
Abstract
Objectives
Schwartz Center Rounds® (‘Rounds’) are multidisciplinary forums where health care staff come together to reflect upon the emotional impact of their work. In each Round, a small number of staff (panellists) share experiences through stories to trigger reflection in audience members. Previous research has identified impacts associated with Rounds’ attendance, but little is known about the experience and impact of Rounds from panellists’ perspectives. This study is the first to explore the role of disclosure and reflection through storytelling in Rounds, specifically exploring panellists’ motivations, experiences and reported impacts associated with panel participation.
Methods
Interviews with 50 panellists, from nine case-study sites in the United Kingdom, representing acute, community and mental health National Health Service trusts and hospices. Data were analysed using thematic analysis.
Results
Most panellists spoke positively about their experience of sharing their stories in Rounds. Reported impacts included: increased emotional resilience and acceptance of experiences; reduced negative assumptions about colleagues and increased approachability and trust increasing tolerance and compassion; the creation of a space to stop and think and to reframe negative patient experiences facilitating greater empathy and emotional disclosure becoming more visible and normative, thereby helping change culture. Impacts on staff were similar regardless of contextual variability, including their professional group or role, with the exception of impact on patient care, which was not mentioned by non-clinical staff. The extent of panel preparation and audience characteristics (e.g. size, composition and response to their stories) influenced panellists’ experiences and outcomes.
Conclusions
Rounds highlight the important role of disclosure and reflection through storytelling to support panellists with the emotional aspects of their work, providing a space for support with the emotional demands of health care, reducing the need for employees to be stoic. Panel participation also offers an important source of validation in organizations marked by scrutiny.
Introduction
Emotions characterize and inform organizational processes and cultures 1 in all organizations, but particularly in health care, where emotional situations are prevalent. 2 Yet, emotions are rarely spoken about, and emotional stoicism (defined as ‘the endurance of pain or hardship without the display of feelings and without complaint’) (see p.178 in 3 ) is highly valued. 4
Stoicism is closely linked with emotional labour, whereby employees alter their outward expression to conceal inner feelings to comply with the demands of the environment. 5 If such behaviour persists, it can lead to stress, 6 poor physical and psychological well-being 7 and burnout. 8 One aspect of burnout is depersonalization, a psychological state in which individuals feel detached from their own emotions 9 and where their view of others may become cynical or indifferent. 10 There is a direct link between staff well-being and patient experiences.11,12 Poor well-being results in health care staff being unable to connect with, or be empathic towards, patients and their relatives 12 and has been linked to poor health care outcomes, including increased frequency of medical errors, increased rates of patient mortality and poorer patient experience. 13 Staff well-being is therefore fundamental to high-quality health care; yet, effective interventions to support it are lacking.4,14 Schwartz Center Rounds® (hereafter ‘Rounds’) are one intervention that may provide a solution.4,15
Rounds provide staff with a (usually monthly) forum to discuss the emotional impact of their work in a safe and confidential environment.4,16,17 In contrast to other forums, Rounds are open to all staff (clinical and non-clinical of any grade), are not a place for problem-solving or clinical reasoning and attendance is flexible. 17 Each Round lasts 1 hour and commences with a 15–20 minutes panel presentation, usually comprising three to four multidisciplinary staff. The panel either present an experience that is collectively shared (e.g. a patient case), where panellists are usually known to each other and work in the same team or department, or present a set of individual experiences based around a theme (e.g. ‘A patient I’ll never forget’), where panellists are mostly unknown to one another.4,16 A multi-disciplinary organizing committee (‘steering group’) of 8–12 members plan the topics and cases in advance, manage the publicity and evaluate each Round. The other attendees at each Round form the audience. The panel presentation is followed by an open discussion, guided by a trained facilitator, in which audience members are invited to share their reflections.
Prior to a Round, the facilitator(s) and panellist(s) meet as part of panel preparation. Panel preparation enables facilitators to support panellists to prepare their stories into a format that is accessible, short (≤5 min) and safe for public disclosure.16,18
Drawing from the psychoanalytic literature, the process of preparing a story for public disclosure can help individuals to better understand 19 and begin to come to terms with their experience. 20 These effects are enhanced when individuals ‘open up’ in a supportive and trustworthy environment. 21 Disclosure through storytelling can allow panellists the opportunity to show vulnerability, which facilitates human connection and promotes reciprocal action when observed by others. 22 It can also trigger reflection, a process of learning in which individuals gain new insights based on critical evaluation of their experience(s). 23
A recent systematic review of studies of Rounds 17 identified impacts and outcomes associated with attendance at Round(s) relating to ‘self’ (improvements in well-being, emotional resilience and capacity for reflection, acceptance of experiences, reduced stress, decreased feelings of isolation and reduced emotional labour), ‘others’ (improved teamwork and increased compassion/empathy towards colleagues and patients) and the ‘wider organization’ (changes to policies and practices, and wider culture change through flattening hierarchies and enhancing connectedness). 17 However, none of the included studies investigated the impact on panellists.
This paper reports the experiences and reported outcomes for panellists, drawing on data from a UK national evaluation of Rounds that took place between 2014 and 2017.
4
The paper explores the role of disclosure and reflection through storytelling in Rounds to support panellists with the emotional aspects of their work. Specifically, this paper aims to:
(a). identify panellists’ motivations for telling their stories in Rounds, (b). explore the role of panel preparation in supporting panellists to participate in Rounds, (c). examine and report panellists’ experiences of presenting at Rounds, and (d). describe impacts associated with being a Round panellist in relation to impacts to self, colleagues/patients and/or the wider organization.
Methods
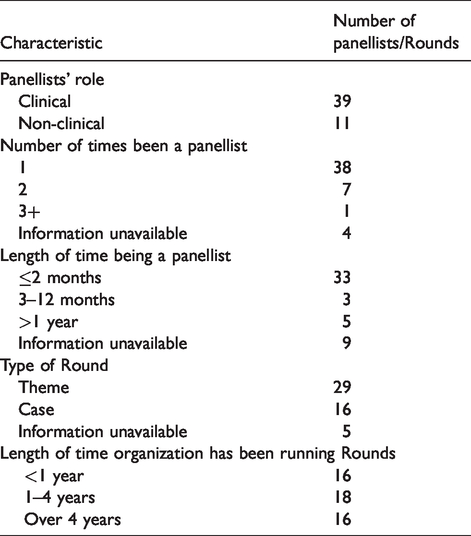
We undertook 50 semi-structured interviews with Rounds panellists from nine case-study sites, selected to maximize variation in organizational type (acute, community, mental health NHS trusts and hospices), size, geographical location and duration running Rounds. Some interviews (n = 11) were with panellists who held other Rounds-related roles (e.g. being frequent attendees, facilitators, steering group members), with their experience of being a panellist forming only part of the interview). Participants were purposively selected in each case-study site to include a range of staff groups and seniority, and also – to include variability in relation to the number of times they had been a panellist – how long ago they were a panellist, and whether the Rounds were theme or case based (Table 1). Each interview lasted 30–45 minutes. The interviews were structured in relation to the study aims and were digitally recorded and transcribed verbatim for analysis.
Characteristics of panellists and Rounds included in the present study.
A two-stage thematic analysis 24 was conducted in NVIVO 10 using (i) inductive analysis on a sample of transcripts to generate initial codes and themes, which fed into the development of (ii) an a priori coding framework, informed by findings from our review of the theoretical literature and observations of panel preparation and Rounds undertaken within the main study. 4 Data were examined across and between participants and compared and contrasted to identify patterns in the data, and also to specifically identify any disconfirming data (negative cases). 25 This included comparing impacts of Rounds between panellists with different characteristics (e.g. clinical vs. non-clinical staff, length of time the organization had been running Rounds, whether the Round was a theme or case-based Round).
Quotes reflecting key themes are used as exemplars and are minimally edited to ensure readability while maintaining and preserving authenticity. Quotations are labelled with a numerical identifier and the professional group of the interviewee. The case-study sites have tree species identifiers to protect anonymity. Findings are structured around the specific aims of the paper.
Results
Panellists’ motivations for telling their stories in Rounds
Motivations for volunteering or agreeing to be a panellist included: opportunities for professional development; to increase visibility of their work, role or team profile; or sharing knowledge and helping others learn from their experiences, especially topics associated with some misunderstanding or a lack of action: I wanted to share that experience because I know that mental illness is quite stigmatized still in the medical profession, especially with colleagues in … A&E departments … I thought it would be a good opportunity to put it out there – that if you’re frustrated, angry, scared and confused with our patients, we feel it as well sometimes. (Willow-29-Nurse)
The role of panel preparation
Not all panellists received panel preparation. Those who did suggested it helped shape their stories, draw out themes, clarify points and ensure they were ready to tell their story in front of others: It was nice to talk to people about what was expected and how the procedure would go ahead, and just to confirm what I was planning to say and whether that was appropriate or not. It reassured me because I was a little anxious. (Juniper-19-Speech and Language Therapist) I was thinking about the experience in terms of my professional viewpoint, but actually when I met with the facilitator it was more how you felt about things. So it made the prep actually quite challenging in a way because you’ve got to think about your own personal perception of things and how you feel. We don’t always talk about how we feel very easily do we? (Ash-01-Accounts Manager)
Panel preparation was not accessible to all panellists, due to other work commitments or time constraints. Some who received no or limited panel preparation felt less prepared having not heard other panellists’ stories: ‘I did feel relieved that I survived it and I felt relieved that [my story] hadn’t been in one direction and everybody else’s had been in the other’ (Ash-04-Nurse).
Those who heard other panellists’ stories for the first time in the Round, felt distracted: ‘I was conscious of the people either side of me and their stories and listening to them … [But I was also] thinking, “Right, what will I say to this bit?”’(Mulberry-01-Chaplain).
Panellists’ experiences of presenting at Rounds
Overall, panellists spoke positively about their experience of Rounds. Indeed, many considered it a privilege, since the chance to be in front of an audience (and be heard) was an opportunity rarely afforded to staff in their daily lives: ‘I was scanning the room as much as I could to see people’s faces and they were all focused … That’s quite an honour – to be in that position, to have people’s attention for that length of time’ (Mulberry-01-Chaplain).
Good facilitation and a safe, non-judgemental and confidential space in Rounds helped panellists speak more openly: ‘It feels safe and feels okay to talk about something that perhaps you haven’t wanted to admit … Nobody was saying, “Did you really do that?”’ (Mulberry-25-Director of Finance).
Some described how the experience had motivated them to speak with unusual honesty: I feel this pressure to always be nice, and sometimes – being human – sometimes you don’t have nice thoughts or feelings, sometimes people irritate you, push your buttons and push boundaries that make you feel uncomfortable. … Rounds are good at drawing that out. (Elderberry-04-Health Care Assistant)
The presence of an audience was central to the panellists’ experience. Almost all spoke of being aware of the audience and described ways they had attempted to read the audience – especially if there was a silence at the end of their presentation. In many cases silence was perceived as a sign of respect: ‘When I’d finished [presenting] there was a long silence … That’s what’s so powerful about Rounds: there’s that pause … that gap wasn’t suddenly filled unnecessarily … It makes it feel really sacred and puts the dignity into what’s being said’ (Elderberry-11- Nurse Educator).
Some expressed discomfort towards the silence: After the panel had spoken, the audience go into this terrible silence … You can almost hear people thinking, ‘Shall I say something? I’d really like to say something, but I’m not brave enough.’ But then once someone gives their opinion, then other people start to put their hand up and speak. (Elderberry-04-Health Care Assistant)
A positive audience reaction was especially valued where the ‘right’ decision was unclear at the time of the event: The first person … stopped to say, ‘It was a massively complicated case and I think you dealt with it really well’, and that was really nice to hear, because, you know, you’re never sure if what you’ve done is the right thing to do when you haven’t got the answer or outcome that you want. (Cedar-228-Occupational Therapist)
Two panellists felt they had made themselves vulnerable, with the facilitator later reflecting that their stories had been too raw, and too soon to share in a Round.
Some panellists assessed the ‘success’ of the Round on whether audience members referred to their story. Those whose stories were referred to felt a sense of approval. Those whose stories were not referred to felt rejected: Because there were different topics, people responded to one more than the other, and actually nobody responded to my story. I actually found that quite difficult because I couldn’t work out why that was, and I felt I’d made myself really quite vulnerable. (Elderberry-02-Bereavement Counsellor)
Impacts upon self, others (colleagues/patients) and the wider organization associated with being a Round panellist
Several found their involvement in Rounds cathartic, and many felt immediately better about their experience once they had shared it. In one case, a panellist recounted a case where a homeless patient in his pyjamas was discharged onto the street: During [the Round] I was so angry. I was gripping the chair and my heart was flooding with misery because of the injustice of it all. And so I felt very tense and upset. And then, immediately afterwards, I felt a bit better. (Ash-12-A&E consultant)
Some panellists felt greater inclination towards self-preservation following the Round. Such behaviour extended into everyday practice, as they began to recognize their own emotional triggers and acted to protect themselves against harm: I kind of have a bit more self-preservation following the panel. I think about trying to protect myself a little bit more, recognizing how situations are impacting on me and my emotions and trying to take a bit of a step back before I’m finding that they’re spiralling. (Cedar-227-Occupational Therapist) There is one thing that happened as a result of the Round … In the week afterwards I actually had lots of phone calls from specialist nurses and doctors who’d been at the Round [asking for advice on the topic] … So that was quite nice – that people were starting to think about things. (Sycamore-09-Nurse) A new psychologist … started with us, and I said opportunistically to her, ‘Oh, I’m doing this at lunch time today. If you’re not busy, why don’t you come along?’ … And one of the things she said afterwards [was,] … ‘I’ll never be nervous about revealing personal matters in supervision to you now, having seen what you and the others did on the panel’. (Willow-03-Psychologist) This lady said, … ‘I just wanted to talk to you because I was in the audience at your Round.’ She’d had a recent bereavement and she wasn’t sure if anyone cared about it and she said, ‘It’s quite clear they do. I understand now that perhaps you’re protecting yourself a little bit’. (Sycamore-09-Nurse) I think it does encourage you to share your problems a little bit more, be more willing to perhaps talk problems through. And I think at a team level that is beneficial – to feel that not only you should be talking about how you’re feeling, but also encouraging members of your team to do that as well. (Ash-03-Consultant Oncologist)
However, some respondents did report the impact on patients, including how being on the panel helped them think about their behaviour towards patients, react differently and be more empathic. Some panellists reframed encounters with patients more positively including a panellist who had been assaulted by a patient: We started talking about how the patient must have felt, how frightened he must have been … and I’ve never really had that kind of thought about what it would have been like for him … [Now] that anger has largely gone … and I felt much more connected to his distress and I was able to get through that anger and, to a certain extent, that hatred for him. (Horse-chestnut-01-Research Nurse)
Wider impacts mentioned by panellists were mostly hypothesized impacts (e.g. ‘I think it will increase empathy and communication within the organization’ (Willow-21-Consultant)), although some stated that Rounds had impacted in a real sense (e.g. the ‘Organization is more reflective’ (Mulberry-25-Director of Finance)). In sharing their experiences, panellists felt they were contributing to the creation of organizational norms where emotional disclosure was permissible: ‘A lot of us are quite … collected and hold our emotions close to us, and I think Rounds are encouraging the opposite of that, which is healthy. It creates an environment where actually it’s okay to have those feelings’. (Mulberry-26-Chief Executive).
In making the emotional impact of health care work more visible, panellists contributed to the promotion of organizational values around the importance of emotional well-being. For some this realization was somewhat unexpected although regarded favourably: I think what struck me, looking around, … all [these people] have made time to prioritize coming to something where we are talking about the stuff which is generally invisible, prioritizing it and acknowledging it … [That says] something about the emotional literacy of the organization. (Sycamore-07-Midwife)
We also examined the association of type of Round (theme vs. case-based) with the reported impacts. Two-thirds of panellists had participated in a themed Round (n = 29) and 16 had participated in case-based Rounds. For the remaining five, the type of Round(s) was unknown. There were no patterns in relation to the impact according to theme vs. case-based Rounds, with virtually all theme-based panellists and all case-based panellists reporting impacts on self and colleagues. Akin to the clinical/non-clinical analyses, there were few impacts reported on patients and wider impacts, regardless of the type of Round.
Discussion
This is the first study to explore the experiences and reported impacts of being a panellist in Rounds. It is therefore the first to explore how disclosure and reflection through storytelling in Rounds support panellists with the emotional aspects of their work.
The experiences reported here support psychoanalytic literature that suggests preparing a story for public disclosure helps individuals to better understand 19 and to come to terms with their experience through disclosure. 20 This can reduce staff stress and improve well-being. 20 In line with previous literature regarding disclosure, our study suggests that these positive impacts occur when panellists feel supported. This enabled them to show their vulnerability, which facilitated human connection, 22 promoted audience response and reflections 22 and allowed staff to gain new insights based on a re-evaluation of their experience(s). 23 Speaking openly diminished the expectation of panellists to behave stoically, 3 resulting in perceived improvements in their physical and psychological well-being. 7
Panellists identified the need to feel safe before speaking openly. Panel preparation was a key aspect of this, and our data highlight instances where psychological safety was reduced, particularly where panellists did not receive preparation prior to the Round. Preparation served many functions in relation to safety. It enabled facilitators to check that it was the right time for the story to be shared, it allowed panellists to hear other panellists’ stories and it prepared facilitators for the emotions and themes that may be raised in a Round. 4
Consideration of the timing of a Round was found to be important, and it is imperative that those preparing Rounds carefully consider who they ask to present and when: not too soon or when the subject matter is emotionally raw.
Psychological safety ‘is a shared belief held by members of a team that the team is safe for interpersonal risk taking’26(p350) and a ‘sense of confidence that the team will not embarrass, reject or punish someone for speaking up’.26(p354) Our data suggest Rounds panellists need to feel emotionally safe to share their story/experience without fear of reprisal or blame. Facilitators foster a sense of psychological safety in Rounds through skilled facilitation, group work and psychological insights. Ground rules and use of an established protocol for Rounds help create a confidential and protective environment. This, together with a sense of community, is necessary for Rounds to work well. 4
The other key influence on the panellists’ experience was the audience’s reaction to their story. This was often perceived as a source of validation. The need for validation is unsurprising, given the criticism that health care employees often encounter due to increased regulation and surveillance and service pressures beyond their control.
Limitations
Our reported findings are based on interviews with a range of staff members who all participated as panellists in at least one Round. Sampling took into account the length of time the organization had been running Rounds and the duration since the individual had been a panellist.
However, some panellists’ interviews took place relatively soon after their involvement on the panel. As a consequence, some post-Round impacts may not have yet been realized. A longitudinal interview design enabling interviews at multiple time-points (including pre- and post-panel preparation, directly after panellists’ participation in the Round itself and over time in the following months) would allow for a deeper exploration.
Conclusion
Panellists are essential in providing the stories central to Rounds. Rounds implementation and sustainability depend on having panellists to share stories about the emotional impact of their work. This study has highlighted how disclosure and reflection through storytelling during Rounds support panellists with the emotional aspects of their work. Rounds create important spaces where health care workers can share their stories without risk of judgement. Rounds lead to increased empathy for self, colleagues and patients, as well as creating organizational cultural change by making emotions visible and normalized.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
The authors declare that this research meets the ethical guidelines. Ethical approval was granted by the National Research Ethics Service Committee London-South East (REC reference: 15/LO/0053).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper presents selected findings from independent research commissioned by the National Institute for Health Research (HS&DR – Project: 13/07/49); awarded to King’s College London. The views expressed in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, MRC, CCF, NETSCC, the HS&DR programme or the Department of Health.