
Abstract
Objectives
Improving patient experience is widely regarded as a key component of health care quality. However, while a considerable amount of data are collected about patient experience, there are concerns this information is not always used to improve care. This study explored whether and how frontline staff use patient experience data for service improvement.
Methods
We conducted a year-long ethnographic case study evaluation, including 299 hours of observations and 95 interviews, of how frontline staff in six medical wards at different hospital sites in the United Kingdom used patient experience data for improvement.
Results
In every site, staff undertook quality improvement projects using a range of data sources. Teams of health care practitioners and ancillary staff engaged collectively in a process of sense-making using formal and informal sources of patient experience data. While survey data were popular, ‘soft’ intelligence – such as patients’ stories, informal comments and observations – also informed staff’s improvement plans, without always being recognized as data. Teams with staff from different professional backgrounds and grades tended to make more progress than less diverse teams, being able to draw on a wider net of practical, organizational and social resources, support and skills, which we describe as team-based capital.
Conclusions
Organizational recognition, or rejection, of specific forms of patient experience intelligence as ‘data’ affects whether staff feel the data are actionable. Teams combining a diverse range of staff generated higher levels of ‘team-based capital’ for quality improvement than those adopting a single disciplinary approach. This may be a key mechanism for achieving person-centred improvement in health care.
Introduction
Patient experience – alongside patient safety and clinical effectiveness – is acknowledged as a key component of quality of care. 1 Whilst there has been considerable focus in several health systems on developing measures and collecting data on patient experience, there remains a gap between measurement and improvement. Collecting data but not using them to improve care is not only wasteful but arguably unethical. 2 Although some hospitals in the United Kingdom (UK) now have a designated ‘Patient Experience Office’, the office’s function is often primarily data collection and reporting rather than quality improvement, which may be led by a different department in the organization.
Previous studies examining how patient experience data are used for improvement have focussed on board or whole-organization level, and have often reported that interest in using experience data is not always matched by action or the skills to work with such data.3,4 Gleeson et al.’s 5 international systematic review of approaches to using patient experience data for quality improvement in health care confirms that quantitative surveys remain the most common form of patient experience data, and that qualitative data are more difficult to use in terms of time and expertise. Gleeson et al. note that patient experience-based improvement remains focussed on small incremental service changes, which do not require infrastructural or clinical-behaviour change.
There is some evidence of promising frontline approaches, including facilitated feedback of survey findings to ward teams 6 and experience-based co-design,5,7,8 using narrative and observational data. Sheard et al.’s ‘Patient Feedback Response Framework’ focusses on ward teams’ engagement with patient feedback 9 and identifies three components needed to effect change: normative legitimacy (staff’s personal belief in the importance of responding to feedback and desire to act); structural legitimacy (staff’s perception of sufficient ownership, autonomy and resources needed to establish a plan of action); and organizational readiness (senior hospital management/organizational support for the team to work on improvement, and capacity for interdepartmental collaboration).
Recurring themes in the literature are the misalignment of managerial expectations with how engaged and supported frontline staff feel to make improvements, along with issues concerning the way staff feel about the nature of the data.3,10–13 Flott et al. 3 outline a familiar set of challenges in using survey feedback at clinical level, including scepticism about data quality; lack of training in social research methods; isolated data not linked to other relevant data sources; statistical complexity and lack of technical guidance; and aggregation of data at National Health Service (NHS) Trust (i.e. institutional) level, which does not inspire local clinical ownership or inform ward-level improvements. More recently, Sheard et al. 13 report that frontline staff struggle with ‘the function and usefulness of the individual data sources’13(p4) and that, while managers recognize this, they seem ‘powerless to prevent the tsunami of ongoing data collection.’13(p6)
Martin et al. 14 outline the value of ‘soft’ intelligence – insights from qualitative and informal sources that might improve care. Despite recognizing its value, staff often do not feel confident to interpret or act on such data, while formal, managerial processes designed to render it useful and credible (including aggregation and triangulation) may inadvertently silence it at source. 15
Gaps in the evidence base
Two trends in the study of how patient experience data are used for quality improvement can be identified. First, the meaning of ‘data’ is often treated as a given, rather than examining what staff do in practice with the information they have and whether this information constitutes data. While ‘data’ are not always defined, they are assumed to encompass formally collected and organizationally sanctioned information, particularly from national and local bespoke surveys. Other sources of data have been less well investigated, leaving a knowledge gap as to what such data are or how they are marshalled by frontline staff in their day-to-day work. Without official organizational sanction, potentially useful intelligence may be disregarded.16,17
Second, studies of how data are used have focussed on contextual and attitudinal factors, but there has been less consideration of how team constitution affects the type and success of improvements undertaken.
In both respects, a focus is needed on the practical undertaking of quality improvement by frontline staff – that is, an orientation to what people do in practice rather than theories of change or post hoc accounts. In this ethnographic study, we documented how frontline hospital ward teams engaged with patient experience data when encouraged to do so, what challenges they faced and how they could be better supported to work on person-centred quality improvement.
Methods
Between July 2016 and July 2017, we undertook a case study evaluation in six hospital sites in England’s NHS, as part of a study commissioned by the UK National Institute for Health Research. 18
A lay panel of 10 people with recent personal or family experience of inpatient care, chaired by lay coinvestigator and coauthor JB, met regularly with the research group to reflect on and make sense of evolving findings.
Focussed team ethnography
Adopting a longitudinal design,19,20 three ethnographers (SP, CM and AC) collected various data from stakeholders at each site to understand how they used patient experience data, including observational fieldnotes, interviews, documents and photographs. Team ethnography is not uncommon in organizational research, but poses challenges and risks,21,22 given that no single ethnographer has detailed familiarity with all the sites and individual ethnographers’ interpretations may be difficult to reconcile or synthesize. This required deliberate strategies to communicate regularly, coordinate data collection and ensure analysis was shared and synthesized.
Among its advantages, team ethnography brings multiple lenses and professional experience to bear. The ethnographers had higher degrees in sociology and psychology, and diverse previous research experience. Schlesinger et al. 23 describe such team-based reflexivity as a positive model which ‘sets up a deliberative process that involves testing the work as it is being done.’23(p66) A team-based approach also enables a greater range, volume and complexity of work within the limited timespan of available funding. Team ethnography therefore enabled us to undertake focussed ethnography across six sites simultaneously. This provided a rapid and condensed alternative to lengthy immersion in conventional ethnography,24–26 with shorter, purposive site visits targeted around specific events or meetings.
Selecting and supporting the sites
Case study sites were purposively selected using a sampling frame derived from analysis of existing national UK survey data and a new survey of NHS hospital patient experience leads. Sites were selected to reflect a range of contexts, from hospitals that were performing well on routinely collected staff and patient experience measures and had a strong track record on quality improvement to those facing organizational challenges and where person-centred improvement was less embedded. Each site nominated a medical ward for the study. A team of staff from each ward took part in a two-day learning community and led their local improvement work. The sites were encouraged to include frontline staff in the core team but were ultimately free to decide on team composition. The learning community met three times during the project. At the first meeting, teams learnt about and discussed with the researchers and lay panel members different types of data such as surveys, narratives/interview data, observations, complaints and online feedback, and approaches to improving patient experience. On returning to their workplace, each team developed and implemented their own ideas for person-centred quality improvement. At the second learning community meeting, they presented their work and the researchers provided formative feedback. At the final meeting, the teams shared their experiences and showcased their achievements with the researchers and invited senior managers from the NHS trusts involved in the study.
Data collection and analysis
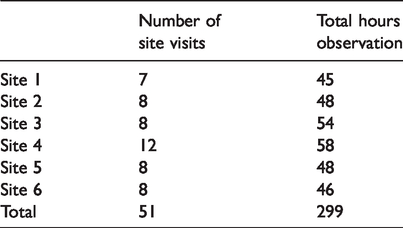
The three ethnographers observed the teams over one year and conducted interviews at the start, middle and end of the fieldwork period. They observed learning community events, local quality improvement planning meetings, meetings of patient and carer experience groups, general staff meetings and workspaces, supplemented by informal conversations with staff. Data collected included written fieldnotes, documents and photographs. The exact nature and amount of observation varied by site, depending on frontline staff’s chosen improvement activities, and was affected by severe workload pressures in the NHS (termed ‘organizational distress’ by one participant) during winter 2016–2017. The pressure on frontline staff to maintain services meant fieldwork was sometimes difficult to arrange or had to be cancelled at short notice. Table 1 summarizes number of visits and hours of observation per site (including learning communities). Not captured here is the amount of time spent emailing, texting and phoning to arrange fieldwork, unquantified activities, which were nonetheless important in building rapport and getting to know and understand teams.
Observations per site.
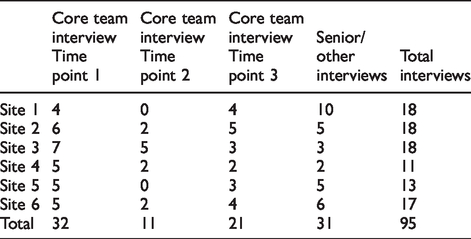
Ninety-five in-depth, audio-recorded interviews with frontline staff and senior managers were undertaken (Table 2), using a shared interview guide. Again, winter pressures created difficulties arranging interviews, particularly at the mid-point of our study.
Interviews conducted by site.
Qualitative data were analysed iteratively by the three ethnographers using an inductively generated coding framework in NVivo 10/11. This included types of patient experience data used, attitudes towards/understanding of data, team composition and membership, relationships with the Patient Experience Office and senior management, and organizational pressures and constraints. As part of the research group’s ethnography design, the group met regularly with the Principal Investigator (PI) during the fieldwork to ensure comparability of data collected and to discuss emerging analysis, developing theoretical explanations as the work progressed. ‘Thick’ case descriptions (incorporating rich contextual detail and interpretation) were produced for each site, along with process maps of each team’s quality improvement projects, as part of a thematic analysis. In line with the protocol, all sites are anonymized to ensure participants felt comfortable sharing more negative views and experiences.
By the end of the project, teams in every site had undertaken improvement initiatives using a variety of data sources. In some cases, this was a single intervention, while in others it involved multiple interlinked projects on a suite of different topics. Our aim in this study was not to quantify change or rank sites in terms of ‘success’ – given that sites were selected deliberately to represent a range of starting points and levels of maturity in working on patient experience, variation in progress was expected. However, some teams undoubtedly struggled more than others. Our focus was rather on a comparative understanding of how staff approached their projects on patient experience, why some struggled and how they made sense of the task.
Below we present an overview of findings on two key themes: the meaning of patient experience data and team-based capital.
Results
The meaning of patient experience data
We observed teams engaging in a process of sense-making, drawing on a spectrum of formal and informal sources of intelligence. However, it was not initially obvious to frontline staff what patient experience ‘data’ were, where to locate them in the organization or how to use them. Surveys were the most recognized source of information; however, available survey data were commonly not ward-specific and therefore less useful for frontline quality improvement.
Qualitative data – such as patient stories and free text feedback at the end of surveys – were appealing to staff, seen as convincing evidence and reflecting real experience, but remained under-utilized due to lack of confidence in how they could be used. Few staff had considered observation or shadowing as a source of data until introduced to this by the research group at the first learning community event. Some teams successfully went on to experiment with observations. Online feedback on social media attracted initial interest, but lack of organizational support to access and use it at ward-level prevented team engagement.
The emotional response that patient experience data elicited in staff was evident. Staff were receptive to and motivated by positive feedback from patients, but did not tend to see this as a source of ideas for quality improvement. Negative feedback was reported to be useful, but in practice could be challenging or difficult to accept for staff and, depending on the form it took, inhibited efforts at improvement.
At times, staff were unable to point to a specific piece of patient experience data that led to a particular improvement project. As one consultant said, ‘[The quality improvement intervention] fits right, but I don’t think they’ve done a survey.’ The ethnographer’s accompanying coding note observed, ‘[This] sums up what I think is happening with a lot of the teams … the issues are known to staff and they are responding, without being able to identify any specific piece of patient feedback.’
In another case, a staff member commented, ‘I hadn’t actually heard of patient experience until I went to the learning community.’ This demonstrated the disjunction between patient experience as an organizational and policy construct on the one hand and daily practice on the other.
Sometimes staff reported acting on what they felt they already knew needed changing. This knowledge might come from caring for and observing people, or conversations with carers or colleagues. Taking part in the project gave them a platform to pursue existing concerns and ideas. In some cases, such staff-initiated improvements were backed up by formal patient experience data. This is demonstrated in an interview with a ward manager: Ward manager: You need to remember that the staff are doing a job all the time. They have ideas that might improve the service … Interviewer: Things like the hearing aid boxes I think came from the staff suggestion board, didn’t it, rather than from the patient experience data? Ward manager: Yeah, all of that just came up because we could see the distress … [The ward administrator] deals with a lot of the lost property, the distress of the patients that have lost an expensive hearing aid and they can’t communicate at a time when they most need to communicate clearly … .That came from, you know, our own experience of what causes them distress.
As the project progressed, those involved in the research – both as participants and as researchers – began to work with an expanded notion of patient experience data. One patient experience officer described this as ‘just general conversations with patients’, encompassing tacit, embodied experience and fleeting observations during daily practice. The officer went on to explain: It depends how we look at data. I think in the ward staff before, if you said to them, ‘What’s patient experience data?’ they will say, ‘Surveys.’ I’m saying to them now, ‘Data is any feedback at all, wherever that’s coming from and in whatever form, whether that’s coming from focus groups from the patients or anecdotal feedback from staff and patients, it’s all patient experience data.’ Ward managers are asked to keep a log of any compliments, and then – it sounds really crass – boxes of chocolates – count the number of boxes of chocolates you have and thank you cards. The challenge is there are several, many staff who work within the Trust who will be completely unable to see the impact of their behaviour or their – let’s say – their brusqueness … So that’s a real fine balance, isn’t it? ‘Cos there are people who won’t get that at all. They won’t see that that’s bad patient experience.
Team composition and resources
The composition of the frontline teams who took part in the project was determined locally. Each consisted of up to five core individuals. When we recruited sites, we encouraged them to identify a core team of frontline staff (and patients) for the first learning community. Teams interpreted ‘frontline’ differently. Some included from the outset a staff member from their local Patient Experience Office who was assigned to work closely with them on the project. Others brought a ward-only team to the event but liaised closely with the Patient Experience Office during the project. Despite an emphasis at learning community events on mapping key stakeholders and sources of support, a few teams maintained a more distant relationship with their in-house patient experience team. Team composition thus ranged from entirely nursing-led to a mix of nurses, doctors, unqualified nursing assistants, ward administrators, allied health professionals and staff from the hospital’s Patient Experience Office (see Table 3). The disciplinary and pay-grade mix of each team varied considerably, suggesting that there wasn’t an accepted home for patient experience improvement within these organizations.
Team composition and quality improvement projects.
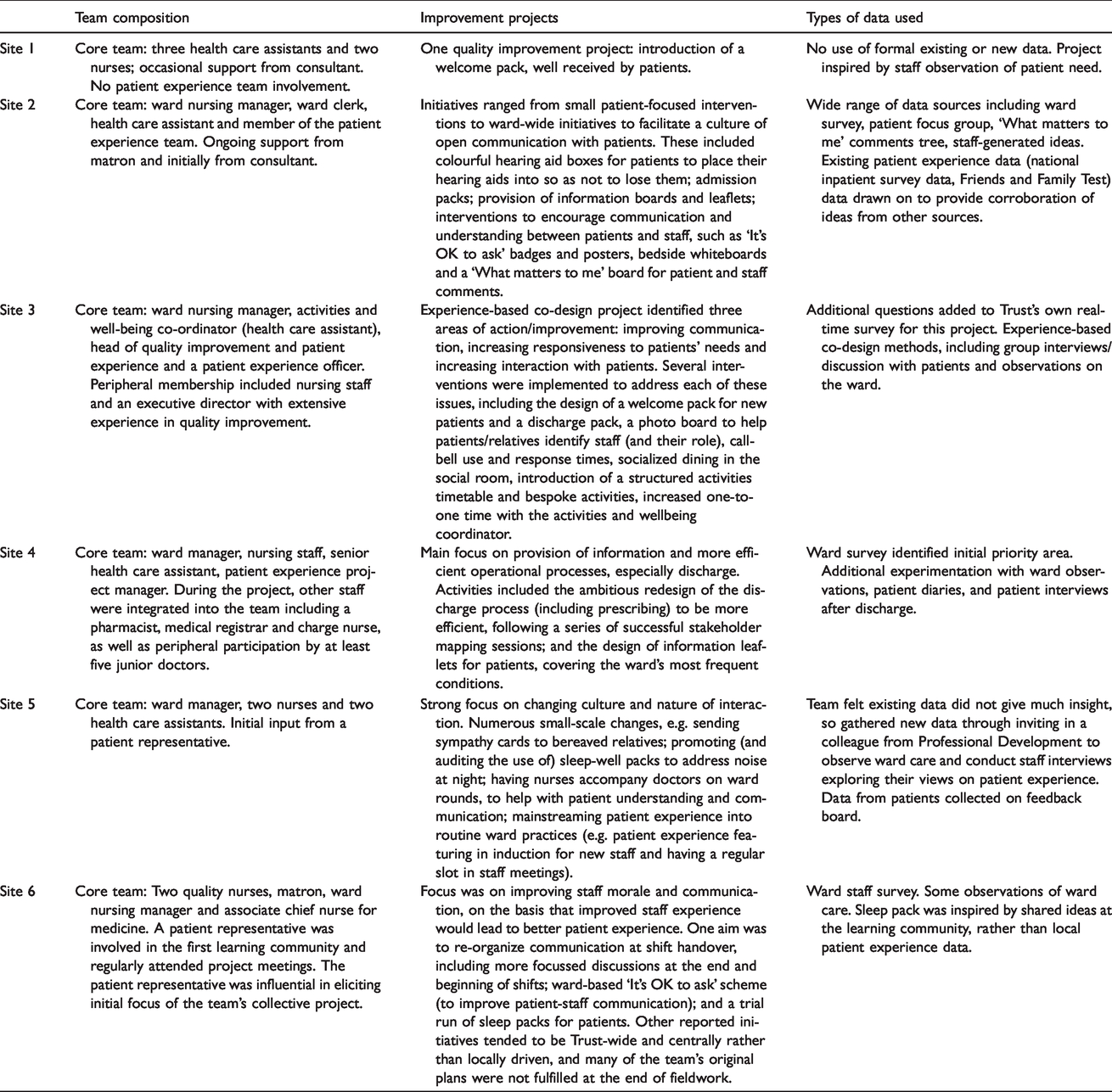
Teams consisting of a variety of different professionals tended to make more progress with their chosen quality improvement projects and work on a wider range of topics. Staff did not necessarily need to be senior or from a particular profession to effect change: in one team, a ward administrator was pivotal in making practical changes; in two sites, nursing assistants played important roles; in another, the dynamic and focus of the project changed as a pharmacist and junior doctors in training became involved as peripheral team members. By contrast, one team, which consisted entirely of relatively senior nursing staff, did not seem to make much progress at ward level. In addition, those teams with a close relationship to the Patient Experience Office tended to be more ambitious in the improvement activities addressed. Patient Experience Office staff were well positioned to provide data (and the skills to interpret it) and act as project managers, variously sourcing materials, generating resources, taking plans forward and maintaining momentum.
‘Space’ was a recurring theme: physical space in terms of places to meet, and figurative space – space in the day amidst heavy workloads and shift patterns with limited handover times, and cognitive capacity to take on projects (or ‘head space’ as one person described it). Below, a senior sister explains how resources provided by a patient experience officer increased team capacity: If you look at my job description, improving is obviously something that’s in there. But I’ve got a full-time job that doesn’t really give me any additional time to take on a big project … So you do need a project manager that’s got the time and resource and that’s her job … It’s a relief that I’ve got someone else in the background, because I know if it was left to me to organize meetings it probably wouldn’t get very far. All I’ve done is the paperwork to say, ‘This is what we want to do, and we want £1000 please.’ … I’ve done loads of bids before, usually for equipment and, yeah, I know how to do it, and I think they looked at it and thought, ‘Oh God, this is going to take us hours,’ but in fact it doesn’t. You know, it took me half an hour … I suppose the nurses would struggle with that because they don’t know these people, and that’s something that I could just do at the click of a button.
Restricted team membership could be compounded by other practical resource challenges. This could be as simple as having no quiet space to meet. One ethnographer’s fieldnote mentioned: [The team member] left her room and took us to the family room, but noting that it was now occupied by junior doctors in meeting, she decided we would have the meeting in the reception area. En route to the reception area, she spotted an empty single bedroom (approx. 8ft by 4ft room) and decided to hold the meeting there. We have found hurdles all of the time … Trying to get money to start with. You know, we were phoning up in our own time, phoning people, companies – ‘Can you do this for such a price? Can you do this for such a price?’ … So, we were bartering all of the time.
Discussion
The formation of teams of people from different disciplines and grades established a network of individuals with assorted levels of Bourdieu’s 27 four forms of capital: economic, social, symbolic and cultural (see Table 4). We suggest this is a key mechanism for achieving person-centred improvement in the NHS.
Capital in the NHS.

NHS: National Health Service.
Team-based capital operates both through the differing knowledge and skills individual team members bring, and through their ability to generate varied practical, organizational and social resources for patient-centred quality improvement. While organizational rhetoric stresses the value of good patient experience, in reality it may still have lower organizational priority than patient safety and clinical effectiveness. 2 A coalition of people and resources is important to challenge this fragile status and raise the profile of patient experience work.
Linked to this is the question of what counts as patient experience data, and what is formally sanctioned by the organization as important and actionable. A key finding from this work is the expanded notion of ‘data’. We question whether data have to come directly from patients to constitute ‘patient experience data’, and for expressions or understandings of patient experience to be formally recorded or documented to count. In her work on patient experience in mental health units, Pols 28 noted that nurses’ intuitive understanding from daily practice was a valuable additional insight alongside interviews. Nurses, she argued, ‘attend to what silent patients like or dislike … They seem to know what individuals prefer, and if they do not, they try to find out by trial and error.’28(p210) At the same time, she acknowledged the risk that ‘there are situations in which a conflict is clear, and in which nurses do not take the appreciations of patients into account or overrule them.’28(p217) This may have a parallel in the patient safety field with the concept of ‘exnovation’ – understanding how good safety is often accomplished through staff’s existing, taken-for-granted practices or ‘hidden competence’, rather than explicit new innovations. 29
Staff with the least power in the organization – unqualified nursing assistants, ward administrators, cleaners and porters – may be rich in this kind of tacit, embodied intelligence but are unlikely to be able to mobilize such knowledge for improvement without wider team capital behind them. This resonates with Sheard et al.’s account of structural legitimacy (whether staff feel they have sufficient ownership, autonomy and resources to act on patient experience data). 9
Limitations
Our findings are derived from only six UK hospital sites, but nevertheless provide rich data relevant for other contexts both nationally and internationally. We did not set out to demonstrate whether particular types of patient experience data or approaches to quality improvement are more effective than others, and we are therefore unable to draw conclusions on this point.
Conclusion
We suggest that frontline ward teams, as well as senior managers, need support in recognizing and harnessing a wider range of patient experience data for health care improvement, and to understand where such data reside within the organization. This signals a shift from top-down measurement for performance to an approach which embraces frontline wisdom and creativity, and involves a broad coalition of staff in improvement work.
We recommend particularly that those leading patient experience work in hospitals actively seek to include not just authoritative senior figures, but also hands-on frontline staff, whose perspective too often remains unvoiced and unnoticed. Patient Experience Office staff themselves also need support in engaging with multiple forms of data. As one contribution to this, we have worked with the Point of Care Foundation, an independent charity providing evidence and resources to support health care in the UK. 30 We have produced an open-access guide to using patient experience for improvement, aimed at frontline staff and patient experience teams and incorporated into face-to-face training courses led by the Foundation. 31
Footnotes
Acknowledgements
The authors would like to thank the following: the ward teams and senior management teams at the six participating case study sites. Neil Churchill, Angela Coulter, Ray Fitzpatrick, Crispin Jenkinson, Trish Greenhalgh and Sian Rees who were co-investigators on the study, contributing to the original design and conduct of the study. Esther Ainley and Steve Sizmur from Picker Institute Europe, who contributed to data collection and analysis. Prof. John Gabbay and Prof. André le May, University of Southampton, for facilitating the learning community meetings. The members of the lay advisory panel: Barbara Bass, Tina Lonhgurst, Georgina McMasters, Carol Munt, Gillian Richards, Tracey Richards, Gordon Sturmey, Karen Swaffield, Ann Tomlime and Paul Whitehouse. The external members of the Study Steering Committee: Joanna Foster, Tony Berendt, Caroline Shuldham, Joanna Goodrich, Leigh Kendall, Bernard Gudgin and Manoj Mistry. At the time of conducting the research LL and SP were employed by the University of Oxford.
Preliminary findings from the study have been presented publicly at the following conferences: European Association for Communication in Healthcare 2016; The International Society for Quality in Healthcare 2017; Health Services Research UK 2017; Medical Sociology 2018.
The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the NIHR Health Services and Delivery Research Programme 14/156/06. EG was funded by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care Oxford at Oxford Health NHS Foundation Trust. LL was supported by Oxford NIHR Biomedical Research Centre.