services), especially in P1 where the MDTs’ caseloads often included patients with very complex challenges and needs, echoing previous research, particularly related to social care.13–15
The challenges facing the MDTs resonated with previous research - for example, the inflexibility of the criteria used by other services to accept patients referred by the MDT or the lack of capacity in the wider social care system. 13 These barriers seemed to persist irrespective of the robustness with which the MDTs themselves operated, thereby limiting their potential impact.
Gaps in staff knowledge about their MDT’s performance beyond their day-to-day experiences, were echoed by strategic level staff in our evaluation. 6 The measurement of outcomes for older patients in community settings is complex and nuanced and, as some MDT staff acknowledged, a reduction of hospital admissions may not in fact be attainable or even an accurate indicator of MDTs’ success. A growing body of evidence, including from the wider Pioneer evaluation, calls into question whether preventing increases in hospital admissions is even feasible through the actions of integrated care MDTs.15–18
Gathering ‘soft’ intelligence assumes that all patients and carers feel equally able to voice their experiences directly to staff involved in their care. Without access to formal performance data, staff relied on ‘soft’ intelligence to generate shared beliefs about the value of implementing holistic care.
Generally speaking, MDT meetings were not designed to be individual case conferences, but rather to provide high level overviews of cases and agree how they might be managed within local systems. Individual team members might bring information from direct contact with patients or present views of colleagues. Thus, decisions regarding referrals and such like were largely undertaken by proxies. in the form of professional team members. It is critical, therefore, that such meetings should be conducted within a well-developed person-centred culture and that direct patient and carer relationships should always be based on the same principles. Non-participant observations of team meetings undertaken as part of our wider evaluation 7 suggested that team meetings revealed a commitment to patient-centredness even in the absence of patients and informal carers. However, some staff in the current study suggested that it would have been beneficial to involve patients directly but acknowledged that it would not be feasible for them to attend meetings in person. Other studies have highlighted the importance of the patient voice, at the very least to be able to explain treatment and support plans to patients and their carers directly.19–21 The absence of patient and/or informal carer voices also risks limiting the potential for improving MDT services and for identifying harms particularly with this patient population, who have been found to be at higher risk of experiencing safety incidents. 22
Implications for policy and practice
The continued ‘integration’ of MDTs into their wider networks may require active facilitation to improve mutual awareness and strengthen relationships between them and other services. Pre-pandemic, there was an urgent need for commissioners to invest in better information technology and systems, 7 especially Wi-Fi in primary care premises and joint health and social care patient records. While the imperative during the pandemic to shift to virtual communication may have improved the situation regarding connectivity, it would be worth examining current provision, in particular, the support for efficient hybrid meetings. 9 Better equipment and access to records will not only improve meeting efficiency, but also the timeliness of care delivery and enhance both patient and staff safety. Likewise, it is worth considering the cost-effectiveness of addressing team-specific gaps in expertise (e.g. from housing services), to enhance internal decision-making.
The identified lack of patients and carer voices in MDT decision-making can be rectified by finding ways of involving them more directly - for example, by having referring professionals routinely taking steps to obtain their preferences before MDT discussions. 12 In addition, following Cribb and Woodstock, 18 by collecting patient-reported outcomes, perhaps alongside much more systematic qualitative data, MDTs would be enabled to better identify what matters most to patients with a view to providing genuinely person-centred care. This would also provide evidence for performance monitoring by system and MDT-specific leadership and foster service improvement initiatives, while providing the feedback that staff desire.
Limitations
There are two main limitations to our analysis. First, our sample of respondents was somewhat restricted by circumstance. We collected the views of those frontline staff willing and able to provide their perspectives, some of whom were operating during a global pandemic when staff were under extreme pressure in the NHS. We were unable to obtain interviews with GPs in two of our four MDTs, who may have provided alternate views on the utility of these MDTs in such conditions.
Second, our results are based on MDT team members’ qualitative assessments of their own MDT’s activities. There is therefore potential for a biased assessment of the effectiveness of the work of the MDTs. This does not necessarily imply a need for quantitative outcome measurement, but rather for a systematic approach to collecting patient narratives and interpreting them. 23 Reliance on anecdote and episodes that professionals remember provides a very incomplete picture. For instance, the MDT patient and carer perspectives from the accompanying analysis by Durand et al. 24 give a different perspective. While patients and carers in that study valued various aspects of care provided by MDTs, views about whether their care in general was ‘joined up’ varied. Some also reported feeling let down and angry by the failings they had experienced.
Conclusions
Staff were generally positive about MDT working, believing that such approaches led to clearly improved ways of working and greater process efficiency, which, in turn, directly enhanced their ability to deliver more holistic care. However, without performance data, these perceptions are often driven by ‘soft’ intelligence alone. The Integrated Care Systems in England should work to ensure that community-based MDTs become more securely networked with one another and within their wider local health and care systems. This should improve communication within and between MDTs and make system navigation more efficient for staff. Unless additional resources, further integration within the wider system, and flexibility to offer complex patients more care are implemented, the MDTs will be impeded in their ability to operationalise their intended purposes and deliver care to its full potential.
Supplemental Material
Supplemental Material - Frontline staff perspectives on multi-disciplinary team working and the effectiveness of integrated service delivery: Findings from the evaluation of the Integrated Care and Support Pioneers in England
Supplemental Material for Frontline staff perspectives on multi-disciplinary team working and the effectiveness of integrated service delivery: Findings from the evaluation of the Integrated Care and Support Pioneers in England by Lavanya Thana, Gerald Wistow, Mary Alison Durand, Agata Pacho, Lucia Rehackova, Nick Douglas, Mustafa Al-Haboubi and Nicholas Mays in Journal of Health Services Research & Policy.
Footnotes
Acknowledgments
We wish to thank all of those - patients, informal carers and staff - who participated in the MDT evaluation, and staff at the Pioneer sites who helped to facilitate its implementation. We also acknowledge the contributions of our former colleagues Nick Douglas, Ties Hoomans and Tommaso Manacorda to the development of our conceptual model of MDT functioning.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is an independent evaluation funded by the NIHR Policy Research Programme (Evaluation of the Integrated Care and Support Pioneers Programme in the context of new funding arrangements for integrated care in England (2015–2022), PR-R10 -1014–25001). NIHR played no role in the conduct of the research or preparation of this manuscript. The views expressed are those of the authors and are not necessarily those of the NIHR or the Department of Health and Social Care.
Ethical statement
ORCID iDs
Data availability statement
The datasets generated and analysed during the current study are not publicly available because they contain information that would identify the research sites, individuals, and/or case-material and it would not be feasible to redact or otherwise anonymise them. The data custodian is Professor Nicholas Mays, London School of Hygiene & Tropical Medicine.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.