
Abstract
Objective
The National Health Service (NHS) in England has introduced a range of policy measures aimed at fostering greater openness, transparency and candour about quality and safety. We draw on the findings of an evaluation of the implementation of these policies in NHS organisations, with the aim of identifying key implications for policy and practice.
Methods
We undertook a mixed-methods policy evaluation, comprising four substudies: a longitudinal analysis of data from surveys of NHS staff and service users; interviews with senior stakeholders in NHS provider organisations and the wider system; a survey of board members of NHS provider organisations and organisational case studies across acute, community and mental health, and ambulance services.
Results
Our findings indicate a mixed picture of progress towards improving openness in NHS organisations, influenced by organisational history and memories of past efforts, and complicated by organisational heterogeneity. We identify four features that appear to be necessary conditions for sustained progress in improving openness: (1) authentic integration into organisational mission is crucial in making openness a day-to-day concern; (2) functional and effective administrative systems are vital; (3) these systems must be leavened by flexibility and sensitivity in implementation and (4) a spirit of continuous inquiry, learning and improvement is required to avoid the fallacy that advancing openness can be reduced to a time-limited project. We also identify four persistent challenges in consolidating and sustaining improvement: (1) a reliance on goodwill and discretionary effort; (2) caring for staff, patients and relatives who seek openness; (3) the limits of values-driven approaches on their own and (4) the continued marginality of patients, carers and families.
Conclusions
Variation in policy implementation offers important lessons on how organisations can better deliver openness, transparency and candour. These lessons highlight practical actions for policymakers, managers and senior clinicians.
Introduction
Openness, transparency and candour are recognised as ethical responsibilities of health care organisations,
1
and as crucial resources for reflection and learning to improve health care quality.
2
Openness – defined by one authoritative inquiry as ‘enabling concerns to be raised and disclosed freely without fear’3(p75) – is seen as vital in ensuring that everyone involved in health care delivery is able to voice concerns about problems of quality and safety, regardless of role or seniority. Yet, delivering on these commitments in health care systems has often proved challenging, as shown by investigations into major organisational degradations worldwide.4,5 In the National Health Service (NHS) in England, examples include catastrophic failings at Stafford Hospital in the 2000s,3,6,7 where the Mid-Staffordshire public inquiry concluded that: For all the fine words printed and spoken about candour, and willingness to remedy wrongs, there lurks within the system an institutional instinct which, under pressure, will prefer concealment, formulaic responses and avoidance of public criticism.6(p184)
Summary of interventions introduced following inquiries and reviews of openness.
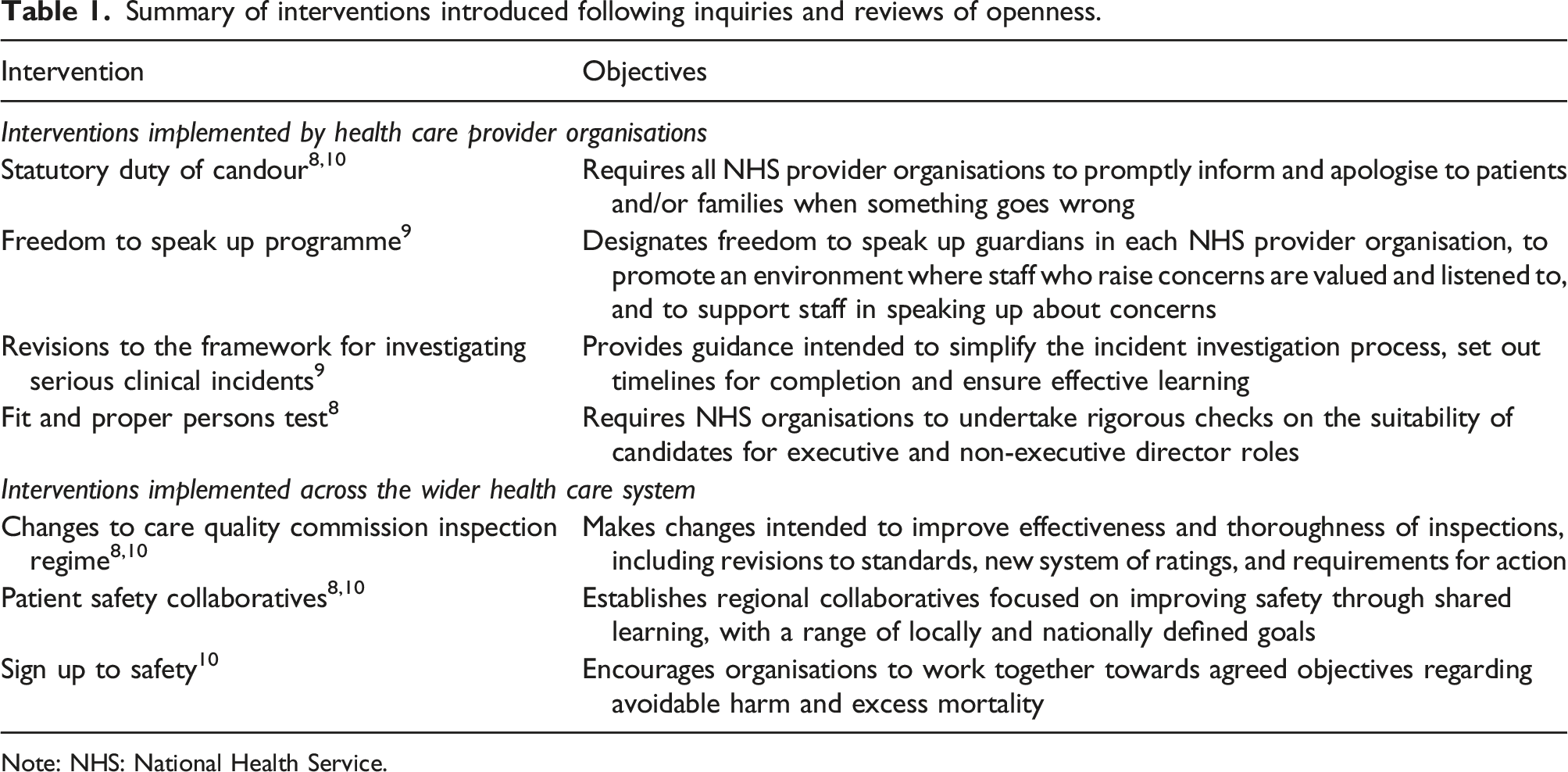
Note: NHS: National Health Service.
In this paper, we present policy- and practice-oriented findings from a large mixed-methods evaluation programme that examined organisational responses to national policies aimed at changing cultures relating to openness. Mindful of the complexities of organisational culture change in health care, 15 our main focus is on high-level implications of our analyses for managers and policymakers grappling with change in heterogeneous organisations.
Methods
From 2017 to 2019, we undertook a mixed-methods evaluation of policies introduced following government-commissioned reports on poor quality of care and failings of openness in the English NHS, particularly at Stafford and Furness hospitals.3,8–10,12 Our focus was the aggregate impact of the policy interventions on culture, attitudes and behaviour relating to openness about problems of quality and safety, rather than the impact of any one policy on its immediate objectives.
Substudies: foci, methods and samples.
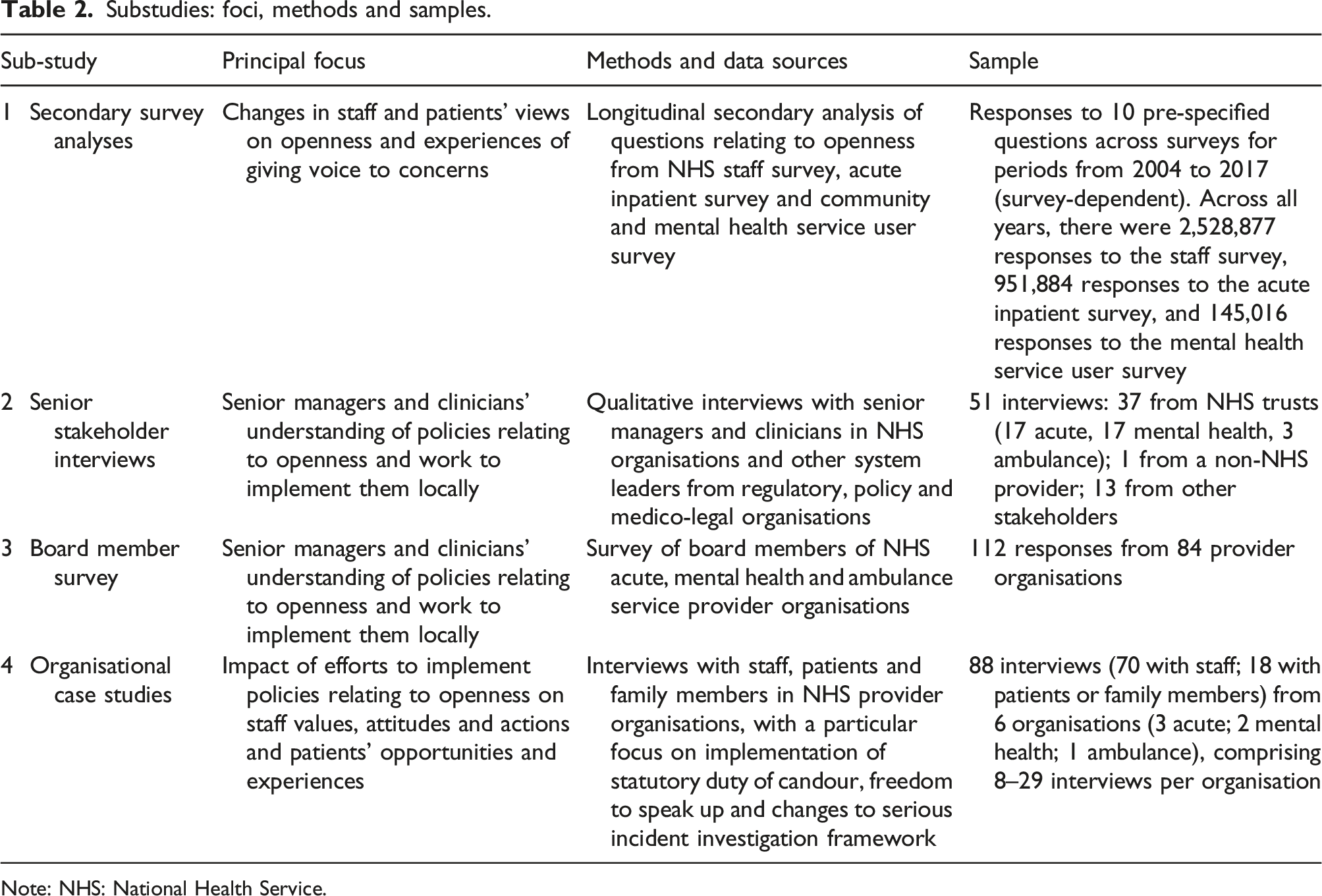
Note: NHS: National Health Service.
Substudy 1: Secondary survey analyses
First, we asked: Are staff and patients’ views on openness, knowledge of performance and experiences of giving voice to concerns changing through time, for better or worse? To answer this question, our first substudy comprised a series of analyses of existing survey data from 2004 to 2017 on the views and experiences of NHS staff, acute hospital patients and community mental health service users. 17 We identified a subset of items within each survey that related most closely to culture around openness. For each item, we used longitudinal statistical methods to identify changes in responses and trends between the periods before and after the publication of the Mid-Staffordshire public inquiry report in 2013. 3
Substudy 2: Senior stakeholder interviews
Second, we asked: How do senior managers and clinicians in organisations providing NHS services understand policies relating to openness and translate them into specific norms, expectations and practices in their organisations? Two substudies primarily addressed this question. We conducted 51 semistructured telephone interviews with representatives of policy and regulatory organisations relating to the English NHS, and senior clinical and non-clinical staff in provider organisations, sampled using a mixture of randomised and purposive approaches. 18 Data collection took place in late 2017 and early 2018. Analysis was based on the constant comparative method. 19
Substudy 3: Board member survey
We commissioned a professional polling company to undertake a survey of NHS board members in early 2018. The survey asked board members about provider organisations’ policies and how the organisations’ chief executives, medical directors, directors of nursing and board leads for risk, governance and safety implemented these policies. The survey elicited 112 responses from individuals across 84 health care organisations. Data were interrogated using descriptive and analytical statistical methods.
Substudy 4: Organisational case studies
Our final research question asked: Are provider organisations’ efforts to increase openness resulting in real changes in staff values, attitudes and actions at the sharp end of care and in patients’ opportunities and experiences around openness – and what features contribute to success? The fourth substudy aimed to address this question by examining the translation of openness policies into organisational practice, and its impact on the experiences and views of staff, patients and families.
We focused on three policies that appeared, from the second and third substudies, to be leading to widespread activity: the statutory Duty of Candour, the introduction of Freedom to Speak Up Guardians and changes to processes for investigating serious incidents (for more details on these policies, see Table 1). We looked at their implementation and impact in six NHS organisations (three acute trusts, two community and mental health care trusts, and one ambulance trust), purposively selected for diversity of organisation type, population served and approach to implementation. Data collection took place from mid-2018 to mid-2019.
We used semistructured interviews to identify approaches to implementation with senior staff in each trust, which we analysed using the constant comparative method. 19 We conducted in-depth, narrative interviews with staff, patients and family members who had experience of the initiatives or of related activities – for example, those who had been involved in the disclosure of a serious incident or who had raised concerns or complaints. We analysed these interviews using narrative analysis techniques. 20 Across the six organisations, we conducted 88 interviews in total (70 with members of staff and 18 with patients or family members). 21
Synthesis across substudies
Following separate analysis of each substudy, we synthesised the key findings and implications. This involved two stages: (1) integrated analysis of qualitative data from substudies two and four; and (2) collective consideration by the whole team of findings from the four substudies together, identifying complementarities, considering how findings from each substudy illuminated or assisted in the interpretation of others, and considering and seeking to explain apparent tensions or inconsistencies between findings.
Our approaches to sampling, recruitment, data collection and analysis were guided by a professional advisory group and a patient and public advisory group. Ethical permissions for the second and fourth substudies were obtained from an institutional research ethics committee and a National Research Ethics Service research ethics committee respectively.
Results
We begin by presenting a summary of the results across the four substudies. More extensive expositions of these findings are available elsewhere.16–18,21,22 We then build on these findings, particularly those from the fourth substudy, to propose four conditions that appear necessary for achieving sustained changes in culture and behaviour. We highlight four persistent challenges that continue to frustrate efforts at improvement.
Summary of findings across the substudies
Results of the secondary survey analyses presented a mixed picture of progress in terms of staff and patients’ experiences of openness over time.16,17 There was a trend towards more positive responses to several of the questions on the staff survey and the acute inpatient survey from the mid-2000s to the mid-2010s. For example, there were improvements in respondents’ views of the quality of communication between managers and staff, and on their ability to contribute positively towards improvements; for acute inpatient survey respondents, there were improvements in views on the information provided about their care, and on their involvement in decisionmaking. We also found statistically significant improvements in the rate or direction of change in the period after publication of the Mid-Staffordshire public inquiry in 2013 compared with the period before: for some indicators, the rate of existing improvement increased in the period after publication, and, for others, a decline in positive responses prior to 2013 was reversed in the period after publication.
The survey of community mental health service users demonstrated a somewhat different pattern, however, with some improvements stagnating or even receding over time. For example, community mental health service users’ responses to the question ‘Did the person or people you saw listen carefully to you?’ worsened at a statistically significant rate from 2013 to 2017, having previously shown statistically significant year-on-year improvement. The apparent contrast between the experiences of patients and service users in acute physical and community mental health is especially striking given the avowed policy commitment to parity of esteem between physical and mental health of UK governments since 2012. 23
Findings from the senior stakeholder interviews and the board member survey16,18 found that participants were largely positive about the policy measures introduced to encourage openness, but noted important challenges and highly variable approaches to implementing key initiatives. Some participants from mental health care provider organisations felt that the Mid-Staffordshire public inquiry and the associated policy response were constructed around one model of an acute health care trust – an organisation where services were centralised in a small number of sites, where patients were seen for relatively discrete episodes of care focused on distinct health care needs, and where unity of purpose and patient and organisational outcomes were perhaps more easily defined – which did not reflect their own organisations. As one respondent, a senior stakeholder from a community and mental health services trust, noted: This is the bit that I suppose we struggle with...It was a national diktat—this is what you’ve got to do. And I think if you’re in an acute trust it’s slightly easier, perhaps, because you’re all on one site. Whereas our staff are all dispersed across the county. So, people respond to an acute issue and then try to transpose it across the whole of the NHS.
Participants from across sectors highlighted the long-term nature of change and the problems of effecting change across heterogeneous organisations with multiple sites, each with its own local culture and history. Recent organisational history was seen as a particularly important influence on implementation. Examples of failures of openness in the past – for example, the perception or reality of harsh treatment of individuals who gave voice to concerns – could cast a long shadow, breeding scepticism about current efforts to improve openness. Conversely, past failings in some organisations had been crucial in giving impetus to local initiatives to increase openness, and were seen as giving some organisations a ‘head start’ in efforts to improve their cultures. 18
We sought to attend to these organisational disparities and to the importance of local history in sampling our organisational case studies, which covered trusts with divergent histories and differing apparent progress towards openness, across sectors. We refer to the trusts as Trusts A to F. The trusts are characterised in terms of the degree to which they had made progress towards improved openness:
16
• Trusts A and B. These two organisations – both acute trusts – appeared to be particularly advanced in their efforts to improve openness. Both had experienced significant problems in quality, safety and openness, which had prompted improvement programmes that preceded or complemented policies introduced nationally. Both were spatially distributed, with services provided across multiple sites, but leadership in both organisations had sought to ensure that policies were implemented across services and sites. • Trusts C and D. These two organisations – one a community and mental health services trust and the other an ambulance trust – had made intermediate progress towards greater openness. They were of medium size, and both were dispersed across multiple sites. The ambulance trust, in particular, had sought to initiate improvements in openness, particularly in relation to openness with patients when things go wrong, following a well-publicised incident some years earlier. • Trusts E and F. These two organisations – one a community and mental health services trust and the other an acute trust – had made limited progress towards greater openness. They appeared to be facing more significant issues. Both were diffuse organisations with wide-ranging functions and strong localised subcultures. The acute trust was the product of a recent merger, while the community and mental health services trust had a very large number of sites and sub-units.
In the remainder of this paper, we focus on identifying the implications of our findings.
Four necessary conditions for change
Our analysis across the substudies identified four conditions that appeared necessary, but not sufficient, for making strong progress in implementing openness policies.
Authentic integration into organisational mission
A distinguishing feature of the organisations that had made greater progress towards openness was the way they framed openness as part of mainstream business, not an optional bolt-on. Case-study organisations varied markedly in, for example, the resources they devoted to openness initiatives, and this was consequential materially and symbolically. Materially, interventions such as Freedom to Speak Up Guardians required significant investment to ensure that role-holders had sufficient time to deliver the role and could make connections across their organisation to foster confidence in speaking up and generate awareness about how to raise concerns. As a Freedom to Speak Up Guardian at Trust C said: I go to every induction, including the student nurses, nursing associates and junior doctors…I targeted each individual directorate, introduced myself to the director, explained what I wanted to do and then found out the matrons, so that I could get invited to team meetings, to make sure that I was engaging with staff as far and wide as possible. Just raising awareness about the role—it was my passion that it was about seeing a face rather than just a brand—and knowing that there’s just another mechanism by which people can speak up.
In contrast, a lack of organisational commitment to openness was often abundantly obvious. If a Freedom to Speak Up Guardian was largely invisible, it was clear that this was not an initiative that was high on the organisational priority list. As the Freedom to Speak Up Guardian in this position at Trust E said: It is very, very difficult. A lot of it I have to do over the phone…I probably don’t get more than about five or six [approaches from staff] in the quarter.
Work to optimise and tailor the policy initiatives, or to integrate them into the wider organisational mission, seemed to reap benefits. Participants described the importance of maximising alignment between ascendant values around openness with other organisational norms, expectations and policies. This could help in making clear that the need for openness was neither a fad nor an exogenous mandate followed reluctantly, but was instead fundamental to improvement and a normative expectation.
Participants also stressed the value of efforts to translate openness into something that was operationally useful to colleagues on a day-to-day basis. They highlighted interventions such as behavioural standards frameworks that staff could use to hold one another to account informally in their daily interactions, though active work was required to ensure that they were more than rarely visited webpages or documents to gather dust. As a respondent at Trust B put it: They promote it a lot at corporate induction, and it does underpin the culture. You do get people coming to raise concerns because these standards are now expected of everyone within the trust. Because it was quite a public launch, that’s been quite good. And supported by the behaviour standards, but it’s more a cultural thing, and there’s been a big thing against [poor behaviour]: ‘It’s not OK to behave that way.’
Participants saw this kind of framework as useful because, although Freedom to Speak Up, the Duty of Candour and other policy initiatives were seen as important, they were also prone to be viewed as pertaining to rare events and moments of high stakes. Normalising openness as part of everyday conduct, rather than a value to be mobilised only occasionally in exceptional circumstances, was therefore a key preoccupation.
Functional and effective administrative systems
A consistent finding across the senior stakeholder interviews, board member survey and organisational case studies was the importance of effective administrative systems in supporting openness, transparency and candour. The policies all represented complex interventions with significant administrative implications. Ensuring that they were aligned with one another and contributed to encouraging openness more broadly required substantial and skilled implementation work.
In the organisations where openness was most advanced, sophisticated socio-technical infrastructures relevant to openness had been built up over several years. These systems offered, for example, tight oversight of disclosure and investigation processes, rapid dissemination of learning and implementation of recommendations, and integration of different sources of organisational intelligence about concerns and risks. A respondent at Trust B explained her organisation’s approach: We started our patient safety summits about four-and-a-half years ago—so Duty of Candour wasn’t out at that point—so it just became part of what we did as the business for the patient safety summit...That is all part of incident-management processes…That all gets tied in—each incident’s got a number attached to it, the rapid reviews, the staff reflections…so that we can prove that they’ve actually had the discussion with the wider team.
Functional administrative systems were particularly important in bringing together multiple sources of intelligence, to inform preventive action. As a respondent at Trust A put it: You listen to everything. It might be you investigate it and there’s really very little substance behind it. But you listen to everything and you triangulate.
In organisations where less progress had been made, approaches to monitoring, responding to and disseminating lessons learned appeared much weaker, with less clarity about the processes, less confidence that they were effective,\ and less attention to how learning could be made meaningful and turned into action. The approach described by a participant in Trust E, for example, suggested a rather less integrated system for processing and disseminating insights from investigations: So, the way it works—whether it works well, I don’t know—the governance team will then draft a vignette, because otherwise it’s just, no-one’s going to read the whole report, not everybody, so they'll draft a vignette. That vignette is then fed back to the different teams, and it goes from top, so there’s a senior management team, then there’s a clinical team, then there’s a local. Everybody has about a thousand meetings, I find! It filters down, so, eventually the ground-floor staff will have it.
The importance of high-quality administration is underscored by evidence from elsewhere – for example, on the role played by clearly understood pathways, proactive management of processes and sound underpinning systems and infrastructure in the effectiveness of all but the simplest of improvement interventions.24,25
Flexibility and sensitivity in implementation
Functional administration of openness initiatives alone was not enough for greater openness, however, and could even have negative consequences. Participants described the negative consequences of systems and processes that appeared bound by their own internal order, timescale and rationality. Coldly efficient systems that ground away inflexibly, giving no quarter to the needs or wishes of the individuals involved, gave the impression that policies to advance openness were above all about serving the system rather than helping those who had been harmed. Approaches to disclosure, investigation and learning that were beholden to inflexible pathways, timescales and forms of interaction were frequently seen by staff, patients and family members as unhelpful and even upsetting. For staff, standardised approaches were not always well suited to learning and improvement. For patients and carers, they could add insult to (sometimes literal) injury.
26
As a respondent at Trust C explained: There’s a vast range of patients that we deal with, and it does vary in terms of what involvement people want. Most of our serious incidents involve patients with mental health needs and sadly a lot of those involve death or serious injury, so quite often then we’re relating to families...Someone personally goes and takes that investigation report back to that patient or family, if they want it. Not everybody does. Some people just—particularly where we've had people that have made things like suicide attempts and not taken their own life—quite often those patients are like, ‘I want to leave it there, I don't want to relive the whole thing.’
Participants in the case-study organisations used techniques to soften systems by giving them a human touch while still ensuring adherence to regulatory and legal requirements. These included learning sessions that complemented formal incident investigations, templates for disclosure letters that indicated what was needed for compliance but also allowed staff to express sorrow, regret and empathy in their own words. In Trust D, staff could volunteer to train to act as points of contact and advocates for family members after serious incidents, including during the often distressing periods of investigation that followed. A managerial staff member at Trust D suggested that this system had been successful in reducing complaints and litigation – but crucially it did so because it prioritised the emotional needs of families: Some families will want a meeting every week or a phone call every week and then others may want no involvement and would like just to be sent the report in the post. So, you really do have to be fluid with it and just go by what the family’s needs are.
This kind of activity represented vital, but easily overlooked, emotional labour, which was time-consuming, messy and fraught. Much of the work involved in achieving openness in practice – the work of disclosure, investigation and speaking up – exceeded what was imagined in formal documents, pathways and processes. Doing it right required judgement, flexibility, discretion, the occasional workaround26,27 and licence from management to work this way.
Continuous inquiry, learning and improvement
Finally, approaches to fostering openness benefited from an organisational ethic of reflection, learning and improvement. Integration into organisational mission and functional administrative systems did not come about by accident and were not perfected at the first time of asking. Rather, they were the product of learning, persistence and improvement.
Participants described protracted and dogged efforts to improve, sometimes using formal improvement approaches, sometimes more ad hoc. This took place at various levels, from improving individual processes (such as procedures for disclosure) to optimising systems for integrating various forms of intelligence to anticipate and pre-empt quality and safety issues. A participant at Trust C recalled: I've said, ‘This is an organic process. I am not saying that by December next year you will have a suite of outcome measures.’ I'm not saying any of that, it is an organic process. It’s, ‘What do we have? What do we need to develop? What do the staff tell us? What do patients tell us? How does it look? How can we do it? What does that picture give us?’ And it’s building that picture, and I'm being quite assertive about that, saying, ‘Don't tell me that you need all these boxes filling, because it’s not going to happen.’
Underlying all these efforts was an approach to implementation that was open-ended and extended beyond individual policies. Treating the policies as discrete, time-limited implementation tasks meant that their potential complementary impact as part of wider efforts to foster openness would be lost.
Four persistent challenges
The substudies also highlighted a range of challenges that hampered progress towards openness. While these challenges were more prominent in the organisations that had made less progress towards openness, they were evident in all the organisational cases, and evaded straightforward resolution.
Reliance on goodwill and discretionary effort
Provider organisations were expected to implement the policies introduced following the Mid-Staffordshire public inquiry without supplementary or ring-fenced resources. Given the direct and opportunity costs of implementation, organisations varied in how much time and effort they invested in openness initiatives. Even in case-study organisations where more progress towards openness had been made, there was a substantial reliance on input from staff over and above their core responsibilities. Some staff embraced additional responsibilities with enthusiasm, seeing the work as important and rewarding. Work, however, was exactly what it was: work that often relied on discretionary effort, and was usually uncompensated by the displacement of other activities or extra payment.
Some trusts sought to spread the burden more broadly, for example, by supplementing Freedom to Speak Up Guardians with ‘champions’. A Freedom to Speak Up Guardian at Trust F appreciated the help, but acknowledged that it reflected a lack of visibility of their own role in large parts of the organisation: I can’t do it without [the champions]. When people really start using them, as I hope they will more and more, that will be particularly useful. I just can’t cover the territory effectively enough, I see everyone who wants to see me, but it’s very time-consuming and I’m not—apart from being a screensaver!—I’m not that visible on some of the other sites.
Further, discretionary effort and goodwill depended, as some senior stakeholder interview participants attested, on relationships of trust. But memories of injuries endured by people who spoke up in the past were hard to displace. Bitter experiences, such as a lengthy dispute over pay and conditions for trainee doctors, left staff less inclined to give of themselves to initiatives of dubious individual benefit. In short, there was a strong sense among some participants that the well of staff goodwill and discretionary effort was at risk of depletion.
Caring for staff, patients and relatives who embrace openness
Participants spoke of the significant emotional work involved in raising concerns, in contributing to investigation processes and in seeking apologies, redress and meaningful learning, particularly when processes did not demonstrate flexibility and sensitivity. As a respondent at Trust F said: [The incident investigation process] wasn’t done in a ‘OK, this situation has happened. Can you just describe to me your thought process? Can you think of any other way that you may have managed this?’…[Instead,] it was: ‘Well, you did this: why did you do that? And, well, the guidelines say this, so why didn’t you follow the guidelines?’…Which I found less supportive.
A family member at Trust B similarly felt the investigation process she faced was focused on the organisation’s benefit: I feel as though we are giving them everything they need for their investigation, but they are not giving to us what we need to close it. One-way traffic.
The relationship between staff wellbeing, organisational wellbeing and quality and safety is well recognised,
28
but participants noted pointedly that the NHS was at risk of neglecting the needs of staff and patients who raised concerns as it embraced openness. In some organisations, moreover, there was a sense that the system was capricious in its response to openness, adding to the perceived risks of raising concerns and the burden on those who did so. As a staff member at Trust F explained: Occasionally, something will get raised and everyone will pat you on the back, or something else will get raised and someone will get selected and thrown under the bus. And there’s no predictability about it.
The limits of values-driven approaches
Many participants described an approach to policy implementation that was based primarily on the principles and ethos of organisational development. 29 This meant seeking to implement the policies by aligning them with the values, objectives and development of individuals, rather than forcing change upon recalcitrant members of staff. But even in organisations that claimed a progressive, enlightened orientation towards openness, there remained areas that appeared intractable to such values-driven approach.
One important barrier to the approach was cliques of staff who wielded an insidious influence on those around them, creating a climate of fear, bolstered by their seniority, their longevity in the organisation, or their advantageous social networks. As a staff member at Trust B noted: It’s really unnerving whenever you’ve got a group of people in a position of power making it very clear that they’ve got a longstanding history here, any of your concerns are not going to go anywhere...I just can’t understand how someone can be so well known and identifiable for their behaviour and for it to be acceptable for continued reports and complaints be made against them and nothing be done.
Such ‘fiefdoms’ were in evidence in parts of even the organisations that had made greater progress towards openness. Convincing staff whose values were aligned with the objectives of greater openness sometimes meant demonstrating resolve in addressing problems caused by those who obstruct it.
The continued marginality of patients, families and openness
Finally, it is notable that openness policies examined focus primarily on organisations and staff. We found that patients and families were mainly bit-part players in enacting the policies. This absence is perhaps surprising, given the critical role of patients had in uncovering – and demanding action about – the problems at Stafford Hospital and in other organisations where openness has been lacking.3,12 Where information from patients and carers was used to inform openness work, it tended to come from surveys and routine datasets rather than from efforts to give patients and carers opportunities for proactive voice. As a staff member at Trust B observed: I wouldn’t have said, at the moment anyway, that we’ve got a huge amount of members of the public involved with the management of our incidents, apart from them being informed and always being transparent when something does go wrong.
In general, patients and family members who had concerns depended on organisations that might or might not offer them opportunities to speak up, and on staff who might or might not listen. Failing to mandate clear routes and organisational responsibilities for patients and family members wishing to raise concerns may increase the risk of problems of quality and safety going undetected for longer.
Discussion
Our findings offer a mixed picture of progress toward improving openness in the NHS, with all substudies reflecting the patchy nature of change. There is little to suggest the significant shifts in culture around openness on the scale sought by inquiry leads, commentators and policymakers3,10,11 have been consistently achieved. Our findings affirm a view of the NHS as a ‘cultural mosaic’, in which top-down efforts to change culture are likely to have inconsistent impacts at best, 15 and offer insights into the reasons for this variation. However, in identifying four features that appear to be important in achieving progress, and four challenges that need to be addressed, our study offers insight into how progress towards openness might be accelerated.
We identified that organisations need to make openness an organisational priority, integrated into their core mission. But declarations of commitment mean little without the infrastructure to convert aspiration into practice. This requires, as others have found elsewhere,24,25 investing in clearly understood pathways, proactive management of processes and sound underpinning systems. Organisations also need to recognise the effort required to deliver on the goals of the systems, which implies sensitivity, tact, and avoiding excessive formalism. Further, maintaining a journey towards openness means moving beyond a mindset of ‘projectness’, 25 and committing to continuous improvement through learning. As one advisory group has put it, this demands that organisations ‘continually and forever reduce patient harm by embracing wholeheartedly an ethic of learning’.11(p5)
We further identified weaknesses in implementation that pose substantial threats to achieving the goals of openness policies. Reliance on the discretionary effort of NHS staff, clinical and non-clinical, is not unique to openness initiatives; the NHS Staff Survey, for example, has persistently found that many staff work significant unpaid overtime every week, 30 and the additional stresses associated with the response to COVID-19 since the fieldwork took place has likely intensified these pressures. 31 The symbolic and material damage associated with a precarious delivery mechanism for such an important priority needs to be addressed. Excessive reliance on values-driven approaches was also a risk, indicating that a broad-based set of strategies may be needed, including a commitment to upholding standards and holding those who persistently fail to adhere to them accountable. 32
One important insight is that much work needs to be targeted at the tangible systems, processes and routines that relate to openness in organisations’ everyday activities. But attending to culture is vital too. Different professional groups and different units within organisations may have different (sub)cultures, different sets of assumptions, different ways of relating to each other and carrying out their work. 15 This requires work to tailor interventions, particularly in organisations – such as many community and mental health trusts and some acute trusts – characterised by multiple, disparate teams, units and sites, each with its own distinct history. 18 Equally, support for the emotional work of openness is needed. 26 A welcome development is the recent increased focus on staff wellbeing, including the use of Schwartz Rounds (discussions with staff about the emotional impact of their work).30,33
Disappointing, and perhaps surprising given their prominence in unearthing problems at Stafford Hospital and elsewhere,3,12 is the continued marginality of patients and their families in the implementation of openness policies. Other than an enhanced role in Care Quality Commission inspections, 10 the principal mechanisms through which patients and family members can raise concerns about quality and safety remain largely the same as they were in the 2000s. While there was some evidence in our study of local initiatives to address this gap, nationally led work may be valuable here, to harness the particular insights that patients and family members can offer into quality and safety. 34
Limitations
Our study has three main limitations. First, it relied primarily on interviews and survey data, so causal inferences are difficult to draw. Second, it was limited in scope, in that it only considered the English NHS and excluded primary care. Third, the study was conducted in a highly dynamic context, where broader shifts in policy and organisational structure may have affected openness over the course of the study – most notably, changes in views and experiences noted in the secondary survey analyses may have been influenced by events other than the response to the Mid-Staffordshire public inquiry.
Conclusions
Our findings help to characterise the key features of and challenges to the implementation of greater openness in health care. They demonstrate the importance of going beyond simple implementation of national policy mandates and reveal the difference that nuanced approaches to policy translation, led by skilled managers and backed by investment and tenacity over the long term, can make.
Footnotes
Acknowledgements
We are grateful to the participants in the study who generously gave their time, and we thank two anonymous peer reviewers for helpful comments.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for substudy 2 was provided by the University of Leicester (reference 10409-sec55-healthsciences). Ethical approval for substudy 4 was provided by the North West–Greater Manchester East Research Ethics Committee (reference 17/NW/0719).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Department of Health and Social Care Policy Research Programme (PR-R15-0116-23001). GPM and MDW are supported by the Health Foundation’s grant to the University of Cambridge for The Healthcare Improvement Studies Institute. The Institute is supported by the Health Foundation, an independent charity committed to bringing about better health and healthcare for people in the UK. MDW is a National Institute for Health and Care Research Senior Investigator (NF-SI-0617-10026). The views expressed in this article are those of the authors and not necessarily those of the NHS, the National Institute for Health and Care Research or the Department of Health and Social Care.