
Abstract
Objectives
Integrated funds for health and social care are one possible way of improving care for people with complex care requirements. If integrated funds facilitate coordinated care, this could support improvements in patient experience, and health and social care outcomes, reduce avoidable hospital admissions and delayed discharges, and so reduce costs. In this article, we examine whether this potential has been realized in practice.
Methods
We propose a framework based on agency theory for understanding the role that integrated funding can play in promoting coordinated care, and review the evidence to see whether the expected effects are realized in practice. We searched eight electronic databases and relevant websites, and checked reference lists of reviews and empirical studies. We extracted data on the types of funding integration used by schemes, their benefits and costs (including unintended effects), and the barriers to implementation. We interpreted our findings with reference to our framework.
Results
The review included 38 schemes from eight countries. Most of the randomized evidence came from Australia, with nonrandomized comparative evidence available from Australia, Canada, England, Sweden and the US. None of the comparative evidence isolated the effect of integrated funding; instead, studies assessed the effects of ‘integrated financing plus integrated care’ (i.e. ‘integration’) relative to usual care. Most schemes (24/38) assessed health outcomes, of which over half found no significant impact on health. The impact of integration on secondary care costs or use was assessed in 34 schemes. In 11 schemes, integration had no significant effect on secondary care costs or utilisation. Only three schemes reported significantly lower secondary care use compared with usual care. In the remaining 19 schemes, the evidence was mixed or unclear. Some schemes achieved short-term reductions in delayed discharges, but there was anecdotal evidence of unintended consequences such as premature hospital discharge and heightened risk of readmission. No scheme achieved a sustained reduction in hospital use. The primary barrier was the difficulty of implementing financial integration, despite the existence of statutory and regulatory support. Even where funds were successfully pooled, budget holders’ control over access to services remained limited. Barriers in the form of differences in performance frameworks, priorities and governance were prominent amongst the UK schemes, whereas difficulties in linking different information systems were more widespread. Despite these barriers, many schemes – including those that failed to improve health or reduce costs – reported that access to care had improved. Some of these schemes revealed substantial levels of unmet need and so total costs increased.
Conclusions
It is often assumed in policy that integrating funding will promote integrated care, and lead to better health outcomes and lower costs. Both our agency theory-based framework and the evidence indicate that the link is likely to be weak. Integrated care may uncover unmet need. Resolving this can benefit both individuals and society, but total care costs are likely to rise. Provided that integration delivers improvements in quality of life, even with additional costs, it may, nonetheless, offer value for money.
Introduction
The sharp demarcation of health and social care systems has been described as a ‘Berlin Wall’. 1 Care systems have typically evolved on the presumption that people who are ‘sick’ can be easily distinguished from those who are ‘frail’ or ‘disabled’. 2 However, an increasing proportion of the population has complex needs. This includes the older population with chronic diseases and multiple morbidities,3,4 children born with complex conditions who are now living to adulthood, and people with learning disabilities who may need continuous care. 5 For these people, care delivery systems that are predominantly designed for acute illness may be both inappropriate and inadequate. 6
The common sense response to this ‘Berlin wall’ is to dismantle it by integrating care across health and social care boundaries. In practice however, integrated care rarely delivers on the high expectations of those who implement it. 7 Financial factors, and specifically lack of integration of budgets across sectors, are frequently cited as a major barrier to success.7–9 However, the effects of integrating funds are rarely considered 10 and this review seeks to address that gap in the evidence base. In order to interpret the evidence, we first set out a framework for understanding the nature of the problem, and how integrated financing may – or may not – address it.
The role of integrated finance in integrated care
The potential impacts of integrated funding on integrated care.
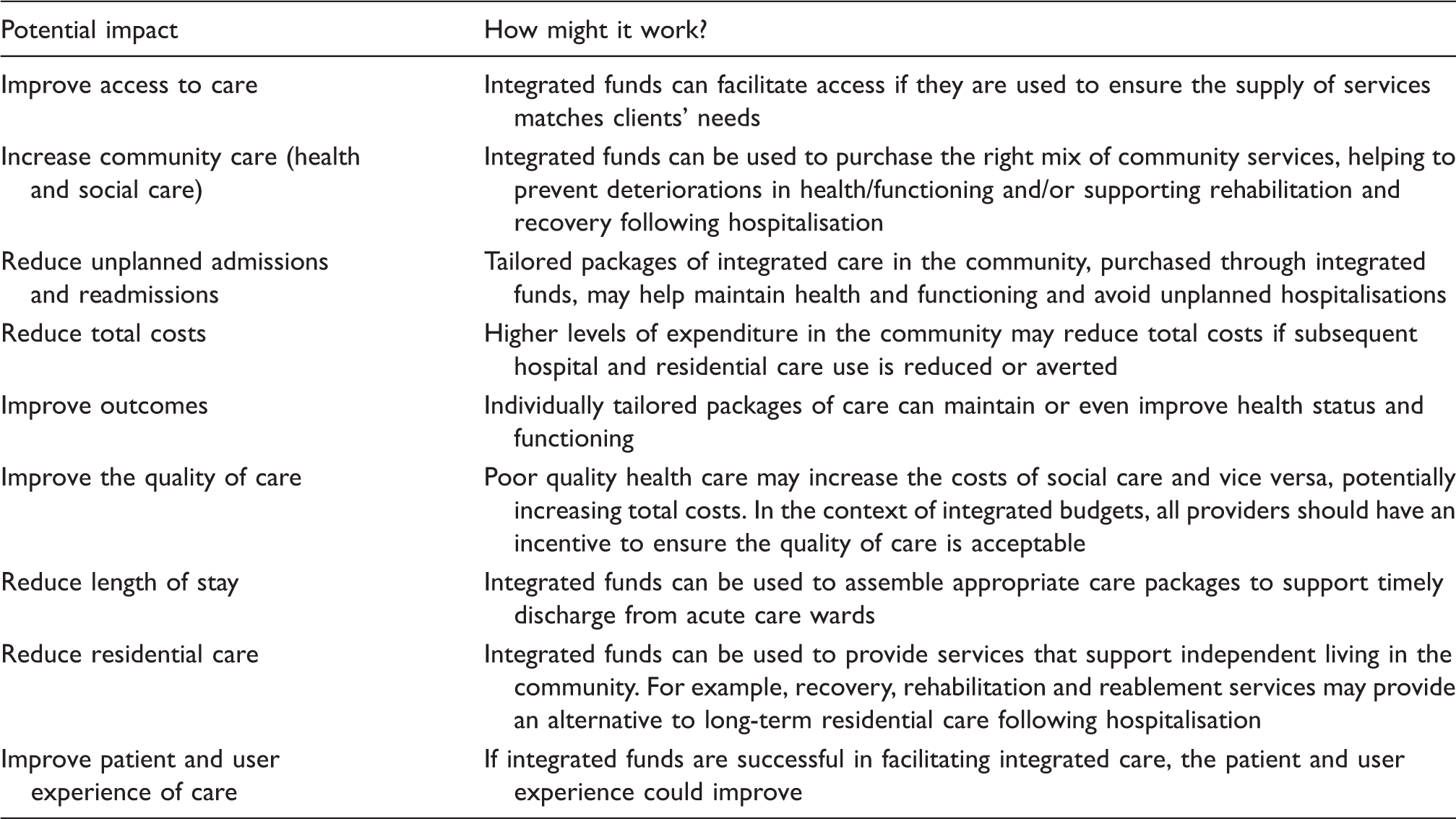
In practice, however, the positive effects listed in Table 1 have proved elusive.1,7,13,14 Financial integration may help to facilitate integrated care.7–9 To understand how this might work, we consider this problem from an economics perspective.
In economics, an agency relationship is said to exist whenever there is an element of delegated decision making. In the health care sector, where patients rely on many different professionals to design and implement their care, agency relationships are all pervasive. 15 Traditionally, managing agency in health care relies on aligning the incentives of a health care provider with those of the patient and (or) the health care funder. 16
The problem in the context of integrated health and social care is, however, much more complex. Where there are two or more providers of different services to an individual (‘user’), those services interact to define not only the benefit to the user but also how much effort and expenditure is required by each provider. For example, inappropriate social care will affect the user’s well-being but may also increase the risk (and possibly the cost) of hospital admission. Equally, hospital care that reduces impairment (such as hip replacement) may reduce social care costs. 17 In other words, the productivity of each provider is interdependent.
A formal model of agency in such a setting is beyond the scope of this article, but some of the practical implications can be understood in relation to a stylized example.
Suppose there are two care providers, a hospital denoted H and a social care organisation denoted S. The level and quality of social care provided by S will affect the expected cost and benefit of hospital care provided by H, and vice versa. If S and H are rewarded separately, for example by a fixed price for each package of care they provide, there is an immediate problem. Each provider will want to achieve the lowest cost of delivery consistent with its own goals (i.e. ‘economize’), which may include an altruistic concern for those they treat but is unlikely to reflect the consequence of their actions on the other provider. But if both act in this way, each is adversely affected, as is the user. Fixed prices have considerable merit in managing a single-agency relationship – they provide strong incentives to make efficient choices – but in this setting, they may result in a poor outcome for all parties.
One response to this problem is to integrate S and H into a single organisation. That does not necessarily solve the problem – organisations face internal agency problems – and it might involve a further loss of efficiency because there are often argued to be benefits of specialisation. 18
An alternative approach is to incentivize both S and H to take account of their actions on the totality of care that a user will need, rather than considering only the implications for themselves. One mechanism is to tie H and S together financially by setting a fixed total budget covering health and social care for an individual (i.e. a capitated budget). The argument is that if S perceives that economising on its care will increase costs to H it will also perceive the impact on itself through a diminished proportion of the total capitated budget that it can claim. In this way, the hope is that a fixed overall budget will internalize some of the external effects of unilateral decisions.
The outcome from integrating budgets depends on the precise interdependency of decisions and, crucially, how the fixed budget is ultimately allocated between S and H (i.e. the extent to which risk is shared). If there is an imbalance of power so that H can override S’s claim on the total budget, the outcome will be the same as that which would prevail under separate budgets. Effective use of the budgets presupposes that decisions are based on good information. If agents have imperfect information on client need, service history or the effectiveness of different care packages – or if one agent has better information than the other (information asymmetry) – then inefficiencies and gaming behaviour may result. Lastly, if governance and regulatory frameworks remain separate, then integrated budgets may offer insufficient incentives to integrate care.
These complex issues that determine the impact of integrated finances raise questions that can only be resolved empirically. We therefore now consider the evidence from the literature.
Methods
Our review was designed to address three questions:
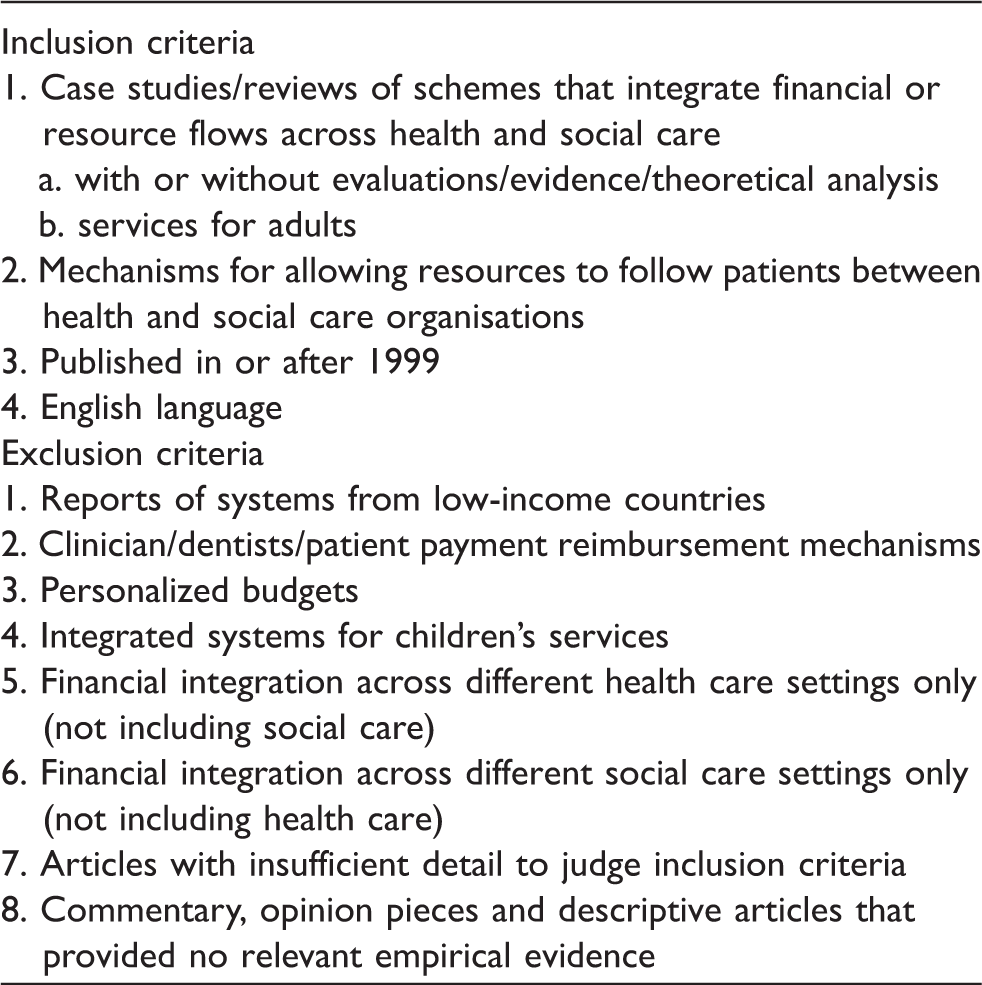
Inclusion and exclusion criteria for the review.
We extracted data on the types of financial integration used by relevant schemes, their benefits and costs (including unintended effects) and the barriers to implementation. Findings were interpreted with reference to the agency-based framework.
Results
Findings from the searches
The searches identified around 3500 records (Figure 1). After screening and checking individual records for eligibility, 122 full-text articles were included in the review (see Appendix 1 for a complete list of references). The articles covered 38 individual schemes from eight countries. Fifty-four schemes were excluded because they did not meet one or more of the inclusion criteria – for instance, there was no financial integration (35%), or funds were integrated only across health care settings (57%).
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram showing results of the literature searches.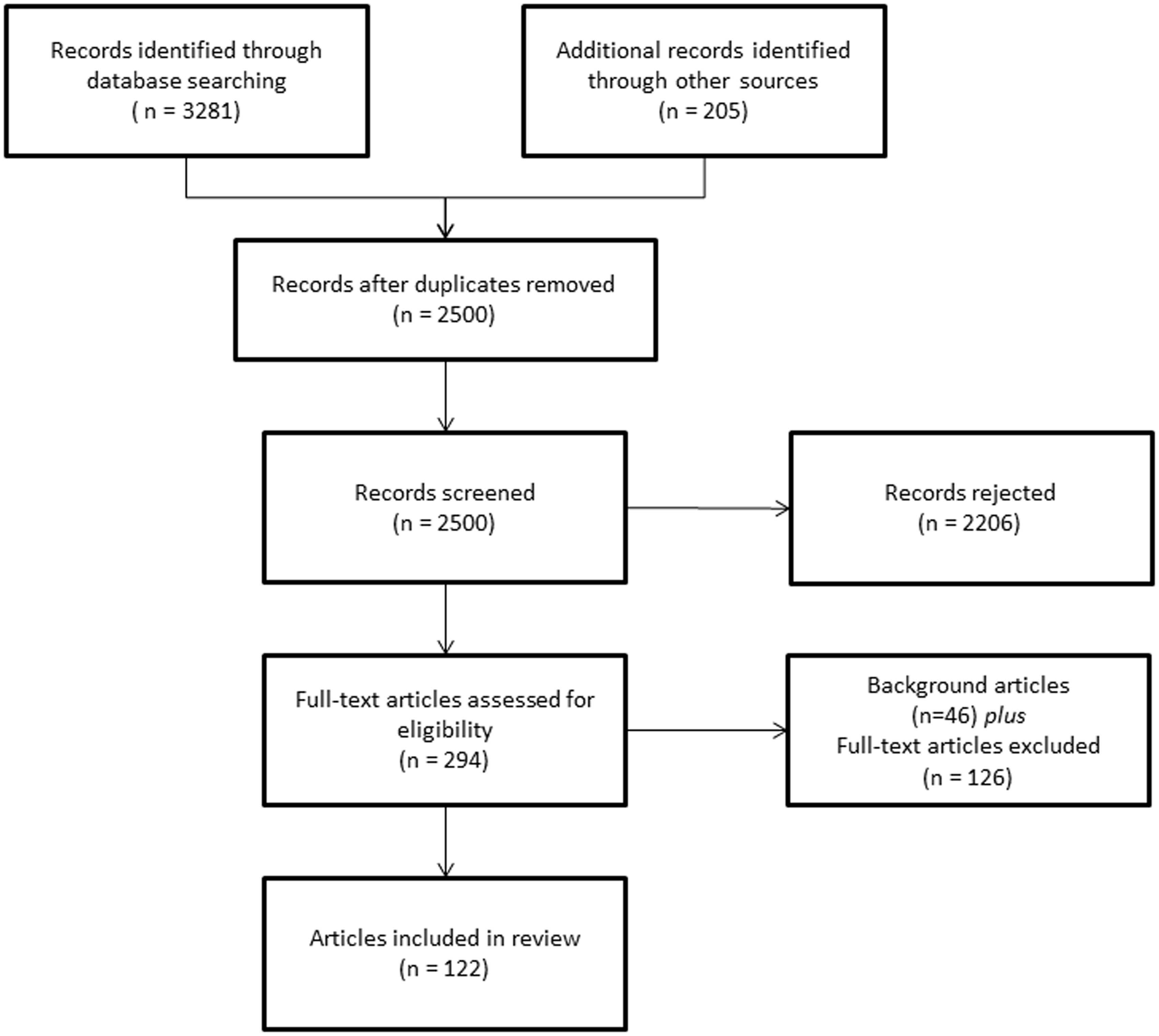
Study designs underpinning the evidence base
Six schemes (16%) were evaluated by randomized controlled trials (RCTs), and there was evidence from quasi-experimental studies for 12 (32%) schemes. The quasi-experimental studies typically compared an intervention group with matched controls drawn from another geographical area. Qualitative studies, such as semi-structured interviews or focus groups, were used to evaluate 17 schemes (45%). Mixed methods studies, usually combining data analysis with qualitative methods, were used for 10 schemes (26%). Fifteen schemes (39%) were evaluated using data from uncontrolled studies and analyses of administrative data were used in 10 schemes (26%).
The methodology varied markedly across countries. With the exception of one Canadian trial, all the randomized evidence came from Australia. Quasi-experimental studies were used in Australia, Canada, England, Sweden and the US. The predominant methodology in the UK was qualitative and/or uncontrolled evaluations.
Types of financial integration
Types of financial integration.
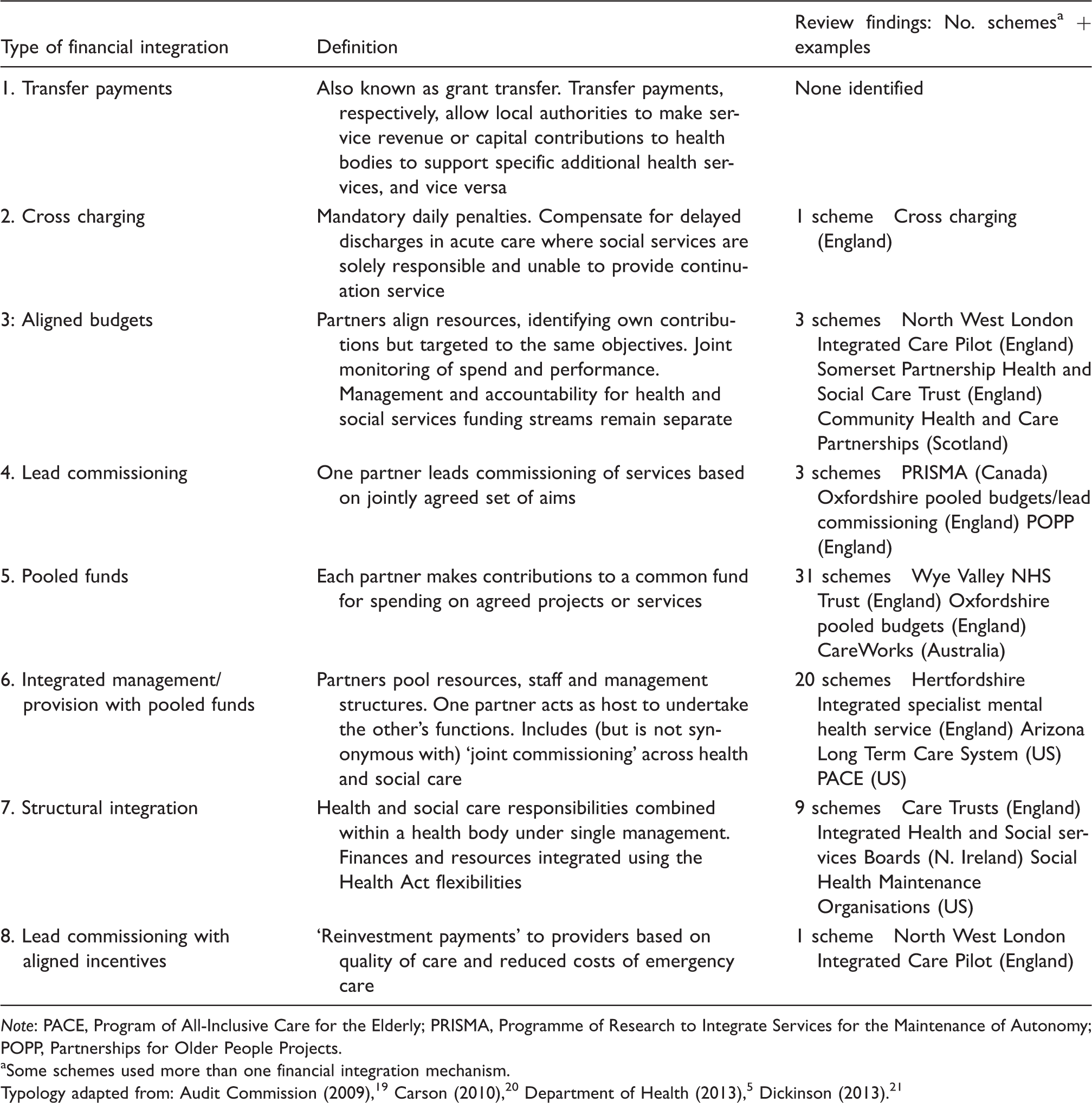
Note: PACE, Program of All-Inclusive Care for the Elderly; PRISMA, Programme of Research to Integrate Services for the Maintenance of Autonomy; POPP, Partnerships for Older People Projects.
Some schemes used more than one financial integration mechanism.
Ideally, we would report findings by the type of financial integration – for example, the impact of pooled funds on health outcomes or on service use or costs. However, this approach proved infeasible for several reasons. First, the funding mechanism was rarely well described – perhaps because evaluations were not designed to test the impact of financial integration. Therefore, categorising the schemes by type of financial integration was often a subjective judgment based on imperfect information. Second, there was a great deal of heterogeneity within the funding types listed in Table 3. For instance, over 80% of the schemes in our review utilized some type of pooled budget. Pooled budgets varied their scope, ranging from budgets that covered a broad set of services to those covering a single service (such as community equipment); in many schemes, the scope was unclear. Third, some used more than one financial integration mechanism (as is clear from Table 3). To disentangle the impact of pooling would require information that was not available from the published reports. Fourth, some ‘schemes’ were actually programmes of initiatives, only a fraction of which used financial integration. Unfortunately, disaggregated results for individual initiatives were not reported. Finally, both the model for integrating care and the target clientele varied between schemes using similar integrated funding approaches. Inferences about the effects of financial integration would need to account for these differences, but this level of detail was inconsistently reported.
The evidence on the impacts of integrated care with integrated financing.

Health effects
The evaluations assessed a variety of outcomes, including measures of health-related quality of life, physical functioning, depression and anxiety, mortality and carer burden. Twenty-four (63%) schemes assessed health outcomes and 13 of these found no significant difference from usual care. In the remaining schemes, findings were mixed (five schemes), health outcomes were better in the integrated scheme (n = 5), or worse in the integrated scheme (n = 1).
All 18 controlled studies assessed health outcomes. In a joint venture between commonwealth, state and territory Australian governments, two rounds of coordinated care trials (CCT) (‘schemes’) were held in the late 1990s (13 trials; CCT1) and the mid-2000s (five trials; CCT2). The schemes were intended to be cost neutral and to improve clients’ health and well-being. 12 Eight schemes met the inclusion criteria for our review, six from round 1 and two from round 2. All eight schemes had pooled funding but used different models of integrated care. Six were randomized and two had geographical controls.
In six of the eight Australian schemes, the intervention did not consistently deliver better health benefits than usual care. In one of the randomized CCT2 trials, the intervention group had significantly better general health, less depression and better health-related quality of life at the end of the study. 12 In the remaining quasi-experimental study, there was a significantly greater deterioration in physical functioning in the intervention group. 22 A randomized trial of the Canadian scheme SIPA (Système de services intégrés pour personnes âgées en perte d autonomie: integrated services for frail elders) found neither health status nor mortality differed significantly from those allocated to standard care. 23
One of the remaining nine controlled studies found a significant health benefit in favour of the integrated scheme. ‘On Lok’ was developed in response to a shortage of skilled nursing beds for the local community in Chinatown, San Francisco. 24 Using adult day care to provide health and social care services, case management was delivered by a multidisciplinary team. By pooling funds from Medicare and Medicaid, the team took financial responsibility for all acute and long-term care, including primary care. A two-year quasi-experimental study reported significant benefits in physical functioning for On Lok clients, 25 and the scheme became a prototype for Program of All-Inclusive Care for the Elderly (PACE). However, the health benefits achieved by PACE were ambiguous 26 and uptake of the programme was poor: in 2008, PACE enrolment equated to less than a quarter of 1% of the 9 million eligible individuals. 27
These results derive from the better designed studies, involving RCTs or geographical controls, although even these often posed methodological issues in relation to the strict comparability of groups. The positive health impacts were found in studies that generally had well-developed and comprehensive pooling arrangements across a range of sources, creating large health and social care budgets (e.g. merging budgets for Medicare and Medicaid in On Lok, and from all major providers in the Australian trial).
Service use and costs
The review identified evidence on secondary care costs and/or utilisation for 34 (89%) schemes. Eleven schemes had no significant effect on hospital costs or utilisation, three schemes reported a significant reduction in utilisation or costs and admission rates were significantly higher in one of the Australian CCT1 schemes. 22 In the remaining schemes, the evidence was mixed (14/34 schemes) or unclear (5/34).
None of the five Australian RCTs found a significant difference in secondary care costs, although both the second-phase Australian RCTs reported a nonsignificant trend towards lower hospital costs in the coordinated care group, reflecting lower rates of hospital admission. The trialists concluded that the intervention was likely to be cost-neutral in the longer term. 12 In one CCT1 trial, there was no significant difference in the admission rate or risk of admission, but length of stay was significantly shorter in the intervention group.22,28 The Canadian SIPA trial was cost neutral, with participants incurring higher community care costs that were offset by the reduction in the costs of institutional care. There was also a significant reduction in the number of acute hospital patients with delayed discharges (‘bed blockers’), and the cost of nursing home care was significantly lower in the subgroup of frail older people who were living alone at the start of the trial. 23
A before-and-after evaluation of England’s cross-charging policy, in which councils were charged a daily fine if they were solely responsible for a case of inpatient ‘bed blocking’, 19 identified that the downward trend in delayed discharges had accelerated after the legislation’s introduction. 29 In the Oxfordshire pooled budgets/lead commissioning model, 30 initial reductions in delayed transfers of care were not sustained.
A difference-in-difference analysis of the English Integrated Care Pilots (ICPs) found that integrated care was associated with significantly higher rates of emergency admission, but rates of elective admissions and outpatient visits were significantly lower. There was no significant difference in the use of emergency room services. 31 However, few of the pilot schemes explicitly integrated funds across health and social care and the evaluations did not attempt to isolate the effect of the funding approach. Cumbria Primary Care Trust set out to integrate funds, although it is unclear whether this was actually achieved (personal communication with evaluators, 6 May 2013). Emergency admissions fell over the study period, but this downward trend predated the start of the pilot. Another ICP pilot, Torbay, successfully integrated funds. When compared against a neighbouring area over a three-year period, the rate of increase in Torbay’s emergency admissions was lower, and reductions in mean length of stay for older people were larger. The extent to which this effect was attributable to integrated funding was not evaluated.
In another scheme targeting this client group, the resource implications were mixed. Funded at a cost of £60 million, the Partnerships for Older People Projects (POPP) pilots employed earlier, targeted interventions within community settings to promote health, well-being and independence and to prevent or delay the need for hospital or institutional care. 32 The national evaluation compared POPP sites using difference-in-difference with geographical controls (usual care) and found a significantly greater reduction in emergency bed days. However, an evaluation of a subset of interventions with the potential to reduce avoidable unplanned hospitalisation found no evidence of reduced use of acute hospitals, 33 except for a high-risk subgroup in one intervention. Data on the use of integrated funds in individual POPP schemes was not available and so the outcome in this particular intervention cannot be linked to a specific funding approach – indeed, it is not clear that integrated funds were used in this POPP scheme. Similarly, an analysis of S/HMO II (Social Health Maintenance Organization, wave 2) identified reduced hospital admissions for a subgroup of people with two or more hospitalizations in the previous 12 months. 34 In both, this case and in the POPP scheme evaluation, 33 the findings may reflect a statistical phenomenon known as ‘regression to the mean’ whereby extreme – high or low – observations are likely to be followed by less extreme observations. 35
Quality of care and user experience
Studies assessed the quality of care in a variety of ways, with many eliciting the views of staff, patients and carers about their experience of the integrated care schemes, collected either via surveys, focus groups or, in some cases, anecdotally. Results were mixed: clients in the Australian trials 12 reported improved access to services and improved knowledge of health services; findings for North West London pilot were similar. 36 In the whole-system evaluation of ICP in England, 31 patients reported some negative experiences such as being unable to see staff of their choice and feeling less involved in care decisions, whilst some mental health service users in the English Somerset scheme reported greater engagement. 37 Most (75%) of the ‘key informants’ surveyed in the POPP schemes 38 felt that the schemes improved access and offered a broader range of services. Studies of the Minnesota Senior Health Options initiative 39 and the PACE programmes 26 found no substantial differences in satisfaction.
In terms of more objective process measures of quality, there were higher numbers of care plans produced for dementia patients and greater use of testing for diabetes in the North West London pilots; 40 the US Veterans Health Administration (VHA) reported significant improvements in the quality of care relative to Medicare fee-for-service and generally outperformed Medicare and Medicaid on a range of quality measures. 41 In the US, the Commonwealth Care Alliance reported high scores for some HEDIS (Healthcare Effectiveness Data and Information Set) process measures of care quality, 42 but evaluations of S/HMO II found no evidence that the quality of care was consistently better than care received by those enrolled in other Medicare HMOs or other comparator groups. 34
Unintended consequences
Studies of PACE found that some programmes denied access to those with psychiatric or substance abuse problems (‘cream skimming’). 24 The S/HMO I evaluations revealed that clients deemed to be ‘nursing home certifiable’ were less frail and complex than expected – which may have been due to the higher fee this paid for this client group (incentivising ‘upcoding’). The assessment of cross-charging in England identified anecdotal evidence that the scheme led to poor outcomes for patients in terms of ‘overly hasty’ discharge and increased risk of readmission. 29 These findings suggest that budgets that do not encompass the full care pathway may fail to align incentives and may still encourage cost shifting between the sectors within the scheme and those outside it. Even where budgets are pooled widely, total resources remain limited and those making decisions about who is eligible to take part in the trial or scheme may face incentives to act in ways that are more likely to produce positive results for the scheme. This may be particularly acute where the schemes themselves are run for a limited duration, but where full realisation of benefits is only likely to emerge in the longer term when the trial is over, as in such instances those engaged in the study may be keen to see quick results.
Barriers to integration
The primary ‘barrier’ to emerge from the review was the difficulty of implementing financial integration, despite the existence of statutory and regulatory measures to support it. This problem affected the Australian CCT2 trials and many UK schemes. The Australian CCT1 trials succeeded in pooling funds, 28 but failed to break down service boundaries or give budget holders control over clients’ service use – some services in the care plan were accessible only if clients met preexisting eligibility criteria. 43 In one Australian scheme, hospital doctors were opposed on the grounds that it would ‘restrict specialist access’. 28 Similar barriers were evident in the SIPA model (Canada), PACE and the Wisconsin Partnership Program (US), the Integrated Health & Social Services Boards (Northern Ireland) and Torbay (England). These examples illustrate how providers may be ‘double agents’, 44 where care for the individual may be influenced by the provider’s personal objectives such as maintaining clinical autonomy (i.e. determining who is treated, how and when).
Relational difficulties also beset the integration of care itself. The demonstration S/HMO I failed to integrate acute and long-term care because relations between care coordinators (typically social workers) and physicians were ‘poorly developed’. 34 The S/HMO II models therefore sought to engage physicians directly in care coordination. Difficulties related to physician engagement were also reported in Torbay (England) 45 and in the Australian trials, where some general practitioners (GPs) reportedly found the care-planning process bureaucratic, burdensome and of uncertain value. 22 One of the rationales for integrated financing is that it can help to align the incentives of agents in the health and social care system. But by itself it cannot address deeply engrained, sometimes cultural, differences between decision makers in each sector, who continue to operate with reference to their own set of objectives, constraints and attitudes to risk sharing. It also illustrates the importance, irrespective of the financial arrangements, of buy-in and leadership by key actors in the system. 46
Another barrier was the difficulty of engaging with those eligible for care. For instance, study recruitment difficulties were reported in the Australian CCTs, PRISMA (Programme of Research to Integrate Services for the Maintenance of Autonomy, Canada), S/HMO II (US) and PACE (US). This may partly be a reflection of the model of care; for example, adult day care, which is a key feature of PACE, is unappealing to many eligible clients. 24
Challenges of implementing a fully operational information management and technology system were reported in many schemes. Technical problems included incompatibilities in software and hardware, coding systems and user access. 47 Despite experience from the first round, all of Australia’s second round trials underestimated the resources and skills required to implement these highly complex systems. 12 Data governance concerns also obstructed implementation. For instance, one Australian scheme successfully produced client records of service use to support coordinated care. However, concerns about the implications for client confidentiality were so serious that the sponsors removed the original requirement that GPs consult with other providers. This fundamentally undermined the collaborative aims of the scheme. 28
In the UK, there were incompatibilities between the national performance and audit systems for health and social care, differences in pension schemes that impeded the transfer of staff across sectors, and uncertainty about whether health organisations could legally employ social workers. 47 Importantly, integrating management did not remove statutory responsibilities and accountabilities and these sometimes provided incentives to act unilaterally. 48 In the English POPP evaluation, translating cost reductions into cost savings was usually impossible due to difficulties in transferring funds across care boundaries. 38
Discussion
The integration of finances should, in principle, facilitate integrated care as suggested by the agency framework presented in this paper; the evidence base for integrated care consistently identifies financial factors as a major barrier to successful delivery, and policy makers frequently invoke financial integration as a panacea for achieving better care at lower cost.49,50
However, despite these expectations, our review finds that the case for integrated funding has not yet been demonstrated. The literature review identified empirical evaluations for 38 schemes that involved integrated financing for health and social care. No scheme demonstrated a sustained reduction in hospital use, although there was some evidence that care could be shifted into the community and access to services improved. Only a small fraction of the schemes included in the review delivered significant improvements in health outcomes.
This does not mean that policy makers should disregard the potential of integrated finance, but rather that expectations should be realistic and careful research should be planned. The literature reveals that incomplete information (e.g. because of the difficulties of linking health and social care data) was a common problem, and that even if cultural and governance differences were resolved at management level, budget holders might remain unable to provide their clients with access to appropriate services. If integrated funds are to be a model for the future, attention needs to focus on how they can be implemented in practice and it will be important not to underestimate the efforts required to forge and to maintain the relationships that underpin the financial mechanisms.
Evaluating the impact of financial integration is methodologically challenging, and the studies reviewed here were not designed to isolate its effects. Given the complexities of financial integration, the likelihood that its benefits will be small according to existing evidence, and the many different factors that confound attempts to reliably assess outcomes, future evaluations should strive to incorporate appropriate – and, preferably, randomized – controls.
Even if well-controlled studies identify a cost-effective model that incorporates integrated financing and coordinated care, the nature of integrated care means that overall system costs may increase. A model that focuses greater attention on patient needs increases the likelihood that coordinated care ‘reveals rather than resolves’ unmet need. 43 Whilst this may be a beneficial outcome for society, its feasibility depends upon policy makers’ willingness and ability to pay.
Footnotes
Authors’ note
The views expressed are those of the authors and not necessarily those of the funders.
Acknowledgements
We are grateful to Kath Wright, Lisa Stirk and Rocio Rodriguez Lopez from the Centre for Reviews and Dissemination, University of York (UK), for undertaking the literature searches. We would also like to thank two anonymous reviewers for their constructive comments, and Dr Fiona Aspinal (University of York, UK) for her insights on an earlier draft of this paper.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This work was supported by a grant from the Department of Health to the Policy Research Unit in the Economics of Social and Health Care (Project reference: 103/0001).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.