
Abstract
Objectives
Networks (multiple organizations or actors coordinating their activities towards a common goal) have been promoted in the cancer programs of a number of countries. But there is little empirical evidence on whether and how they overcome the siloed functioning endemic in specialized domains. This study examines how collaborative governance takes shape to support integrated network-based practices within a prescribed national cancer program.
Methods
A longitudinal qualitative single-case study was conducted of the Quebec cancer network in Canada. Data were collected in 2018-2020 through semi-structured interviews with stakeholders (n = 37) involved in regional and/or national cancer network structures and a review of documents (n = 45) generated at national and regional level. Abductive thematic analysis during and post-field work was based on Emerson’s collaborative governance framework. It aimed to identify how collaborative governance mechanisms (principled engagement, shared motivation and capacity for joint action) were activated in the network, and their contribution to translating a national cancer program into network-based practices at the point of care.
Results
Principled engagement was driven through interdisciplinary committees at national and regional level, communities of practice and trajectory-development efforts. These mandated structures supported knowledge exchange and contributed to the recognition of interdependencies, distribution of leadership and development of mutual understanding and trust. Shared motivation benefitted from a vision of patient-centred care but was hindered by top-down communication vehicles that did not allow regional priorities to filter upwards to central level. Between care providers in different settings, trust and candidacy were identified as mechanisms important to shared motivation, though network actions did not sufficiently support trust across care settings, or even between members of the same profession. Candidacy issues hindered family physician participation in cancer network structures that mirrored ongoing difficulties to including them in cancer care practice. Institutional arrangements were important drivers of capacity for joint action in the network. Common indicators were recognized as important to generating efforts towards common goals; however, questions around their validity reduced their contribution to capacities for joint action.
Conclusions
Despite favorable starting conditions from the national cancer program and its central leadership promoting collaborative governance, tensions that emerge through the pursuit of network integration limit the transition to a more collaborative practice. Taking the time to work out these tensions as integration proceeds in waves appears essential to arrive at a governance model that is appropriate and acceptable for all network members.
Introduction
Health care systems are struggling to provide quality cancer care in the face of growing demand, greater complexity, and the siloed functioning of specialized teams. 1 Recognizing and managing interdisciplinary work within and between teams is especially challenging in the cancer context, which is distinguished by professional autonomy based on expertise, the uniqueness and trajectory of each patient and the bounded rationality of decision-makers.2,3
As a result, people living with and beyond cancer (PLWBC) still get ‘lost in transition’ 4 (p. 1) despite efforts over some 20 years to address the gaps arising from cancer care fragmentation.
A number of cancer care systems are looking to integrated network-based practices as a means of supporting smooth and effective transitions between providers and care settings, from specialized centres to follow-up in the community to self-management at home.5,6 Networks, defined as multiple organizations or actors that coordinate their activities towards a common goal, are seen as organizational models for enhancing the dissemination of best practices, enabling rapid learning and improving proximal coordination between providers while also keeping up with rapid advances in highly specialized technologies and treatments. To produce tangible benefits in people’s experience of care, network coordination must reach into multiple levels of person-centred practices to develop proximity within and between teams and organizations, cultivate different dimensions of integration (e.g. professional, clinical, organizational, normative), 3 carefully navigate patient’s needs and preferences4,6 and manage political and managerial demands. 7
Research evaluating clinical network efforts reveals benefits, but also unanticipated or unwanted outcomes. For instance, formalizing roles in a network can weaken informal ties, 8 clinical expertise can be diluted, and the considerable costs of establishing networks may not bring tangible benefits. 5 These occur partly because networks are developed and prescribed at macro government level but are operationalized at micro clinical level, where professionals have a central role in transforming the provision of care and have the power to openly or passively resist top-down changes.5,7 Network transformation to fundamentally shift multi-level behaviours towards coordinated care across the cancer continuum requires inputs into network governance from the full range of stakeholders, including health care professionals, patients and caregivers, policymakers, managers, and non-profit community organizations. Alongside these efforts, competing needs that frame network activity can affect ‘sharing capacities’ which is the most prominent characteristic of collaborative governance. 9 (p. 1195)
Networks can be mandated and governed by a more or less agile lead organization or be more informal with distributed governance, and the governance model influences a network’s inclusiveness, legitimacy, flexibility and stability. 10 The governance model also influences the ability of network coordination to reach across macro, meso and micro levels. Collaborative governance appears as a means of aligning a wide variety of actors on a vision of network functioning based on collaboration, deliberative approaches and trust. 11 While network governance focuses on structures, collaborative governance appears as a process concept, focused on ‘how a diverse set of actors engage in collaboration in order to govern a particular problem field.’ 9 (p. 1188)
In cancer care, experience internationally and in Canadian provinces3,10,12 shows that structural levers are necessary, but not sufficient to optimize coordinated care for people living with and beyond cancer in an enduring way. Romiti and colleagues consider that, in cancer networks, formal arrangements may be better at influencing organizations but must be accompanied by informal mechanisms if they want to influence professionals. 10 As well, cancer care often involves a ‘network of networks’10(p. 9) that must contend with regional particularities and sub-regional dynamics while driving overall (national or provincial) network coordination. Understanding how collaborative governance emerges and takes shape over time to increase capacity for integrated care in this challenging context is the research question that guides this study of the cancer network in the province of Quebec in Canada. 13
Collaborative governance and networks
Emerson et al. define collaborative governance as arrangements that intentionally involve multiple stakeholders.
11
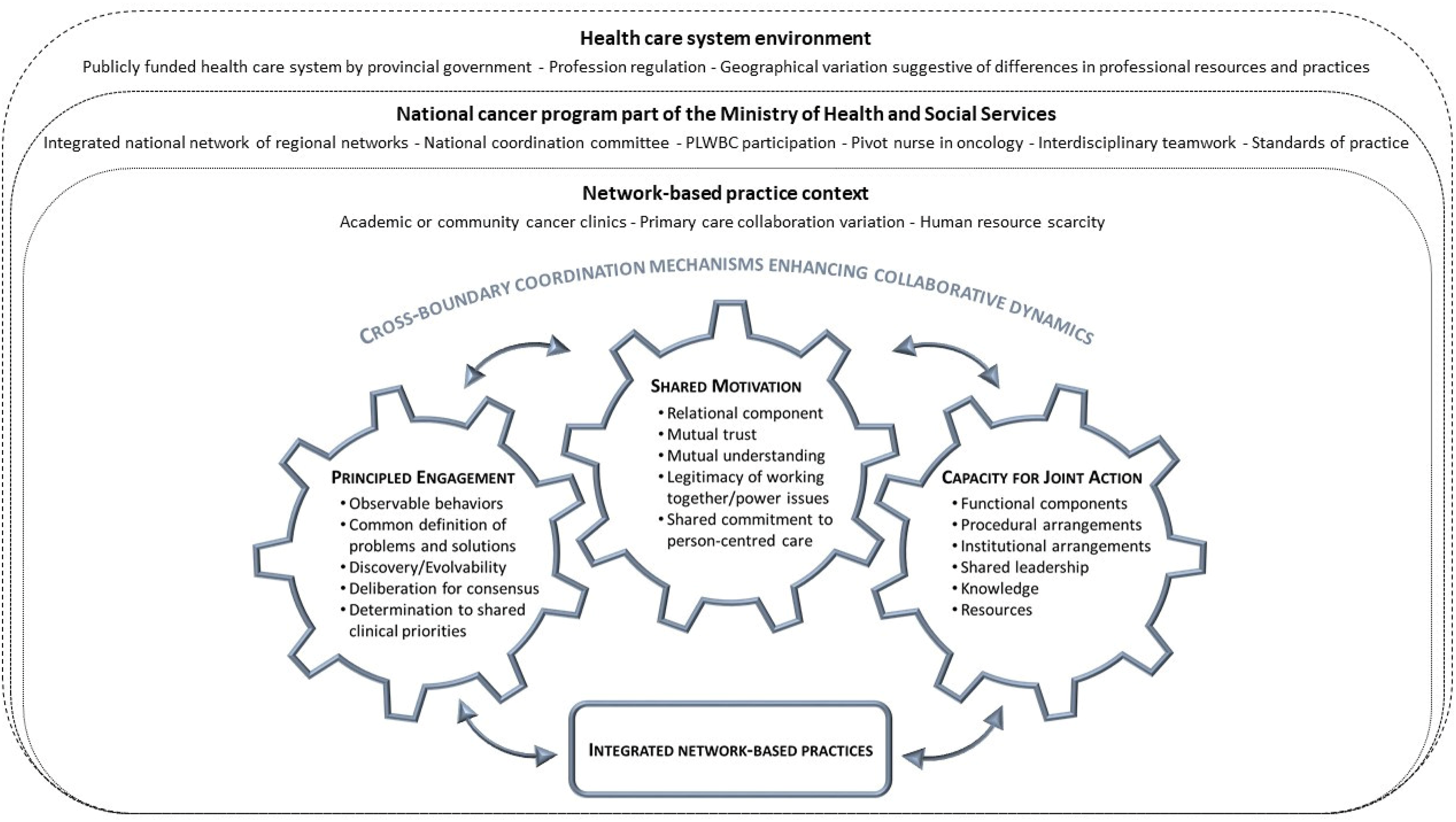
They explore ideas for improving policy execution and program implementation through collaboration between upstream and downstream actors in both policy design and a form of adaptive policy implementation. Their framework identifies starting conditions of ‘multipartner governance’11(p. 3) and collaborative processes nourished by facilitative leadership and institutional design to enhance collaborative practices (Figure 1).
7
Emerson et al. describe collaborative governance as an overarching mechanism driven by three underlying mechanisms that interact to affect interactions and decision-making, which in turn may support or impede cross-boundary collaboration: principled engagement, shared motivation, and capacity for joint action.
11
Analytical approach to collaborative governance in cancer networks, adapted from Emerson.
11
Translating collaborative governance into network-based practice
There has been considerable work on collaborative governance since Emerson’s framework was first conceived. Common elements include ‘a network of partners that represent diverse interests’, ‘the authority and autonomy to decide and to act - in other words to govern’, and a ‘demand-driven’ ‘problem-driven’ approach.14(p. 500) Little research is yet available on how collaborative governance is driven and takes shape in specialized networks - such as cancer care - nor on factors that influence governance dynamics over time. 15
The Quebec cancer network provides an opportunity to explore these questions.
Single-case description
The province of Quebec in Canada has a publicly funded cancer system in which physicians work largely on a fee-for-service basis. In 1998, the Ministry of Health and Social Services sought to induce integration of cancer care within a national network. It initiated a national program to improve coordination of cancer care across the province and adapt services to the needs of populations in different regions. The program was based on a number of key concepts: an integrated network, a ‘pivot nurse’ playing a coordination role within interdisciplinary cancer teams, and a whole-person approach. 2 Interregional service corridors were formalized for referrals to specialized cancer care. A cancer directorate within the Ministry mandated and supported various committee structures, and projected a vision of patient-centred care across the cancer trajectory.
This empirical study of the Quebec cancer network aims to find out how mechanisms of collaborative governance are activated to support integrated practices across the cancer continuum and understand factors that contribute to transformative capacity over time. It focuses on deliberate actions to activate mechanisms within the network and factors that influence the persistence of these mechanisms in driving collaborative governance efforts. Mechanisms are underlying entities, processes, or structures which operate in particular contexts to generate tendencies of interest. 16
Methods
Study design
A longitudinal qualitative single-case study design is well suited to a comprehensive examination of a phenomenon in a natural setting from the perspective of those who are directly involved.17–19 A qualitative single-case study meets the authors’ pragmatic objective of understanding a phenomenon in its evolving context and providing knowledge for applied practice in the field to inform decision-making. 20
Data collection and sampling
Characteristics of the key informants (n = 37).
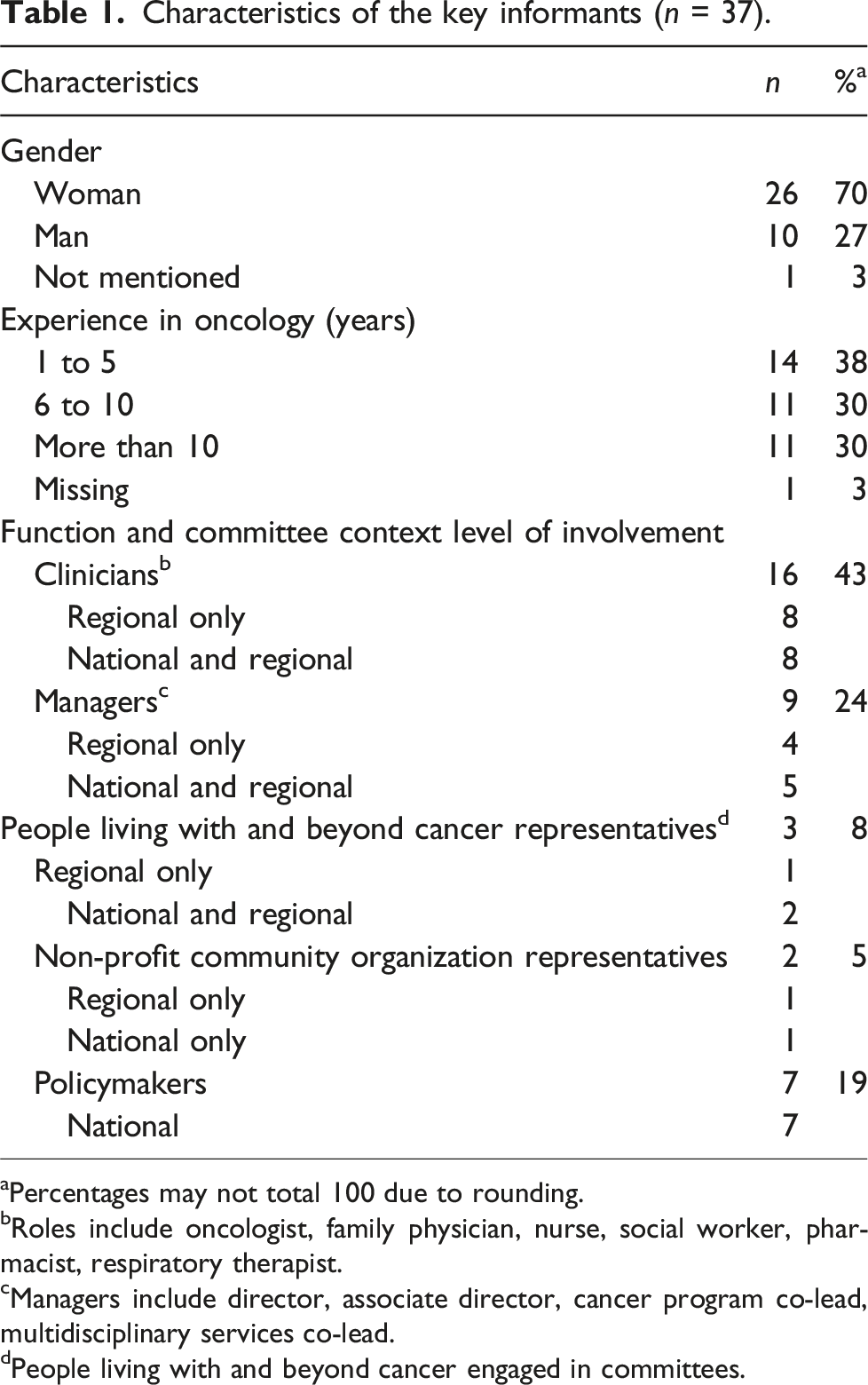
aPercentages may not total 100 due to rounding.
bRoles include oncologist, family physician, nurse, social worker, pharmacist, respiratory therapist.
cManagers include director, associate director, cancer program co-lead, multidisciplinary services co-lead.
dPeople living with and beyond cancer engaged in committees.
Semi-structured interviews with informants active in the network conducted in gathered data on network governance and how mechanisms of cross-boundary collaboration were activated to support network-based practices. Interviews lasted 20 to 60min (mean = 54min) and were transcribed and anonymized. Data were also extracted from 45 documents: 17 open access ministry publications and minutes from 19 regional and nine national committee meetings that were distributed to cancer network members and accessible to the principal investigator. Documents were selected for their relevance to understanding how the context of the Quebec cancer network evolved from the first expression of the ministry’s network intention in 1998, providing a longitudinal perspective. The data collection guide drew on Emerson’s collaborative governance framework (Figure 1), to distinguish manifestations of the three key mechanisms in cancer settings and capture interactions that bridge macro and micro governance levels. Data collection and analysis were conducted iteratively so that the interpretation of data according to the framework was considered in subsequent interviews. 22 Iterative approaches are particularly useful when studying evolving phenomena such as mechanisms in natural context.
Abductive data analysis
Interview transcripts and documents were grouped and managed as a single database in QDA Miner (version 5). 23 To capture recursive patterns from raw data and organize content to generate pragmatic results, abductive thematic analysis involved moving between empirical data and existing theoretical understanding 24 of collaborative governance during and after field work. The analysis included recursive non-linear steps inspired by Braun and Clarke 24 : (1) familiarisation with raw data; (2) organization of raw data using an open-ended coding strategy to identify activation of the three mechanisms of collaborative governance (principled engagement, shared motivation, capacity for joint action) and influential context elements (Figure 1), extracting illustrative quotes; (3) discussion among research team members to compare interpretations of empirical data; and (4) thematic grouping of initial codes that helped explain mechanisms at ministry and regional level and their interaction across levels of the cancer network. The first step was undertaken by two co-authors (DT, SU) and a research professional in several rounds, while the second step deepened the analysis with all co-authors. Steps three and four involved the analytic work to select overarching themes in a way that improved reliability and credibility of the qualitative study. 24 Credibility and reliability criteria were assured by triangulating data sources, drawing on co-authors’ different disciplinary backgrounds (public administration, health service research, cancer nursing research), and their longstanding research experience with integrated cancer care 3 and the collaborative governance framework. 12
Results
Key informants provided a diversity of perspectives on the activation of collaborative governance mechanisms at multiple levels within the cancer network. Results reveal regularities that occur over time in a dynamic way across levels to either facilitate or impede the activation of the three main mechanisms. Illustrative quotes are given below. The online supplement provides a comprehensive table of network features for each of the mechanisms, along with supporting evidence from documents and interviews.
Principled engagement is supported by mandated structures
Principled engagement manifests in observable behaviours at both national and regional level that enhance the ability to adapt program objectives to real world practices. These include efforts to define problems and solutions, discover the potential contributions of actors from different disciplines and settings, and deliberate to achieve consensus and establish priorities. They include committees that serve to communicate overall network objectives and evidence-based practices, along with committees that bring regional multidisciplinary actors together and communities of practice that assemble members of a given profession (or role, i.e. patient partners) from different regions: The national level seeks to play a ‘coach and connector’ role, encouraging regional actors to talk to each other about particular issues they face, opening lines of communication. (Policymaker)
Interactions within these structures lay the groundwork for achieving a common understanding of problems, determining objectives and deliberating on each other’s potential contribution to achieving them. Committee meetings at regional level enable actors from different disciplines to find out about one another’s efforts and preoccupations and, over time, develop understanding and trust: I’ll find myself with an oncology specialist, a nurse, a patient and the information technology guy. It’s very mixed and that makes committee meetings interesting and allows the concerns and knowledge of each party to be taken into consideration. (Oncologist, regional and national committees)
Various factors appear to speed, slow or interrupt the evolution of principled engagement in the network, including changes in regional leaders that weaken connections and teamwork. A number of informants highlighted that the departure of key professional leaders in the network’s evolution created insecurity. The risk of reverting to top-down leadership, from central to regional level, and within the regional level, is ever-present and palpable among network actors. We are aware that it [shared leadership] rested mainly on one person … When the original pillars left, we wondered if we would be able to reproduce some kind of leadership to sustain the vision. (Manager, cancer program co-lead, regional and national committees)
These mandated network structures provide opportunities to recognize interdependencies and activate and sustain the mechanism of principled engagement. However, the effect is limited to actors who participate in the venues where such opportunities are created. Regional network committees are effective at bringing together a range of professionals and PLWBC. But primary care and non-profit community services providers are largely absent, jeopardizing the capacity for joint action in a broad integrated cancer network that would align with the national cancer program objective. As one participant said about forging links with community organizations: We haven’t even touched on that yet, despite it being on our work plan for two years. (Nurse, primary care provider, regional committee)
As a result, awareness of the contributions of primary and community care providers remains low, and hospital staff very rarely refer PLWBC to primary care providers for services such as psychosocial help.
The development of treatment trajectories by tumour site, promoted by central network leaders at government level, generates principled engagement at the regional level and increases mutual knowledge. It highlights ways of recognizing interdependencies between providers across care settings and between providers and PLWBC, and was seen as enabling a real breakthrough in bringing people together: Work on the continuum enabled people to get to know each other’s contributions, identify gaps and prioritize action around them. (Oncologist, cancer program co-lead, regional and national committees)
However, informants also saw a risk that working on trajectories for specific tumour types might create new silos of super specialized teams even as it increases collaboration among actors from different care settings.
Shared motivation remains difficult to achieve across network levels and care settings
Interviewees described a form of inherent shared motivation among people who choose to work in cancer care. Shared motivation is driven by a patient-centred vision of cancer care, promulgated by central network leadership and embodied by PLWBC participation in committees at regional and national level:
In the national committee, the PLWBC seem to have influence when they raise an issue. There are presentations about what is done elsewhere and how it could be implemented in our settings. (Manager, cancer program co-lead, regional and national committees)
However, the manner in which central network leadership communicates with regional network actors impedes the development of shared motivation across levels. Informants at both regional and national level described national committee meetings as primarily a means of communicating central directives. The fact that these meetings are held by teleconference emphasized this top-down dynamic, providing little or no opportunity for exchange with or among regional actors: The national coordinating committee sometimes feels more like a pipeline for transmitting directives than a network. (Policymaker)
The perception of the national committee as a forum where the central level prescribes and judges and leaves no room for upward communication of regional concerns, leads to mistrust and impedes mutual understanding: Ministerial directives are often issued without taking our realities into account … We need to see what’s acceptable at a clinical level, in real life. (Nurse, primary care provider, regional committee)
But regional actors did also express appreciation for the strong central leadership function. In part, this was because it was seen to help promote the status of cancer care within the health system overall and within each of their organizations. The legitimacy and clout of central leadership within the Ministry of Health and Social Services, and its constancy over time, reduces resistance to prescriptions from above: I don’t see it as a problem to have things come from the top, from the cancer care experts in the Cancer Care Directorate. I have no problem with taking what is prescribed and adopting that locally. I trust the prescription. (Manager, multidisciplinary services co-lead, regional committee)
Discrepancies between national program expectations for regional levels and actions at the central level weaken the legitimacy required for shared motivation and may contribute to variations between regions to pursue network objectives. For example, regional committees are expected to include PLWBC, which some do enthusiastically, ensuring they have a point on the agenda of each meeting, while others engage PLWBC on a pro forma basis, benefitting less from their experiential insights. This might reflect wavering commitment to the principle of PLWBC engagement at central level, where some still express concerns around ‘the ability of PLWBC representatives to represent collective rather than individual interests’ (Policymaker).
Shared motivation is also less evident between actors in different care setting within regions. It is sometimes hindered by persistent mistrust, even between members of a same profession practicing in hospital versus community settings. A number of participants reported that cancer team members lack confidence in the ability of primary and community care providers to contribute to the care and follow-up of PLWBC. Trust does not extend to providers outside the hospital: Physiotherapists will keep patients in hospital longer because they don’t know how physiotherapy will be provided in home care. They feel responsible for patient well-being. (Manager, multidisciplinary services co-lead, regional committee)
The mistrust has an impact on referrals and on communication between oncologists and family physicians that would otherwise encourage joint follow-up. It also affects the willingness of non-profit community organizations to invest time in network committees led by hospital actors: [Community organizations] always start off with a certain mistrust of the CISSS [regional Integrated Health and Social Services Centre] and its structures, then come to the table, but then most often hit a wall and retreat to their corner ... The CISSS make too many promises they don’t keep. (Director, community organization representative)
Shared motivation is compromised when regional actors see collaborative structures being used as one-way communication vehicles without enabling regional priorities to filter upwards to central level.
Capacity for joint action is enhanced by mandated structures and projects
This mechanism involves procedural and institutional arrangements and structures that create opportunities to build relationships among actors (committees, communities of practice). It includes the use of shared knowledge resources - such as ministry-prescribed indicators - that orient various actions towards a common objective, enable learning and making actors accountable for achieving targets. All hospitals with cancer clinics are required to have a functional and operational coordinating committee in cancer care, which includes the director, clinical-administrative co-manager and the medical co-manager of each establishment’s cancer program. Each committee monitors the action plan, evaluates performance on indicators and reports annually to the cancer directorate. The national committee highlights promising practices seen in certain regions and encourages their diffusion. For instance, information was relayed from the national committee to communities of practice about one hospital using radioactive beads instead of harpoons for radiotherapy in breast cancer. A clinical leader described the opportunities for joint action that arose due to the promulgation of that information: We looked to see if we could do the same. We consulted evidence-based guidelines from the National Institute for Excellence in Health and Social Services. Finally, we were able to start treating patients in this way. (Manager, regional and national committees)
Information relayed through communities of practice also supports joint decision-making between regions to deal with unanticipated situations, such as shortages of a particular drug. As one participant noted: The [community of practice] is where we see what it means to work in a network, allows us to keep learning, to develop a sense of belonging that I see as a form of resilience ... Being able to share and belong makes us more engaged in our work ... and better able to accompany people with cancer. (Social worker, regional committee)
Knowledge resources - such as indicators (e.g. intervals in the cancer diagnostic and treatment journey, percentage of participants in clinical research, length of stay after surgery, percentage of reference to primary care) - are seen as important in inculcating a culture of measurement and generating efforts toward common goals. However, the validity of indicators is questioned, particularly when they fail to reflect the interdependencies involved in achieving results and bring together data from across care sites:
Recognizing this problem, the Ministry of Health and Social Services provides targeted funding to enable the integration of local cancer registries and inter-establishment information sharing. (Manager, cancer program co-lead, regional committee)
Informants said that specific projects, such as the design of tumour-type trajectories and the planning of a new cancer centre, drive capacity for joint action, at least temporarily. The projects create new procedural arrangements and assembling knowledge about available resources, including community resources: The many meetings held to get the centre going, including people beyond the centre, created proximity. Those meetings helped identify allies who can be called upon to help solve problems later. (Oncologist, cancer program co-lead, regional and national committees)
However, the divide between specialized cancer teams and community-based providers remains wide: There’s a multitude of community resources and we know they’re there. But we don’t know when or how to use them, we don’t have their contacts. (Oncologist, cancer program co-lead, regional and national committees)
Discussion
To the best of our knowledge, this study is the first to use the lens of collaborative governance to explore network-based practices in cancer care. Our findings contribute to understanding how the mechanisms of collaborative governance are activated to varying degrees within a cancer network to support integrated network-based practices. They add to previous research focusing on structure, pointing to measures that support relational dynamics, along with insights into factors that limit the potential impact of collaborative governance.
Recent work on collaborative governance recognizes that it ‘complements, rather than supplants, existing policy structures,’14(p501) emphasizing the importance of bridging the macro/micro divide in which collaborative governance operates. This appears relevant to the cancer context, where objectives and orientations prescribed top-down by central authorities remain distant from care and services delivery. Our findings support the synergies of formal structures and informal relational drivers of coordination, integrating real-world clinical perspectives and patient experience 25 in activating collaborative regimes. Our results suggest a need to balance the flexibility to collaborate across multiple loci of decision-making (from specialized cancer teams to primary care providers and patient self-management) with the stability needed to prevent risks to the quality and safety of care.
The activation of collaborative governance via national coordination and communities of practice in the Quebec cancer network reflects central efforts to steer network-based practices through rules and processes of centralisation/decentralisation, with the ultimate goal of shaping and directing particular forms of network governance.
Some authors refer to this as meta-governance. 26 Meta-governance is an approach for central institutions to enhance resource mobilization and the capabilities of heterogeneous actors that recognizes the complementarity between hierarchical and collaborative arrangements. Ansell and Gash find that ‘collaborative platforms’26(p. 16) of meta-governance can function as relatively stable overarching governance mechanisms for a multitude of local collaborative activities while also allowing for self-organization within these activities. Involving care providers and service users in the co-development of network governance is key to cultivating broad-based ownership of an overall strategy and preventing counter-currents from steering activities off course. Governance that is able to adapt and innovate requires both institutions that ‘foster inclusive deliberation, knowledge sharing and joint learning’27(p. 36) and institutions that balance centralization and distributed leadership. 27
Joint action across levels remains emergent in the Quebec cancer network, with central prescription exerting both positive and negative impacts on the likelihood of activating principled engagement, shared motivation, and capacity for joint action. On the one hand, mandated structures provide venues that enable the activation of these mechanisms; on the other hand, top-down communication of orientations hinders trust and engagement across network levels. The combination of communities of practice (i.e. pharmacists, oncology nurses), where good practices are shared among regional actors, and multidisciplinary committees at regional and national level, where professionals become aware of interdependencies, appears promising to maintain specialization while also cultivating interprofessional and cross-level coordination. The combination appears helpful in accepting that health care specialization coexists with coordination and collaboration, 28 and escape silo functioning. Linking agents play crucial roles here; however, dependency on individuals to maintain trust makes this fragile. Like Vindrola et al., 29 who studied a network of cancer surgical services in the UK, our findings reveal that constancy in leadership is important, that leaders at different levels in the network play essential roles in orienting work towards a shared patient-centred goal, and that patient participation contributes to minimizing resistance to change. While Vindrola et al. argue for distributed leadership to compensate the absence of a system-wide authority, our results suggest that distributed leadership can also support collaborative practice when there is a strong and agile central body at national level.
To reduce the dependence on individual leaders found in our case, a culture of measurement could provide a more stable and less personalized ‘intermediary’ to ‘connect subsystems’ and ‘intermediate’ between system-level policy and micro-level practice in a network. 18 (pp. 795, 803) However, to be accepted and exert an effect on capacity for joint action, indicators need to reflect the contributions of actors across the cancer network continuum.
Trade-offs between bringing actors together in collaboration and creating (new) zones of exclusivity must be acknowledged, both in prescribed network structures (i.e. committees that have difficulty integrating family physicians and community organizations) and in the specific projects (trajectory design and opening of a new cancer centre) that appear so effective at activating (at least temporarily) collaborative dynamics.
Limitations
The main limitation of our study is that the key informants may not include all stakeholder perspectives. Our analysis achieved redundancy in its sample of interviewees, but not saturation. Thus, not all perspectives and experiences on collaborative governance may have been identified. Patient associations, professional colleges and scientific advisory bodies may have contributed additional insight. Considering the early stage of work on collaborative governance in specialized areas, the full range of perspectives that have an influence is not fully understood.
Conclusion
The stated ambition to extend collaboration on cancer care to community-based care providers remains unfulfilled in the Quebec cancer network. As in many other countries, greater involvement of primary care physicians in cancer care is seen as a way to alleviate pressure on cancer centres and ensure that a person’s broader care needs are covered. Our study reveals persistent invisible walls and deep uncertainties about candidacy to participate in cancer care. The inclusion of primary care in the cancer network is hindered by a lack of confidence from specialized cancer teams in their primary care colleagues, by the lack of initial training in cancer care for family physicians and by the reluctance of some PLWBC to trust non-specialists to detect cancer recurrences. 4 Informational discontinuity is one barrier, but persistent challenges between governance levels over decades, in Quebec and elsewhere, to integrate primary care providers into cancer care 3 should prompt deeper examination of the ambition itself.
Our study focused on deliberate actions that drive the underlying mechanisms of collaborative governance in cancer care. Future research could seek to capture how the network-based practices made possible by collaborative governance contribute to patient and system outcomes.
Supplemental Material
Supplemental Material - The role of collaborative governance in translating national cancer programs into network-based practices: A longitudinal case study in Canada
Supplemental Material for The role of collaborative governance in translating national cancer programs into network-based practices: A longitudinal case study in Canada by Dominique Tremblay, Susan Usher, Karine Bilodeau and Nassera Touati in Journal of Health Services Research & Policy
Footnotes
Acknowledgments
We would like to thank all collaborators and informants from the various local cancer networks and national agencies in Quebec for their commitment and support. We are grateful to our academic partners, namely the Faculty of Medicine and Health Sciences of the Université de Sherbrooke and the Research Chair on improving the effectiveness of care for people living with and beyond cancer, for their valuable institutional support. We thank Mrs. Sylvie Lessard, research professional, for her contribution in editing the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fonds de recherche du Québec – Santé [grant numbers: 27193, 265874].
Ethical statement
Approval from the Research Ethics Board of the Research Centre of the Montérégie-Centre Integrated Health and Social Services Centre was obtained yearly for all study procedures (file number: MP-04-2019-316). Written informed consent, including data confidentiality and security, was obtained from all interview participants.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.