
Abstract
Objectives
This study aimed to explore the policy implementation of non-specific symptom pathways within the English National Health Service.
Methods
A multi-site ethnographic project was conducted in four hospitals that contained non-specific symptom pathways between November 2021 and February 2023. The research involved observation (44 h), interviews (n = 54), patient shadowing, and document review.
Results
The study examined how the policy concept of ‘holistic’ care was understood and put into practice within four non-specific symptom pathways. Several challenges associated with providing holistic care were identified. One key challenge was the conflict between delivering holistic care and meeting timed targets, such as the Faster Diagnosis Standard, due to limited availability of imaging and diagnostic tools. The interpretation of a holistic approach varied among participants, with some acknowledging that the current model did not recognise holistic care beyond cancer exclusion. The findings also revealed a lack of clarity and differing opinions on the boundaries of holistic care, resulting in wide variation in NSS pathway implementation across health care providers. Additionally, holistic investigation of non-specific symptoms in younger patients were seen to pose difficulties due to younger patients’ history of health anxiety or depression, as well as concerns over radiological risk exposure.
Conclusions
The study highlights the complexity of implementing non-specific symptom pathways in light of standardised timed cancer targets and local cancer policies. There is a need for appropriately funded organisational models of care that prioritise holistic care in a timely manner over solely meeting cancer targets. Decision-makers should also consider the role of non-specific symptom pathways within the broader context of chronic disease management, with a particular emphasis on expanding diagnostic capacity.
Introduction
Around half of patients diagnosed with cancer present initially with non-specific or vague symptoms.1,2 However, the diagnostic process can be protracted as symptoms may be linked to different cancers or non-cancer causes, which in turn may lead to delays in diagnosis and treatment. 3 There is also a risk of overdiagnosis and overtreatment for people experiencing these symptoms due to their undifferentiated nature and systemic approaches to diagnosing cancer. 4 Non-specific symptoms include signs such as cough or constipation, as well as non-cancer site specific symptoms such as anaemia, fatigue and weight loss.
Building on the experience in Denmark, 5 the UK has implemented Rapid Diagnostic Centres (RDCs) and Non-Specific Symptom (NSS) pathways to reduce delays in cancer diagnosis and improve outcomes. These are urgent referral services that are located in hospitals equipped to investigate the causes of non-specific symptoms. Emergent evidence points to the impacts of these services on the time to diagnosis interval, with one study on Denmark finding a reduction from a median of 49 to 32 days. 6 Work in Wales showed that a rapid diagnostic clinic reduced the mean time to diagnosis from 84.2 days in usual care to 5.9 days if a diagnosis was made at the clinic; where further investigations were necessary and these were booked during the rapid diagnostic clinic, time to diagnosis was still less than half that in usual care. 7 Shortening the time to diagnosis can potentially improve survival rates at the population level through increased detection at an earlier stage. 8 Shorter diagnostic intervals may also improve patient experience and reduce psychological distress,9,10 although overall there remains a lack of robust evidence for NSS services.
As noted, in the UK, non-specific symptom pathways were developed based on evidence elsewhere, 11 but how to best organise these services is not well understood. 12 People with non-specific symptoms typically present in primary care and are referred to specialist services after a series of tests. 11 Specialist care teams that include internal medicine, 13 radiology, 12 and gastroenterology 14 then offer advanced diagnostic tests such as computer tomography (CT) in a timely and coordinated fashion. National guidance in England further stipulates that NSS pathways take a ‘holistic’ approach to patient needs, provide a ‘tailored pathway of clinically relevant diagnostic tests’ and deliver ‘streamlined support’ in order to support earlier and faster diagnosis. 15 Holistic care typically refers to considerations of physical, emotional, social, economic, and spiritual aspects of health care provision and self-care. 16 However, what ‘holistic’ is meant to convey in the context of NSS pathways is not specified any further 14 nor how well they deliver on these aims. A lack of defining ‘holistic’ may lead to varied interpretations and implementation of the NSS, which may, ultimately, affect patient outcomes. This study explored the implementation of NSS pathways in England, with a particular focus on understandings of holistic diagnostic investigation.
Methods
Study design and setting
This was a multi-site ethnographic project conducted in four National Health Service (NHS) hospitals in the South East of England. An ethnographic approach appeared most suitable to capture every-day health care practice and local values, and to investigate the relationship between individuals and organisations, the policy context, and the complexity of NSS pathways using systems thinking. 17 We used multiple methods of data collection including shadowing patients going through the NSS pathway, observing and shadowing staff working in the services, collecting local documents, and conducting formal semi-structured interviews with a range of professionals with expertise in NSS services (e.g., decision-makers, health care providers) to develop thick descriptions of phenomena in context. 17 Our data collection or ‘field’ encompassed individual elements such as patient characteristics, staff tasks and practices, as well as broader structures such as organisational policies and financial context. 18 Our data collection process was exploratory; the issue of holistic care arose inductively from the interviews, observations and documents that we collected.
Data collection
Data were collected between November 2021 and February 2023. We used in-person and virtual observations (44 h) of patient-facing clinics, staff meetings and desk work at the four sites. Virtual observations were used, largely, during the COVID-19 pandemic, which imposed restrictions on in-person data collection options; they mainly included NSS team meetings. One researcher (GBB) worked with NHS trust staff to understand the different environments that were relevant to the study. Observational data collection ceased by agreement with clinical teams when the researcher had spent some time in each of these environments. We collected a range of documents including policy documents, referral forms, business cases and minutes of meetings; documents were both offered by local staff members and identified through targeted searching of the internet and requests for confidential sharing of documents.
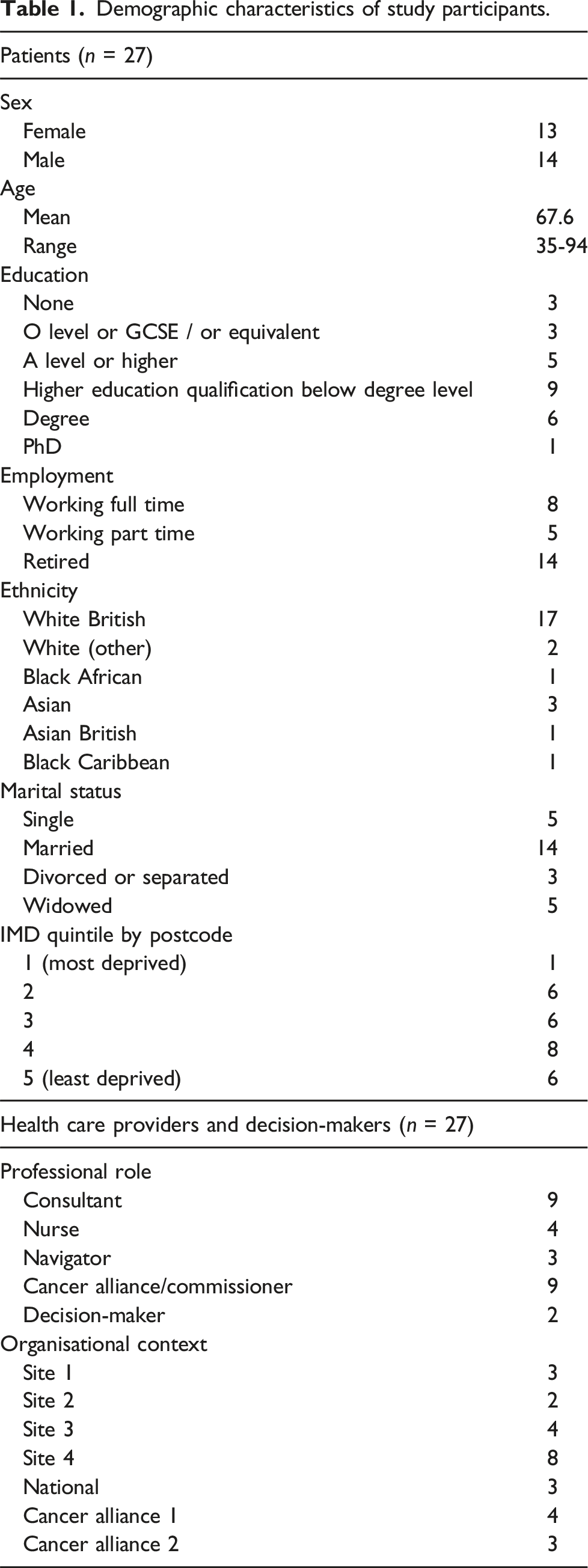
Twenty-seven patients undergoing NSS pathway investigations were recruited for interview from the four sites taking part in the research; they were approached through a clinical intermediary. All patients were eligible who had been accepted onto the NSS pathway; we sampled by quota for gender, age, educational level and ethnicity. Interviews included open-ended biographical questions about their experiences in primary care, referral, clinical contacts, and any other relevant experiences or perspectives. Some patients gave additional consent for patient shadowing: this included accompanying patients to clinic waiting rooms, phlebotomy services, and radiology suites, as well as using brief recorded telephone interviews to relay recent events. These telephone calls did not include a topic guide, but followed an unstructured format after an opening question such as ‘what has been going on since we last spoke?’. These conversations often included the experience of waiting for tests or results, access to and understanding of information, and breakdowns in communication between hospital and primary care. The first author completed the patient interviews and shadowing. Only one participant did not complete a formal interview but participated in shadowing. 12 participants were shadowed and interviewed. 14 participants completed the formal interview only.
Demographic characteristics of study participants.
Analysis
We conducted an iterative analysis underpinned by inductive coding of the entire dataset. The research group met regularly during the fieldwork, developing ideas and explanations as the work progressed. Overall, the iterative coding and analysis process facilitated nuanced understanding of the complex factors influencing patient experience and quality improvement efforts in the context of the health care settings.
We contrasted national and organisational drivers with staff tasks and practices. 18 This highlighted certain issues relating to interpretation of policy documentation, with the most prominent being different views of what the service should provide, and the value of ‘holistic’ care. Our interpretations were informed by our overarching interest in non-specific symptom pathways and the values and ideas associated with them. While patient shadowing and interviews were analysed as part of the whole dataset, the current paper mainly draws on observations, documents and interviews with professionals, which we use as a summary term for health care providers and decision-makers.
Results
We present our findings in three parts. First, we report on how a holistic approach was defined in policy, and how this was interpreted locally. Then we present two challenges to promoting holistic care: (1) meeting cancer targets within NSS pathways and (2) lack of clarity about the boundaries of the NSS. Quotations and observation extracts are given throughout.
Defining a ‘holistic’ approach in policy
Reviewed policy documents and key text relating to non-specific symptom pathways.
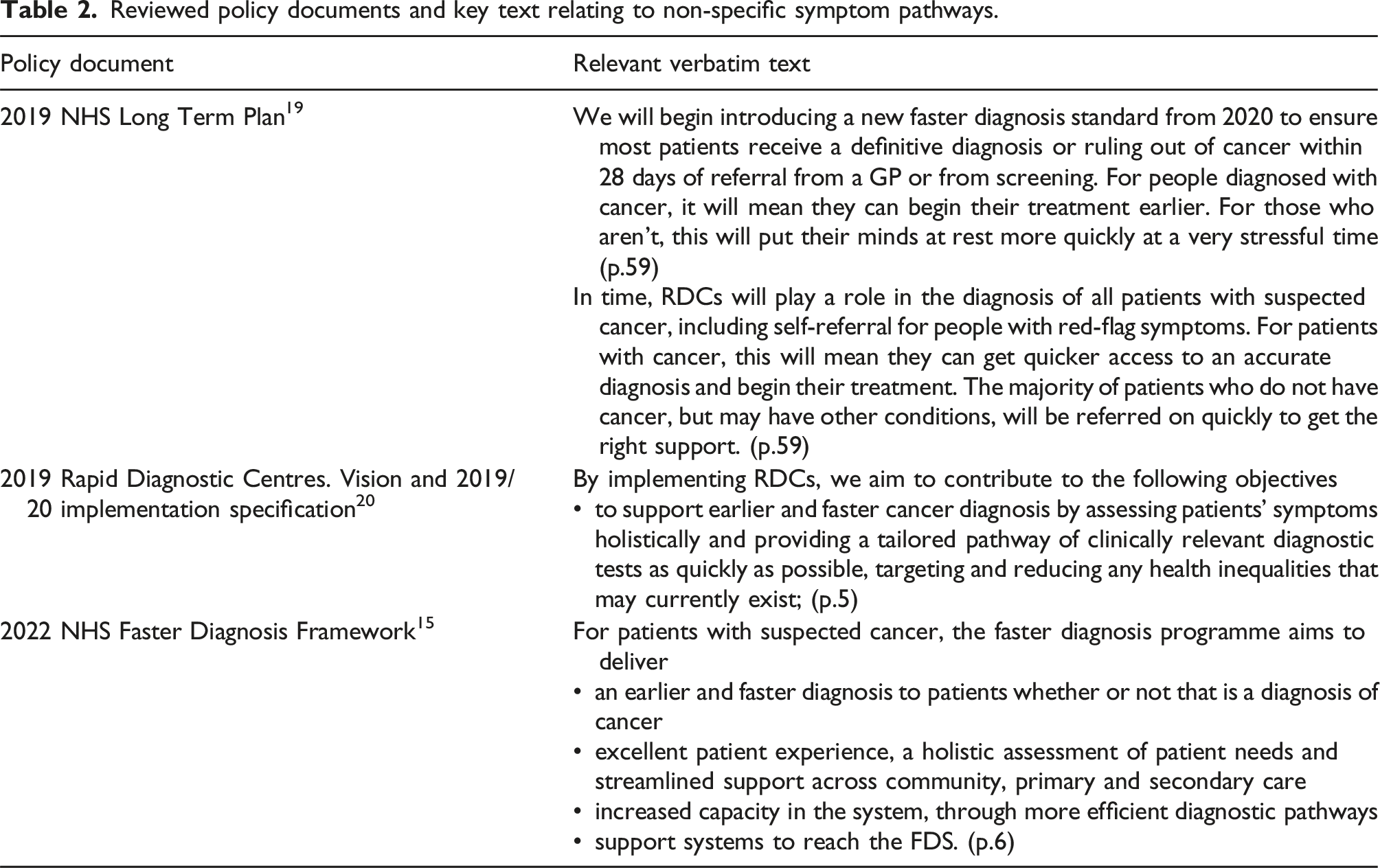
The reviewed policy documents did not specifically define a holistic approach or the underlying evidence for this (if any). The term ‘holistic’ in the context of NSS services was used to describe a broad investigation of patients’ symptoms rather than assess their wider needs, such as emotional, practical (employment, housing) or spiritual. For example, that patients should be referred to the appropriate pathway whether or not cancer was the underlying condition, and that all concerns should be addressed early on in the process and not require multiple referrals to different specialists. 17 Also, initial policy stipulated that patients who were eligible for other urgent suspected cancer referral pathways should not be accepted onto NSS pathways, and this was subsequently specified further, with people with site-specific symptoms who, for example, had specific alarm symptoms warranting referral onto a single site-specific pathway, were too unwell or unable to attend an appointment, were likely to have a non-cancer diagnosis, or who were already being investigated for the same problem elsewhere, to be excluded from the NSS pathway.
Several decision-makers interviewed for this study agreed with these policies, stating that the triage and re-direction functions of NSS pathways were core to their ability to deliver holistic care and avoid inefficient pathways for patients. The really successful NSS pathways are actually able to divert or redirect those patients who, for whom you know a suspected cancer, a specific suspected cancer has been ruled out but where there is potential for another serious pathology to exist into their services and process those patients in the same quick and efficient way. (RDC05, national policy team)
Holistic onward referral described in the Faster Diagnosis Framework included clarity about the remit of the service with respect to non-cancer diagnoses, stating that “an NSS pathway should support patients until they are diagnosed and referred onward or their symptoms resolve”. 15 (p. 15) This document established boundaries at the limits of the NSS pathway, where responsibility for any further radiology, histology or molecular diagnostic testing needed for patients diagnosed with cancer should sit with the specialist team following onward referral.
Interpretations of providing a holistic approach in practice
Participants described their interpretation of a holistic approach to NSS pathways in two ways. First, as a set of intrinsic holistic values, such as the idea of ‘owning the patient’ until a diagnosis was reached. And one of the things that I say is that I just want doctors to be doctors, so like just, if you have got a patient with something and they have raised a clinical concern with you and it’s rang an alarm bell with you, then you should sort out that problem. Don’t shaft it on to another team, don’t shaft it back to the GP. Like pick it up and run with it, the patient is in front of you there, like it takes you five minutes to request a CT scan, if that is what you think needs to happen then do that. Don’t write a letter that takes three weeks to get to the GP that says please refer to scan and the GP is like oh yes sure that’s probably the right thing to do. (RDC16, navigator)
The second interpretation was that NSS pathways should provide investigations and advice beyond ruling out cancer, although views varied. In some sites, participants conceptualised NSS pathways as a filtering mechanism to rule out cancer whereas other sites saw it as their role to investigate a wider range of health care problems once cancer had been excluded. Many participants felt that it was clear that NSS pathways were not just cancer exclusion pathways, but that they had a remit to also provide advice and guidance to GPs. Other participants questioned whether it was right to deploy resources within an urgent pathway to investigate non-progressive or acute conditions, considering that some patients would be more effectively diagnosed in a different setting.
While endorsing a holistic approach, several participants recognised that providing holistic care beyond cancer exclusion was not aligned with the current service funding model; for example, exploring a wider range of diagnoses would require greater resources, with implications for the wider system. I think a big issue for all RDCs [Rapid Diagnostic Centres] or a big question for all RDCs in the future is what is the model of care [...] is there a cancer causing the weight loss, no, back to GP or is it a holistic service [...] But that's going to take more resources than just doing a CT, chest, [abdomen], pelvis and say it’s probably diabetes or depression we need to sort out. [...] I think we have actually been much more holistic than we're funded to be, and I think that's a problem. (RDC12, consultant)
Challenges to promoting holistic care: Meeting cancer targets within non-specific symptom pathways
During the data collection period, NSS pathways began reporting data to meet existing standards and targets applied to other urgent cancer pathways as part of their transition to routine care. This was primarily the Faster Diagnosis Standard target to have cancer ruled out within 28 days from urgent referral, but also other time targets such as the 62 days target from referral to start of cancer treatment. 21 Participants reported that this presented a significant challenge to holistic care, and a change from their reporting requirements in the pilot phase of development.
Operating the NSS pathway in a similar way to other cancer pathways was seen as challenging. This related both to practical difficulties meeting the Faster Diagnosis Standard, and the values driving the service. Increasing standardisation was seen to conflict with the holistic approach of NSS pathways. So a key point of the RDC principles which is very sensible for NSS, is around this kind of upfront holistic diagnosis and triage and the kind of redirection. And then the kind of owning the patient until they’ve got a diagnosis. And that worked well for NSS. What doesn’t work so well is that you’ve got that and then you’ve also got a direction of like very high volume, very kind of standardised protocolised pathways. And like they can sit alongside each other but a pathway can’t do both at the same time. (RDC01, local decision-maker)
Other NSS staff participants noted that the NSS pathway should not be like other cancer pathways, which were perceived to be more like a “factory line” (RDC04, Consultant).
This view was not held by all however, with some participants highlighting that the principle of urgent cancer referral pathways was adequate for NSS pathways, and that NSS should be held to the same high standards as any other pathway. Another aspect of success would be in the quality of the non-specific pathway itself, so does it meet, is it held to the same sort of waiting time standards etc, as any other type of cancer referral is, does it navigate the patient appropriately, do they have a reasonable patient experience, do they get cancer screening or diagnosed in a reasonable timeframe and so on. So, I think the marks of success for a non-specific symptom’s pathway should be aligned with the marks of success for any other kind of pathway. (RDC06, local decision-maker)
Organisational tensions between meeting targets and providing holistic care: imaging and reporting availability
Delivering holistic care and meeting the Faster Diagnosis Standard target was highly dependent on the availability of imaging and endoscopy within the NSS pathway. Different sites used different strategies to accelerate testing such as through protected imaging or endoscopy slots, or using flexible capacity in Trusts with multiple sites. Many patients required multiple diagnostic tests, and these were particularly difficult to move through the pathway at speed. Local radiology capacity also determined services’ ability to deliver the Faster Diagnosis Standard target, with some significant delays in reporting. Views were divided between whether diagnostic tests should be sequential or ordered in parallel. One policy maker suggested or assumed that all tests were booked simultaneously. If you have multiple appointments on the same day you are much, much more likely to, not to breach the cancer waiting time standards. So you know again if you’re, if you’re coming in, you’re getting triaged and they’re saying look we’re going to give you a CT scan and an MRI scan. We’re just going to get it all done. You come in, we’ll do those, like you are expediting the pathway down the line like hugely because you cut out the kind of even if it’s relatively quick, even if it’s like you know you could get your CT scan and then you get your MRI scan requested and turned around in a week which is like you know a reasonable performance for a diagnostic test, it’s still another week and our diagnostic waiting times are actually quite tight our targets. (RDC11, national policy team)
Clinicians reported that the Faster Diagnosis Standard target was ambitious and sometimes required services to prioritise speed over a sequential approach to testing and diagnosis. Services sometimes had to book multiple tests in parallel to ensure patients receive a timely diagnosis, and book patients into clinics even when they could not be sure that their test results would be available. However, it was acknowledged that this approach may not be ideal from a holistic diagnostic perspective. The reality is if you were being a purist, you would do an endoscopy first, wait for the finding and then if that was negative then think about doing a CT scan, that’s an example of a patient, right. But the reality is we don’t have the leisure of all this time. And what I would do is I would book for an endoscopy and a CT scan in parallel, so when I speak to that patient or when a nurse speaks to that patient, he or she has all that information to hand. They can make a decision there and then and decide yay or nay and I think that is the reality of it. (RDC13, consultant)
Delivery of holistic care challenged by stringent inclusion criteria
For some participants, the holistic approach to redirecting and triaging patients set out in the 2022 NHS Faster Diagnosis Framework challenged other holistic values such as ‘owning the patient’. In two sites, consultants preferred to meet with patients prior to redirecting them to other services, particularly if the patient’s presentation did not meet the pathway criteria. Yes, so when we receive a [inappropriate] referral like that usually we are meant to reject it, however [consultant] does say that we shouldn't book any investigations yet, the first thing to do is just to see them face-to-face and have a conversation with that patient, you know maybe assess them face-to-face and then the outcome of that appointment will determine whether yes you know what maybe this patient might have something cancer related that’s wrong with them so we'll book them in for further investigations but usually when they send [inappropriate] referrals like that we just refer them back to their GP. (RDC08, navigator)
One NSS pathway nurse explained that sometimes it was easier to proceed with investigations because the exclusion symptoms would often only emerge once the patient had been accepted onto the pathway and was being assessed in detail by the nurse or navigator. So if they have specific [gastro-intestinal] symptoms, also sometimes actually that might not even be in their referral. Sometimes that comes from like nurse assessments because we just go through everything step by step to make sure we don’t miss anything. So if they have specific [gastro-intestinal] symptoms, even if they’re like [the faecal immunochemical] test is negative, like that kind of stuff then we’ll send them for like [orogastric tube] or colonoscopy. (RDC02, nurse)
Despite these challenges, most sites agreed that it was important to redirect patients to the most appropriate pathway, and that rejecting or redirecting patients could additionally provide educational feedback for GPs. A minority of participants reported that GP referrals had improved as a result of this strategy.
Challenges to promoting holistic care: Lack of clarity about the boundaries of the NSS
Differing interpretations of guidance about whether holistic care should include treatment and surveillance
As noted, the 2022 NHS Faster Diagnosis Framework indicated that “an NSS pathway should support patients until they are diagnosed and referred onward or their symptoms resolve”. 15 (p.15) However, the Framework does not specify the end point of the service, namely whether the NSS should offer only investigations and advice, or whether treatment, follow-up, or surveillance of incidental findings were also part of the NSS. This lack of specificity led to different interpretations.
Several sites were clear that their role was limited to providing diagnostic advice only and there was a reluctance to retain any ongoing responsibility for patients in order to protect service capacity and ensure the patient was treated by someone with the appropriate expertise. We want to find out the diagnosis and after that then we have to refer to the speciality like I said before, like this is just sometimes to manage expectations that sometimes patients think that we are going to provide treatment and we don’t. That’s also important that they understand that we don’t do treatment like I can’t keep prescriptions for gastritis because it’s not really up to us, you know, it’s up to the gastro team. We can also ask the GP and recommend the GP to prescribe it. (RDC03, nurse)
This view was not necessarily shared by everyone, however, with some noting that offering simple treatment was part of the holistic approach. We will, if there is simple treatment that we can start we will. We will start a patient, let’s say it’s Crohn’s, we will tend to refer to them as we discussed earlier to a gastroenterologist who will take on their more dedicated care. But we will get the ball rolling and rheumatoid arthritis, vascular, we can get all of that, but the reality is we can get this patient in pretty quickly. [...] When I joined two years ago I was under the impression that we were going to try and be a bit more holistic, not just yes to cancer, no to cancer, go to oncologist and go back to the GP. (RDC13, consultant)
There was lack of clarity of whether the NSS pathway included follow-up care to patients, referral to other hospital services or discharge to primary care. This was seen especially relevant given the large quantity of incidental findings that necessitated follow-up. This led to variation in implementation, with some participants explaining that they would be happy to organise follow up scans for patients even after discharge.
There was recognition that surveillance and follow up created more work, but this was seen to be important for patients, and therefore worthwhile. I mean that’s completely outwith the remit of cancer, patients who are having non-specific scans on the non-specific pathway [...] And it’s good because it will save lives in the future but it’s creating a huge additional workload or a [NSS] pathway for [GPs]. And that’s, I think often we don’t really resource that as part of the implementation, so we have resourced the non-specific pathway but we haven’t resourced all the incidental findings or all the additional pickups that we make on it. (RDC18, local decision-maker}
Lack of clarity about how to deliver holistic care for younger patients
The 2020 Framework notes that “any adult referred onto a NSS pathway should be triaged, investigated and safety netted, regardless of their age”
15
(p.11), but it does not specify how NSS pathways apply to younger adults. Local decision-makers highlighted that they had a responsibility to ensure that younger patients had an appropriate NSS pathway, and that their referrals were not being rejected by NSS teams. Clinicians reported that investigating non-specific symptoms in younger patients was particularly challenging. This was, in great part, because many younger patients referred to the service had a history of health anxiety or depression. As a result, some sites changed their service pathway to better meet the needs of their younger patients, for example, offering face-to-face appointments before ordering any imaging. So if we are triaging someone, I think so the people that normally get seen are if there’s someone particularly young. So like under 40 let’s say with like these very vague symptoms. So like we normally see those people. (RDC2, nurse)
There were concerns about exposing young patients to radiological risk, and several participants reported that they would make extra efforts to investigate any recent imaging in this patient group. Others also mentioned the importance of taking childhood history, recent emergency presentations and drug or alcohol use. This was seen as an important use of NSS pathway time, as GPs did not have capacity to provide lengthy assessments for these patients, and there was still an underlying risk of cancer.
Discussion
This study explored the implementation of NSS pathways in England, with a particular focus on understandings of holistic diagnostic investigation. We found that there was a lack of policy detail about what was possible or desirable within the current NSS pathway, with a narrow conception of ‘holistic’ care in this context. Implementation of holistic investigation varied between the four sites, with differing interpretations of holistic care provision in terms of values as well as practical activities to investigate patients beyond cancer exclusion. Delivering holistic care in NSS pathways was challenged by timed targets such as the Faster Diagnosis Standard due to limited availability of imaging and diagnostic tools. Investigating non-specific symptoms in younger patients posed a challenge due to their history of health anxiety or depression, and concerns over radiological risk exposure.
To the best of our knowledge, this is the first study to examine how clinicians approach patients with non-specific symptoms in dedicated NSS services. We found tensions about whether the NSS pathway should be delivered in a similar way to other cancer pathways, and whether the term ‘holistic’ is relevant and deliverable. Our findings show that while national policies may encourage holistic care, the main driver of delivery is the underlying values and beliefs of staff in NSS pathways. The paradigm of patient-centred care acknowledges that policies should support and facilitate health care staff to design innovative pathways to deliver holistic care. 22
Participants in our study strongly supported the view that investigating patients with non-specific symptoms potentially required more steps in the pathway (e.g. multiple tests and assessments) than other cancer pathways, which made it inequitable to impose a 28 days target for delivery of a cancer diagnosis. An evaluation of the NSS pathway in Hertfordshire, England, found that timed targets were challenging, with about 40% of patients not meeting the 28 days target. 23 Similarly, an analysis of professionals’ views of national cancer waiting time targets in England suggested that organisational differences for more complex diagnostic investigations had not yet been adequately considered from a policy perspective. 24
Concerns about unintended negative consequences of diagnostic timed targets have been raised in other areas of medicine. For example, a qualitative study of health professionals’ views about diagnostic pathways for young onset dementia found that timed targets were seen to undermine the substantial time and resources needed for holistic diagnosis of the condition. 25 Those resources include prioritised testing and imaging, highlighting the need to expand diagnostic capacity in the UK. 26 Our participants described having to make diagnostic choices in order to meet timed targets rather than considering optimal care; concerns about the impact of timed targets were also reported for cancer pathways in Denmark. 27
Our analyses found variation in local approaches to the management of incidental findings and other types of follow up care. An evaluation of a referral pathway for non-specific cancer symptoms in England reported that 95% of patients had incidental findings from a computed tomography scan, and 29% received further investigations. 28 Other studies also reported a lack of policy focus on the end point of patient pathways, with discharge and surveillance policy often underspecified and under-resourced. 29 It is unclear whether NSS pathways should be responsible for surveillance of incidental findings and ongoing symptoms; primary care professionals may not have sufficient knowledge to manage incidental findings without further advice and recommendations. 30 Other studies have suggested that responsibility for follow up should remain with the ordering physician rather than to a primary care physician. 31
Strengths and limitations
Data was collected during the COVID-19 pandemic, when competing priorities in cancer diagnostics may have affected delivery of care, as well as staff and patient experiences. The use of a multi-site ethnographic design and multiple data sources is a significant strength. It enabled us to capture variation between different NHS trusts, providing a robust and generalisable account. However, other NSS pathways in England or in other countries may have different approaches to holistic care, which were not represented in this study. It is also a strength of this research that it was carried out at a time when NSS service specification documents reviewed here (Table 2) were relatively new, and the policy implementation issues were a current preoccupation for staff.
The study only focused on the implementation of NSS pathways, and it did not include data collection in other cancer pathways for comparison. For example, patients referred to site-specific cancer pathways may have experienced different practices which were not captured in our study, and which limit our understanding of the overall impact of policy implementation.
Implications for research, practice and policy
Future research could explore the effectiveness of different models of NSS pathways in promoting earlier cancer diagnosis, as well as their impact on patient outcomes such as mortality and quality of life. There is also a need for further implementation research investigating the interplay between NSS pathways, other site-specific cancer pathways and pathways for the most frequent non-cancer diseases detected through NSS pathways. Additionally, research should focus on resource use, cost and unintended consequences on other patient pathways, as well as risks of overdiagnosis and overtreatment. Studies should also investigate the factors that influence the interpretation of a ‘holistic’ approach among health care providers, as well as patient and caregiver experiences with NSS pathways.
As the roll-out of NSS pathways progresses across England, local commissioners and decision-makers should specify best practice with respect to holistic care, underpinned by appropriately funded organisational models. This should include local hospital policies with respect to the management of younger patients and surveillance of incidental findings. Practical strategies for addressing the challenges of investigating non-specific symptoms in younger patients, such as using alternative diagnostic methods or involving mental health professionals, may be warranted.
Our findings can support the development of non-specific cancer pathways internationally, following similar initiatives in other countries. Our findings suggest that NSS diagnostic routes should not be viewed and monitored as an additional urgent cancer referral pathway. Any changes made to NSS pathways should balance the waiting times crisis in England against longer term aspirations. 26 There is a more general need for a clear national policy direction to ensure that high quality care is implemented in NSS pathways and guidance on what constitutes ‘holistic’ care to ensure that this approach is prioritised and adequately resourced in NSS pathways. Consideration should be given as to whether cancer-specific policies should be applied to NSS pathways, or whether they would be better placed within policies targeting general medicine. There is a need for decision-makers at different levels to recognise that timed targets may lead to opportunistic behaviour that does not benefit patients. Further consideration should be given to defining the boundaries of NSS pathways and whether they should take on the responsibility for follow-up care, and further research is needed to determine the best approach. Decision-makers should consider the input of health care staff in making these decisions, as they are best positioned to identify the challenges and opportunities for improvement in NSS pathways.
Conclusions
In England, patients with non-specific symptoms can now access rapid pathways to investigate the cause of concerning symptoms. Questions remain about the effectiveness of different models of NSS pathways in improving outcomes, as well as their impact on patient experience and quality of life. We have shown that NSS pathway implementation has been complicated by the need to adhere to standardised timed cancer targets and local cancer policies. There is a need for appropriately funded organisational models of care that incentivise providing holistic care in a timely way over meeting cancer targets. Decision-makers should consider the role of NSS pathways in the broader context of chronic disease management, with a particular focus on expanded diagnostic capacity.
Footnotes
Acknowledgments
We would like to thank Julie-Ann Moreland, Vinay Sehgal, Andrew Millar, Larysa Kwintkiewicz and Derralynn Hughes for their support with research governance and recruitment. The authors would like to thank the patients and staff who gave their time generously for this research, particularly the clinical non-specific pathway teams.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fellowship from The Institute of Healthcare Improvement Studies (University of Cambridge) (RG88620/PD-2019-02-004). GBB acknowledges funding from Barts Charity (G-001520). GL acknowledges support by Cancer Research UK Advanced Clinician Scientist Fellowship Award (C18081/A18180). NJF is an NIHR Senior Investigator. BDN is an NIHR GP Academic Clinical Lecturer and Cancer Research UK postdoctoral fellow (RCCPDF\100005).