
Abstract
Objectives
The lack of Indigenous health care data in Canada makes it challenging to plan health care services and inform Indigenous leadership on the health care needs of their respective Nations and communities. Several Canadian health care organizations have implemented a voluntary Indigenous identifier of patients within their electronic medical records. This study examines facilitators and barriers to implementing such a voluntary self-reported Indigenous identifier, from the perspective of key stakeholders who work at four Canadian health providers where an Indigenous identifier has been implemented.
Methods
The four Canadian sites comprise three hospitals and one health authority. At each site, key stakeholders participated in semi-structured qualitative interviews. Interviews were transcribed and coded. Relevant documents that were publicly available or provided by each site were reviewed.
Results
There were four primary findings. First, for the introduction of an Indigenous identifier to be successful there must be pre-existing strong and trusting relationships between Indigenous communities and health care organizations. Second, health care organizations must provide training for those who ask clientele to self-identify as Indigenous, to overcome issues such as any patient backlash. Third, for the relationship between Indigenous people and health organizations to flourish, data governance must be Indigenous-led. Finally, the collection of Indigenous identifier data can enhance Indigenous health care services and health care service planning and delivery.
Conclusions
Due to the ongoing distrust of government and health care services among Indigenous peoples and communities, special considerations are required prior to the implementation of an Indigenous identifier. Of primary importance is how health care organizations can contribute to Indigenous data governance and minimize potential harms associated with the collection of such data. The findings of this study can be used to guide other health care sites and Indigenous leaders aspiring for more robust health data by implementing voluntary Indigenous identity data collection.
Introduction
The Truth and Reconciliation Commission of Canada is a government-funded agency established to allow those affected by previous Canadian governments’ policy of separating Indigenous children from their families and communities, relocating them in residential schools, the opportunity to share their stories and experiences. 1 In 2015, the commission issued a set of calls to action to redress the legacy of this policy. Call to Action 19 exhorted the Canadian government ‘to establish measurable goals to identify and close the gaps in health outcomes between Aboriginal and non-Aboriginal communities. 2 (pp.2-3) Despite this call, health care utilization and health outcomes for Indigenous peoples remain difficult to measure across Canada. This is due to several reasons, such as many health care service organizations do not collect Indigenous identity data and among those that do there is no consistent Indigenous identifier in administrative health datasets.3,4
Canada’s health information system is primarily informed by the national census, provincial vital registration systems, primary and tertiary health care utilization records, disease surveillance and registration systems, and national health and social surveys. These all use inconsistent, inconclusive, and unreliable methods of gathering Indigenous identity information, if it is collected at all. 3 For example, the national Aboriginal Peoples Survey excludes First Nations people living on-reserve. 5 Furthermore, government and health care organizations data collection practices are often top-down initiatives that have historically excluded Indigenous participation in design and analysis.
While data quality problems exist, it is estimated that there are 1.8 million Indigenous peoples in Canada, accounting for approximately 5% of the Canadian population. 6 Indigenous peoples and nations across Canada are diverse, with unique governance structures, cultural practices, and local contexts that drive health outcomes and health care options. They nevertheless share one of the single most important determinants of health among Indigenous peoples today: a common experience of colonization. 7 Due to colonialism, Indigenous identity is complex and deeply personal. Colonialism has resulted in severed ties between many Indigenous peoples and their traditional territories and kin. 8
Across Canada, Indigenous people experience a disproportionately high burden of physical, mental, spiritual, and emotional health issues compared to their non-Indigenous counterparts.9,10 These health disparities can be attributed to the enduring impact of colonialism, such as inadequate funding for Indigenous health care services and an ongoing problem of systemic racism in Canadian health care settings.11–13 Racism can discourage efforts to seek health care or lead to avoidance of health care until a condition becomes urgent which can contribute to the burden of disease and injury. 11 Despite ongoing colonial violence, Indigenous peoples and communities have displayed remarkable resistance and strength, and there has been a resurgence of Indigenous culture, language, healing and wellbeing practices.14,15 The complexity of Indigenous identity and a shared history of colonial violence and displacement raise important questions around how best to track the health status of a diverse but underserved population as means of overcoming health inequities. Given the distrust among Indigenous peoples of government, research institutions, and health care organizations, such initiatives require special consideration prior to collecting Indigenous identity data.
Across Canada, there has been growing interest among Indigenous communities and researchers to collect Indigenous health data that is accessible and relevant to Indigenous communities. 3 In response, we conducted a case study of four Canadian health care sites that have implemented a voluntary self-reported Indigenous identifier into their electronic medical records (EMR). The interviews conducted for this project reveal that the self-reported Indigenous identifier was implemented with the intention to improve access to Indigenous-specific health care services, such as cultural supports, and to enhance Indigenous health care data for service planning purposes. We wished to learn from these sites’ experiences, to provide guidance and insight into a self-identifier as one potential avenue to improve Indigenous health data. Specifically, we sought to examine lessons learned, challenges, and successes in implementing a voluntary self-reported Indigenous identifier from the perspective of key stakeholders at each of the health care sites.
Methods
The core research team includes First Nations (KW) and non-Indigenous (MG, RH, RO) researchers located within university and health services settings with extensive experience of working with Indigenous research partners. The research was guided by a Research Advisory Committee (RAC) comprised of six members, four of whom are Indigenous and two who are non-Indigenous. The RAC brings extensive expertise in Indigenous health care. The intention of the RAC was to ensure accountability in the research process, such that the research would be beneficial to Indigenous communities and decision makers, in addition to providing methodological and analytical guidance. The core research team and the RAC met on two occasions to discuss the methodology and provide feedback on key themes emerging from the work. The RAC members were invited to be co-authors on the paper.
We carried out a multiple-site qualitative case study. Voluntary self-reported Indigenous identification for health administrative data was the focus of inquiry. We utilized the approach described by Yin, which involves two key components: (1) an in-depth investigation of a contemporary phenomenon to understand its context; and (2) exploring multiple variables using various sources of evidence for triangulation. 16 Case study research is beneficial for in-depth description of a social phenomenon and to expand the knowledge of a specific site. 17 A multiple case study approach is required when the study contains more than a single case, all of which emerged from different contexts to identify similarities and differences between the cases. 18
The selection of sites included three hospitals in small cities (populations under 150,000) in Canada, and a health authority in Western Canada. Health authorities differ from hospitals in that they govern, plan, and deliver health-care services within a geographical area rather than a single location. 19 Three of the sites using an Indigenous identifier were found through Google searches, with the fourth recommended through snowball sampling. The three hospitals had implemented the identifier within the last 3 years. The health authority implemented an identifier over a decade ago, being the first health care organization in Canada to do so.
Participants included health care leadership at each site, recruited via purposive sampling. Seven of the nine interview participants self-identified as Indigenous and two identified as non-Indigenous.
Semi-structured interviews were conducted between March and June 2022. The interviewers relied on an interview guide but allowed room for additional questions to emerge organically. Participants were asked about the organizational decision to develop an Indigenous identifier and the implementation process, with lessons learned, challenges, and successes in mind. Each interview lasted between 30min to 1 hour. The interviews were recorded and transcribed verbatim. In addition, each site was invited to provide relevant documents to the identifier’s implementation that they were comfortable sharing with the research team. All publicly available documents - including press releases, informational guides, and news articles about the Indigenous identifier for each site. These documents were used to provide additional context to the interview data.
Interviewee and site characteristics.
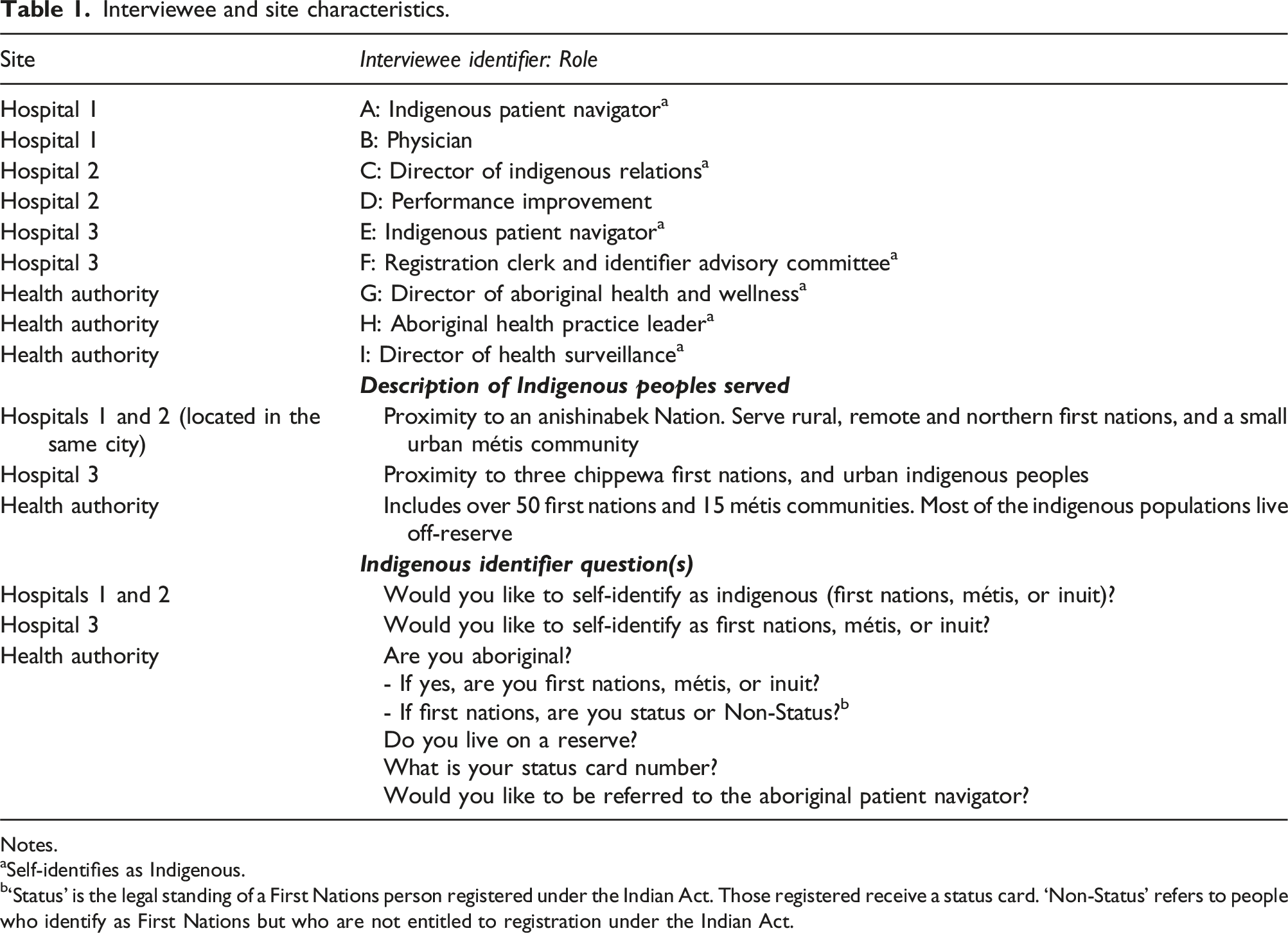
Notes.
aSelf-identifies as Indigenous.
b‘Status’ is the legal standing of a First Nations person registered under the Indian Act. Those registered receive a status card. ‘Non-Status’ refers to people who identify as First Nations but who are not entitled to registration under the Indian Act.
Data collection and analysis occurred concurrently. 16 Consistent with multiple case study design, each case was viewed as a separate entity instead of a single sampling unit. 16 The cases were then taken together to identify synthesis between the cases. The transcripts attributed to each case were read together along with any other accompanying data provided by the site or available publicly to triangulate data and identify any points of contention within the site. This phase led to the identification of meaningful patterns relating to the project aim regarding lessons learned, challenges, successes, and outcomes from the implementation of an Indigenous identifier across the sites.
Results
The four case studies taken together identified four major findings that are interwoven throughout each of these steps of implementation: (1) the implementation of an Indigenous identifier requires strong relationships with local Indigenous communities; (2) extensive training for any staff that will be collecting an Indigenous identifier in health care settings; (3) Indigenous-led data governance is crucial for such relationships to flourish; and (4) the collection of the Indigenous identifier can enhance Indigenous health care services and health care service planning and delivery.
Strong relationships with local Indigenous communities
All four sites reported that the implementation of the Indigenous identifier was initiated by an Indigenous person in a leadership role. At three of the sites, the initiative was started by an Indigenous leader within the health care system and, at the fourth, by a local First Nations community leader.
Once the need for an identifier was identified, the first step was for the health care organization to engage surrounding Indigenous communities and organizations that served urban Indigenous peoples, to better understand their concerns and assess local support for the identifier. All the interview participants described their relationships with the surrounding Indigenous communities as strong and existing before the identifier was created, which allowed for fruitful discussions to take place. Following this, the three hospital sites set up internal working groups prior to implementation. The working groups included a diverse range of members, including Indigenous leaders, Elders, senior management, frontline staff, and patient representatives. The working groups were tasked with establishing how the identifier would be asked, when, and how frequently. For all the sites, disclosing Indigenous identity was voluntary and relied on self-disclosure, which was considered imperative by community partners at all the sites to build trust with Indigenous patients.
Extensive training for sites’ registration clerks who ask identifier questions
One of the interviewee’s spoke about the time and care that went into deciding how the question would be asked at registration: We actually did a whole brainstorming: we ended up with about 20 questions ... Then we had decided, ‘OK, I think we need to now go a community and really get a sense of what their thoughts are.’ We did a little more work on narrowing the question down. We were being very cognizant of using the proper language. We wanted to use Indigenous language. (Interviewee E)
Prior to launching the identifier, each site engaged in outreach activities to inform the local Indigenous community about the identifier. This was done to reduce surprise once the identifier was launched and patients would be asked to voluntarily self-identify during health care registration. The outreach activities continued after the launch of the identifier and included a range of tactics, including YouTube videos, social media posts, traditional media releases, and brochures specifically for Indigenous communities and service providers. The other element of implementation was to train registration clerks (RCs) tasked with asking each health care client whether they wanted to self-identify as Indigenous.
Hospital 1 and 3 reported pushback from RCs tasked with asking every patient if they wanted to self-identify as Indigenous. RCs raised concerns about the increase in workload due to the additional question at registration. Some staff were also concerned that because every person being registered would be asked to self-identify as Indigenous, they would be accused of being ‘racist’ by the public, presumably seen to be racially profiling patients. Some of the staff also said they believed the initiative itself was ‘racist’ because to openly discuss or acknowledge Indigenous identity was problematic. Such sentiments among RCs required the organizations’ management to challenge this perspective among non-Indigenous staff by raising awareness about the initiative for achieving Indigenous health equity. As one participant who led the implementation at a hospital noted: We had to very intentionally be very mindful because [the staff] were referring to this initiative as a burden and as racist themselves. So, just changing those internal conversations and we tried to find opportunities to interject in … [what] didn’t come naturally. (Interviewee A)
The RCs’ response at Hospital 1 resulted in the launch of the identifier being delayed pushed back by 4 months to allow time for more RC training on the initiative. RCs’ discomfort asking if patients wanted to self-identify as Indigenous was a major barrier for these two sites and hindered the systematic collection of the data, which impacted the quality of data and potentially the ability to connect Indigenous patients with beneficial services. An RC at a different site said that, whereas her department was asking every patient if they wanted to self-identify, other departments were not routinely doing so: I don’t know what the hesitation is: do they just not find it valuable? Or are they tired of hearing the comments [from the public] and so they’re just not asking now? … [A patient] came from emergency …] but that question hasn’t been asked. And you can see [the same patient] had three prior visits and that question hasn’t been asked. (Interviewee F)
Reflecting on the implementation process, one interviewee reported that if they had the opportunity to launch the identifier again, they would have dedicated more time on training the RCs about how to respond to questions about the identifier data collection from both non-Indigenous and Indigenous peoples. Once the identifier was launched, the hospital observed that some staff did not provide accurate information about the purpose of data collection, which had grave consequences: [M]any staff initially did not respond [to questions about the identifier] with the information that we provided. And [RCs] were creating information that was not reflective of the intended purpose, which landed us in hot water. Big hot water. We were doing a lot of back peddling with individual patients who I'm sure were so close to putting in a lawsuit against us because they were given very incorrect information [about how the data would be used] … So it was quite alarming, some of the information that [RCs] were sharing … We had to get senior [management to] deliver the message [to Indigenous partners] that this will not happen again. (Interviewee A)
An Indigenous RC spoke about her experience registering non-Indigenous people, who responded to the identifier with uninformed and sometimes discriminatory responses such as using slurs or falsely claiming to be Indigenous. Unwanted reactions were noted as a potential factor for RCs deciding not to ask clients to self-identify, as a means of avoiding potential discomfort or being exposed to racism themselves. To reduce the spread of misinformation, Hospital 1 implemented training for RCs that included scenario-based exercises to develop confidence in responding to questions about the identifier or potential allegations of ‘racism’. Despite additional training, the data generated revealed that several staff still resisted asking patients if they wanted to self-identify as Indigenous. At the time of our interviews, senior management, in partnership with the Indigenous health office at the site, were working together to create clear processes to shift the attitudes among RCs. They also explored the potential to take disciplinary measure against staff who were routinely refusing to ask about self-identification.
Indigenous data governance in non-indigenous organizations
Prior to the implementation of the identifier, the health care sites worked with local Indigenous communities and organizations to identify interest in the data and priorities of how the data could be used. The next consideration was how Indigenous data would be used by the health care system. For all the sites, sharing the aggregate level non-identifiable health care utilization data with local Indigenous communities was imperative, as well as restricting external non-Indigenous researchers access to the datasets without patients’ explicit knowledge and consent.
One of the sites noted that their health care organization would never publish reports using the Indigenous administrative data, in accordance with their commitment to Indigenous data sovereignty: When First Nations ask for their data, we give it to them. If [an Indigenous leader] or other [First Nations] representatives we worked with asked for data, we'll give it to them. Doesn't happen too often, but you're not going to see a whole bunch of reports from [the Health Authority] with Aboriginal data that's publicized. (Interviewee I)
The refusal to publish Indigenous health care data without explicit consent and participation from the Indigenous community is a key consideration for compliance with the First Nations Information Governance Centre’s Ownership, Control, Access and Possession (OCAP®) principles.
21
Another key consideration made among the sites with respect to OCAP® was to restrict researcher and non-Indigenous organizations access and use of the data collected. One of the interviewees shared a recent experience of another health care organization asking to use the First Nations health care data that was collected at the site she worked at: [A health care organization] asked about tapping into our data. And I said I think this is a conversation we need to have with the First Nations. It is their data. It's their local data here. I mean, to me, [our hospital] is housing it, but we don't own it. To me, it’s those OCAP® principles, right? … So, I just said I can tell you what stuff we collect, but actually sharing it, I think we need to sit with the First Nations. (Interviewee E)
Navigating data governance in this context is not always straightforward. At the time of interviews, the three hospital sites did not have formal legal agreements with the surrounding Indigenous communities or Indigenous health organizations. In 2009, the Health Authority site and one of the local First Nations created a Letter of Understanding (LOU). The LOU is not legally binding but was used to outline the roles and responsibilities and how the two parties could work together for service and program planning. Since the first LOU, other First Nations have also created LOUs with the Health Authority, all of which look somewhat different depending on the needs and desires of each Nation. The two participants from the Health Authority spoke of the ongoing relational efforts to establish data governance structures with the needs of each of the surrounding communities, which has delayed some of their work while they attempt to work out how such governance models can work in practice: The missing link in all this is, we don't have a good data governance framework, right? So that's our next step in the pandemic and opioid overdose [crisis] … [Data governance] is a pressing community priority that Aboriginal partners have. (Interviewee H)
Another participant spoke to the complexity of deciding how to move forward with formalizing Indigenous data governance within health care systems: Where we're looking to head is, what does [data governance] look like? Is it kind of a regional thing that, you know, there's multiple kind of signatories, for example, to a data sharing agreement? Or, is it with each Nation, and then we negotiate how and when we share data with each Nation? So really in infancy, and probably with the next kind of 5 to 10 years, we'll really play out those pieces. (Interviewee G)
Enhanced health care services, planning, and delivery
The key stakeholders at all of the sites reported that the identifier enhanced the health care, social and cultural services available for Indigenous peoples while accessing health care services. For example, in hospital settings, Indigenous patient navigators could identify and support Indigenous patients easier. Indigenous patient navigators are staff at the heath care organization who provide various supports to Indigenous people accessing health care services, including support to identify relevant social services, connection to Elders or Knowledge Keepers, and patient advocacy. Prior to the implementation of the identifier, Indigenous patient navigators would rely on referral, which required patients or hospital staff to be knowledgeable that Indigenous services existed, by personal relationship (i.e. someone from the community was aware of the Indigenous services to make a referral), or by reviewing hospital records to see if they recognized any common Indigenous last names. One RC elaborated on the benefit of the identifier: I think that the Indigenous patients have really benefited because [an Indigenous patient navigator] can now go see them in the hospital to offer them the services and the healing that they need, and their cultural needs can be met. I know that there’s other purposes, as far as identifying the Indigenous community that we deal with in our areas and whatnot. But I think as far as gaining trust with Indigenous patients, it’s been beneficial. Because they know that they’re actually being thought of, that we have a program for them, … that things are changing, they see that change. (Interviewee F)
An Indigenous patient navigator spoke about how, prior to the identifier being established, it was difficult to discover that Indigenous patients were at her organization: How do I know when an Indigenous patient is here? How do I connect to them? So that was the big gap … I know a lot of folks and I would get community that would reach out to me, but, still, that's not capturing everybody that comes through the door. So, we had to sit down and say, how am I going to know if [an Indigenous person] is here? How are they going to know about me? (Interviewee E)
One concern among the study RAC was that disclosing Indigenous identity could result in the individual experiencing racism if the information is visible on their EMR. From the perspective of the interview participants, the identifier had not resulted in any reports of racism. The participants understood that Indigenous peoples experienced racism in health care settings and attempted to mitigate this in several ways. Two of the sites ensured that once the identifier was recorded in the EMR, the information was only available to be accessed by the Indigenous patient navigators. Two Indigenous patient navigators at different sites explained this decision: [The identifier] doesn’t pop up on anybody’s chart … [because the Indigenous] community told us, ‘Don’t do that. If social work is not working with that patient; they don't need to know. If physiotherapy isn’t working with them - we just didn’t want [an Indigenous identifier] flashed out on the record.’ (Interviewee E) [The identifier] is not there and that’s very intentional because that was the feedback we got ... They didn’t want the nurse, and I’m going to pick on the Emergency Department, to pull up your name and see instantly that they were Indigenous, because of the concern that [the client] would be treated differently. (Interviewee A)
By contrast, at another site the identifier information was available to everyone on the care team because the information could influence health care decisions, such as referrals to Indigenous specific health care services. Another safeguard put in place at one of the hospitals was that the identifier would not be asked every time someone checked into the hospital. Once the response had been entered into the EMR, the question would not be asked again. At another site, clientele was asked every 3 years if they wanted to self-identify as Indigenous, in case the person wanted to change their response to the identifier. One of the sites provided the option for people to self-identify on an online portal to eliminate the need to self-disclose at registration entirely.
The Indigenous identifier was used by all the sites to guide decision making about health care services for Indigenous peoples. The data provided concrete evidence to health care executives to allocate funding to specific initiatives tailored to Indigenous health care needs. One of the Indigenous patient navigators spoke about how they used the data to improve Indigenous specific services: Now we have a more true look, the true data of the people that are flowing through here. And it's been really helpful. I use that data for service delivery and making improvements. I can look at - when we're able to pull data from the Emergency Department: ‘Hey, I got 200 Indigenous people that come through our [Emergency Department] and we're not even helping those people. How do we start working so that we can start supporting them?’ So, it is helpful to look at improving services or programs. (Interviewee E)
One of the senior leaders interviewed at the Health Authority shared a similar sentiment: [The data] has been really helpful in planning services where there’s maybe a higher access of a certain service. Or noticing patterns of use of health care services, patterns of non-use of health care services and why that might be, identifying spaces in places where cultural safety and racism might be a factor in the health care services being provided. (Interviewee G)
This quote highlights that beyond identifying need, the data could in fact be used as a tool to identify racism within the health care system, which could then be monitored and targeted by health care leadership. One of the participants shared that the data collected was shared with Indigenous health care organizations to improve their services as well: One of our commitments in there is to provide [the data] to Indigenous organizations who have a health mandate, to inform their programs, prevention programs, treatment or whatever it might be right. We will give them the data relevant to their catchment area if they ask, where it’s possible without identifiers for individual patients. (Interviewee A)
Discussion
Overall, Indigenous identifiers in Canadian EMRs remains relatively rare.3,4 But Indigenous researchers and organizations have argued that Indigenous identifiers in administrative data are necessary for improving the available Indigenous health data and in turn health outcomes.20,21 Moreover, improved health care data is necessary for advancing Indigenous sovereignty and self-determination. 22
Just as Indigenous peoples are not monolithic, the approach to implementing an Indigenous identifier in health care settings will not be uniform. The interviewees noted that moving forward with the proposed Indigenous identifier required strong relationships and trust to be developed between the health care system and the local Indigenous communities.
Given the high proportion of Indigenous peoples who report facing racism and discrimination within health care, many Indigenous clients have apprehensions towards health care providers.11,12 Another study examining the acceptability of asking about Indigenous identity in health care settings among patients found participants worried about the misuse of information and expressed concern about privacy. 22 Our interview participants identified several actions that could help build trust including meaningful and ongoing inclusion of Indigenous communities in the development of the identifier (for example, the language used to ask people if they wish to self-identify as Indigenous) and creating data-sharing agreements with local Indigenous communities and organizations. Other actions included educational campaigns for Indigenous communities that will help them understand why they are being asked to self-identify and how the data will be used.
The RCs’ discomfort asking patients to self-identify as Indigenous was a major barrier to implementation at two of the sites. The staff reluctance and sometimes refusal to collect the identifier hindered the collection of the data and may have resulted in Indigenous patients not receiving access to Indigenous specific services. This finding aligns with international studies where an identifier has been implemented that found that Indigenous peoples were often under-identified in health care settings with one of the primary reasons being that health care staff did not systematically collect Indigenous identity data.21–26 One of the major barriers to routine Indigenous identity data collection was entrenched attitudes among staff about the identifier due to a lack of knowledge about why the identifier was being collected.25,26 Another significant barrier is the RCs’ refusal to ask about identity due to discrimination from non-Indigenous people. This issue is particularly poignant when the RC is also Indigenous, making the essential task of accurately recoding demographic information more challenging and emotionally taxing. It comes at a tremendous cost to Indigenous RCs, as they are placed in a position that makes them vulnerable to experiences of racism.
For quality data, health care staff need to be aware of the value of the Indigenous identifier for Indigenous patients and for health care service planning. Such training must also be situated within a larger historical context of colonialism. This aligns with The Truth and Reconciliation Commission of Canada’s Calls to Action for Canadian health care systems to enhance cultural competency training for health professionals. 2 Ensuring cultural safety and security in health care settings is crucial because if an Indigenous person perceives that the setting is unsafe, it is unlikely that they will choose to self-disclose. 27
Indigenous data governance is a paramount consideration for advancing Indigenous identity data collection. 28 The debate over how health care systems can incorporate Indigenous-led data governance models into their practice is still in its early stages in Canada. Globally, there have been significant developments in Indigenous data sovereignty and governance.22,29,30 While all the sites acknowledged the need for Indigenous data governance, how Indigenous data governance principles could be embedded into formal legal agreements between the organization and the surrounding Indigenous communities was still being developed at the four sites. The shift in data ownership is a significant departure from the status quo because, for the most part, large administrative datasets are governed and controlled by public institutions with little or no engagement with Indigenous communities about what purposes such data may serve and what accountabilities to affected communities may exist. 3 Legally binding agreements between health care organizations and local Indigenous communities would ensure that Indigenous peoples can access data that pertains to them, can expect accurate data, and can contribute to the strengthening of data collection, analysis, and interpretation, while also restricting unauthorized use of their data by researchers and organizations. 29 Indigenous nations and peoples have an inherent right to self-determination and governance, which includes a right to jurisdiction over information management and research.22–29
Limitations
There are two main limitations to this study. First, the interviews were limited to those working within the health care system. Future research should examine the perspectives of Indigenous peoples about being asked to self-identify in health care settings.
Second, the insights derived from this study stem from a limited number of health care professionals, and therefore may not be representative of other organizations experiences in implementing an Indigenous identifier. This is because we were only able to approach sites that have publicly announced that they use an Indigenous identifier. While there may be other sites in Canada that are collecting Indigenous identity data, the four included here are the only ones we were aware of.
Conclusions
There is a demonstrated need for improving health outcomes for Indigenous people across Canada. One potential method is the introduction of an Indigenous identifier to tailor services to Indigenous patients to enhance access to Indigenous-specific services as well as improve Indigenous health data. The ongoing consequences of colonialism and general distrust of health care systems among Indigenous peoples mean that health care systems must approach the collection of Indigenous identity with special consideration. Any Indigenous identity data collection must go beyond partnership with Indigenous peoples and be led by Indigenous peoples in terms of design, analysis and data governance.
Footnotes
Acknowledgments
We would like to thank the interview participants for their time and expertise. We would also like to thank Gary Teare (Alberta Health Services) for his role as an advisor on this project and Marty Landrie (Alberta Health Services) for assistance with participant recruitment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Canadian Institute for Health Research and Alberta Health Services, through the CIHR Health System Impact Fellowship.