
Abstract
Objectives
Globally, populations are rapidly ageing and countries have developed health promotion and wellbeing strategies to address increasing demand for health care and old-age support. The older population is not homogeneous however, and includes a large group in transition between being active and healthy to being frail, i.e. with early frailty. This review explores the extent to which policy in England has addressed this group with a view to supporting independence and preventing further progression towards frailty.
Methods
A narrative review was conducted of 157 health and social care policy documents current in 2014–2017 at three levels of the health and social care system in England.
Findings
We report the policy problem analysis, the shifts over time in language from health promotion to illness prevention, the shift in target populations to mid-life and those most at risk of adverse outcomes through frailty, and changes to delivery mechanisms to incentivize attention to the frailest rather than those with early frailty. We found that older people in general were not identified as a specific population in many of these policies. While this may reflect a welcome lack of age discrimination, it could equally represent omission through ageism. Only at local level did we identify some limited attention to preventative actions with people with early frailty.
Conclusion
The lack of policy attention to older people with early frailty is a missed opportunity to address some of the demands on health and social care services. Addressing the individual and societal consequences of adverse experiences of those with the greatest frailty should not distract from a more distinct public health perspective which argues for a refocusing upstream to health promotion and illness prevention for those with early frailty.
Background
Globally, most populations are ageing rapidly, accompanied by an epidemiological shift to a predominance of chronic and long-term health problems. 1 This transition requires decision makers to address increasing demand for health care and old-age support in the context of a declining labour force. 2 Principles and key actions for national policy makers were agreed in the 2002 Madrid International Plan of Action on Ageing. This addressed three priority areas: older people and development; advancing health and well-being into old age; and ensuring enabling and supportive environments. 3 It also included agreement on implementation strategies, 3 with for example the regional strategy for Europe committing “to strive to ensure quality of life at all ages and maintain independent living including health and well-being” (p.13), underpinned by policies supporting health promotion and disease prevention. 4
Older people are not a homogenous population however and the concept of frailty provides a means to differentiate those most at risk of adverse outcomes and who use most health and social care resources. 5 Frailty “is a state of vulnerability to poor resolution of homeostasis following a stress and is a consequence of cumulative decline in multiple physiological systems over a lifespan” and is common among those aged over 75 years. 5 A spiral of worsening frailty has been identified with increasing disability, risk of unplanned hospital admission and moving into care homes. 5
Reducing distressing and costly unplanned hospital admissions for older people is a policy objective in many health care systems although the evidence base on the preventative actions that could best achieve this goal are unclear. One strategy could be to re-focus attention ‘upstream’ 6 to health promoting and preventative actions with older people who are in transition from being robust towards frailty, i.e. with early frailty. This group is reported to constitute 44% of older people in high and middle-income countries. 7 The extent and mechanisms within health policy that this re-focusing involves have not been explored. This paper reports on a policy analysis 8 of the extent to which health and social care policy in England addresses health promotion with older people with early frailty. We use the term early frailty throughout, in line with the accumulation of deficits conception, which considers a gradation of frailty and vulnerability rather than using pre-frailty, which describes a specific clinical state or phenotype. 5
Policy review and analysis help explain successes and failures, identify gaps as well as plan for future reforms. This study focused on one country, England, recognizing the importance of context in policy analysis. 8 It was framed by theories of public policy as processes including problem analysis, formulation and implementation in which different interests, interest groups, institutions and ideas interact. 9 These theories include recognition of the exercise of power (overt, indirect and latent) by different interest groups; within this context, we considered the influence of ageism, that is discrimination or unfair treatment based on a person’s age. 3
In England, the evidence of changing demography, epidemiology and their potential impact on the economy and public spending has been known to governments for decades and this was recently re-quantified. 10 There has been ministerial commitment to the Madrid Plan of Action 3 and subsequent re-affirmations. This has translated into a range of policies that specify the promotion of health and wellbeing for older people and maintaining independence features as strategic objectives, including those for longer working lives, 11 housing 12 and transport. 13 We investigated how health promotion for older people with early frailty has been constructed within English health and social care policy documents, which policies have been developed, and how they have been implemented at different levels of the legal and administrative system.
Method
A narrative review was undertaken using documentary analysis.
14
We considered policy development at three
levels:
9
(i) state
laws, (ii) strategies and plans of government-mandated national bodies for health and social
care and (iii) government-mandated bodies at local administrative levels for health and
social care. Policies had to be current between 2014 and 2017, that is, we considered
current legislation, strategies and plans published in 2014–2017, or that were referred to
as current on government websites or documents of the period (which could also include
policy documents that were published before 2014 but that had remained valid in the
observation period). Policy documents had to address one of the following: A population of older people (without an age-specific definition). Public health and wellbeing for whole populations including older people. Publicly funded health and social care services for whole populations including older
people.
We conducted internet searches of government websites periodically between 2014 and 2017 and of a representative sample (covering all regions and a range of socio-demographic features) of 10 local government websites and those of the corresponding local National Health Service (NHS) health services commissioning organizations (Clinical Commissioning Group, responsible for the planning and purchasing of most health care services for their local patient population) in 2015 and updated in 2017. We used snowball technique to follow linked policies. Included documents were reviewed for key words, such as ‘older people’, ‘elderly’, ‘frail’, ‘frailty’, ‘health promotion’, ‘ageing well’. Relevant surrounding text on the problem analysis, planned actions and stated intent as well as absence of attention to this group was noted. The iterative analysis was discussed within the research team and synthesized using narrative analysis.
Findings
Our searches identified 79 national level and 78 local level documents for analysis.
All policy documents re-stated, at the beginning, the policy problem analysis of the ageing
population with a changing epidemiological profile and the consequences for society
(national and local). This is exemplified in the 2010 national public health white
paper,
15
the 2014
NHS Five Year Forward View (a national plan for the English NHS)
16
and local government Health and Well Being
Strategies,
17
respectively: “Today, people in England are healthier and are living longer than ever
before……. We expect more people to have long-standing illnesses in future, and common
mental health disorders are on the rise.” (Department of Health,
15
p.11) “So the NHS needs to adapt to take advantage of the opportunities that science
and technology offer patients, carers and those who serve them. But it also needs to
evolve to meet new challenges: we live longer, with complex health issues, sometimes
of our own making.” (NHS England,
16
p.2) “The ageing population, economic downturn and resultant austerity measures has
placed an even greater burden on the health challenges for our city.”
(Liverpool City Council,
17
p.4)
Policy formulation: Shifts in language and target group
Policy formulation at national level included directions for Local Authorities, 18 the NHS 16 and for social care provision 19 to take ‘preventive actions’ for all adults. We noted a change of language over time in these documents. The term ‘health promotion’ was evident in an overarching document guiding services for older people, the 2001 National Service Framework for Older People (NSFOP), 20 which was re-endorsed without revision in 2017. Yet this term was not used in subsequently published and current policy documents. It was used only in policies addressing children and young people. 18 Policies concerned with older adults used more specific language such as ‘prevention of ill health’ in pursuit of the policy objective of reducing premature deaths. 21 Prevention of ill health became a priority strategy for the health and social care system in addressing the ageing population as embedded in legislation and government directions to national public services15,18,19 and in the objectives passed from national bodies to local public services.22,23
The 2014 Care Act 19 for the first time mandated the social care system to promote wellbeing and prevent or delay the need for care, recognizing different levels of preventative activity. 24 Prior to the issue of the law, these were objectives associated with the ‘health’ system. This is perhaps illustrative of the wider policy aspiration for greater integration between the health and social care systems, particularly in relation to increasing care provided outside hospitals for older people (among others) with long-term conditions.18,25
Our analysis further showed that the target population for prevention has also shifted. The aforementioned NFSOP of 2001 identified three groups: the well and healthy, the frail and a transition group between the two, 21 essentially those with early frailty. However, there was little explicit consideration of those with early frailty in later policies reviewed here.
Policy implementation and delivery mechanisms
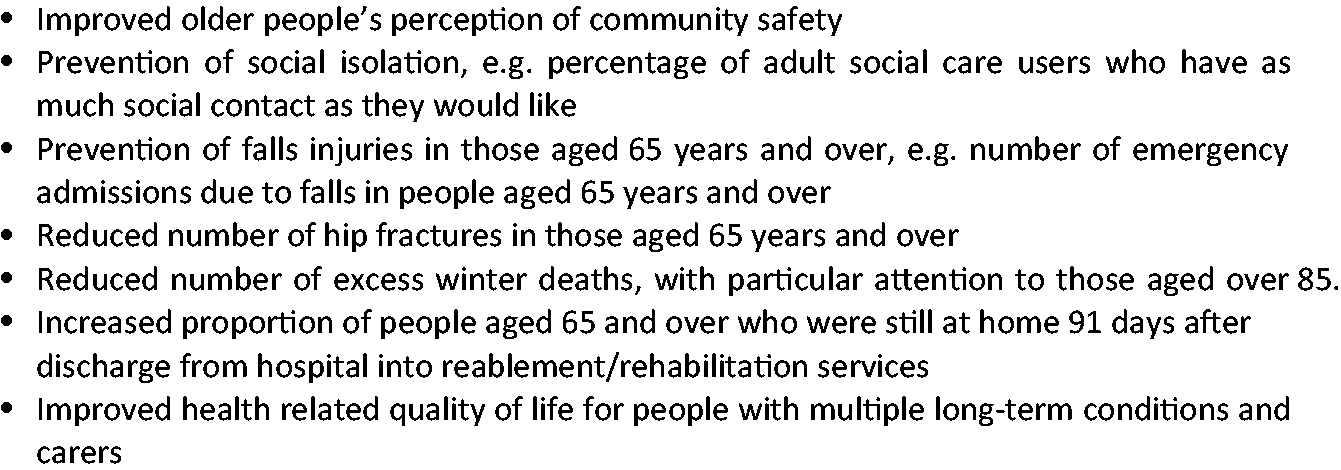
Policy implementation has been directed from the national level with specified health improvement outcome measures for public health, the NHS and adult social care that include older adults.26–28 These include the public health objectives across the population for increasing physical activity, decreasing obesity and decreasing smoking. Primary prevention objectives of cancer screening and vaccination coverage targets are age specific, for example, increasing influenza vaccination coverage in the over 65s. Other objectives and outcomes are summarized in Figure 1.
The term ‘older people with frailty’ featured rarely at the different levels examined here. In social care policy, it was only used three times as one of a number of examples of types of people who needed additional social care attention. This concerned older people as a specified group in judicial determination of intimidated witnesses, as an example of the types of people with care home debts and as people with confusion due to infections. 24 In public health policy, it was used only in relation to the population experiencing excess winter deaths 16 and translated into local level action through the annual joint cold weather plans as directed by Public Health England. 29 In health service policy, it was only used in relation to improved integration of services for the most vulnerable, particularly for those with long-term conditions.25,30
We identified a range of mechanisms for achieving these objectives set out in
national-level policies. Within the responsibilities assigned to Local Authorities, we
identified the following mechanisms, some of which were more prescriptive than others:
Directions for inclusion of preventative actions for older people across all
responsibilities and activities, for example for safe neighbourhoods, leisure and
housing,
24
The provision of the NHS Health Check programme (through their public health
function from 2013) aimed to prevent heart disease, stroke, type 2 diabetes and
kidney disease, and raise awareness of dementia both across the population aged
40–74 years and within high risk and vulnerable groups.
31
This has mostly been commissioned
through general practice but in some areas through local pharmacies and community
leisure/sports facilities.32,33 The creation of community agent roles (volunteer support in rural areas) and
community groups by the voluntary sector to support adults over the age of 60 at
risk of becoming socially excluded.
15
Within the responsibilities of the NHS, we identified the following mechanisms for
achieving the outcomes: The provision of primary prevention activities such as discussing and recording of
smoking status and offering smoking cessation support within the Quality and
Outcomes Framework (a pay-for-performance scheme in primary care) in general
practice.
34
The provision of a named and accountable general practitioner (GP) for all those
patients aged over 75,
35
with a responsibility to provide a health check on request if
there has not been a medical examination in the previous year. The option for general practices to provide the proactive care programme within the
general practice contract 2014–2015.
36
This programme aimed at preventing
unplanned hospital admissions and support living at home for the most frail and
other vulnerable groups.
These seven delivery mechanisms span statutory and voluntary services, utilizing general medical practice for four of them. The mechanisms involve volunteers, trained peers, non-professionally qualified staff as well as professionally qualified staff. They range from broad types of preventative actions without associated identified finance to those for general practice which were more specific and financially incentivized.
The extent to which the preventative actions address those with early frailty is
debatable. For example, the NHS Health Check primarily targets a younger
population
32
and
the provision of a health check for those over 75 did not specify what that included or
suggested that it presented the opportunity for prevention in those with early frailty.
The proactive care programme
36
was targeted at the frailest two per cent of the older population at
risk of unplanned hospital admission. It was a companion to other policies aimed at
supporting frail older people to remain independently at home, such as the improved
integration of health and social care services
25
and the creation of the Better Care Fund
(a programme seeking to join up health and social care services).
37
These policies aimed to
build bridging mechanisms in the context of a system where publicly funded health care and
social care are divided by different funding mechanisms, governance, commissioners and
provider organizations.
38
These exemplars35,39,40 illustrate the attention
given at all levels of the legal and administrative system to integration of planning and
services in order to reduce unplanned hospital admissions of frail older people: “The NHS Commissioning Board [NHS England from 2014; the national
public body leading the NHS in England] is uniquely placed to coordinate a
major drive for better integration of care across different services.…… Local
commissioners have the vital role of stimulating the development of innovative
integrated provision – for example, across primary, secondary and social care, or
for frail elderly patients.” (sections 2.7, 2.8, 2.9 in Department of
Health
39
) “The new 2014/15 enhanced service (‘Avoiding unplanned admissions: proactive
case finding and patient review for vulnerable people’) now referred to as the
‘proactive care programme’– is designed to bring about a step change in the quality
of care for frail older people and other patients with complex needs.” (NHS
England
35
,
p.1) “Improving primary care … to do this we will implement the clinical
commissioning improvement plan which is designed to support the strategic principle
of shifting the delivery of care closer to home, building strong local integration
of care, focussing on supporting improvement in the management of frail elderly and
complex patients; building on the requirements to support people over 75 contained
in the core primary care contracts, as well as the new admission avoidance Directed
Enhanced Service.” (Dorset Clinical Commissioning Group,
40
p.13).
The extent to which the other mechanisms listed above were visible in local strategies in 2015 varied, with most being described in broad non-specific terms as illustrated in Figure 2.41,42 It should also be noted that one third of the local areas’ Joint Health and Wellbeing Strategies of the nine we examined did not contain specific priorities for older people.
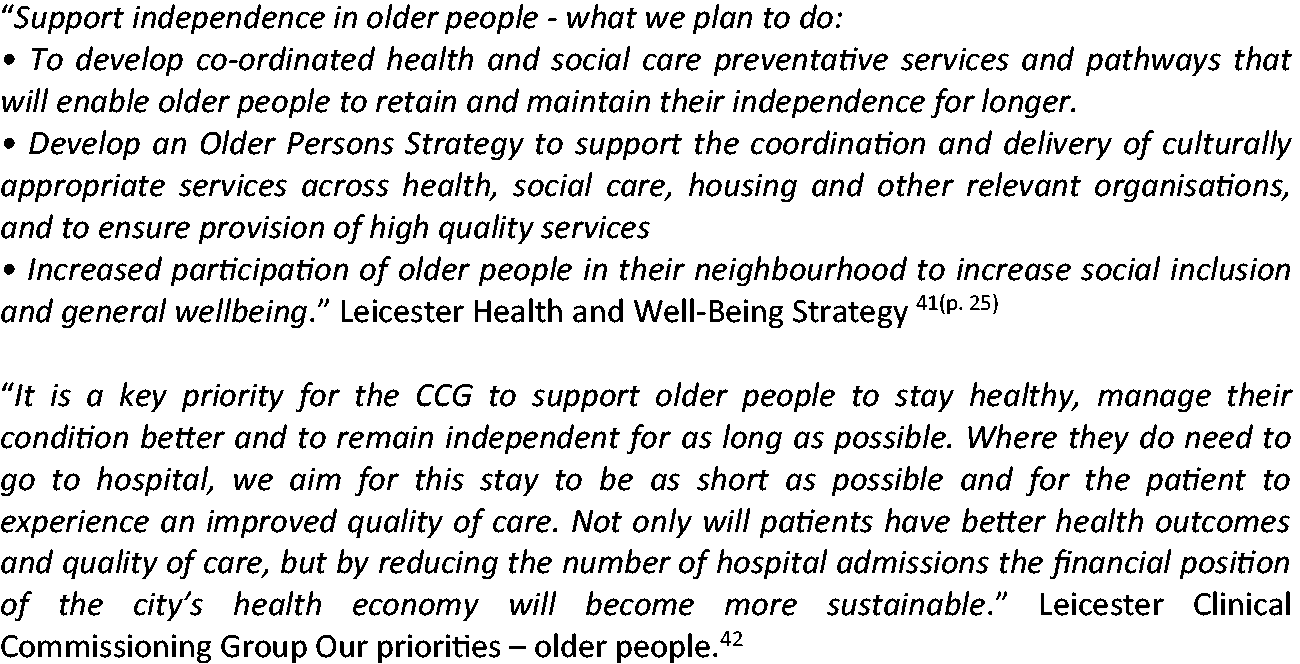
Exemplars of priorities for health and care of older people in local strategies.
Our review also included nine joint NHS and Local Authority Sustainability and Transformation Plans (five-year plans covering all aspects of NHS spending in England in a defined geographical area), which covered our 2015 local areas. All had priorities for preventative activities but only four related these to the older population. Four mentioned services for frail older people and two of these only in relation to those who were medically unwell (Appendix 1).
Policy iterations and outcomes
A key challenge for policy evaluators is to quantify the impact of preventative measures which are often long-term in their ambitions. 43 Just as there has often not been a specific focus on older people or those with early frailty in the policies reviewed here, there has been no specific published evaluation of impact for this group. One explanation may be the localism inherent in the major policy reforms of the period under review (2014–2017) that resulted in an absence of evaluation at scale. Another possible explanation is that the lack of attention is influenced by the pervasive nature of ageism in society. Oliver et al. 44 argued that it is the latter, citing the absence of older people and those with frailty in the planning and scrutiny work of joint Health and Wellbeing Boards composed of Local Authorities, local NHS commissioners and others.
Mechanisms that did not have specified public funding attached, such as community agents, are harder to judge in respect of the extent of implementation and outcome. An internet search identified that some rural areas have incorporated these ideas in wider village agent schemes (Appendix 1), but these were not necessarily focused on older people or those with early frailty.
Conversely, for initiatives that were supported by public funding, there is some evidence of published evaluations and indications of implementation. For example, an evaluation of the NHS Health Check found higher uptake by those aged 60–74 years than younger groups and variable patient experiences. 45 However, it was not designed to address the needs of those with early frailty. The proactive care programme was focused on the most frail older people and funded for three years (2014–07). By 2015, the majority of general practices were providing the proactive care programme (7431 of 7841 in England). 46 Evidence of its specific impact for frail older people and other vulnerable groups is difficult to separate from the wider range of local interventions addressing improved integration of services 37 and care management for people with multiple long-term health conditions. 47 However, the policy has now changed and the proactive care programme has been replaced within the national 2017–2018 general practice contract. 48 All general practices are now required to identify those with moderate and severe frailty, using a defined index and then focus clinical attention on those “living with severe frailty, the practice will deliver a clinical review providing an annual medication review and where clinically appropriate discuss whether the patient has fallen in the last 12 months and provide any other clinically relevant interventions”. 48 There are no explicit specific health promotion or prevention components to this contractual requirement.
Discussion and conclusion
This review has analysed contemporary health and social care policy for health promotion for older people with early frailty in England. The review is time limited but this is mitigated by the inclusion of current policies some of which were published before the period under investigation. However, even by using a defined time period and type of policy document, our searches may have missed some local examples with greater focus on early frailty although we tried to address this through our iterative search processes.
We found that the older population was not always identified separately as a policy priority. From documentary evidence alone, it is not possible to determine whether this represented a positive lack of age discrimination or a negative lack of attention to the specific problems of some older people. Other analysts have argued that institutional ageism exists in international health policy. 49 Over time the discourse in these policy documents changed from broad health promotion for older adults, to the specific prevention of ill health and targeted either those most frail or those in mid-life, that is an ‘upstream’ public health solution 6 to earlier in the life course.
There was an absence of policy focus on those on a pathway to frailty. As noted in the introduction, this group is estimated to comprise a considerable proportion among those over 65 years, 7 a population that is predicted to grow in all countries. 1 Publicly funded or supported services seeking to develop health promotion for older people with early frailty may find it difficult to legitimize their plans without a policy ‘rationale’ to support it among other competing priorities. By merely addressing the adverse events experienced by those with frailty, opportunities are being missed to ‘refocus upstream’ 6 on health promotion and illness prevention among those on the pathway to frailty.
Supplemental Material
Appendix - Supplemental material for Moving upstream in health promoting policies for older people with early frailty in England? A policy analysis
Supplemental material, Appendix for Moving upstream in health promoting policies for older people with early frailty in England? A policy analysis by Vari Drennan, Kate Walters, Christina Avgerinou, Benjamin Gardner, Claire Goodman, Rachael Frost, Kalpa Kharicha, Steve Iliffe and Jill Manthorpe in Journal of Health Services Research & Policy
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is funded by the National Institute for Health Research (NIHR) Health Technology Assessment (HTA), grant reference number 12/192/10. The views and opinions expressed are those of the authors and do not necessarily reflect those of the Health Technology Assessment programme, NIHR, NHS or the Department of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.