
Abstract
Objectives
This study sought to describe feelings and perceptions of burnout and moral distress experienced by health care providers in the Canadian province of Saskatchewan during the COVID-19 pandemic.
Methods
This study was part of a larger mixed methods project, and we here report on the qualitative results relating to burnout and moral distress experienced by medical doctors, registered nurses and respiratory therapists. We used an exploratory, qualitative descriptive design involving one-one-one interviews with 24 health care providers. Interview data were analysed using a reflexive thematic analysis approach.
Results
We identified three overarching themes each for health care provider burnout and moral distress. Interviews revealed that providers experienced burnout through (i) increased expectations and (ii) unfavourable work environments, which led most of them to recognise (iii) a need to step back. Regarding moral distress, key themes were: (i) a sense of compromised care, (ii) feelings of bumping heads with authorities and patient families, and (iii) seeing patients make difficult decisions.
Conclusion
Our study found that medical doctors, registered nurses and respiratory therapists working during the COVID-19 pandemic experienced and continue to experience significant burnout and moral distress. This was often driven by both institution- and system-level factors. There is a need for sustained investment to build and support a motivated health care workforce to prepare for future pandemics and health emergencies.
Introduction
The global COVID-19 pandemic has had devastating effects on economies and communities, with the mental health impacts becoming a major concern for health systems globally. 1 Health care providers (HCPs) were especially affected. About half (51%) of HCPs responding to a global survey conducted in April 2020 reported burnout associated with high workload, job stress and impacts on their personal lives. 2 Many of the mental health effects of COVID-19 on HCPs have continued beyond the pandemic. For example, one study of staff working in intensive care units in England found that more than one in seven staff and nearly one in five nurses had thoughts of self-harm or suicide. 3 The mental health impacts of the pandemic continue to pose challenges to HCPs’ ability to remain motivated and provide services. 4
In this study, we considered two important mechanisms by which HCPs in Canada experienced poor mental health and wellbeing during the COVID-19 pandemic, burnout and moral distress. Burnout has been defined in terms of three core dimensions: exhaustion, that is workers feeling overwhelmed, overextended and depleted; cynicism, referring to workers feeling increasingly detached from the job and becoming negative towards clients and service recipients; and inefficacy or reduced efficacy, meaning that workers feel incompetent, with a low sense of accomplishment in the workplace. 5 Less attention has been given to understanding and developing appropriate interventions to respond to the challenge of HCP moral distress. Moral distress in medicine refers to uncomfortable feelings and negative emotional responses experienced by clinicians as a result of a discordance between what they believe they ought to do and what they actually do. 6 Moral distress is typically linked to challenges that HCPs face in clinical decision making, but it might also be created by the wider context, for example health care reforms, that constrain HCP’s ability to make ethically informed decisions.
The empirical evidence on burnout and moral distress among HCPS linked to COVID-19 in Canada remains somewhat patchy. Burnout rates have tended to be relatively high even before the COVID-19 pandemic, with one study estimating the rate of emotional exhaustion among physicians to be as high as 80%. 7 The existing literature suggests that the pandemic has worsened burnout rates, with evidence of statistically significant associations between a sense of lack of support in the workplace and burnout among HCPs. 8 Regarding moral distress, one study in the USA suggested that nurses experienced many instances of feelings of fear, guilt, powerlessness and frustration linked to the pandemic. 9 Less is known about experiences of moral distress by HCPs during COVID-19 in Canada. In a survey of community health nurses across Canada, 82% of respondents reported experiencing moral distress and over 90% indicated that their current levels of moral distress were higher than pre-pandemic levels. 10 The Canadian Medical Association has recognised the pervasiveness of this issue and produced guidelines to support HCPs experiencing moral distress, suggesting self-care and organisational procedures to improve physician wellbeing. Despite such efforts moral distress remains common.
Overall, there is a need to better understand HCPs’ lived experiences of burnout and moral distress in the context of the COVID-19 pandemic and how these may be implicated in the ongoing mental health challenges faced by HCPs. Such evidence will help inform the development of potential interventions and provide directions for safeguarding HCPs wellbeing in future pandemics and health emergencies. For clarity, we treat the constructs burnout and moral distress separately, while recognising that they are highly correlated. Morally distressing situations where clinicians are unable to make the ethical choice they desire can lead to a sense of depletion and cynicism associated with burnout. Similarly, HCPs experiencing burnout are more likely to feel morally distressed, often through a sense of depersonalisation.11,12
In this study, we explored the mental health impacts of the COVID-19 pandemic on three groups of HCPs, medical doctors (MDs), registered nurses (RNs) and respiratory therapists (RTs) in Canada. Specifically, we sought to describe feelings and perceptions of burnout and moral distress experienced by these groups, drawing on interview data from the Western province of Saskatchewan.
Methods
This study was part of a larger mixed methods project, and we here report on the qualitative results relating to burnout and moral distress experienced by HCPs. We used an exploratory, qualitative descriptive design, 13 focusing on participants’ experiences and perceptions of the impact of the COVID-19 pandemic on providers’ resilience, wellbeing needs, and provincial and health authority policies that affected them. We engaged one medical doctor, one registered nurse, one respiratory therapist and two patients as research team members.
Setting and sample
The setting for this study was the province of Saskatchewan, Canada, with a population of 1.2 million people, ranking 6th by population size among the 10 Canadian provinces. With a history of ensuring fair access to health care, the provincial health and social care system has seen major changes over recent decades, including budget cuts, closure of rural hospitals and health worker shortages. These factors made the province more vulnerable to the COVID-19 pandemic, 14 as reflected in a higher-than-average death toll from the pandemic and a political response that involved the premature lifting of COVID-19 pandemic restrictions, which resulted in acute capacity shortages requiring moving critically ill patients to other parts of Canada. 15
Recruitment
We used a convenience sample of HCPs who we recruited from an online survey of 1497 HCPs that was conducted as part of the larger project. The survey included an option for respondents to participate in an interview to further explore their experiences and perspectives. Interested individuals were directed to a separate webpage not linked to the survey where they could leave their contact information. They were then contacted by a research team member (JAKA), screened for eligibility and consent obtained. Eligible HCPs had to be English-speaking adults who were registered as a MD, RN, or RT in Saskatchewan and who were currently or previously working in that role from March 2020 onward.
A total of 24 HCPs participated in the interviews including nine MDs, eight RNs, and seven RTs. The majority of interview respondents were female (n = 19) and worked in urban centers: Saskatoon (11), Regina (6), Prince Albert (3), other (2), while two (2) respondents were from a rural community in northern Saskatchewan.
Data collection
One-on-one interviews were conducted via telephone or videoconference (Zoom); we used a semi-structured topic guide (see Online Supplement) that focused on provider experiences related to a variety of topics including job satisfaction, burnout, moral distress, resilience, intention to leave, and wellbeing needs. Interviews were conducted between May and August 2022 and lasted approximately 60 min.
Data analysis
Data were transcribed verbatim, and the recordings were compared with the transcripts to ensure accuracy. Data was stored and managed using NVivo software. 16 We used thematic analysis as described by Braun and Clarke. 17 The reflexive thematic analysis approach included six stages: 1) data familiarisation through initial readings; 2) generating codes through labeling the data; 3) constructing themes by synthesising and combining codes to form categories; 4) reviewing potential themes for similarity and mutual exclusiveness; 5) finalising themes; and 6) reporting themes and attributing quotes to synthesised themes. 17 Burnout and moral distress were analysed as separate constructs, identifying overarching themes for each for clarity. Each theme served to express one aspect of HCPs’ experiences with moral distress and burnout during COVID-19 in Saskatchewan but was not exhaustive.
Data analysis was performed by one master’s graduate student research team member (TP), guided by her supervisors (NR and JAKA). These three team members reviewed the data during the coding and analysis process to achieve consensus agreement on codes and themes. The remaining team members reviewed the findings for agreement, understanding, and fit to ensure rigour within the data analysis process.
Ethics approval
Research ethics approval was obtained from the University of Saskatchewan (BEH 3051).
Results
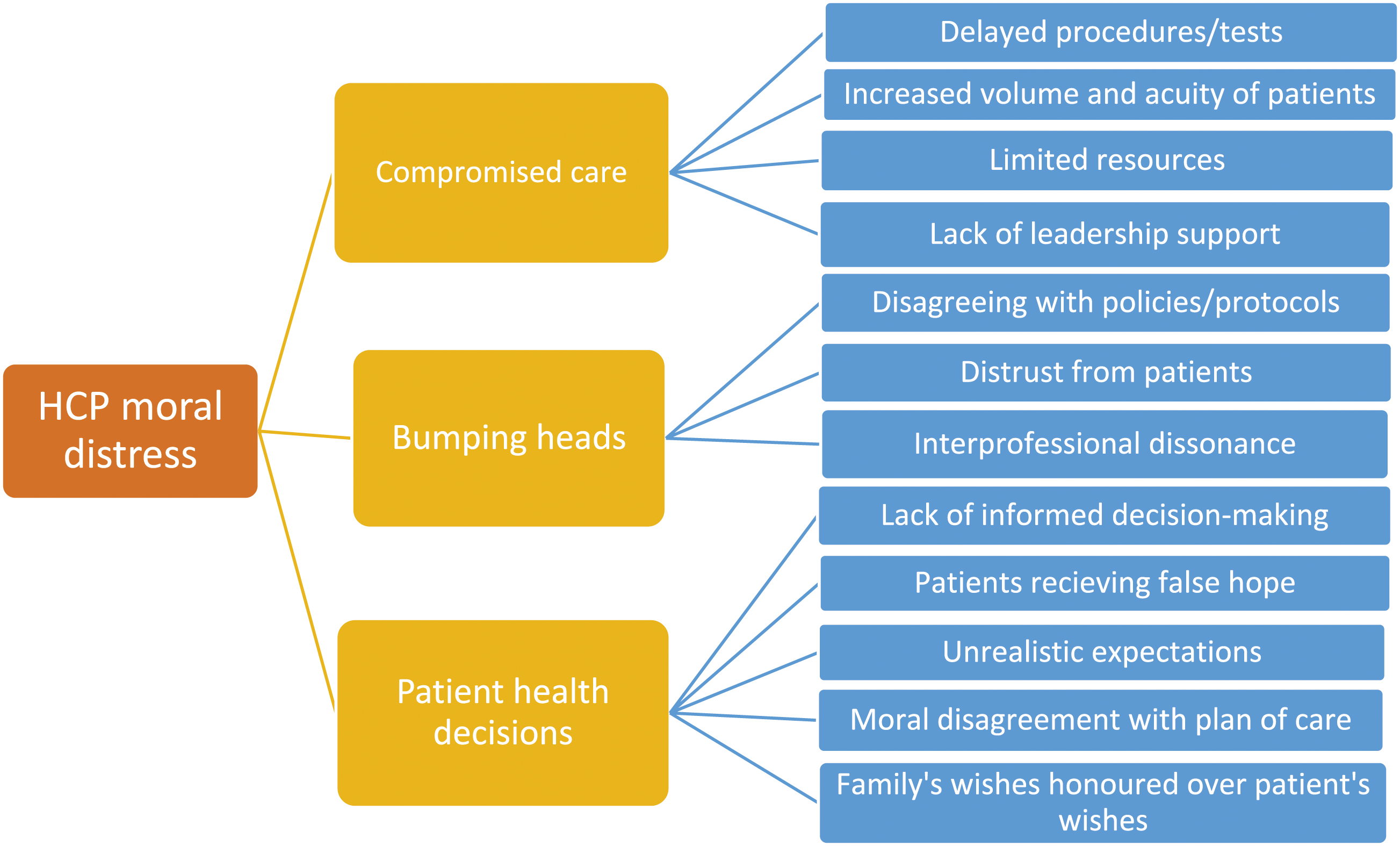
HCP interview analyses identified three overarching themes each for HCP burnout and moral distress in Saskatchewan during the COVID-19 pandemic (Figures 1 and 2). As noted, for clarity, we describe each construct separately while recognising that they are deeply interrelated. For example, an unfavourable work environment that contributes to burnout also amplifies ‘compromised care’, one major factor associated with moral distress in this study. Similarly, increased expectations associated with burnout cause the ‘bumping of heads’ which was related to moral distress. Identified themes related to HCP burnout. Identified themes related to HCP moral distress.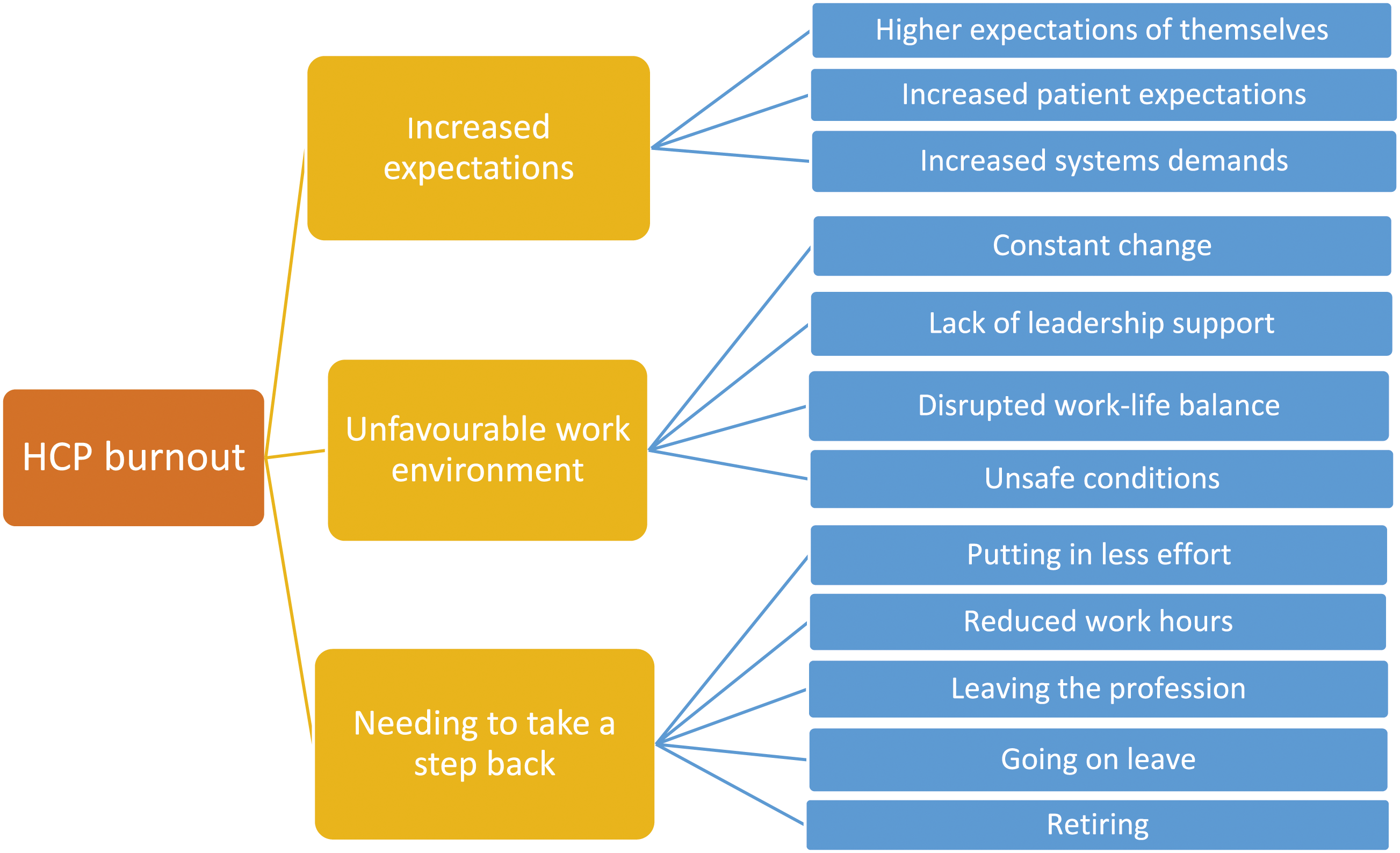
Health care provider burnout
HCPs experienced varying levels of burnout depending on their roles, responsibilities, and locations of work, but many described similar feelings. They described their experiences with burnout as feeling frustrated, hopeless, anxious, guilty, and overwhelmed, which ultimately led to them feeling that their mental health was negatively impacted. We identified three overarching themes: (a) increased expectations, (b) unfavourable work environment, and (c) needing to take a step back (Figure 1).
Increased expectations
HCPs reported experiences of increased expectations to work demanding schedules and excessive overtime due to a lack of staff. They felt personally responsible for maintaining patient care through staff shortages and that they had risked their lives by being exposed to COVID-19. There were also reports of increased effort required to meet the increasing and complex demands of the health service and system more widely, with expectations to care for higher acuity patients and an increased volume of patients and responsibilities while being understaffed and lacking administrative support. The burnout because of reliance [on us] became so much… we’re supposed to work eight hours a day… and it wasn’t unusual for us to be working ten and twelve hours a day, five days a week… It was just that there was no staff for us, and the patients we were getting were very, very sick. (HCP 23, RT 7)
HCPs also noted increased expectations from their patients. Some HCPs explained scenarios in which patients assumed they would have quick access to health care services due to the advancement of telehealth or virtual care. HCPs felt that patients had unrealistic expectations, expecting staff to ‘function’ as they did prior to the COVID-19 pandemic with little understanding of the difficult circumstances within which they were working.
Unfavourable work environment
Experiences of an unfavourable work environment were characterised by constant change, lack of leadership support, disrupted work-life balance, and an unsafe workplace. Constant change was related, largely, to changes in COVID-related policies or protocols and to being redeployed to areas of work without adequate training. This led HCPs to experience a lack of control, of being ‘worn down’ (HCP 17, MD 8), and of having a general sense of frustration (I was just getting tired of it. Just constantly not knowing or not having that right answer, or not being able to find that right answer’ (HCP 19, RN 6)). Lack of leadership support was experienced as micromanagement by supervisors, supervisors being unreliable, and supervisors expressing favouritism towards certain staff members. HCPs reported feelings that their needs were ignored by management and that they were given little or ineffective guidance.
An important facet was a perceived lack of work-life balance, with HCPs citing mental strain, perpetual exhaustion, and isolation from working in an unfavourable work environment as reducing their motivation to spend time with social relations. HCPs described experiences of returning home from work feeling angry, irritable, exhausted, unmotivated, and hopeless, resulting in disconnection from social networks and a feeling of ‘falling behind’ in several aspects of life: ‘…for me like I’ve fallen behind in my studying, I’ve fallen behind in my research, I’ve fallen out of touch with friends just because you’re mentally just done when you come home from work’ (HCP 11, MD 5).
Finally, perceptions of an unsafe work environment also contributed to HCP burnout. As noted, HCPs reported becoming responsible for an increasing number of patients of higher acuity, which, along with inadequate staffing and resources, they experienced as placing both themselves and patients at increased risk not only of infection itself but also making it challenging to maintain the standard of care, which, in turn, contributed to experiences of stress and burnout. HCPs noted high levels of understaffing, which they attributed to job vacancies that were not being filled, in addition to HCPs retiring early, going on sick leave, finding other jobs or leaving their profession altogether.
Needing to take a step back
A common theme around how HCPs navigated the factors described above was the need to take a step back. Taking a step back was described as putting less effort into work, reducing work hours, going on sick leave, or feeling the need to retire sooner than originally planned. Some HCPs indicated the pandemic as their primary reason for retiring early and many HCPs worked in less stressful positions in the hope of avoiding or reducing burnout. Some HCPs even considered leaving their profession altogether to seek out less stressful jobs. HCPs who felt required to take a step back likely directly contributed to short-staffing, including at senior levels, which, in turn, contributed to HCP burnout.
Health care provider moral distress
HCPs expressed experiences of moral distress in scenarios where care was compromised due to circumstances induced by the COVID-19 pandemic, as well as health care system inadequacies that were further compounded by the pandemic. HCPs described feelings of helplessness, hopelessness, guilt, and frustration. While levels of expressed moral distress varied depending on HCPs’ profession and workplace, it was most frequently mentioned in intensive care settings. We identified three overarching themes regarding HCP experiences of moral distress: (a) compromised care, (b) bumping heads, and (c) patient health decisions (Figure 2).
Compromised care
Participants described compromised care as the inability to maintain standards of patient care and settling for inadequate alternatives. Reasons for compromised care during the COVID-19 pandemic included delayed procedures or diagnostic tests, the aforementioned increases in patient numbers and acuity, limited resources, and lack of access to hospital leadership and other support.
Existing staff shortages were a key reason for compromised care associated with moral distress. These shortages were further compounded by the health care ‘slowdown’ as a result of the COVID-19 pandemic. HCPs stated they were overextending themselves to make up for these shortages, further reducing their already limited time with patients and thus compromising care, which caused moral distress. HCPs also experienced a lack of available members of interdisciplinary teams as directly impacting patient outcomes. They reported delayed tests and procedures, and reduced services from phlebotomists, social workers, RTs, and many other specialists, which they thought would have negative knock-on effects for patients such as need for intensive care and, possibly, death because of high acuity seen during the COVID-19 pandemic. Although HCPs knew that these delays would lead to low quality care and possibly patient deaths, they had no option but to provide such compromised care and this caused moral distress among many study particpants.
Compromised care was not only perceived as problematic for patients who were seriously ill with COVID-19; HCPs also referred to a ‘trickle-down effect’ on other patients ‘who need these treatments also [but were not] getting these treatments because we don’t have access to these medications or to this equipment that we need. (HCP 4, MD 3). Similar to COVID-19 patients, feelings of moral distress resulted from HCPs believing that higher quality care would have been more appropriate for some non-COVID-19 patients or that some of these patients ‘could’ve been managed differently’ (HCP 23, RT 7).
Bumping heads
HCPs reported experiences of moral distress when engaging in conflict with patients, family members, authorities, or other providers. ‘Bumping heads’ was described as disagreeing or having clashing views with others and/or with policies. Moral distress was especially experienced in relation to the strict visitor restrictions within health care facilities, especially regarding critically ill or dying patients. HCPs stated that they felt it was immoral and inhumane to deprive patients from their social networks when they needed them most.
Some HCPs also reported observing expressions of distrust from their patients towards the health care system due to COVID rules. Participants frequently noted that they felt unable to provide medical advice or guidance to patients as COVID-19 information was constantly changing and the difficulty to ensure they were informed of the most recent updates. The perceived lack of patient and public trust in HCPs and the health care system was viewed as detrimental to vaccine distribution, deterring patients from seeking health care.
The most prominent issue identified in the HCP interviews regarding ‘bumping heads’ was between RTs and RNs with MDs. RTs and RNs frequently reported feeling that MDs ignored their questions and concerns regarding their patients and that patient outcomes may have improved if their concerns had been listened to: ‘…the doctors… they wouldn’t really listen. So, we would know so many things were wrong, but didn’t have the support to advocate for our patients…’ (HCP 13, RN 4).
Patient health decisions
The COVID-19 pandemic meant that patient health decisions about their plan or goals of care, which were shared with HCP teams, were difficult to follow-through. HCPs described morally distressing scenarios where patients were not informed, were given false hope, were unrealistic in their expectations or were ignored. HCPs also noted that they did not always agree with a given plan of care, and, in some cases, they felt like they were prolonging a patient’s suffering. I found a lot of moral distress in treating [patients admitted with COVID-19 to intensive care]. These are patients who were so immensely ill on ventilators that would be near death for weeks and especially at the beginning, there was a lot of ‘what are we doing here?’ It felt like we were just providing futile care for weeks and weeks and weeks. (HCP 9, RN 3)
HCPs reported experiencing barriers to provide patients with the required information to make informed decisions about their care. Barriers included lack of time or because patients were too ill to understand the implications of their decisions. There were reports of information being withheld from patients at times regarding the possibility of negative health outcomes or false hope was given to patients which directly influenced patients’ health decisions.
HCPs described situations where patients’ wishes were not listened to, but the family’s wishes were, causing them moral distress, especially where family’s wishes or expectations contradicted those of the patient or where a family’s decision was causing the patient more harm than benefit: ‘I think that's the hardest part is, knowing that people are suffering but we continue going along because that's what the family wants’ (HCP 20, RT 6).
Discussion
The mental health impacts of the COVID-19 pandemic have been severe for HCPs, with implications for health worker recruitment, motivation and retention, and health systems more widely. We document HCPs’ experiences of burnout and moral distress among three professional groups with varying levels of professional autonomy, experience and resources in Saskatchewan, Canada. We found that experiences of burnout and moral distress were relatively high even three years into the COVID-19 pandemic.
The urgency of the pandemic, particularly in the early months, often meant that HCPs had to consistently work above and beyond what would be considered a healthy and normal volume of work. Elsewhere, this was described as HCPs being on a “hamster wheel from hell”. 18 (p.4) Evidence of HCPs experiences during the pandemic pointed to increasing volumes of work as a major driver of burnout, 19 reflecting the findings from our study. This was, in part, driven by HCP shortages, highlighting the need for a broader long-term solution to improve HCP wellbeing and pandemic preparedness. In Canada, it was estimated that there would be a shortage of about 117,600 nurses by 2030. 20 More recent reports from Ontario indicate a projected shortage of 330,000 nurses and personal support workers by 2028. 21 The Canadian Medical Association recently noted that half of all Canadians do not have a family doctor 22 and the vacancy rates for respiratory therapists over the last decade was 20%–25% due to workforce shortages. 23 Thus, there is not only a need to improve the working conditions of HCPs and provide adequate support, but also for greater public investment in training a sufficient number of HCPs.
Evidence on HCPs’ experiences of burnout has highlighted the critical role of leadership in protecting HCPs particularly in highly stressful situations such as pandemics. 24 Several of the HCPs interviewed for this study highlighted the impact of constantly changing rules, procedures and protocols, as well as changes in roles. Pre-pandemic research on the role of leadership styles found that physicians who believed that their supervisors were good leaders were up to 47% less likely to experience burnout. 25 Further, Siddiqui and colleagues 8 reported that HCPs who perceived their work environments to be supportive had a reduced risk for several negative mental health outcomes. Thus, strengthening clinical leadership to create supportive environments could play a powerful role in reducing HCP burnout. Formalised programmes, such as the Social Support, Tracking Distress Education and Discussion (STEADY) programme developed in Canada to support the wellbeing of HCPs experiencing burnout during the pandemic may help reduce burnout levels and promote the wellbeing of HCPs. 26 While promising, leadership and commitment at clinical and system level will be important for the effective and sustained long-term implementation of such initiatives.
Moral distress was another critical focal point through which HCPs experienced the COVID-19 pandemic. We found that moral distress often emerged in the context of caring for COVID-19 patients or providing care during the pandemic. Thus is similar to D’Alessandro-Lowe et al. 27 who noted that Canadian RTs working in COVID-19 wards were much more likely to report moral distress than those working in other wards. Moral distress resulted from the need to provide compromised and sub-optimal care, conflict with others, and the experience of seeing patients being ill-informed about available care options. Baxter et al. 10 identified four key elements driving the experiences of moral distress among HCPs in Canada: severely limited health care resources, reactive rather than proactive pandemic responses, heavy workloads connected with staff shortages, and abrupt and repeated redeployments of HCPs. In our study, HCPs working in intensive care units were among some of those who struggled the most with moral distress as they found it increasingly difficult to ‘leave work at work’ and were often ‘bumping heads’ particularly when working in multidisciplinary and interprofessional teams. Trachtenberg and colleagues 28 noted the challenges faced by HCP working in intensive care, with experiences of moral distress and burnout pushing many clinicians into ‘survival mode’, making it very difficult to simultaneously advocate for patients and practice self-care.
Despite the adversities experienced by many HCPs due to stress and trauma associated with the COVID-19 pandemic, evidence suggests important narratives of resilience that have encouraged renewed professional commitment. A systematic review highlighted the value of HCP resilience during the pandemic and identified several factors enabling HCPs to develop and cultivate resilience, including: moral purpose and moral duty, connections to family and peers, collaboration with others interested in providing care, supportive organisational culture, personal character and coping strategies, and the ability to see potential for growth. 29 Moral resilience is defined as the “capacity [of a person] to sustain, restore, or deepen her or his integrity in response to moral complexity, confusion, distress, or setbacks”. 30 (p.13) However, moral resilience should not be seen as an individual responsibility and is only possible when environments are sufficiently supportive to cultivate it, requiring systemic solutions.
Several tools are being developed to safeguard HCPs from moral distress and burnout and it remains imperative for health system stakeholders to consider and pilot these. Examples include organisational strategies to improve HCP wellbeing as proposed by the Mayo Clinic. These include: acknowledging and assessing the problem of HCP poor mental health; harnessing the power of leadership; developing and implementing targeted interventions; cultivating community at work; using rewards and incentives wisely; aligning values and strengthening culture; promoting flexibility and work-life integration; providing resources to promote resilience and self-care; and facilitating and funding organisational science. 24 However, while helpful, there is a need for broader system-level responses to the structural drivers of burnout and moral distress including staff shortages, poor leadership and acute lack of resources in order to prepare for future pandemics and health emergencies.
Conclusion
This study described experiences of burnout and moral distress among HCPs in Saskatchewan three years into the COVID-19 pandemic. Doctors, nurses and respiratory therapists reported many instances of and continue to experience significant burnout and moral distress, which was frequently driven by organisational and system-level factors. Residual mental health effects of the pandemic continue to be experienced by many. Governments should consider investing in training a larger number of HCPs to respond to staff shortages as well as developing and implementing psychological first aid training for the HCP workforce. The lessons from the present pandemic offer an opportunity for institutional change as a key strategy for pandemic preparedness.
Supplemental Material
Supplemental Material - Health care providers’ perceptions of burnout and moral distress during the COVID-19 pandemic: A qualitative study from Saskatchewan, Canada
Supplemental Material for Health care providers’ perceptions of burnout and moral distress during the COVID-19 pandemic: A qualitative study from Saskatchewan, Canada by Jacob Albin Korem Alhassan, Noelle Rohatinsky, Taylor Peru, Carmen Levandoski, Dennis Kendel, Jeff Dmytrowich, Tenille Lafontaine, Matthew Cardinal and Juan Nicolás Peña-Sánchez in Journal of Health Services Research & Policy
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Saskatchewan Health Research Foundation (SHRF #6409).
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.