
Abstract
Objectives
Hospital in the Home models are rapidly expanding in response to increasing bed pressures. This study examined patient and multidisciplinary health professional perceptions of a new geriatric evaluation and management and rehabilitation hospital in the home service in Australia. The service was unique, as adults of all ages with a variety of rehabilitation or geriatric evaluation and management needs were within scope.
Methods
A qualitative descriptive approach was used with a consumer co-researcher and a consumer advisor being integral to decision-making. Patient feedback was collected via a paper-based patient satisfaction survey between August 2020 and February 2022. Additionally, interviews with current and past staff were conducted from July to November 2021. Reflexive thematic analysis was conducted for qualitative data and descriptive statistics used for quantitative data.
Results
Patient surveys were analysed (n = 199, 42.2% response rate) with 60.8% of participants aged 75 years or over and 26.6% speaking a language other than English. High satisfaction was expressed. Feelings of comfort, familiarity, convenience, and reassurance were voiced. A person-centred approach enhanced involvement in care. Challenges included carer burden and clear communication. Sixteen staff (33% response rate) were interviewed. In general, staff said the service was inclusive and responsive, and the home environment beneficial, particularly for patients from culturally diverse backgrounds. A strong hospital partnership and comprehensive multidisciplinary approach were vital. Challenges included fragmentation due to part-time roles and combining with a pre-existing acute hospital in the home service.
Conclusions
This qualitative exploration of staff and patients’ perceptions of a geriatrician-led, multidisciplinary geriatric evaluation and management and rehabilitation hospital in the home service demonstrated that it was person-centred and optimised patients’ control and ownership of care. The inclusive service parameters ensured responsiveness to diverse needs whilst allowing earlier return home from hospital, both of which are vital for quality patient care.
Introduction
Hospital in the Home (HITH) models are rapidly proliferating internationally to reduce demand on hospital beds due to the increased burden of ageing, chronic disease, and multimorbidity.1–4 The terminology used to denote HITH services varies and may also include Hospital at Home5,6 and early supported discharge.7–9 For the purposes of this paper, the defining feature of HITH is that it provides the skills, technologies, and support required to treat patients who would otherwise require hospital inpatient admission. 3 HITH may be a substitution for hospital admission (hospital avoidance) or help reduce hospital length of stay (early discharge). 4 The COVID-19 pandemic has added further urgency to the uptake of HITH models as hospitals struggle to meet increased demand.10,11 However, HITH models have traditionally had a narrow scope, delivering care to patients with a small number of acute medical conditions, 3 and there is a need to expand HITH services to better support the needs of older patients.12–14
There is emerging research in relation to HITH for older persons such as services focussing on acute delirium, 15 acute orthopaedics, 12 comprehensive geriatric assessment admission avoidance,11,14 and a geriatrician-led acute medical crisis service. 13 Most HITH model evaluations support positive patient and service outcomes. HITH services can increase hospital bed capacity without the delays and expense of new builds 16 and have been shown to be safe and feasible.10,11 Other benefits particularly relevant to older persons, include reduced rates of nosocomial infection, functional decline, incontinence, and malnutrition;8,11,17 improved sleep; and more support from family and friends.2,18 When health care providers see patients at home, they are better able to review patients’ individual situation, and to address social determinants of health including social/community context, the built environment, education needs and access to ongoing care. 10 The ability to re-establish home routines through HITH models may particularly benefit older patients with delirium or dementia.11,19
The evidence regarding the effect of HITH on readmission rates is unclear. A systematic review indicated that HITH made little to no difference to the risk of readmission for patients post stroke or after orthopaedic surgery, increased risk for a mix of medical conditions, and decreased risk for chronic obstructive pulmonary disease. 6 Other research has demonstrated readmission rates to be lower following HITH care,4,17 or higher at one month but no different at 3 months. 11 The evidence regarding cost is also mixed. A systematic review indicated uncertainty about HITH effect on cost across stroke, medical and elective surgery services. 6 Costs were possibly reduced with direct admission to HITH from the emergency department 16 and in another admission avoidance model. 14 HITH services may reduce admission to residential aged care at 6 months,6,11,14 although this was not supported in a recent systematic review. 8
Value-based care includes understanding patient experiences and perceptions of quality of care, and as such, patient perceptions are core to HITH evaluations.5,20 Previous research has shown high patient and carer satisfaction for acute HITH services.2,21,22 However, limitations include a low response rate and few qualitative text comments. 21 When compared to traditional inpatient models, HITH patient satisfaction was demonstrated to be slightly improved in a systematic review 6 and higher in a randomised control trial. 11 Health care professionals (including medical, allied health, and nursing staff), older adults and family members provided their perspectives regarding a potential HITH service for older medical inpatients. They identified that a new HITH service could improve discharge processes, enhance patient dignity and independence, decrease strain on inpatient staff, reduce the adverse effects of prolonged hospitalisations, and strengthen communication between hospital staff, patients, families, and community providers. 9 A recent metasynthesis of 16 qualitative studies examining HITH stakeholder perspectives across multiple service models concluded that strong partnerships between health professionals and patients promoted high patient satisfaction. 4 However, a limitation was that allied health professionals and clinical assistants were participants in only one study. A recent scoping review indicated that research is required to explore and evaluate interdisciplinary care in HITH models that include unrepresented disciplines such as social work and occupational therapy. 23 The perspectives of HITH from people from culturally and linguistically diverse backgrounds are also required, as they may be less likely to access HITH services. 2
The current study seeks to address those research gaps, reporting research on a geriatric evaluation and management and rehabilitation HITH initiative that includes a wide range of disciplines, including allied health, and includes patients from diverse ethnic backgrounds.
GEMRHITH service delivery model
Sub-acute care is defined as specialised multidisciplinary care where the primary care need is to optimise a patient’s functioning and quality of life. 24 A new sub-acute HITH service was developed at a 200-bed hospital in an Australian state capital city to address rising health care demands. The service is called GEMRHITH (Geriatric Evaluation and Management, Rehabilitation, Hospital In The Home). GEMRHITH commenced in October 2019, 10 months prior to data collection for this study. It is geriatrician-led, with medical registrar support and a dedicated multidisciplinary team comprising nursing, allied health assistant, dietician, occupational therapy, speech pathology, pharmacy, physiotherapy, psychology, and social work. Nursing staff are employed within a pre-existing acute HITH service, located at the hospital but reporting through the health service community division. Acute HITH provides acute care to patients who have a well-defined, stable condition and are able to self-care or have a responsible carer(s).
Referrals are received from the treating medical/surgical teams in the emergency department, inpatient wards, or outpatient areas to the geriatrician. Multidisciplinary team members provide support to facilitate and triage referrals. Adult patients are eligible for the service if they require inpatient care, have a telephone, live in the hospital catchment, and are able to be safe in their home with daily support for hygiene, medications and meals, and less frequent support for household tasks and shopping. The main patient conditions targeted for GEMRHITH include geriatric evaluation and management, debility, orthopaedics, stroke, other neurological conditions, and patients post orthopaedic or other surgery who are slower to recover. All patients must be able to manage toileting/continence, oral intake, transfers and mobility, and medications independently or with family/own carer support. Bed-bound patients are eligible if their family/own carers are able to provide support as above. Patients are not eligible if they are at high risk of a medical emergency, living in a residential aged-care facility, or are more suitable for post-acute or community services.
All patients receive at least one daily home visit, a state government requirement. The discipline visiting is determined by patient need and staffing availability. Nursing staff provide all weekend visits, with a medical and nursing remote on-call service available 24 hours per day. Discharge planning occurs whilst many patients are in hospital and is continued in GEMRHITH. Referrals to community services – such as for personal care, medication management, cleaning, shopping, meals, and allied health services – occur as relevant. Family, unpaid carer, and community service provider handover and training occur in the home whilst patients are on GEMRHITH to support person-centred, safe, and sustainable discharge.
Methods
Diverse perceptions were examined using a qualitative descriptive approach 25 to explore patient perspectives and to gain insights into the experiences and perceptions of staff. The study was part of a larger project evaluating the service outcomes of the GEMRHITH model. Other aspects of the service evaluation will be reported in the future elsewhere. The study was conducted during the peak of the COVID-19 pandemic. Whilst the model of care did not change during the peak of the pandemic, it impacted methods of data collection and participant recruitment. Specifically, patient interviews were not conducted, as it was against infection control advice to send an additional person (i.e. the interviewer) to the patients’ homes.
This paper has included extensive consumer partner involvement. One consumer was a co-investigator and co-author (AM) and the second was consulted during study development and data analysis (see acknowledgements). One of these consumers (AM) brought the lived experience of being an older person with a disability and long-term rehabilitation service user, and the other the carer perspective of having cared for a GEMRHITH patient who was from a culturally and linguistically diverse background. Neither consumer was directly involved in contributing to the data or collecting data for this research and hence there were no conflicts of interest. Consumer involvement has been reported throughout the manuscript. More details regarding the consumer influence on the study plus benefits and challenges of the consumer involvement are included in Online Supplementary File S1, to further meet GRIPP2-SF Checklist requirements. 26 The consumer partners were aware that there was no dedicated funding for the project and received a small honorarium for their time.
Patient surveys
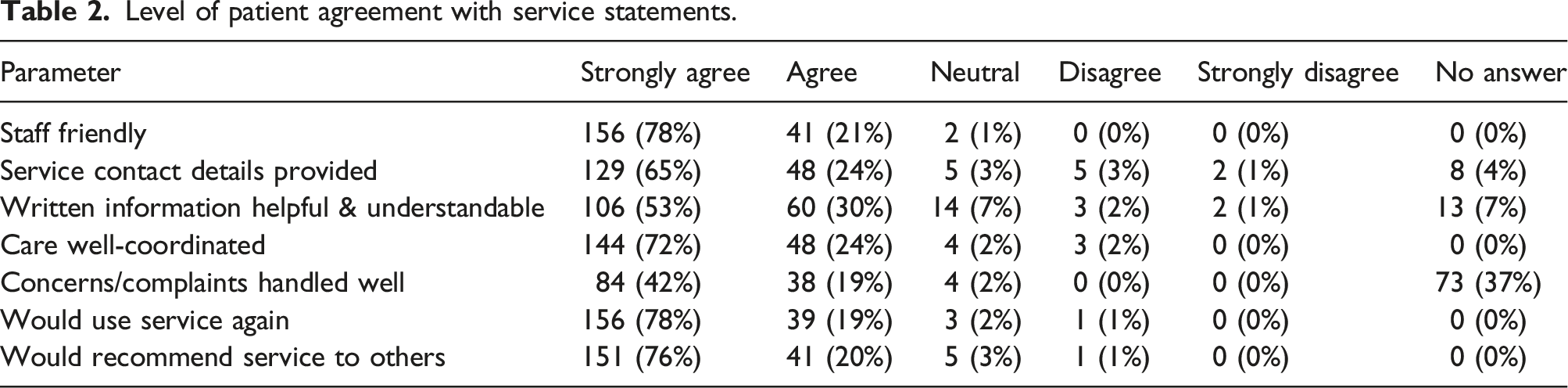
Patient feedback was collected via a paper-based survey (adapted from the survey used in acute HITH). The hospital Consumer Advisory Council and the consumer partners in this research reviewed the survey tool on two occasions, and adaptations were made to enhance question clarity. The survey collected (1) demographic information, (2) patient preferences on a five-point scale regarding staff friendliness, whether service contact details were given, quality of written information, whether care was well co-ordinated, handling of complaints, whether the patient would use the service again, and whether they would recommend the service to others, and (3) open-ended responses covering likes/dislikes and other feedback. The survey tool is available as Online Supplementary File S2. Follow-up phone calls (typically by the allied health assistant) were used to increase survey response rates. Telephone calls also aimed to support patient engagement from culturally diverse backgrounds, as recommended elsewhere. 21
As approved by the relevant ethics committee, patients were not required to provide written consent for the survey as it was collected during business-as-usual service evaluation. All patients had access to GEMRHITH staff, including social work and psychology if they became distressed when completing the survey.
The survey was provided to all GEMRHITH patients discharged between August 2020 and February 2022 (n = 472). A total of 199 patient surveys were completed, representing a response rate of 42.2%. The surveys were personally completed by 103 patients (51.8%) and 50 carers of family members (25.1%). A further 45 (22.5%) of surveys were completed by staff on behalf of a patient or carer/family member and it was unknown who completed one survey (0.5%).
Staff interviews
A semi-structured interview guide (see Online Supplementary File S3) was developed by the research team including the consumer partner. The research team developed the interview guide and four staff in the service provided feedback on a draft of the guide. Two staff information sessions were conducted to introduce the research and to answer questions. All staff participants provided written consent. Interviews were conducted by GK, who had not been involved in the GEMRHITH service, in order to encourage open comment and maintain participant anonymity. Interviews were conducted by telephone, were audio recorded, transcribed verbatim, and verified against the recording by GK. The participant information and consent form included details regarding options if the interviewee experienced concerns or distress.
All multidisciplinary staff involved with GEMRHITH from its inception, including those no longer involved (n = 48), were invited to participate in the interviews. Half of the staff (48%) consented to be interviewed. However, only 16 (33%) actually completed an interview, due to workload demands during COVID-19. Interviews lasted an average of 31 min and took place between July and November 2021.
Data analysis
Fixed-choice survey data were analysed using descriptive statistics. Open patient survey responses and staff interviews were inductively analysed via reflexive thematic analysis using the updated six stage process. 27 The approach was suitable given the rich detail and emotive content. Data analysis was an interpretative process with each researcher bringing their own social, cultural, historical, disciplinary, political, and ideological lens. 27
Two of the team (RC and AS) developed codes from patient surveys and preliminary themes, which were iteratively reviewed by three others, including a consumer partner (GK, AM, and MM). Staff interviews were coded by GK, and a random sample of 25% independently coded by RC. Codes were compared and discrepancies resolved by consensus. Given coding similarity, the 25% sample was deemed sufficient. RC then led development of preliminary themes. The interviewer (GK), one consumer partner (AM), and another author (MM) iteratively collaborated with RC to refine and name the themes.
Results
Patient surveys
Patient survey respondent characteristics (n = 199).
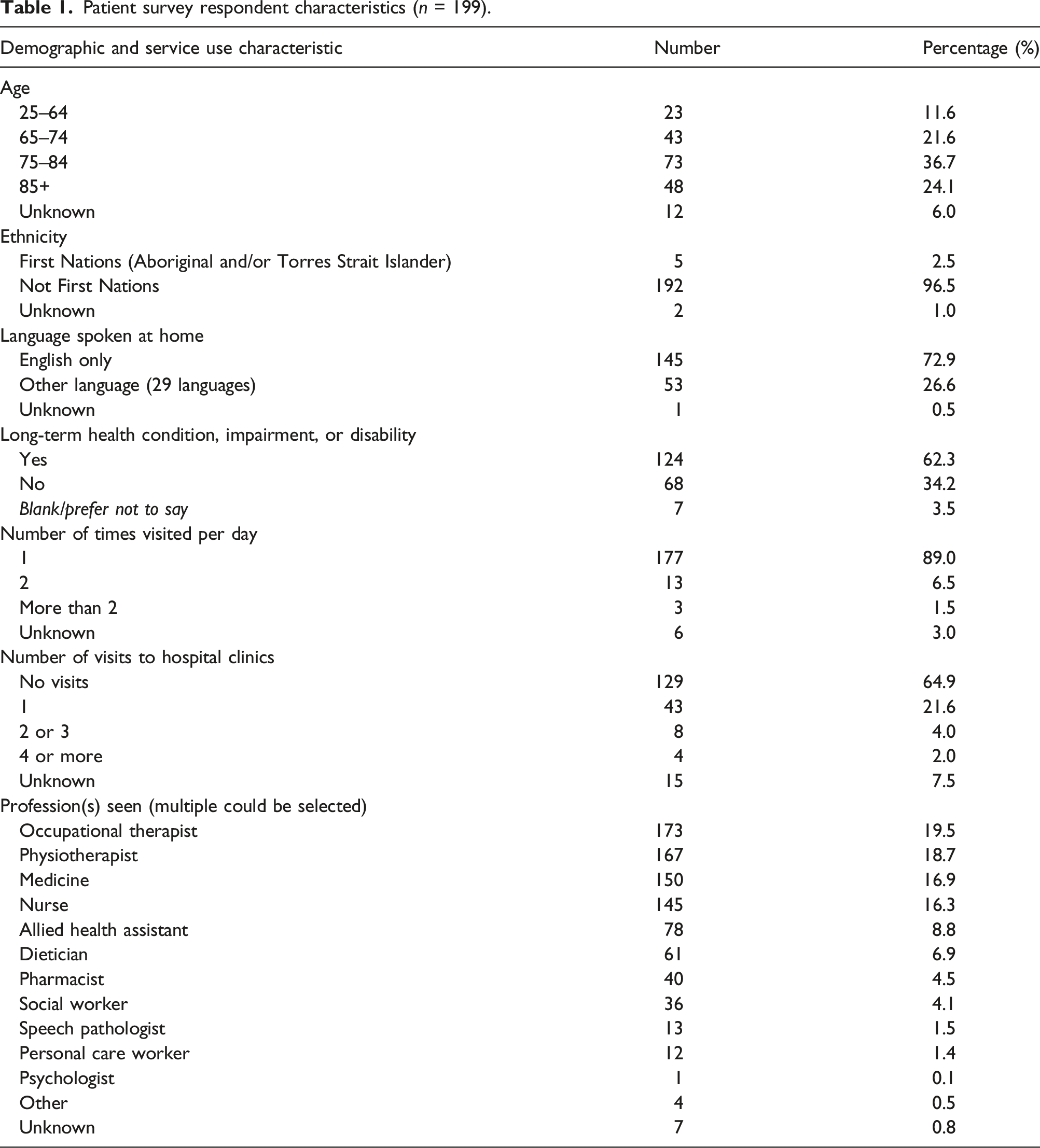
Most patients (n = 171, 85.9%) indicated a preference for GEMRHITH home care with 17 (8.5%) indicating hospital or home, and only seven (3.5%) preferring hospital. The main reasons for preference of home care location (participants could choose more than one reason) were convenience (n = 116, 58.3%), comfort (n = 112, 56.3%), and environment (n = 78, 39.1%). See Online Supplementary File S4 for further details.
Level of patient agreement with service statements.
A total of 180 patients (90.4% of respondents) provided at least one qualitative comment in the open-ended questions in the survey. Reflexive thematic analysis of 358 comments resulted in three themes. Patients who identified as culturally and linguistically diverse, or from a First Nations background, have been noted beside quotes.
It’s more comfortable and familiar at home
Many patients liked having services at home: ‘Lovely to get care and treatment at home’ (Bangladeshi). A relative of a patient who spoke Tagalog noted: ‘Easier for the patient to receive care from home as doesn’t speak English. Hospital was very confusing and distressing’. Being more comfortable at home was a frequent comment. Additionally, patients recognised the advantages of the GEMRHITH service for their recovery: ‘Very convenient and was able to rest in my own home, which was very important to me’. A Dutch patient alluded to gaining a more realistic idea of returning to life with their health condition by being at home. Being at home also provided more privacy and freedom.
Home was viewed as an easier venue than hospital from which to communicate with and receive support from relatives and friends. The son of a patient who spoke Gujarati noted the ability to easily visit his father at home compared to the hospital during a COVID-19 lockdown. Another patient’s relative wrote about difficulties phoning her loved one in hospital. The option for people to pop in, have a chat and help as needed was also reported. Receiving hospital-equivalent care at home reduced stress for relatives. Patients talked about reduced anxiety: ‘[It was] stressful if I was in hospital worrying about [my] husband at home’.
Conversely, the initial transition to home could be challenging. ‘At first, bit overwhelming but now I have become used to it’. Some patients noted that they were concerned about falling at home. One pointed out how reliant she was on her husband as her carer at home: ‘Sometimes worried if he gets unwell and no one home besides me’ (Cantonese). Not having a doctor physically nearby for medical emergencies was also a concern.
Convenient and supportive but sometimes challenging
The home visit model was generally perceived as being more convenient than visiting hospital. As one respondent said: ‘[GEMRHITH staff] came to me and [I] didn’t have to travel. Brilliant’. Multidisciplinary follow-up was reported as positive, including checking tablet-taking, exercise regimes, or identifying home modifications: ‘Very impressed … staff picked up other issues in the house such as needing grabrails’. Furthermore, some patients reported they liked the autonomy of being at home: ‘Being able to do what I wanted without having to wait for staff’ (Samoan).
It was noted that the service was well coordinated, and staff rang before visiting. However, some found it frustrating having to wait indoors for a scheduled home visit: ‘I disliked being in home, couldn’t go out’. Others reported staff not arriving when expected and not communicating when running late. The weekend service was reassuring, but at times the purpose of visits was questioned. A patient who spoke Cantonese noted that they sometimes became confused over which staff member was coming to visit them.
There were many positive comments about the service supporting family carers. The daughter of one patient said she appreciated ‘Having external health professionals helping me make decisions about my mum’s care and coping at home in her own home, rather than making the decision in hospital’. Conversely, the extra burden the service put on carers was an issue. In one case, the patient’s aged wife was his carer. He reported: ‘Wife is 90 years old and [it] was quite a lot sometimes for her’.
Expecting more care and more than one visit per day was noted by a patient (Serbian). There was also an expectation by some patients that the service length of stay be longer: ‘Seemed dismissive. I understood [the] service would be at least 10 days’. However, other comments were supportive: ‘Good transition to follow-up service. Made a big difference’.
Person-centred, caring, and clearly communicated
Patients noted with gratitude how person-centred the approach was and that the staff were kind and caring. One patient said: ‘Professional care and felt I was their main priority’. There were also complimentary comments about individual team members’ expertise, including that of the geriatricians, nurses, and psychologist.
The quality of communication was usually viewed as high: ‘Really, really good at explaining. Genuine and caring attitude, personal approach. It was beautiful’ (Torres Strait Islander). Beneficial and clear patient education was often remarked on, such as wound care and medication management. The right amount of repetition for understanding was noted, but conversely too much repetition was reported: ‘A lot of people repeating themselves … could have been more efficient’. Written handouts were regarded as useful: ‘Written information [was] set out in plain English that could be understood’. However, others noted that service handouts had ‘a lot of irrelevant info, and forms [were] given with limited explanation of what they were for’. Additionally, a patient remarked: ‘Confused, regarding all the information that was given, unsure which number to call’ (Persian). In another case, a patient complained: ‘Nothing was written and hard to remember everything’ (Dutch).
Staff interviews
Staff were from a range of professions, with five being physiotherapists (31.3%), three occupational therapists (18.7%), two geriatricians (12.4%), two nurses (12.4%), and the remaining four being a dietician, a pharmacist, a psychologist, and an administrator. The higher number of physiotherapists and occupational therapists reflected the rotational nature of those positions (three to 6 months, and nine to 12 months, respectively). Most staff (62.5%) worked full-time and had experience working with older or rehabilitation clients (87.6%). A table detailing staff participant characteristics is included in Online Supplementary File S5.
Reflexive thematic analysis resulted in four themes. The interviewees are designated P1, P2, etc.
Inclusive responsive service, hospital beds the driver
Participants felt that GEMRHITH could facilitate quick transfers to home. ‘We can accept patients really quickly … there’s a lot of flexibility in the service’ (P2). This flexibility enabled the service to be person-centred and provide specialised support to patients who otherwise would stay in hospital for safety reasons: A large population of people with different kinds of diagnoses and issues, ranging from dealing with dementias to people with chronic illnesses … what our service is really good at is, I guess, identifying what those needs are and the risks and the education that's needed for family and patients themselves, and to keep them kind of safe (P3).
Another positive factor identified by interviewees was GEMRHITH’s ability to provide families with an opportunity to trial care at home with multidisciplinary support, rather than discharging patients against medical advice. Interviewees also mentioned the ability to include patients who would not fit the criteria for traditional rehabilitation services, such as people with advanced dementia. These were the patients ‘no other service will take [and] who the family want to look after … because they don’t necessarily have rehabilitation goals’ (P12).
Conversely, there were challenges in accepting patients when the acute HITH service, which shared nursing staff, was at capacity. An interviewee reported that decisions about admissions ‘are not made in just the patient's best interest or … to free up a bed on the hospital ward. It’s made based on staffing levels from our nursing side’ (P2).
Many benefits from the home environment
There was universal acknowledgement of the many benefits to patients being at home, which was usually the patient and family preference. ‘Often, we feel, as clinicians, that people are better under our care in hospitals. But, actually … they prefer to be at home’ (P11). Staff believed patients were more comfortable, confident, independent, and slept better at home. ‘I’ve actually seen them on the ward … and then have gone and seen them the next day in their home and it's been like a completely new patient’ (P2). Patients with specific needs, such as culturally diverse backgrounds, benefitted greatly from being at home: They wouldn’t thrive in that setting [hospital], because they’re not around people and their supports … where their communities are really important to them, and actually help them with rehab (P13). [GEMRHITH ] allows that support to go home, and either be successful or fail one more time … that allows family and patients to kind of have that one last chance mentality ... carer training… and helping set up equipment (P2).
Collaboration with the hospital critical to success
Staff believed the close involvement of hospital staff in service development followed by ongoing links were key factors for service success: It’s very valuable having on-the-ground clinicians being involved … [in] higher level discussions, to help give the service realistic goals and capture the right type of patients (P12). Operating out of [the hospital] is really important from a handover view, from a risk-assessment point of view, but also just for that congruency of care … Those links with the people in the hospital that help, basically, discharge to happen effectively … to stop people from coming back to the hospital (P3). I think what really works well is having that one foot in the door at the hospital and one out in the community (P16). It makes the service more efficient, having a base at the hospital, because it enables those clinicians to more easily identify and pull patients from the ward and communicate with the ward staff (P10).
Comprehensive multidisciplinary model provides holistic care
Participants reported that the inclusion of a geriatrician, a broad range of allied health disciplines, and a strong nursing team meant the GEMRHITH model was comprehensive and holistic. Staff believed patients and families appreciated this range of expertise: I hear feedback from family members all the time saying it's great how they can get access to a dietitian, physio, OT, a geriatrician, which is quite rare … [A] psychologist is an invaluable thing to have (P3). Having that geriatrician available, if [a patient has] fallen over or they’ve got a new medical issue, being able to just get straight on the phone and call them, is reassuring for the patient and is more efficient for the health service’ (P12).
However, many positions were part-time due to funding limitations and the service size. Hence, part-time and shift work arrangements sometimes interfered with team communication and an up-to-date picture of the patient journey: We’re not getting everyone coming to the handovers … So, a lot of the times, not everyone in the team will know the patients and know what’s happening (P7).
The physiotherapists and occupational therapists were the only full-time day-shift clinical staff in GEMRHITH. Consequently, they adopted a case-coordination role, which, whilst beneficial, was seen as a service gap: ‘An allocated person, that could oversee a bit of the case management stuff [would allow the physiotherapists and occupational therapists] to focus more on the rehab’ (P1). A heavy reliance on the allied health assistant to follow-up on therapies and team recommendations was seen as a service strength, although a full-time position would add more value.
The advantages and disadvantages of combining nursing staffing from acute HITH and GEMRHITH were discussed. One positive was that it provided cover when an assigned nurse ended their shift or was otherwise unavailable. But not all nurses were satisfied with working in GEMRHITH. Some expressed concern ‘… that their job or job that they had not signed up for, was changing … it’s a completely different type of patient that we’re getting’ (P2).
Discussion
To our knowledge, this is the first exploration of staff and patients’ perceptions of a combined geriatrician-led, multidisciplinary geriatric evaluation and management and rehabilitation HITH service for adults of all ages and across multiple medical and surgical diagnoses. An additional strength is that the research team included a consumer partner with relevant lived experience and ongoing advice from a carer of a patient who used the service.
Whilst the GEMRHITH model emerged from an organisational need to optimise patient flow and ease inpatient bed-pressures, these findings suggest that the service overwhelmingly met stakeholder expectations. Themes highlighted patient preference for the service over traditional inpatient care, along with the many advantages of receiving home-based geriatric evaluation and management services and rehabilitation services, with access to a wide range of multidisciplinary team members. These sentiments are consistent with previous studies evaluating acute HITH models, particularly for older persons. 4 A specific strength of the GEMRHITH model is its scope to target sub-acute goals with patients experiencing a broad range of medical and surgical diagnoses, compared to traditional acute HITH models.
Patients and staff recognised that the GEMRHITH model enabled increased patient comfort in a familiar environment, and was generally more predictable, convenient and person-centred. Staff indicated that the model enabled a more realistic assessment of people’s functioning. This aligns with Levine et al., 17 who reported that interacting with a patient in their home (via an acute HITH service) provided greater opportunities to tailor care to the individual’s lived experience and establish more meaningful connections between patients and staff.
The benefit of supporting patients from diverse backgrounds was emphasised by staff and the many positive comments from patients who spoke languages other than English. In particular, the ability for diverse patients to be surrounded by a familiar environment, language, and for carers to be present during staff visits and included in care planning was perceived as advantageous. The literature recognises such factors as facilitators for improving health equity and access in HITH service delivery.2,10
An important theme in patient and staff responses was patients/families having greater control and ownership of their care in the GEMRHITH model. Previous evaluations of acute HITH models have discussed the impact of patient locus of control on the success of these services. A metasynthesis by Chua et al. 4 reported that HITH models that facilitated patients’ involvement in their own care promoted patient empowerment, created positive relationships with the care team, and increased overall satisfaction. It is clear, however, in the current study, that promoting patient control is not suitable for all patients as some may prefer to leave care responsibility with hospitals. Some patients expressed specific concerns regarding falls risks, and anxiety regarding the initial hospital to home transition, which has been reported elsewhere. 7 Thus, the HITH model may cause increased burden for some patients and their caregivers/family members.14,28 Future improvements to HITH models could include technology to mitigate safety concerns, such as falls/medical emergency alarm systems 21 and remote monitoring. 11 Previous studies have also acknowledged that, to date, most HITH services (including the GEMRHITH model) do not have specific support structures to recognise and mitigate caregiver stress associated with increased care burden.4,11,16,19 This is an important area of further research and service model optimisation.
A key area of perceived GEMRHITH success was the holistic nature of care – incorporating medical, nursing and allied health input – and the linkage of teams and services across hospital and community. The importance of close links with the hospital and of inpatient staff having confidence in the service was highlighted in this study and in others.7,9 Staff said the GEMRHITH model also provided a unique opportunity to cross traditional service delivery boundaries.
Whilst some respondents welcomed the opportunity to provide a more interdisciplinary service, others acknowledged that operational constraints, fiscal/resource limitations, and staff rosters negatively impacted their satisfaction and ability to run the service effectively. Communication and collaboration among health professionals is an essential aspect of the hospital to home transition, and thus HITH services must ensure continuity and quality of care.4,7,21
Previous studies have acknowledged that inter-professional collaboration, coordination, and communication were common challenges for HITH models as these services require organisations to shift away from traditional siloed practices, reorganise the structure of care delivery, and maximise home visit efficiency.9,28 The ability to effectively recruit/train multidisciplinary staff with sufficient generalist skills to service the clinical heterogeneity of HITH patients, whilst also enabling the effective management of complex cases is a significant challenge.29,30 This is worthy of future investigation, especially for services that combine several sub-speciality areas such as acute, rehabilitation and geriatric evaluation and management services.
The greatest area of improvement for the GEMRHITH model related to enhanced communication between staff and patients/families, particularly surrounding expectations of the scope of the service and educational resources. Previous studies have identified that effective communication between care teams and patients/families is essential in enhancing patient confidence towards HITH models. 28 As discussed in the literature, 2 further work may be beneficial to streamline and coordinate how information is relayed among all stakeholders (patients and staff) to optimise delivery and satisfaction with the GEMRHITH model. A key-worker model was discussed as an enhancement by staff and has been recommended elsewhere. 9 Future investigation into the health literacy needs of patients and the capabilities of staff to meet them is also required.
Limitations
Six main limitations to the current study are acknowledged. First, potential response bias is acknowledged due to the convenience sample in both the patient and staff cohorts. It could be the case that we simply did not reach those patients and staff unhappy with the programme.
Second, to improve response rates and to support culturally diverse patient engagement, the majority of patient surveys were facilitated and completed over the phone and 22.5% completed by staff on behalf of patients or carers/family members. This may have introduced a degree of acquiescence bias in the cases where a prior relationship existed between patients and interviewers. Additionally, the lack of funding for interpreters to assist with telephone surveys may have added to this bias, as responses were obtained from bilingual patients or through a family member interpreting. Similarly, despite the interviewer being independent of clinical services, and raw data being deidentified, it is possible that staff did not discuss team challenges in detail as they were aware that some of the research team were clinicians or service managers.
Third, whilst the timing of the patient surveys at point of discharge is a relative strength, staff interviews may have been impacted by recall bias, as some staff had moved out of the GEMRHITH service at the time of interview. Additionally, staff redeployment and furlough cover requirements due to the COVID-19 pandemic may have disproportionately reduced nursing participation, as the community service through which they reported provided a COVID-HITH service which was in high demand.
Fourth, the sample was obtained from a single Australian metropolitan health service, thus the generalisability of findings may be limited.
Fifth, the service model did not include patients who resided in residential aged-care facilities, and this is an area of need for further HITH service expansion and research. 13
Sixth, some potentially interesting data were not collected. The gender of respondents and details of their long-term conditions, impairment, or disability were not recorded.
Conclusions
This study provides the first qualitative exploration of staff and patients’ perceptions of a geriatrician-led, multidisciplinary sub-acute GEMRHITH service. The perspectives of a consumer co-investigator and a consumer advisor strengthened the consumer voice in the study.
Participants reported that the model provided patient-centred care that was convenient, comfortable, and optimised patients’ recovery, control, and ownership of care. Additionally, GEMRHITH may have been particularly advantageous to patients from culturally diverse backgrounds. Access to a team approach and the inclusive service parameters for all adults with geriatric evaluation and management or rehabilitation goals ensured responsiveness to diverse needs whilst facilitating early discharge home from the hospital. Many carers described having their loved one at home as advantageous, but carer burden and stress was also identified, and this warrants further research.
Areas for improvement centred around clear communication regarding service parameters and enhanced patient education materials and strategies.
Supplemental Material
Supplemental Material - Patient and multidisciplinary health professional perceptions of an Australian geriatric evaluation and management and rehabilitation hospital in the home service
Supplemental Material for Patient and multidisciplinary health professional perceptions of an Australian geriatric evaluation and management and rehabilitation hospital in the home service by Ruth Cox, Greg Kyle, Anya Suzuki, Laurelie Wishart, Melissa McCusker, Alexander McConnell, Elizabeth C Ward, Leo Ross, and Clare Webb in Journal of Health Services Research & Policy.
Footnotes
Acknowledgements
Thank you to Salvatore Spoto for his consumer perspectives and advice regarding this study and to Dr Amanda Siller, Dr Alicia Wu, Victoria Tilby, and Sally Courtice who were all integral to development of the service.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The project received ethical and site governance approvals (HREC/2021/QMS/69168) and staff interview participants provided written informed consent.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.