
Abstract
Objective
Research exploring the enablers and barriers that exist for military veterans seeking to address their poor mental health has produced ambiguous results. To identify the enablers and barriers correctly, this study systematically reviews the literature, including research that included alcohol and had a clearly defined veteran population.
Methods
Six databases were searched. Inclusion criteria specified that empirical studies related to veterans that had ceased military service and were seeking help for poor mental health and/or alcohol difficulties. Critical Appraisal Skills Programme and AXIS appraisal tools were used to assess quality and bias. A narrative synthesis approach was adopted for analysis. From 2044 studies screened, 12 were included featuring 5501 participants.
Results
Forty-four enablers and barriers were identified, with thirty-two being statistically significant. Post-traumatic stress disorder had the greatest number of enabler/barrier endorsements to veterans seeking help. Depression, anxiety, experience and attitudes also acted as enablers/barriers. Most studies were of fair methodological quality. Limitations included that samples were skewed towards US army veterans. Little research exists concerning those that have ceased military service.
Conclusions
Veteran help-seeking is likely enabled by poor mental health symptomology and comorbidity, which suggests veterans reach a crisis point before they seek help. Further research on alcohol misuse and attitude formation is required. The field would also benefit from alternative study designs including qualitative studies with non-US participants.
Introduction
Existing veteran mental health (MH) literature suggests veterans have a greater vulnerability towards mental illness than the general population. When Rhead et al. 1 compared UK veterans with the general population and found veterans were 30% more likely to suffer from common MH disorders. One explanation relates to elevated levels of career-specific trauma exposure encountered by veterans.2,3 Veterans were nearly twice as likely to suffer post-traumatic stress disorder (PTSD) and alcohol problems when compared with the general population. 1
Jones and Fear 4 reported that the military has a long history of considering alcohol as a ‘cure-all problems’ substance. Historically, alcohol was handed to soldiers to relieve the anxieties associated with difficult and traumatic combat situations. Over time, alcohol within the military became normalized and was consumed excessively for stress management, commemorations, celebrations, peer bonding, pain management, insomnia and relaxation. Normalized military-shaped beliefs and attitudes often cascade into veteran life; thus, alcohol may continue to be consumed excessively post-military service. 5 In their profile study of 600 help-seeking UK veterans, Murphy et al. 6 found that while 43% reported problematic alcohol use as their main MH difficulty, 93% suffered alcohol issues comorbidly with two to three other MH problems. These findings suggest excessive alcohol use is an issue for many veterans, in the context of other mental illnesses.
Particularly within military culture, help-seeking for poor MH and problematic alcohol use is often delayed or avoided. According to a review by Hom et al., 7 approximately only one-third of the armed forces community globally engages in help-seeking via health care or professional organizations. This is not to suggest that only one-third of this population needs to seek help but, rather, there may be many more who could benefit from help-seeking but who choose not to. In any event, global veteran help-seeking figures are unlikely to be entirely accurate, as much help-seeking research is conducted in the US where veterans have a different health care system to other countries (e.g. UK and Australian veterans often use channels that would not necessarily recognize or record them as veterans).
However, it is generally reported across the literature that help-seeking rates are relatively low for veterans. 8 Several reasons for this have been proposed. For one thing, aside from alcohol being (potentially) a barrier to adaptive help-seeking, veterans may also delay or avoid seeking help due to military ideology and veteran culture. Research indicates that help-seeking may be inhibited by veterans’ strong sense of pride and a fear of stigma.9–12 An alternative explanation is that veterans have limited knowledge or negative attitudes towards MH. 13 A 2017 review by Kantor et al., 14 which included participants from the armed forces, found that limited MH knowledge was a barrier to help-seeking. The Health Belief Model 15 proposes that attitudes towards symptoms and treatment can enable or hinder help-seeking; therefore, it could also be that veterans have had negative treatment experiences on occasions when they did seek help, in turn reinforcing their negative attitudes towards care. Poor help-seeking experiences have been suggested as potential barriers to future help-seeking for veterans.7,16 Johnson and Possemato 17 found that cognitive predictors, such as problem recognition and treatment beliefs, were linked to support service use over and above practical factors. Rafferty et al. 18 also found problem recognition was a key barrier to help-seeking.
While the existing literature does indicate that some veterans avoid seeking help, there are many veterans who do seek support. Murphy et al. 6 found that a main motivator for help-seeking in UK veterans was severity of poor MH symptomology, particularly PTSD. It was not necessarily the presence of PTSD symptoms that enabled help-seeking but rather the extent to which the symptoms impacted the veterans’ ability to function and quality of life. A further potentially salient enabler of help-seeking is positive social support. 19 When others within a positive support network recognize the signs of poor MH, they often offer a veteran the requisite encouragement and assistance (physical and emotional) to seek support. 20
Previous systematic reviews have been conducted to explore enablers and barriers to veterans’ help-seeking (see online Supplement). But these have often produced inconsistent findings. One possible explanation for this could relate to mixing military-affiliated populations within the same review. For example, in the US the definition of a ‘veteran’ is often someone who has been operationally deployed, whereas in the UK it is someone who has ceased military employment. 21 Arguably, a deployed (yet still employed) veteran faces different barriers and enablers to a retired veteran. An employed veteran may suffer workplace stigma 22 as a barrier, whereas a retired veteran may experience support access barriers. 14 Randles and Finnegan’s review 23 concluded that research based on the US-veteran definition lacks generalizability to other veteran populations, which, in turn, is a limitation for reviews that include both US and non-US veteran studies.
A further source of inconsistency relates to alcohol. There is a lack of agreement over whether alcohol is a barrier to help-seeking. Some reviews failed to include alcohol altogether,23,24 despite the literature suggesting that MH and alcohol misuse are linked. A final critique relates to the appropriateness of mixing quantitative and qualitative methodologies within the same review. Several mixed-method reviews provided no details of study design or justification for mixing the methods, meaning it was difficult to assess the quality of the reviews.25,26
To our knowledge, the current systematic review is the first to include alcohol within the context of help-seeking enablers/barriers for veterans who have ceased military employment.
The purpose of this study was to address two questions: (1) What are the barriers and enablers to help-seeking for veterans having ceased military employment, for those with MH and/or alcohol issues (comorbid or otherwise)? (2) How many enablers and barriers exist?
Methods
We followed the Centre for Reviews and Dissemination’s guidance regarding search strategy development, inclusion and exclusion criteria, quality assessment, data extraction and data synthesis. 27 A systematic review protocol was registered on PROSPERO, reference CRD42021227097. 28
Eligibility criteria
Studies were considered for inclusion if they met the following criteria: ⁃ Not currently serving personnel. The target population was defined as veterans consistent with the UK definition of a veteran.
21
Reserves were excluded, as they could technically still be classed as serving. ⁃ Featured or measured enablers and barriers to help-seeking contact or initial service use. Support services were either MH-specific and/or could assist MH indirectly. ⁃ Included measures of MH and alcohol to assess if these variables affected help-seeking. ⁃ Retrospective (‘would you consider help-seeking?’) or actual help-seeking behaviour (did/did not help-seek). ⁃ Measured correlates of actual or retrospective help-seeking behaviour. ⁃ Quantitative study designs.
Exclusion criteria included the following: ⁃ Non-veteran populations (an exception to this was where the general population was considered as a comparison group). ⁃ Long-term, repeated service use or attrition studies, as long-term service use is not considered comparable to the more initial stages of help-seeking. ⁃ Studies featuring general substances, which did not differentiate alcohol misuse. ⁃ Non-English studies not using primary data collection and non-peer reviewed papers. ⁃ Qualitative studies.
Selection process
CH electronically searched six databases on 21 December 2020 and again on 1 December 2021. For search inclusivity, no ‘search from’ date was included in the initial search, whereas the second search spanned 21 December 2020 to 1 December 2021. Databases were PsychINFO, Medline, Embase, CINAHL, SCOPUS and PILOTS. Keywords used within the literature search related to veterans, help-seeking, enablers, barriers, mental health and alcohol (see online Supplement for the full search strategy).
CH screened the sources identified. The screening process was piloted with a random sample of 20 studies. All titles and abstracts were screened, followed by full-paper eligibility checking. The reference lists of included articles were also screened for inclusion. A subset of 10% was cross-checked by PT at each stage.
Bespoke data extraction sheets were created, to extract information relating to study objectives, participants, study design, outcomes, results, discussion, generalizability, limitations, funding and ethics. Data extraction sheets were piloted to test suitability. CH extracted all relevant data from included studies, which were checked by PT.
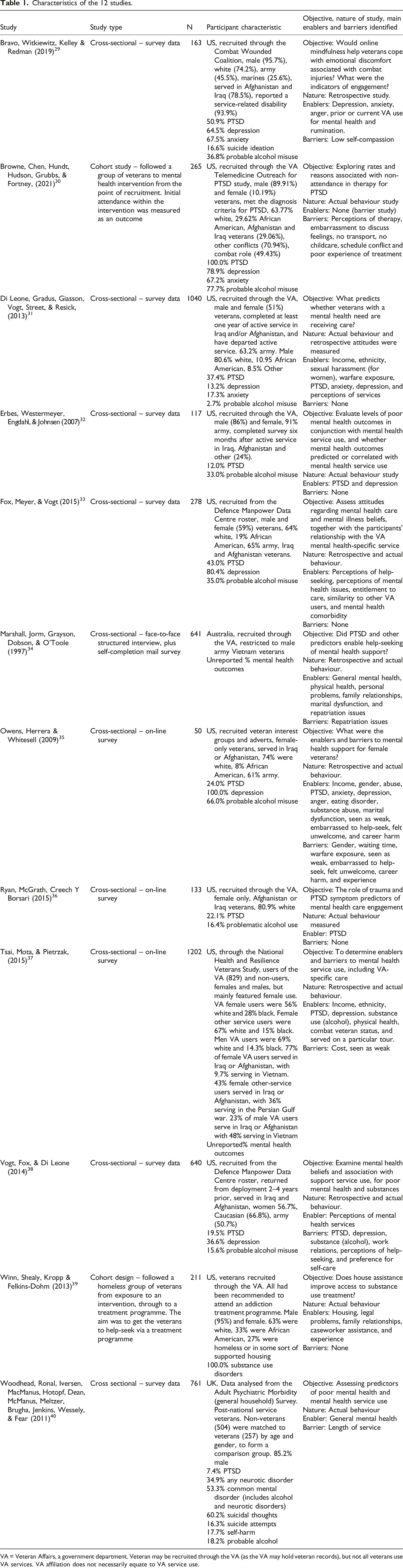
The literature search identified 2044 results. After removing 154 duplicates, 1890 titles and abstracts were screened. A full paper review was conducted on 253 papers, and 12 articles were selected for inclusion (see Figure 1). Details of the 12 included studies29–40 are summarized in Table 1. Flow diagram on study selection. Characteristics of the 12 studies. VA = Veteran Affairs, a government department. Veteran may be recruited through the VA (as the VA may hold veteran records), but not all veterans use VA services. VA affiliation does not necessarily equate to VA service use.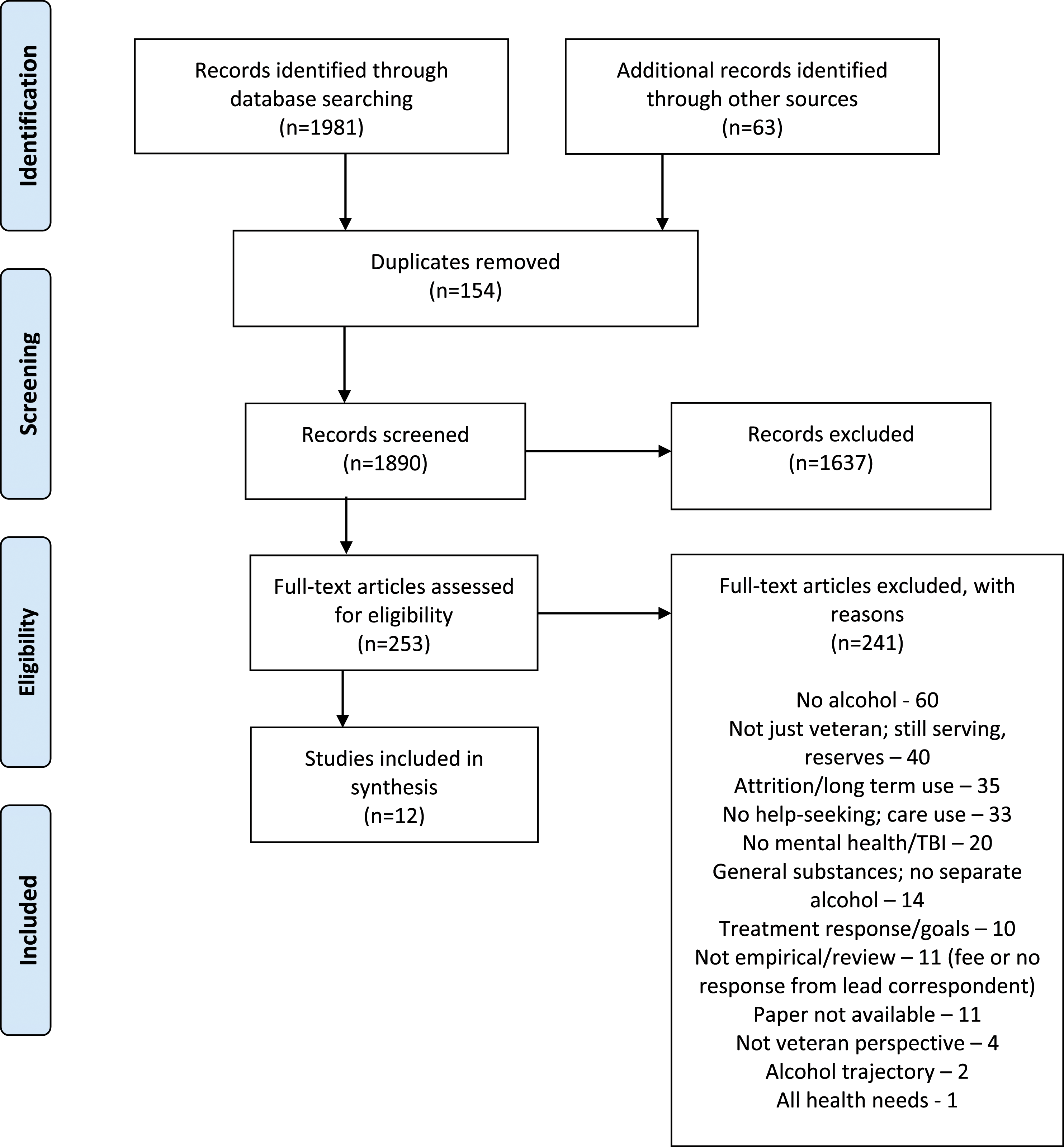
Enablers and barriers.
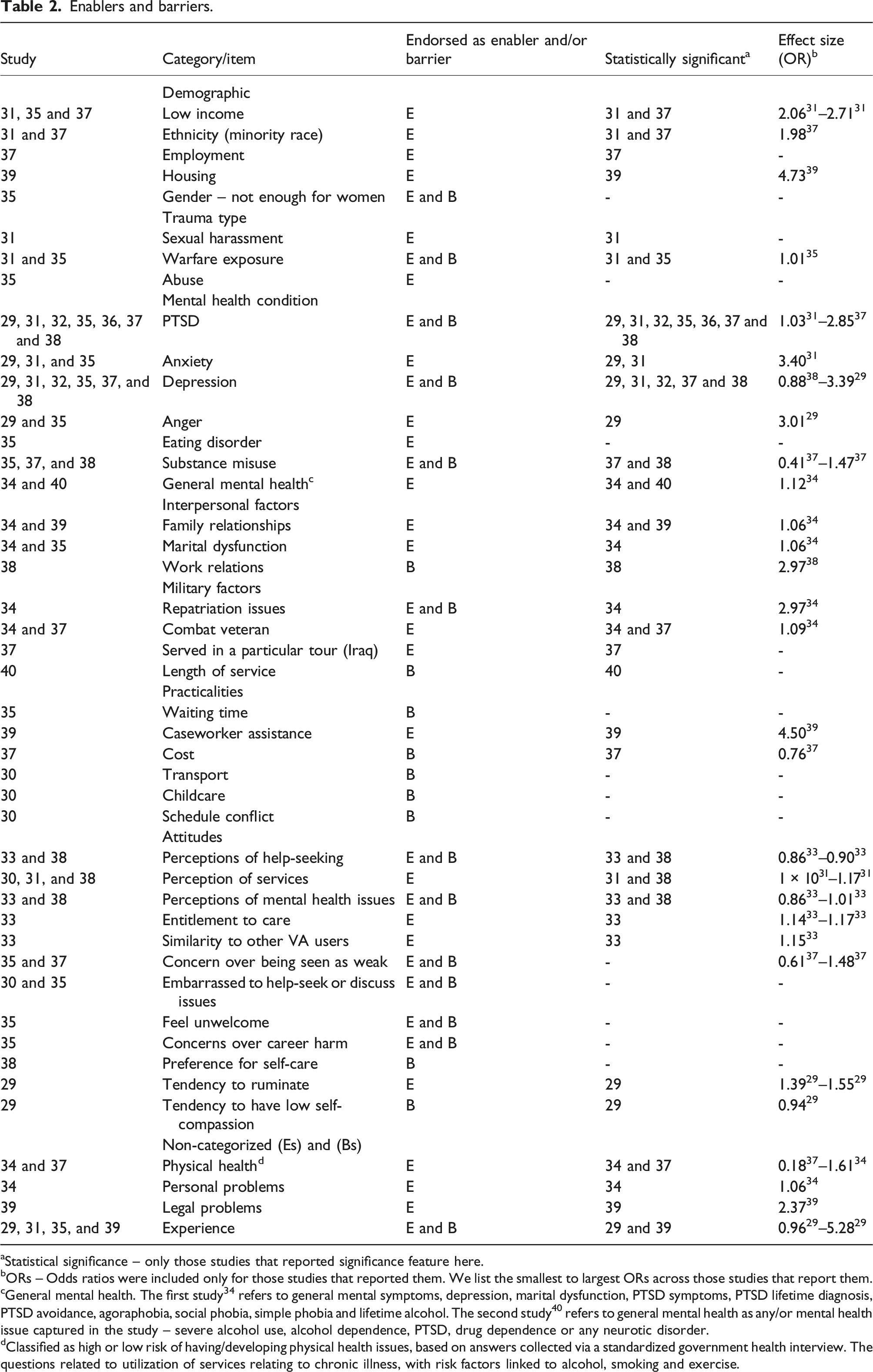
aStatistical significance – only those studies that reported significance feature here.
bORs – Odds ratios were included only for those studies that reported them. We list the smallest to largest ORs across those studies that report them.
cGeneral mental health. The first study 34 refers to general mental symptoms, depression, marital dysfunction, PTSD symptoms, PTSD lifetime diagnosis, PTSD avoidance, agoraphobia, social phobia, simple phobia and lifetime alcohol. The second study 40 refers to general mental health as any/or mental health issue captured in the study – severe alcohol use, alcohol dependence, PTSD, drug dependence or any neurotic disorder.
dClassified as high or low risk of having/developing physical health issues, based on answers collected via a standardized government health interview. The questions related to utilization of services relating to chronic illness, with risk factors linked to alcohol, smoking and exercise.
The quality of each study’s research method was assessed via two critical appraisal tools: the Critical Appraisal Skills Programme (CASP) for assessing cohort studies 41 and the AXIS 42 tool for assessing cross-sectional studies. The Equator website 43 was also referred to regarding reporting transparency and quality of health research. A quality assessment matrix was created based on the CASP and AXIS indicators of quality, 44 with each study awarded a score out of 25. CH assessed the overall quality of the research, with PT cross-checking a 10% subset.
Results
Study characteristics
Ten studies were cross-sectional,29,31–38,40 with the other two30,39 being cohort studies. Only one study 29 was solely retrospective regarding help-seeking.
Ten out of the twelve studies29–33,35–39 were from US, conducted with Iraq and Afghanistan veterans. Although these were US studies, the personnel in these studies nevertheless conformed to the UK definition of a veteran. Of the two remaining studies, one was Australian 34 and the other United Kingdom. 40 In total, the studies included 5501 participants, with 4099 (74.51%) participants being US veterans and 2014 (36.61%) identifying as serving in the army. Males accounted for 3329 (60.52%) of all participants, and Caucasians were represented by 2768 (50.32%). Not all studies reported each demographic described here. Six studies30–32,34,36,39 recruited participants via the Veteran Affairs (VA) administration, amounting to 2290 (41.63% of all participants). Across all studies, the proportions of participants that were reported as having likely or actual MH and alcohol difficulties were PTSD 7.4–100%, depression 13.2–100%, anxiety 17.3–67.5% and alcohol misuse 2.7–77.7%. One study 39 reported 100% of the population were misusing substances, but it is unclear how many experienced alcohol misuse.
Enablers and barriers
All the studies, bar one, 30 identified enablers. Seven studies29,30,33,35,37,38,40 identified barriers. See Table 1 for a full list of enablers and barriers.
The total number of individual enablers and barriers was 44. Thirteen barriers and enablers were regarded as both barriers and enablers, including PTSD and repatriation issues. Thirty-two barriers/enablers were statistically significant.
The most common MH conditions found to predict help-seeking were PTSD (most frequently occurring predictor), depression (strongest MH predictor, OR up to 3.3929), anxiety and substance misuse: • PTSD (presumed or actual) significantly predicted help-seeking across seven studies.29,31,32,35–38 Two further studies34,40 found ‘general’ MH was a significant enabler, with PTSD being captured within general MH measures. One study
32
reported that PTSD was the most significant predictor when controlling for all other correlating variables. Another study
29
found PTSD symptom severity acted as a help-seeking enabler. However, one study
38
suggested that when PTSD correlated with negative beliefs help-seeking reduced – therefore, PTSD was considered to act as a help-seeking barrier within this study. • Depression was found to be a help-seeking enabler or barrier across six studies.29,31,32,35,37,38 Five studies29,31,32,35,37 suggested that depression predicted help-seeking and acted as an enabler. One study
38
found that depression acted as a barrier when correlated with negative beliefs. • Anxiety was found to be a help-seeking enabler across three studies.29,31,35 • Substance misuse predicted help-seeking across three studies.35,37,38 In one study,
35
general substance misuse predicted help-seeking, but alcohol specifically did not. Alcohol was a significant enabler in one study.
37
Yet, alcohol was a significant barrier in another study
38
when correlated with negative beliefs.
Experience had the strongest (enabling) effect on help-seeking, increasing the odds of help-seeking by up to 5.2829 times. Housing or caseworker assistance also had a large enabling effect (ORs 4.73 and 39 4.50 39 ). Low income31,35,37 (enabler), repatriation 34 (enabler/barrier) and work relationships 38 (barrier) saw similar effect sizes of approximately three times on help-seeking. Regarding MH and alcohol outcomes, anxiety had the greatest enabler effect (OR 3.40 31 ), followed by depression (OR up to 3.39 29 ), PTSD (up to OR 2.8527), and substance misuse (up to OR 1.47 37 ).
Other regularly occurring individual enablers/barriers to help-seeking were experience of service use and perception of mental health services. Experience of service use was endorsed across four studies,29,31,35,39 as both an enabler and barrier to help-seeking. Perception of mental health service use was endorsed across three studies30,31,38 as a help-seeking enabler.
The final individual item, with three endorsements (as an enabler), was income.31,35,37 The remaining 38 individual enablers and barriers were endorsed by one or two studies only.
We found we could aggregate forty one of the enablers and barriers into seven categories: demographic factors, trauma type, mental health condition, interpersonal factors, military factors, practicalities and attitudes. The remaining four uncategorized enablers and barriers were physical health, personal problems, legal problems and experience
The attitudes category contained the most individual enablers and barriers – twelve different help-seeking enablers and barriers were reported across seven studies.29,30,31,33,35,37,38 Within the category of attitudes, perception of services had the most enabler endorsements, with MH-specific rumination having the largest enabler effect (OR 1.55 29 ). Also, within a single category, attitudes had the most items that were endorsed as both help-seeking enablers and barriers (six items30,33,35,37,38).
Quality and robustness of research
We assessed the methodological quality of most of the 12 studies as fair, with overall scores ranging from 11 to 19 out of 25. The details are given in the online Supplement.
All studies provided clear objectives and described appropriate study designs to investigate those objectives. All studies clearly defined their participant populations, but there were differences in the populations recruited (e.g. MH status and deployment location). All studies collected quite detailed demographic information, but this varied across the studies concerning what was collected and how it was measured (e.g. education, income, employment and ethnicity were measured differently). Four studies33,35,36,38 asked what MH issue(s) had prompted participants to engage in help-seeking.
We turn our attention now to the 10 cross-sectional studies. Only one study provided sample size calculations. Likewise, only one study 38 oversampled women to create even gender ratios. Six studies30,31,33,34,35,39 featured a sample that had entirely screened positive for MH issues, had received a positive MH diagnosis, or who were actively help-seeking for MH difficulties. Three studies33,34,38 mentioned randomization, which apparently related to participant selection, yet no study confirmed how randomization of participation occurred.
All 10 cross-sectional studies used questionnaires that were distributed in various ways (mail-back, web-based and face-to-face). The questionnaires utilized varied, totalling 41 different scales (see online Supplement for details). Most scales were valid and reliable. Two studies33,38 used adapted scales and reported alpha scores to demonstrate scale reliability. Most studies29,31,33,35,36,38,40 reported cutoffs for all scales used where relevant (e.g. clinically relevant levels of MH condition), whereas some32,34,37 reported no cutoffs or only for some of the scales. Several studies32,34,37,40 had omitted some details of scale/scoring administration; thus, it was not possible to assess that the measurement instruments had been administered correctly.
All 10 cross-sectional studies, apart from two,29,30 provided overall response rates together with reasons for dropouts. Despite some studies29,32,35,36 having low response rate sample sizes, the sample size was deemed to be acceptable by the authors of those studies. Sample sizes also seemed comparable with similarly published studies. Three studies31,33,38 statistically compared responders with non-responders, to check for response bias. All studies, aside from one, 30 reported statistical significance; one study 30 described its findings in relation to frequencies rather than statistical analysis. Three studies30,32,35 did not report confidence intervals or odds ratios for the analysis conducted. One study 37 set the confidence interval at 99% to improve the robustness of findings.
Regarding the two cohort studies,30,39 both included an intervention with separate conditions. However, it is unclear whether the studies had a within-participant or between-participant design. The studies inferred that participants could partake in all conditions, but this was not clearly reported. Therefore, it is unclear whether any randomization of conditions occurred.
Across all 12 studies, there was an inconsistency in the reporting of effect sizes (ORs) linked to enablers/barriers. ORs were only reported within studies29,31,33,34,36,37,38,40 (see Table 1 for the dispersion of reported effect sizes).
Discussion
This is the first review to identify enablers/barriers to help-seeking for veterans who have completely ceased military employment, in the context of alcohol as well as other MH difficulties. The inclusion of alcohol as a potential barrier/enabler is important as it often appears with other MH issues. Also, the specific definition of a veteran adopted in this review is salient as the term veteran differs globally, 21 which has implications for what is considered an help-seeking barrier/enabler. Forty-four different enablers and barriers were identified, with 13 more enablers being recognized than barriers. While this is contrary to Kantor et al.’s 14 review findings, who reported that more help-seeking barriers than enablers exist for veterans, our result is unsurprising as the focus of help-seeking research has shifted towards enablers over recent years.
Regarding individual enablers and barriers predicting help-seeking, PTSD was the most frequently endorsed enabler across not only MH conditions but also across all studies reviewed. This is to be expected, as research is often driven by the perspective that military veterans and PTSD difficulties are synonymous, 45 which has created a PTSD-focused agenda within veteran research. Existing research shows that it is likely functional impairment caused by symptom severity (frequently associated with PTSD specifically) that leads to veteran help-seeking.6,46 In this review, a veteran was up to three times more likely to engage in help-seeking if they had PTSD. While separate MH conditions were noted as individual barriers/enablers to help-seeking (and were mainly found to enable help-seeking – e.g. anxiety increased the likelihood of help-seeking by up to 3.5 times and depression up to 3.4 times), many studies found MH difficulties to be comorbid. This finding supports the view that veteran MH can be complex,3,6 and it is often comorbidity complexity with symptom severity that drives help-seeking. 39
Substance misuse, as an MH difficulty, was identified as impacting help-seeking; two studies found alcohol to be a significant enabler or barrier.37,38 However, where alcohol was found to be a barrier it was correlated with negative beliefs or a negative disposition. 38 Therefore, if beliefs were positive or negative beliefs were not included, alcohol would likely not be a barrier. One study 37 found that alcohol had a stronger predictive effect on help-seeking via the VA for male veterans than females, even when controlling for other covariates. It was suggested within this study that male veteran VA users were more likely to screen positive for a lifelong alcohol use disorder than females. Incidentally, aside from study, 39 it was difficult to distinguish whether participants were help-seeking for alcohol misuse specifically or other MH conditions, as few studies30,35,39 reported which difficulties were being sought help for.
We now look further afield, at studies that were not included in our review because they did not match our selection criteria (e.g. they were qualitative papers or used a non-UK definition of a veteran). Our review has produced a salient finding to suggest that alcohol is not necessarily a main enabler or barrier to veteran help-seeking, a finding which aligns with the literature that suggests alcohol is not found to act as a help-seeking barrier.47-49 A possible explanation could be that excessive alcohol use is associated with less functional impairment than, for example, PTSD symptoms, leading to a reduced perceived need for help. 48 Both Gribble et al. 50 and Hines et al. 51 found that where veterans may require support for problematic alcohol use specifically they may be less likely to help-seeking, due to a reduced sense of perceived need or problem recognition. A study that was included in our review, Erbes et al., 32 observed that heavy alcohol use could be associated with poorer quality of life in the domain of emotional dysregulation (and people may consume alcohol to manage the dysregulation). People with PTSD, in contrast, may suffer poorer quality of life and functional impairment in many other domains, thus prompting earlier help-seeking.
Other, more cognitive, factors were found to act as barriers and enablers to help-seeking. Experience of MH services (which in turn shapes feelings, thoughts and behaviours towards MH support services) had a high number of endorsements as enablers and barriers to help-seeking and the largest effect size. This finding was anticipated, as service experience has been found to predict help-seeking or future service use within the veteran community. For instance, several qualitative studies have investigated the process of veteran help-seeking and suggest that help-seeking is a journey that is motivated by mixed experiences.20,52–54 However, help-seeking is not necessarily linear, as poor help-seeking experiences (creating poor feelings, thoughts and behaviours towards service use) can cause veterans to stall or regress with help-seeking (i.e. poor experiences become help-seeking barriers). 18
Another cognitive factor relates to perceptions of services. Perceptions of services received three endorsements30,31,38 as an enabler to help-seeking, implying that positive perceptions of services are more likely to lead to help-seeking behaviour. This finding was mirrored by Johnson and Possemato’s 17 veteran cohort study of MH service use and attrition, which reported that treatment beliefs were a major enabler/barrier to service use. It could be inferred that positive perceptions of services are likely to be linked to positive service use experience, which impacts on the help-seeking journey and improves help-seeking motivation. 18 Positive perceptions also undoubtedly feed into positive health beliefs, causing positive health and treatment beliefs to act as a help-seeking enabler. Positive health and treatment belief leading to help-seeking is a core principle of the Mental Health Belief Model. 15
Perception of services is an example of ‘attitudes’ that may act as a barrier/enabler to help-seeking. Across the studies, a total of 12 separate enabler/barrier attitudes were identified, suggesting that attitudes, collectively, may act as a major barrier/enabler to help-seeking. This finding is unsurprising, as Johnson and Possemato’s 17 study relating to veteran support service help-seeking and attrition found that cognitive enablers and barriers had a greater impact than other, more practical, barriers. Johnson and Possemato found the strongest predictors of help-seeking were ‘attitude to the problem’ and ‘attitude towards mental health care’.
Further barrier/enabler attitudes identified through this review were a preference for self-care, being seen as weak, embarrassment and career harm. These enablers and barriers could be classified as military-shaped, stigmatized attitudes. Yet, several other non-stigmatized attitudes were also found to impact help-seeking in this review. Therefore, the view that it is fundamentally stigma as an attitude that impacts help-seeking is unsupported.10,16 Stevelink et al. 55 found in their study of help-seeking within the armed forces community that the third most cited reason for help-seeking was the realization they could not self-manage their issues, despite holding pro self-care beliefs. It is likely that symptoms had become so unmanageable that help-seeking was enacted despite holding stigmatized beliefs. Help-seeking could also be encouraged or arranged by the veteran’s social circle, while the veteran maintains their stigmatized beliefs. Johnson and Possemato 17 proposed that stigma can act as a barrier, but it is perhaps not the strongest barrier, as help-seeking occurs even in the presence of holding stigmatized beliefs and attitudes.
Surprisingly, social support was not found to be a main category in this review. Three studies29,31,34 included scales that could be classified as social support measures. The first 29 included a friendship scale, but found that friendship did not particularly support help-seeking and did not discuss this finding within the paper. The second 31 included a social support scale. However, that study was barrier-focused, and as social support is generally considered an enabler, it was not identified in the findings. The third 34 included measures of repatriation, family and marital relationships. That study found that repatriation issues acted as a barrier, whereas marital and family relations acted as help-seeking enablers. Repatriation into the community had a similar sized effect to PTSD, which indicates its salience. The limited social support endorsements identified do support social support themes elicited in the extant veteran help-seeking literature. Evidence of family and marital relations acting as an enabler has been found,19,20 together with help-seeking being enabled by wider community support via local repatriation. 56
The final enabler/barrier to help-seeking relates to income, which was endorsed as an enabler in three studies.31,35,37 We were not surprised by this finding; given that 80% of studies in this review were conducted in the US, where health care predominantly comes at a cost (albeit at a lower cost if via the VA 12 ). As such, veterans were nearly three times as likely to help-seeking if they had a lower income, suggesting that veterans probably used the VA as this was the most affordable option for them. The effect of low income on help-seeking via the VA was comparable in size to that of having likely PTSD; thus, it was a relatively important driver of help-seeking behaviour. Income would not necessarily be endorsed as an enabler in other countries (e.g. the UK or Australia), where veterans could be cared for through a nationally available (largely free) health care system. That is not to say income is not potentially a barrier to those with access to free services. Those that reside in rural areas may have access issues such as transport costs. Access to services may also be more difficult where some preferred services are privately funded. Whether or not income is a barrier or an enabler to help-seeking for veterans is likely dependent on the context health care is delivered and how it is accessed.
The main design limitation in the research we reviewed was its lack of diversity. Most of the studies were cross-sectional analyses using samples predominantly composed of US male, army veterans, who served during the same conflicts. However, it has to be noted that cross-sectional data collection is a pragmatic method of accessing specific populations, such as hard-to-reach populations, such as veterans. 57 Furthermore, as the veteran population predominantly consists of ex-army males (the army being the largest of the armed forces), the risk of using mainly male, army participants will not likely reduce in the future.
A final issue with the studies was that approximately 42% of participants were directly recruited through the VA. Such veterans could already be help-seeking and be on the VA ‘system’. If the findings of help-seeking research are to be used to encourage or help non-help-seeking to come forward, it is less helpful to conduct research focused on those who already engaged in help-seeking.
Limitations
There are two main limitations with this review. First, it was difficult to distinguish what help-seeking was conceptualized as. There is a difference between veterans reaching out in help-seeking over a defined period (e.g. sessions or weeks) versus longer term support use. We made a differentiation between more initial stages of help-seeking versus longer term support engagement. But the overlap between the stages of initial help-seeking and service user engagement is somewhat blurred. Therefore, two studies30,39 in particular were included that could be viewed as straying from initial help-seeking.
Second, all the studies were in the English language. As such, our review could be viewed as skewed towards the experiences of English-speaking veterans in the West.
Conclusions
Collectively, it seems that veterans are reaching a mental crisis point before engaging in help-seeking. Although the findings relating to alcohol remain unclear, we can say that where veterans are choosing to manage symptom severity and functional impairment with alcohol, it is likely they are attempting to avoid some sort of crisis point. They may be unaware that they are potentially creating a comorbid MH issue, which will likely lead to worse outcomes ultimately.
While this review found PTSD was the main predictor of help-seeking, a broad range of other more cognitive enablers and barriers were elicited that are potentially modifiable, to either aid help-seeking or to potentially avoid a crisis point being reached. Practical barriers – mainly associated with access difficulties linked to cost, availability and location – could be addressed by support provider organizations. Attitudinal barriers/enablers could be improved by improving MH literacy and beliefs surrounding support. Such interventions need to be directed at both veterans and support service stakeholders, in order that stakeholders are fully invested in improving service user experience for veterans.18,58
To design effective interventions, it is essential to understand more fully the underlying help-seeking processes specific to veterans classified as having ceased military employment. It would be beneficial to investigate such processes qualitatively, as context and culture may influence attitude formation. 59 Aside from clarifying what veterans are help-seeking for, a qualitative approach may elicit clearer findings on the role alcohol plays.
Supplemental Material
Supplemental Material – Enablers and barriers to military veterans seeking help for mental health and alcohol difficulties: A systematic review of the quantitative evidence
Supplemental Material for Enablers and barriers to military veterans seeking help for mental health and alcohol difficulties: A systematic review of the quantitative evidence by Catherine Hitch, Paul Toner and Cherie Armour in Journal of Health Services Research & Policy.
Footnotes
Acknowledgements
The authors would also like to thank the Royal British Legion for funding the PhD research programme resulting in this specific review. The funders had no role in the study design or interpretation of results.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Royal British Legion, the United Kingdom (under grant EGR17Q4/100015).
Ethical approval
Ethical approval was not required for this systematic review article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.